Examination of Neck. Initial evaluation and examination of neck is very important in patient’s having head and neck cancer. Examination of regional lymph nodes is prognostically important and must be assessed for each patient and tumour. It helps in staging the disease and planning the appropriate management strategy.
Lymph nodes are described as ipsilateral, bilateral, contralateral or midline. Midline nodes are considered ipsilateral nodes, except for thyroid cancers. Direct extension of the primary tumour into lymph nodes is described as lymph node metastasis.
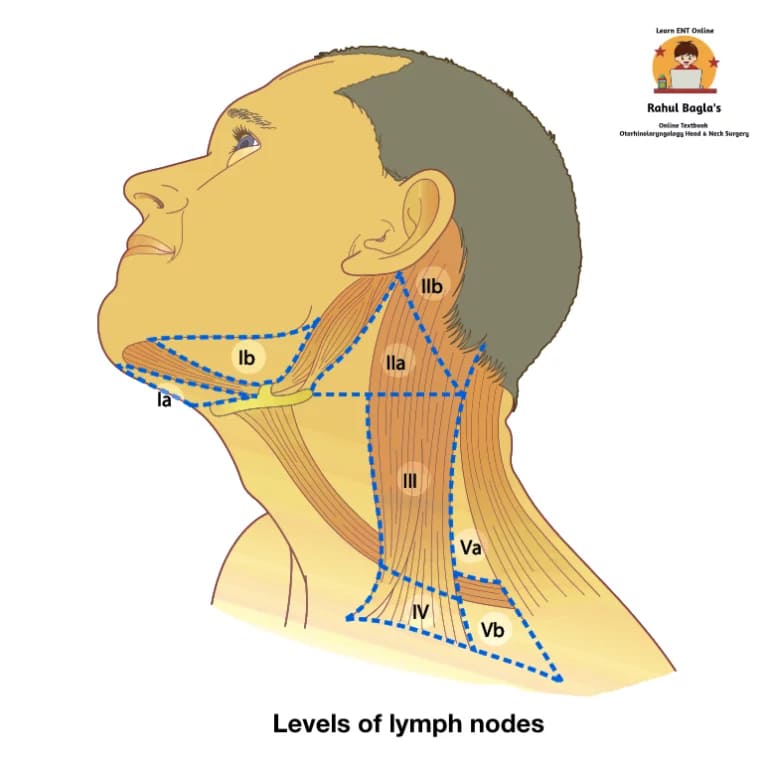
Classification of levels of lymph nodes.
It aims to differentiate nodal areas that drain the visceral structures of the head and neck.
| Level | Group of lymph nodes | Nodal areas |
| IA | Submental lymph nodes | Nodal area is located in single midline zone, corresponding to the submental triangle. – Laterally. Anterior belly of digastric muscles – Inferiorly. Hyoid bone – Superiorly. Mandible. |
| IB | Submandibular lymph nodes | Nodal area is located in submandibular triangle. – Superiorly. Lower border of body of mandible and its projection to the mastoid process. – Posteriorly. Posterior belly of digastric and by stylohyoid muscles. – Anteriorly. Anterior belly of digastric muscle. |
| II | Upper jugular lymph nodes | Nodal area extends from – Superiorly. Skull base. – Inferiorly. Inferior border of the Hyoid bone. The vertical plane defined by the spinal accessory nerve divides level II into IIA, (Caudal to the spinal accessory nerve) and IIB, (Cranial to the spinal accessory nerve). Level IIB is also known as Suárez’s triangle. |
| III | Middle jugular lymph nodes | Nodal area extends from – Superiorly. Inferior border of the Hyoid bone. – Inferiorly. Inferior border of the cricoid cartilage. |
| IV | Lower jugular lymph nodes | Nodal area extends from – Superiorly. Inferior border of the cricoid cartilage. – Inferiorly. Clavicle. |
| VA | Spinal accessory chain lymph nodes | Nodal area is located in upper part of posterior triangle. – Anteriorly. Posterior border of the sternocleidomastoid muscle. – Posteriorly. Anterior border of the trapezius – Inferiorly. Imaginary horizontal line from the inferior border of the cricoid cartilage. (Level V is subdivided into Va and Vb by an imaginary horizontal line at the level of the inferior border of the cricoid cartilage.) |
