|
The following CBME core competencies are covered in this chapter.
|
Acute Otitis Media
Introduction and Definition
Acute otitis media (AOM) is an inflammatory condition of the middle ear cleft of rapid onset, caused by viral or bacterial infection, and characterised by the presence of middle ear effusion along with signs and symptoms of acute inflammation. It is primarily a disease of childhood, with peak incidence between 6 and 24 months of age, though it can occur at any age.
Key distinction from Otitis Media with Effusion (OME): In OME, middle ear effusion is present without signs or symptoms of acute infection (no ear pain, fever, or erythema of tympanic membrane). OME is not a stage of AOM; it may precede or follow AOM, but requires different management.

Classification of Otitis Media
Otitis media includes a group of inflammatory and infectious conditions affecting the middle ear cleft. It is classified as:
| Type | Duration | Key Feature |
| Acute otitis media (AOM) | <3 weeks | Acute infection + effusion + inflammation |
| Sub-acute otitis media | 3 weeks – 3 months | Transitional; may resolve or progress to chronic |
| Chronic otitis media (COM) | >3 months | Chronic inflammation of the middle ear cleft ± perforation, with or without cholesteatoma |
| Otitis media with effusion (OME) | Variable | Effusion WITHOUT acute inflammation |
| Adhesive otitis media | Chronic | Atelectasis, TM retracted & adherent to promontory |
For PG: OME and adhesive OM are sequelae, not acute infections. They are covered separately.
Epidemiology
- Peak age: 6–24 months with slight male predominance.
- Seasonal variation: Winter and early spring season.
- Incidence: ~50% of children have at least one episode by age 1 year; ~80% by age 3 years.
- Recurrence: 10–20% of children experience ≥3 episodes by age 3 years.
Aetiology
AOM results from viral, bacterial, or mixed infection. The microbiology has changed after the introduction of pneumococcal conjugate vaccines (PCV7, PCV13).
Viral pathogens:
- Respiratory syncytial virus (RSV) and Rhinovirus – most common
- Influenza A and B, Adenovirus and Coronavirus – less common
Bacterial pathogens:
- Streptococcus pneumoniae – most common, 25–50% of cases (declining post‑vaccine)
- Non‑typable Haemophilus influenzae – 15–30% (now relatively more common)
- Moraxella catarrhalis – 10–20%
- Group A Streptococcus – 2–5%
- Staphylococcus aureus – 1–2% (more common in recurrent AOM)
Viruses can cause AOM alone or predispose to bacterial superinfection by causing Eustachian tube dysfunction.

Routes of Infection
- Eustachian tube (most common): Ascending infection from the nasopharynx. Predisposed in children due to shorter, more horizontal, and more compliant Eustachian tube.
- Tympanic membrane perforation: Direct spread from the external auditory canal (rare in AOM; more relevant in chronic suppurative otitis media).
- Haematogenous: Uncommon, but possible in septicemia.


Risk Factors
- Host factors: Age <2 years, male sex, prematurity, low birth weight
- Eustachian tube dysfunction due to adenoid hypertrophy, upper respiratory tract infection or sinusitis.
- Anatomic: Cleft palate, Down syndrome, Turner syndrome, craniofacial anomalies
- Immunologic: IgG2 subclass deficiency, low mannose-binding lectin, primary ciliary dyskinesia
- Environmental: Daycare attendance, household crowding, passive smoke exposure, pacifier use
- Feeding: Lack of breastfeeding (especially <3 months), bottle feeding in supine position
- Previous history: Recurrent AOM, family history of otitis media
- Malnutrition
- Vitamin A deficiency
- Low socioeconomic status


Pathogenesis
URTI / Allergy
↓
Nasopharyngeal inflammation ± adenoid hypertrophy
↓
Eustachian tube dysfunction
↓
Negative middle ear pressure
↓
Fluid accumulation (effusion)
↓
Bacterial/viral invasion
↓
Suppuration (pus formation)
↓
Bulging TM → severe pain
↓
Perforation → otorrhea + pain relief
↓
Healing / Residual OME
Clinical Features and Stages of AOM
The course of the disease is usually divided into five stages, which begin from the stage of eustachian tube occlusion, pre-suppuration, and suppuration and end with either the stage of resolution or complications. If appropriate antibiotic therapy is started early in the course of AOM, the disease process may regress from any stage. Regression may also begin without rupture of the TM.
