|
The following CBME core competencies are covered in this chapter.
|
Vestibular Function Tests
Introduction
The central nervous system receives sensory input from three major systems:
- Vestibular system (inner ear)
- Visual system (eyes)
- Proprioceptive system (body position sense)
The brain integrates these inputs and maintains equilibrium and posture by coordinating movements of the eyes, head, and body. The equilibrium system functions like a two-sided push–pull mechanism, where both labyrinths maintain equal tonic activity in the neutral state. Therefore, any disruption in vestibular, visual, or proprioceptive input—due to trauma, disease, or degeneration—can produce dizziness, imbalance, or vertigo.
Classification of Vestibular Function Tests
Vestibular function tests are broadly divided into two groups:
- Clinical tests (Bedside Examination): These are simple, quick tests performed in the clinic without specialised equipment.
- Laboratory Tests (Instrumental Evaluation): These are quantitative tests performed using specialised equipment to measure vestibular responses and analyse vestibular function objectively.
Table: Vestibular Function Tests
| Type | Section | Tests |
| Clinical tests (Bedside Examination) | A. Tests for Spontaneous & Gaze-evoked Nystagmus | 1. Spontaneous Nystagmus |
| B. Positional Tests | 2. Dix-Hallpike Manoeuvre (Positional Test) | |
| C. Tests for Fistula | 3. Fistula Test | |
| D. Tests for Static & Dynamic Balance | 4. Romberg’s Test and Sharpened Romberg Test 5. Gait Test 6. Tandem Gait Test 7. Unterberger Stepping Test (Fukuda Stepping Test) 8. Past-pointing Test (Pointing Test) |
|
| Laboratory Tests (Instrumental Evaluation) | A. Semicircular Canal Function Tests | 1. Video Head Impulse Test (vHIT) 2. Caloric Test 3. Rotational Test |
| B. Otolith Function Tests | 4. Vestibular Evoked Myogenic Potentials (VEMPs) – cVEMP and oVEMP | |
| C. Eye Movement Recording Systems | 5. Videonystagmography (VNG) / Electronystagmography (ENG) 6. Optokinetic Test |
|
| D. Global Balance Assessment | 7. Posturography (Dynamic Posturography) | |
| E. Historical / Obsolete Tests | 8. Cupulometry 9. Galvanic Test |
Clinical Tests (Bedside Examination)
1. Spontaneous Nystagmus
Nystagmus is an important tell-tale sign in the evaluation of vestibular function. Nystagmus is defined as a rhythmical, involuntary, oscillatory movement of the eyes without a cognitive, visual or vestibular stimulus.
The direction of nystagmus may be:
- Horizontal
- Vertical
- Rotatory (torsional)
Generally, horizontal canal lesions produce horizontal nystagmus, superior (anterior) canal lesions cause rotatory nystagmus, and posterior canal lesions lead to torsional-upbeat nystagmus.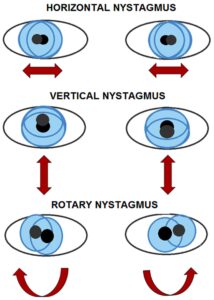
Diagram: Types of Nystagmus
Mechanism of Vestibular Nystagmus
Vestibular nystagmus comprises two distinct components or phases: a slow phase and a fast phase. The slow phase is due to the abnormality in the vestibular system, while the fast phase is due to the corrective central mechanism that brings the eyes back to the primary position. However, while only the slow phase plays a part in image stabilisation, it is the fast phase that is actually detected, and hence by convention, the direction of the nystagmus is attributed to that of its fast phase.
For example, in acute right-sided vestibular failure, the slow phase is towards the right (the weak side), but the fast phase will be to the left, thus causing left-beating nystagmus. However, crucial for interpretation, the patient’s past-pointing and falling will still occur towards the slow component, indicating the side of vestibular weakness (i.e., towards the right in this example).
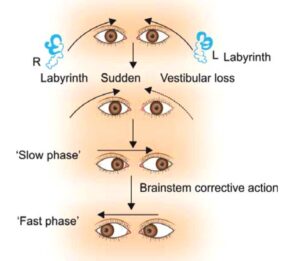
Diagram: Showing the mechanism of nystagmus
Degree of nystagmus
Intensity of nystagmus is indicated by its degree (Alexander’s law):
| Degree | Description |
| 1st degree | It is a weak nystagmus and is visible only when the patient looks in the direction of the fast phase. |
| 2nd degree | It is stronger than 1st degree and is visible even when the patient looks straight ahead. |
| 3rd degree | It is stronger than the 2nd degree and is visible even when the patient looks in the opposite direction of the fast phase. |
*Note: These degrees may not hold true for nystagmus of central origin.
How to look for nystagmus
Patient sits on the examination chair or lies supine. The clinician keeps his finger about 30 cm centrally in front of the patient’s eyes, moves it in all four directions (up, down, left, right) and asks the patient to follow. The finger should not move beyond 30° from the centre (to avoid physiological gaze-evoked nystagmus). The presence of spontaneous nystagmus strongly suggests an organic lesion. Differentiating its origin (peripheral vs. central) is paramount for diagnosis and management. Use Frenzel glasses (+20 D) to abolish optic fixation – peripheral nystagmus becomes more visible.