| VB | Transverse cervical chain lymph nodes | Nodal area is located in lower part of posterior triangle. – Superiorly. Imaginary horizontal line from the inferior border of the cricoid cartilage. – Inferiorly. Clavicle. |
| VI | Anterior cervical lymph nodes | It is single midline nodal area which extends from – Laterally. Medial aspect of the common carotid arteries. – Superiorly. Inferior border of the hyoid bone. – Inferiorly. Innominate artery and suprasternal notch. |
| VII | Superior mediastinal lymph nodes |
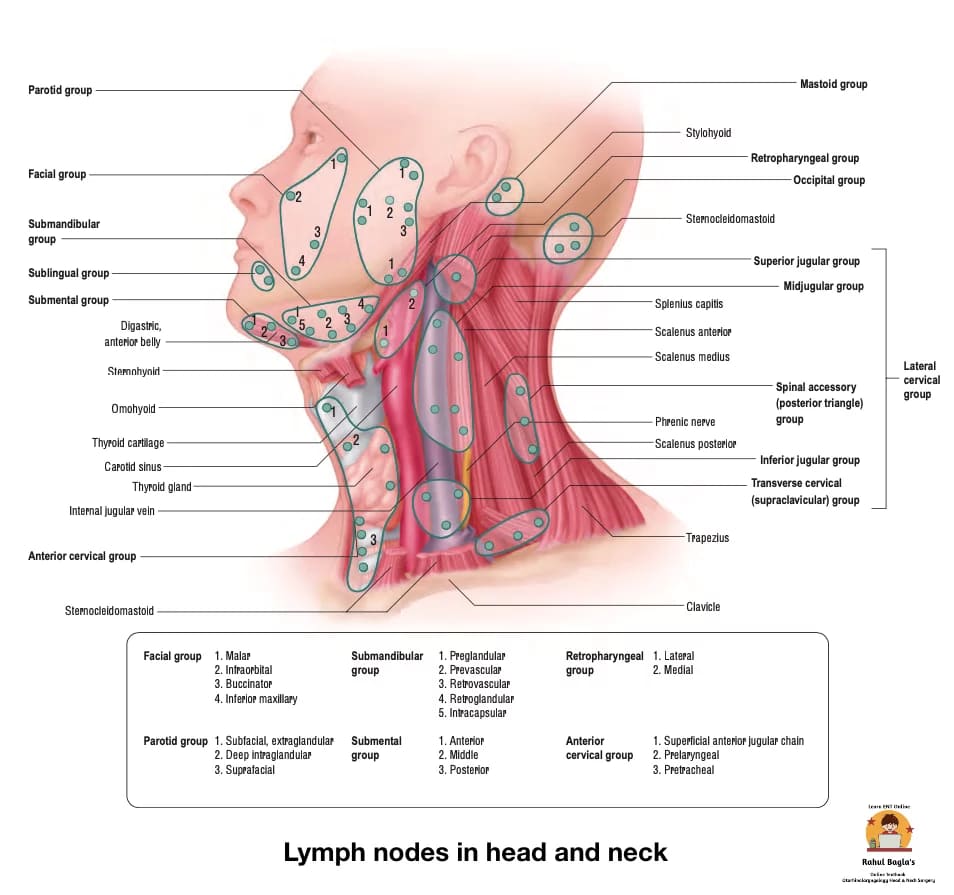
Classification of lymph nodes in head and neck
| Upper horizontal chain of nodes | Submental, Submandibular, Parotid, Postauricular (mastoid), Occipital, Facial lymph nodes. |
| Lateral cervical nodes. | They include nodes, superficial and deep to sternocleidomastoid muscle and in the posterior triangle. a. Superficial external jugular group b. Deep group 1. Internal jugular chain (upper, middle and lower groups) 2. Spinal accessory chain 3. Transverse cervical chain |
| Anterior cervical nodes | 1. Anterior jugular chain 2. Juxtavisceral chain a. Prelaryngeal b. Pretracheal c. Paratracheal |
Lymphatic drainage occurs from superficial lymphatics to deep lymphatics and then from cephalic to caudal direction. It follows somewhat predictable pattern of lymphatic spread and drainage is usually site specific in untreated patient. Therefore nodal area or level involved can help to predict the primary site in cases of unknown primary.
(i) Nodes of Upper Horizontal Chain
- Submental nodes. They lie on the mylohyoid muscle in the submental triangle, 2–8 in number. Afferents come from the chin, middle part of lower lip, anterior gums, anterior floor of mouth and tip of tongue. Efferents go to submandibular nodes and internal jugular chain.
- Submandibular nodes. They lie in submandibular triangle in relation to submandibular gland and facial artery. Afferents come from lateral part of the lower lip, upper lip, cheek, nasal vestibule and anterior part of nasal cavity, gums, teeth, medial canthus, soft palate, anterior pillar, anterior part of tongue, submandibular and sublingual salivary glands and floor of mouth. Efferents go to internal jugular chain.