Eustachian tube occlusion (Stage 1).
Generally, viral infection of the upper respiratory tract precedes otitis media involving the mucosa of the nose, nasopharynx, middle ear mucosa, and eustachian tubes. Oedema and hyperaemia of the nasopharyngeal end of the eustachian tube block the tube, resulting in a decrease in ventilation. This leads to a cascade of events resulting in the absorption of air and negative pressure in the middle ear. There is retraction of the tympanic membrane with some degree of effusion in the middle ear, but the fluid may not be clinically visible.
- Symptoms. Mild hearing loss, Ear fullness, Mild Earache and no fever.
- Signs. There is retraction of the tympanic membrane with loss of the light reflex. The handle of malleus is more horizontally placed and the lateral process of the malleus is more prominent. Tuning fork tests show conductive hearing loss.
Pre-suppuration (Stage 2)
This stage occurs if the eustachian tube is still not opened because the patient is not taking medications or taking inappropriate medications. This results in the development of more negative pressure in the middle ear and the production of inflammatory exudate from inflamed hyperaemic middle ear mucosa. Due to ineffective drainage from the eustachian tube, there is also a collection of mucosal secretions. This allows invasion of bacterial and viral organisms in the middle ear, but there is still no pus formation in this stage. That is why this stage is called as “stage of pre-suppuration”.
- Symptoms. There is a severe throbbing earache that may disturb sleep. There is a high-grade fever. Hearing loss and tinnitus are present.
- Signs. Tympanic membrane appears red due to congestion, giving a “cart wheel appearance” (leash of blood vessels along the handle of the malleus and at the periphery of the TM). There is a bulge of the tympanic membrane due to the collection of exudate and mucosal secretion in the middle ear. Tuning fork tests show conductive hearing loss.
Suppuration (Stage 3).
In this stage, due to bacterial organisms in the middle ear, there is the formation of pus in the middle ear and to some extent in the mastoid air cells. It is due to an immunologic response that destroys the offending bacterial organism, culminating in the collection of pus in the middle ear. In the stage of pre-suppuration, there was a bulging of the tympanic membrane, but now in the stage of suppuration, the bulge will reach to the point of rupture. Sometimes a nipple-like protrusion may also be seen in the tympanic membrane with a yellow spot marking the point of rupture.
- Symptoms. There is excruciating ear pain. Increasing deafness. Due to the absorption of toxins, the child develops constitutional symptoms like fever of 102–103 °F, accompanied by vomiting, diarrhoea and even convulsions.
- Signs. The tympanic membrane appears red and bulging to the point of rupture with loss of landmarks. The handle of malleus is engulfed by the swollen and bulging tympanic membrane. There is tenderness present over the mastoid antrum. There is clouding of air cells in the X-ray mastoid due to the presence of exudates.
Resolution (Stage 4).
The tympanic membrane, which was at the point of rupture in the stage of suppuration (stage 3), ruptures (due to pressure necrosis) in this stage, with the release of pus, and there is relief from symptoms. The inflammatory process begins to resolve. If appropriate treatment is started early or if the infection was mild, resolution may start even without rupture of the tympanic membrane.
- Symptoms. With the release of pus, the earache is relieved, the fever comes down, and the patient feels better.
- Signs. The external auditory canal may contain blood-tinged discharge (serosanguinous), which later becomes mucopurulent. The discharge can be pulsatile, showing the characteristic “lighthouse effect” (i.e. pus comes out under pressure and synchronises with each arterial pulse). Usually, a small perforation is seen in the posteroinferior quadrant of the pars tensa. Hyperaemia of the tympanic membrane begins to subside with the return to normal colour and landmarks.
Complications (Stage 5).
Usually, AOM is self-limiting in children and subsides well to medical treatment. If the virulence of the organism is high and the resistance of the patient is poor, the infection may spread beyond the middle ear boundaries. Complications usually occur in the second week, and signs and symptoms reappear. It may lead to acute mastoiditis, subperiosteal abscess, facial paralysis, labyrinthitis, petrositis, extra-dural abscess, meningitis, brain abscess or lateral sinus thrombophlebitis.