- Parotid nodes. They lie in relation to the parotid salivary gland and are extraglandular and intraglandular. Preauricular and infraauricular nodes are part of the extraglandular group. Afferents come from the scalp, pinna, external auditory canal, face, buccal mucosa. Efferents go to internal jugular or external jugular chain.
- Postauricular nodes (mastoid nodes). They lie behind the pinna over the mastoid. Afferents come from the scalp, posterior surface of pinna and skin of mastoid. Efferents drain into infra-auricular nodes and into internal jugular chain.
- Occipital nodes. They lie both superficial and deep to splenius capitus at the apex of the posterior triangle. Afferents come from scalp, skin of upper neck. Efferents drain into upper accessory chain of nodes.
- Facial nodes. They lie along facial vessels and are grouped according to their location. They are midmandibular, buccinator, infraorbital and malar (near outer canthus) nodes. Afferents come from upper and lower lids, nose, lips and cheek. Efferents drain into submandibular nodes.
(ii) Lateral Cervical Nodes.
They are divided into:
(a) Superficial lymphatics group. They drain the skin and perforate the investing layer of deep cervical fascia to drain into the deep lymphatics system. It lies along external jugular vein and drains into internal jugular and transverse cervical nodes. Malignant lymph nodes invade the skin requiring skin resection to ensure complete excision.
(b) Deep lymphatics group. The deep lymphatics group lies in proximity to the vessels, nerves and muscles of the neck. More than 80% of lymph nodes in the neck are closely related to the IJV. It is divided into three chains: internal jugular chain, spinal accessory chain and transverse cervical chain.
- Internal jugular chain. Lymph nodes of internal jugular chain lie anterior, lateral and posterior to internal jugular vein and extend from the digastric muscle to the junction of internal jugular vein with the subclavian vein. They are arbitrarily divided into upper, middle and lower groups. Upper group (jugulodigastric node) drains oral cavity, oropharynx, nasopharynx, hypopharynx, larynx and parotid. Middle group drains hypopharynx, larynx, thyroid, oral cavity, oropharynx. Lower jugular group drains larynx, thyroid and cervical oesophagus.
- Spinal accessory chain. It lies along the spinal accessory nerve. Upper nodes of this chain coalesce with upper jugular nodes. Spinal accessory chain drains the scalp, skin of the neck, the nasopharynx, occipital and postauricular nodes. Efferents from this chain drain into transverse cervical chain.
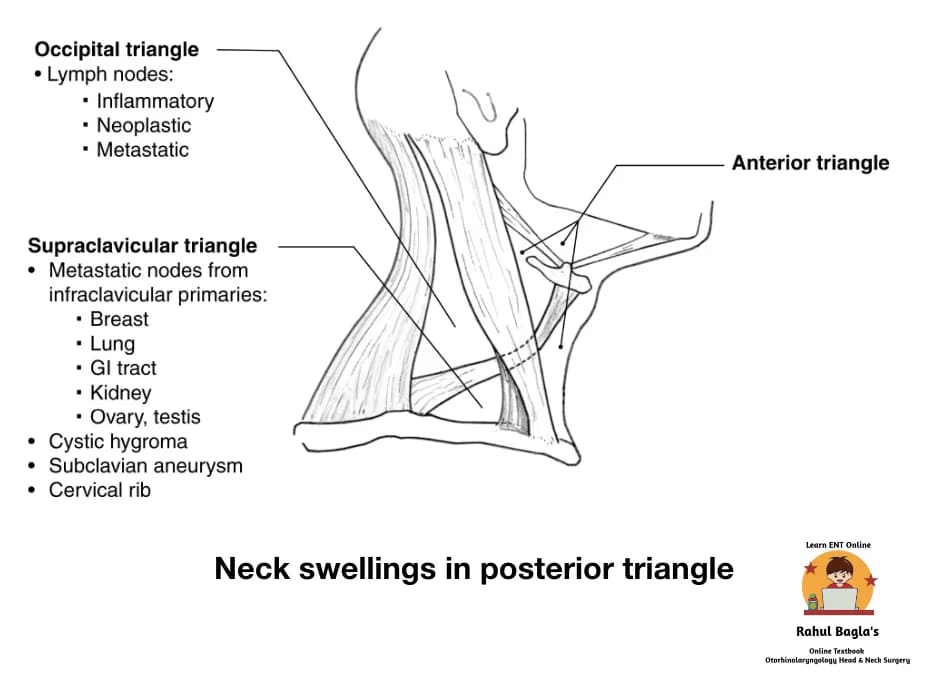
- Transverse cervical chain (supraclavicular nodes). It lies horizontally, along the transverse cervical vessels, in the lower part of the posterior triangle. The medial nodes of the group are called scalene nodes. Afferents to those nodes come from the accessory chain and also infraclavicular structures, e.g. breast, lung, stomach, colon, ovary and testis.
(iii) Anterior Cervical Nodes.
They lie between the two carotids and below the level of hyoid bone and consist of two chains:
(a) Anterior jugular chain. It lies along anterior jugular vein and drains the skin of anterior neck.
(b) Juxtavisceral chain. It consists of prelaryngeal, pretracheal, and paratracheal nodes.
- Prelaryngeal node (Delphian node) lies on cricothyroid membrane and drains subglottic region of larynx and pyriform sinuses.
- Pretracheal nodes lie in front of the trachea, deep to pretracheal fascia, and drain thyroid gland and the trachea. Efferents from these nodes go to paratracheal, lower internal jugular and anterior mediastinal nodes.
- Paratracheal nodes (recurrent nerve chain) lie along recurrent laryngeal nerve and drain the thyroid lobes, subglottic larynx, trachea and cervical oesophagus.
Lymph Nodes Not Clinically Palpable
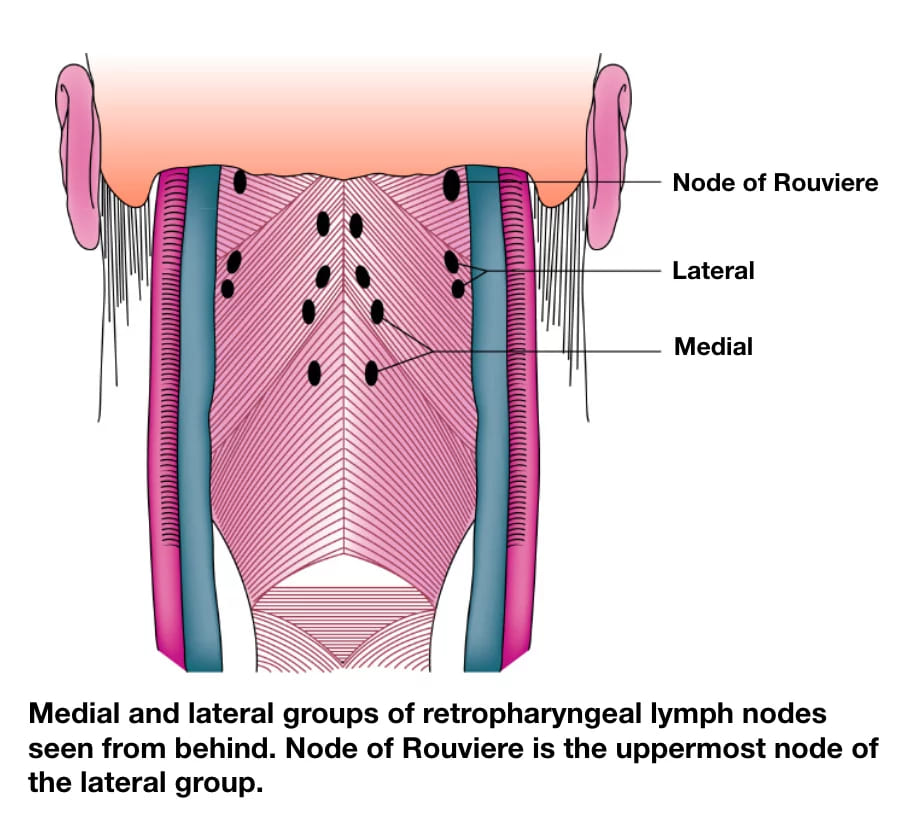
(a) Retropharyngeal nodes. They lie behind the pharynx and are divided into lateral and medial groups. Lateral group lies at the level of atlas, close to the base of skull. Most superior node of the lateral group is called node of Rouviere. Medial group lies near the midline but at a little lower level. Retropharyngeal nodes drain the nasal cavity, parana- sal sinuses, hard and soft palate, nasopharynx, posterior wall of the pharynx and send efferents to the upper inter- nal jugular group.
(b) Sublingual nodes. They lie deep along the lingual vessels and drain anterior part of the floor of mouth and ventral surface of tongue. Lymphatics from these nodes end in the submandibular or upper jugular nodes.
Examination of neck.