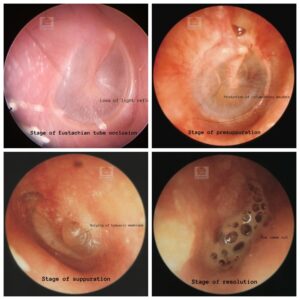
Endoscopic images of TM in various stages of ASOM
Clinical Features by Age Group
- Infants (<2 years): Non‑specific presentation – fever, irritability, crying, pulling at ear, poor feeding, vomiting, diarrhea. Otalgia cannot be verbalized.
- Children (2–12 years): Earache (otalgia), hearing loss, fever, sometimes ear discharge (if perforation). Child may be restless and hold the ear.
- Adults: Ear pain, fullness, hearing loss; fever less common. Often associated with upper respiratory infection or Eustachian tube dysfunction (e.g., barotrauma).
Diagnostic Criteria
Diagnosis of AOM requires all three of the following:
- Acute onset – of signs and symptoms (duration <3 weeks per original definition, but clinically <48–72 hours for acute management).
- Middle ear effusion – documented by pneumatic otoscopy (bulging TM, decreased mobility, otorrhea, or air‑fluid level). Tympanometry (Type B curve) confirms effusion.
- Signs/symptoms of middle ear inflammation – otalgia (ear pain) or erythema of TM.
Pneumatic otoscopy findings – diagnostic hierarchy:
- Bulging TM (marked or moderate) – highest specificity for AOM
- Otorrhea (new onset, not due to otitis externa) – confirms perforation, almost diagnostic
- Erythema (redness) alone – low specificity (can occur with crying, fever)
- Retracted TM without bulging – suggests Eustachian tube dysfunction or OME, not AOM
Exam Pearl: AOM is overdiagnosed when only redness of TM is present (e.g., a crying child). Always use pneumatic otoscopy to assess mobility. A red but mobile TM is usually not AOM.
Differential Diagnosis
- Otitis media with effusion (OME): Middle ear effusion present, but no signs of acute inflammation (no pain, no fever, TM not red or bulging).
- Acute otitis externa: Pain on tragus manipulation or pinna pull, ear canal oedema/erythema, TM normal (unless secondary).
- Myringitis: Inflammation of the TM without middle ear effusion; may be bullous (bullous myringitis), often viral.
- Referred otalgia: Normal TM and middle ear; causes include dental infection, temporomandibular joint pathology, tonsillitis, pharyngitis.
- Eustachian tube dysfunction: Fullness, popping, TM retracted but mobile; no effusion or inflammation.
Management
1. Analgesia and antipyretics – first line for all patients
- Paracetamol (acetaminophen) 10–15 mg/kg/dose every 4–6 hours.
- Ibuprofen 5–10 mg/kg/dose every 6–8 hours.
- Avoid aspirin in children.
- Topical anaesthetic drops (e.g., benzocaine with antipyrine) can provide transient relief but are not recommended if TM perforation is suspected.
2. Watchful waiting (observation without antibiotics)
Indicated for select children based on age, severity, and laterality. Observation period is 48–72 hours with rescue antibiotics if symptoms worsen or fail to improve. Clear instructions must be given to caregivers.
Criteria for observation (AAO‑HNS guidelines):
- Age ≥6 months with non‑severe illness (mild otalgia, temperature <39°C) AND
- Unilateral AOM if age 6–23 months, OR unilateral or bilateral if age ≥2 years
- No high‑risk conditions (immunodeficiency, craniofacial anomaly, cochlear implant)
3. Antibiotic therapy – indications for immediate antibiotics
- Age <6 months (any AOM)
- Age 6–23 months with bilateral AOM
- Any age with severe symptoms (severe otalgia, temperature ≥39°C, toxic appearance)
- Presence of perforation with purulent discharge
- High‑risk children: immunosuppression, cleft palate, Down syndrome, cochlear implant, recurrent AOM on prophylaxis
- Failure of watchful waiting (no improvement or worsening at 48–72 hours)
Antibiotic regimens:
- First‑line, uncomplicated AOM: Amoxicillin 80–90 mg/kg/day orally in two divided doses (maximum 3 g/day). Standard dose (40–45 mg/kg/day) is less effective due to resistant S. pneumoniae. Duration: 10 days for children <2 years or severe illness; 5–7 days for children ≥2 years with mild‑moderate illness.
- Penicillin allergy (non‑anaphylactic): Cefdinir 14 mg/kg/day orally once or twice daily, OR Cefuroxime axetil 30 mg/kg/day orally twice daily. Same duration as above.
- Penicillin allergy (anaphylactic): Azithromycin 10 mg/kg on day 1 then 5 mg/kg days 2–5, OR Clarithromycin 15 mg/kg/day orally twice daily for 10 days.
- Treatment failure (no improvement at 48–72 hours): Amoxicillin‑clavulanate (90/6.4 mg/kg/day) OR Ceftriaxone 50 mg/kg IM/IV daily for 3 days.
- Recurrent AOM (on amoxicillin within 30 days): Amoxicillin‑clavulanate or Ceftriaxone, 10 days.
4. Topical antibiotic drops
Use only when tympanic membrane perforation is confirmed (purulent otorrhea through a visible perforation or via tympanostomy tube). Avoid ototoxic drops (e.g., gentamicin, neomycin) if possible; use fluoroquinolone drops (ofloxacin, ciprofloxacin) as they are non‑ototoxic.
5. Myringotomy
Reserved for:
- Impending perforation with severe pain and bulging TM that fails to respond to 48–72 hours of medical therapy.
- Complications (mastoiditis, facial palsy) needing drainage.
- Treatment failure with persistent effusion and pain despite appropriate IV antibiotics (less common).
Myringotomy relieves pain immediately, allows culture of middle ear fluid, and prevents spontaneous irregular perforation. The incision is made in the postero‑inferior quadrant to avoid ossicles and facial nerve.
6. Adjuvant therapies – NOT recommended now
- Antihistamines – no benefit, may thicken secretions.
- Decongestants (oral or nasal) – no benefit, adverse effects.
- Corticosteroids (systemic) – not proven beneficial; reserved only for specific complications (e.g., facial palsy).
- Complementary medicine (e.g., chiropractic, probiotics) – insufficient evidence.
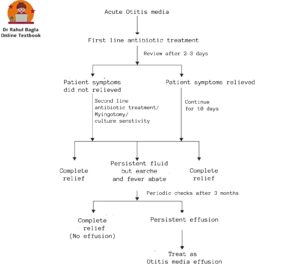
Flowchart of Treatment
Prevention of AOM and Recurrence
- Breastfeeding – reduces risk by about 50%. Encourage for at least 3–6 months.
- Avoid pacifier use after 6 months – modest benefit.
- Eliminate passive smoking – significant reduction.
- Pneumococcal conjugate vaccine (PCV13/PCV15/PCV20) – reduces vaccine‑type AOM by 30‑40%. Routine childhood immunization.
- Annual influenza vaccine – reduces AOM episodes. Recommended for all children ≥6 months.
- Tympanostomy tube (ventilation tube) – prevents recurrent AOM while in place. Indicated for recurrent AOM (≥3 episodes in 6 months or ≥4 in 12 months) failing medical management.
- Adenoidectomy – reduces recurrence, especially with nasal obstruction. Indicated for children ≥4 years with recurrent AOM and adenoid hypertrophy. Not first‑line for isolated AOM.
Complications of Acute Otitis Media
Complications are rare (<1% of AOM cases) but life‑threatening.
Intratemporal Complications
- Acute mastoiditis: Presents with post‑auricular swelling, erythema, tenderness, protruding pinna, and TM bulging or otorrhea. Management: IV antibiotics (ceftriaxone + clindamycin), myringotomy, ± cortical mastoidectomy if abscess present.
- Facial nerve palsy: Ipsilateral facial weakness (lower motor neuron type), usually due to inflammation via dehiscent facial canal. Management: IV antibiotics, steroids, myringotomy. Recovery is common if treated early.
- Petrositis: Deep facial pain (retro‑orbital), persistent otorrhea, Gradenigo’s syndrome (abducens palsy + facial pain + otorrhea). Management: Prolonged IV antibiotics, ± surgery (petrous apicectomy).
- Labyrinthitis: Vertigo, sensorineural hearing loss, nystagmus. Can be serous (toxic) or suppurative (purulent). Management: IV antibiotics, corticosteroids, ± labyrinthectomy (suppurative, non‑responsive).
Intracranial Complications
- Meningitis – most common intracranial complication. Presents with fever, neck stiffness, altered sensorium, Kernig/Brudzinski signs. Emergency management: IV antibiotics (3rd generation cephalosporin + vancomycin), lumbar puncture, ENT consult for source control.