Examination is done to find out clinically enlarged lymph nodes. During examination of neck nodes, clinician stands behind the patient. Neck of the patient is slightly flexed towards the side of examination to achieve relaxation of muscles. Palpation is done in a systematic manner to include all lymph node groups and triangles of the neck.
Procedure of examination of lymph nodes.
- Remove patient’s clothes till the shoulders.
- Level V nodes. They lie between the skin and muscles of the floor of the posterior triangle and therefore palpation is done by rolling movement between skin and muscles. Gentle lateral movement of the head to the examined side helps in examination.
- Level II – IV nodes. About 80 percent of the nodes lie under the sternocleidomastoid muscle within the jugular chain. Palpation is done by placing fingers in front of and medial to the muscle with the thumb behind it, thus forming a ‘C’ around the muscle.
- Level VI nodes. Palpate suprasternal notch and the space within it (the space of Burns). Trachea should also be palpated for any restricted movement or pain which may indicate invasion of postcricoid carcinoma.
- Level I nodes. Now palpate the submandibular gland and nodes along with the submental nodes. Submandibular nodes (level Ib) lie in submandibular triangle in relation to submandibular gland and facial artery. Submental nodes (level Ia) lie on the mylohyoid muscle in the submental triangle. From the posterior border of the submandibular gland, the examination is continued upwards towards the face to assess the preauricular and facial nodes.
When a node or nodes are palpable, look for the following points:
- Location and number of nodes.
- Size of nodes.
- Discrete or matted nodes.
- Consistency. Metastatic nodes are hard; lymphoma nodes are firm and rubbery; hyperplastic nodes are soft. Nodes of metastatic melanoma are also soft.
- Tenderness. Inflammatory nodes are tender.
- Fixity to overlying skin or deeper structures. Mobility should be checked both in the vertical and horizontal planes.
Fine needle aspiration cytology (FNAC) is done in patients with cervical lymphadenopathy. It is a safe procedure with almost no cell seeding reports. Ultrasound-guided fine needle biopsy can be done if neck mass is not easily palpable.
Radiology. It provides vital information about the primary tumour, neck nodes and distant metastases. It helps in accurate staging of the extent and spread of disease. Combination of CT, MRI or PET-scan are the mainstay radiological investigations in the pre-operative work up of patients with head and neck cancer.
Role of radiological investigations.
- Site and extent of the primary lesion.
- Size of the primary lesion.
- Neck node involvement (number of nodes, size, position, fixation).
- Distant metastases.
- Detection of synchronous primary tumours.
- Confirmation of diagnosis.
- Baseline and postoperative assessment in tumours that have a high risk of recurrence or recur slowly, i.e. adenoid cystic carcinoma.
Differential diagnosis of neck swellings may be present during palpation.
| Lymph node group | Differential diagnosis |
| IA (Submental) | Lymph node, Thyroglossal cyst, Dermoid cyst, Plunging ranula. |
| IB (Submandibular) | Submandibular gland pathology, Lymph node, Cystic hygroma / lymphangioma (both can affect the entire neck) |
| II (Upper jugular) | Lymph node, Parotid gland pathology, Branchial cyst Parapharyngeal pathology (e.g. Paragangliomata or nerve sheath tumours) |
| III (Mid jugular) | Lymph node, Branchial cyst, Parapharyngeal pathology, Laryngocoele |
| IV (Lower jugular) | Lymph node (including Virchow’s node on the left) |
| V (Posterior triangle) | Lymph node, Lipoma, Cervical rib |
| VI (Anterior compartment) | Thyroid gland pathology, Thyroglossal cyst, Parathyroid neoplasm, Lymph node, Direct extension of a laryngeal neoplasm |
——– End of the chapter ——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
Please read. Glomus Tumour. https://www.entlecture.com/glomus-tumour/
Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
Join our Facebook group:
Great job Dr. Rahul! I am an Otolaryngology resident in Makerere University, Kampala, Uganda. I am glad to have landed on your notes because they are easy to read and comprehend. Bravo.
I am still reading through as I am particularly looking for notes on Fascia and fascial spaces of the neck. I would be honoured to hear from you and to learn from you. Thank you
Hello Dr. Ronata! 😊
Thank you so much for your kind words. I’m so glad to hear that the book have been helpful for you. It’s always wonderful to connect with fellow ENT residents from across the globe, especially from such a respected institution like Makerere University!
I’d be more than happy to share insights on Fascia and fascial spaces of the neck. I’ll make sure to put together something clear and concise very soon.
Please feel free to reach out anytime. Wishing you all the very best in your residency journey!
Warm regards,
Dr. Rahul Bagla
Sir we are unable to download in pdf