- Brain abscess – usually temporal lobe or cerebellum. Presents with headache, focal neurological deficit, fever. Management: Neurosurgical drainage, IV antibiotics (metronidazole + 3rd generation cephalosporin).
- Lateral sinus thrombophlebitis: Persistent fever, headache, papilledema, ± otitic hydrocephalus. MRI/MRV shows thrombus. Management: IV antibiotics, anticoagulation (controversial), mastoidectomy with sinus exposure and thrombectomy if needed.
- Extradural empyema: Often silent; may present with persistent fever, headache. Management: Surgical drainage via mastoidectomy.
- Otitic hydrocephalus: Increased ICP without focal signs; headache, vomiting, papilledema. Management: Treat lateral sinus thrombosis, acetazolamide or CSF diversion if refractory.
Exam Pearl for PG students: Any child with AOM and high fever not responding to 48 hours of appropriate antibiotics should be evaluated for mastoiditis (post‑auricular signs) and intracranial complications (altered sensorium, focal signs, persistent headache).
Special Clinical Patterns
- Sporadic AOM: Infrequent episodes associated with upper respiratory tract infections. No special management beyond standard.
- Resistant AOM: Persistence of signs and symptoms beyond 3–5 days of appropriate antibiotics. Indicates treatment failure; switch to second‑line antibiotics (amoxicillin‑clavulanate or ceftriaxone).
- Persistent AOM: Recurrence of symptoms within 6 days after completing antibiotics. Differentiate relapse (same organism) versus reinfection; culture the middle ear fluid if recurrent.
- Recurrent AOM: Three or more attacks in 6 months OR four or more attacks in 12 months. Consider tympanostomy tubes, adenoidectomy (≥4 years), immunologic evaluation, pneumococcal vaccine, and influenza vaccine.
Outcomes and Prognosis
- Complete resolution occurs in about 80% of cases with or without antibiotics. Spontaneous resolution within 2–7 days in most viral or mild bacterial cases.
- Persistent middle ear effusion is seen in 30‑50% at 1 month and 10% at 3 months. Monitor; if persistent >3 months with hearing loss, consider tympanostomy tube.
- Perforation with otorrhea occurs in about 10% of cases. Usually heals spontaneously within weeks; persistent perforation requires ENT follow‑up.
- Recurrence within 6 months occurs in 20‑30% of cases. Higher risk if first episode before 6 months of age or daycare attendance.
- Complications (mastoiditis, etc.) occur in less than 1% of cases. More common in untreated or immunocompromised children.
———— End of the chapter ————
High-Yield Points
- AOM = acute onset + effusion + inflammation
- Bulging TM is the most specific sign
- Red TM alone is not diagnostic
- Most common organisms: S. pneumoniae, H. influenzae, Moraxella
- Viral URTI triggers AOM via Eustachian tube dysfunction
- First-line antibiotic: high-dose amoxicillin (80–90 mg/kg/day)
- Severe AOM always needs antibiotics (fever ≥39°C, severe pain, toxic child)
- Watchful waiting is allowed in mild cases with follow-up at 48–72 hours
- Failure at 48–72 hours → amoxicillin-clavulanate or ceftriaxone
- Mastoiditis is the most common intratemporal complication
- Gradenigo syndrome = otorrhea + retro-orbital pain + abducens palsy
- Recurrent AOM = ≥3/6 months or ≥4/12 months
- Tympanostomy tubes prevent recurrence while in place
NEET PG Style MCQs
- Most specific otoscopic finding of acute otitis media is: A. Retracted tympanic membrane B. Bulging tympanic membrane C. Cone of light preserved D. Tympanic membrane with normal mobility.
- First-line antibiotic for uncomplicated AOM in children is: A. Azithromycin B. High dose amoxicillin C. Ceftriaxone IM D. Ciprofloxacin ear drops.
- A 1-year-old child has bilateral AOM with fever. Best management is: A. Observe for 72 hours only B. Oral decongestants + analgesics C. Start antibiotics immediately D. Give antihistamines.
- A red tympanic membrane alone in a crying child indicates: A. Definite AOM B. Not sufficient to diagnose AOM C. Definite mastoiditis D. Otitis externa.
- Most common route of infection in AOM is: A. Hematogenous spread B. Eustachian tube route C. Direct spread via TM perforation D. Spread from inner ear.
- AOM with sudden pain relief followed by purulent discharge suggests: A. Otitis externa B. TM perforation C. Cholesteatoma D. Otosclerosis.
- A child fails to improve after 72 hours of amoxicillin therapy. Next best step is: A. Stop antibiotics B. Add antihistamines C. Switch to amoxicillin-clavulanate or ceftriaxone D. Start topical neomycin drops only.
- Recurrent acute otitis media is defined as: A. ≥2 episodes in 1 year B. ≥3 episodes in 6 months or ≥4 episodes in 12 months C. Persistent discharge for 3 months D. OME lasting 6 months.
- Gradenigo syndrome is associated with: A. Facial palsy + mastoid swelling B. Vertigo + SNHL + fever C. Otorrhea + retro-orbital pain + abducens palsy D. Fever + neck stiffness + photophobia.
- Tympanostomy tube insertion is indicated in: A. Recurrent AOM despite medical management B. First episode of AOM C. Mild unilateral AOM in 5-year-old D. Viral URTI with ear block only.
Answers
1: B. 2: B. 3: C. 4: B. 5: B. 6: B. 7: C. 8: B. 9: C. 10: A.
Clinical Case Scenarios (Practical/Viva-Oriented)
Case 1
A 2-year-old child has fever (39.5°C), irritability, and severe ear pain for 1 day. Otoscopy shows a bulging congested tympanic membrane.
Most likely diagnosis: Acute otitis media (severe)
Best management: Immediate antibiotics (high-dose amoxicillin) + analgesics
Case 2
A 10-month-old child has mild ear pain and fever 37.8°C. Otoscopy shows unilateral bulging TM with reduced mobility. Parents can return for follow-up.
Most likely diagnosis: Non-severe unilateral AOM
Best next step: Watchful waiting 48–72 hours + analgesics, rescue antibiotics if no improvement
Case 3
A 4-year-old child has ear discharge with pain relief after severe otalgia. Otoscopy shows perforation.
Most likely diagnosis: AOM with tympanic membrane perforation
Best management: Systemic antibiotics + topical fluoroquinolone ear drops
Case 4
A child treated for AOM still has high fever after 2 days. Examination shows post-auricular swelling, tenderness, and protrusion of pinna.
Most likely diagnosis: Acute mastoiditis
Best management: IV antibiotics + myringotomy ± mastoidectomy if abscess
Frequently Asked Questions (FAQs) in Viva
- What is the most specific sign of acute otitis media? Bulging of the tympanic membrane is the most specific otoscopic sign.
- Can AOM be treated without antibiotics? Yes, mild AOM in selected children can be observed for 48–72 hours with analgesics.
- What is the first-line antibiotic for AOM? High-dose amoxicillin (80–90 mg/kg/day) is the first-line antibiotic.
- How is AOM different from OME? AOM has acute pain and inflammation, while OME has effusion without fever or otalgia.
- When should ceftriaxone be used in AOM? Ceftriaxone is used in treatment failure after 48–72 hours or severe resistant infection.
- What is recurrent AOM? Recurrent AOM means ≥3 episodes in 6 months or ≥4 episodes in 12 months.
- What is the most common complication of AOM? Acute mastoiditis is the most common intratemporal complication.
———— End ————
Download full PDF Link:
Download PPT
Acute Suppurative Otitis Media Best PPT Notes Lectures Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: ASOM in children, Suppurative otitis media treatment guidelines, Acute otitis media complications, Bacterial causes of ASOM, ASOM management in adults, Understanding Acute Suppurative Otitis Media in Children: Symptoms and Treatment, Comprehensive Guide to Suppurative Otitis Media Treatment Guidelines, Exploring the Complications of Acute Otitis Media: What You Need to Know, Identifying Bacterial Causes of Acute Suppurative Otitis Media, Effective Management Strategies for ASOM in Adults, ASOM, case presentation, Earache in children, Cartwheel appearance, Lighthouse effect, ASOM, CSOM, Acute chronic suppurative otitis media.
Very nice
Thanks
Clear ,crisp , clinically relevant text
Clear and clinically relevant text
This book for ENT is genuinely one of the most student-friendly resources I’ve come across. The way concepts are broken down into simple, structured notes makes even the more complex topics easy to grasp and retain. What stands out the most is the teacher’s clarity of thought—every topic feels well-organized, concise, and exam-oriented without losing conceptual depth. It reflects not just strong subject knowledge but also a deep understanding of what students actually need. Truly a great effort in making ENT approachable and less overwhelming.