Table: Differentiating Peripheral vs. Central Nystagmus
| Feature | Peripheral Nystagmus | Central Nystagmus |
| Lesion Site | Labyrinth or CN VIII | Central pathways (vestibular nuclei, brainstem, cerebellum) |
| Fatiguability | Fatiguable (decreases with repeated testing) | Non-fatiguable |
| Reproducibility | Reproducible | Variable/inconsistent |
| Optic Fixation | Suppressed by fixation; enhanced with Frenzel | Not suppressed |
| Direction | Unidirectional; horizontal or horizontal-rotatory | Multidirectional; vertical, pure torsional, or gaze-changing |
| Associated Symptoms | Severe vertigo, nausea, vomiting, hearing loss, tinnitus | Milder vertigo; often with neurological signs (ataxia, diplopia, dysarthria) |
| Specific Patterns | Irritative lesions → nystagmus towards lesion side; Paretic lesions → nystagmus towards healthy side | Downbeat (craniocervical junction), Upbeat (pons/medulla), Pendular (congenital, MS), Disconjugate |
2. Dix-Hallipke Manoeuvre (Positional Test)
This manoeuvre is critical for diagnosing Benign Paroxysmal Positional Vertigo (BPPV) and differentiating peripheral from central positional vertigo. This test should be conducted when the patient complains of vertigo provoked by specific head–neck movements or in certain head positions. Typical symptoms are brief, intense spells of rotatory vertigo which usually precipitate during an abrupt change in head position (e.g., getting out of bed, turning over in bed, bending over, looking up or when extending or flexing the neck).
The Dix-Hallpike test is done to elicit vertigo, and the patient should be informed and warned. Careful examination of the patient’s eyes is essential during the test. It also helps to differentiate a peripheral from a central lesion.
Method
- Patient sits on the examination couch with legs extended.
- The examiner holds the patient’s head, turns it 45° horizontally to one side.
- Patient keeps eyes open and fixes gaze on the examiner’s nose/bridge.
- Rapidly guide the patient into the supine position with the head hanging 30° below horizontal.
- Keep the head-down position for 20–30 seconds, observe for nystagmus and ask about vertigo.
- Return the patient to sitting, allow recovery, then repeat with the head turned to the opposite side.
- If both sides are negative, perform with head straight-hanging (testing the superior semicircular canals, though BPPV commonly affects the posterior canal).

Four parameters of nystagmus are observed
It helps to differentiate peripheral (typically BPPV) from central positional nystagmus:
- Latency: The delay between assuming the provocative position and the onset of nystagmus/vertigo.
- Duration: How long does the nystagmus and vertigo last?
- Direction: The characteristic beating pattern of the nystagmus.
- Fatiguability: Whether the nystagmus and vertigo diminish with repeated testing in the same position.
Table: Differentiating Peripheral vs. Central Positional Nystagmus (Dix-Hallpike Findings).
| Feature | Peripheral | Central |
| Latency | 2–20 s | No latency (immediate onset) |
| Duration | Less than 1 min | More than 1 min |
| Direction of nystagmus | Direction fixed, towards the undermost ear | Direction changing |
| Fatiguability | Fatiguable (decreases or disappears with repeated testing in the same position) | Non-fatiguable (persists with repeated testing) |
| Accompanying symptoms | Severe vertigo | None or slight |
| Intensity of vertigo | Severe | Mild |
| Incidence | Common | Rare |
| Reproducibility | Reproducible but fatigues | Persistent and reproducible |
*Horizontal Canal BPPV – If history strongly suggests BPPV but Dix-Hallpike is negative, perform the Supine Roll Test. (supine, head turned 90° left/right) – look for geotropic or apogeotropic nystagmus.
3. Fistula test (Abnormal Middle-Inner Ear Communication)
The fistula test identifies an abnormal communication (fistula) between the middle and inner ear. Normally, pressure changes in the external ear canal do not transmit to the labyrinth.
Principle
If a fistula exists, pressure changes applied to the external auditory canal transmit to the labyrinth, stimulating it and inducing nystagmus and vertigo.
Method
The test is performed by applying intermittent pressure on the tragus or by using Siegel’s speculum, in order to produce pressure changes in the ear canal. If there is an abnormal communication between the middle and inner ear, the pressure changes are transmitted to the labyrinth. Stimulation of the labyrinth results in nystagmus and vertigo. The direction of nystagmus may vary depending on canal stimulation and pressure/negative pressure. Therefore, the key point is the presence of induced nystagmus and vertigo.
Interpretations
| Result | Meaning | Causes/Notes |
| Negative fistula test | No fistula | 1. Normally, the pressure changes in the external auditory canal cannot be transmitted to the labyrinth. 2. When the labyrinth is dead (non-functioning), no nystagmus will be elicited even with a fistula. |
| Positive fistula test | Fistula is present | 1. Erosion of the horizontal (lateral) semi-circular canal (e.g., due to cholesteatoma) or a surgically created window in the horizontal semi-circular canal (e.g., following fenestration operation). 2. Abnormal opening in the oval window (post-stapedectomy fistula) or the round window (rupture of the round window membrane). 3. In another way, a Positive fistula also implies that the labyrinth is still functioning. |
| False negative fistula test | Negative fistula test, but fistula is present | It is seen when a fistula is there but is covered by cholesteatoma or granulation tissue and does not allow pressure changes to be transmitted to the labyrinth. |
| False positive fistula test (Hennebert’s Sign) | Positive fistula test without the presence of a fistula | 1. Congenital syphilis. The annular ligament is lax and mobile, causing the stapes footplate to be hypermobile. 2. 25% cases of Meniere’s disease. It is due to the fibrous bands connecting the utricular macula to the stapes footplate. |
Tullio’s Phenomenon: This refers to giddiness or vertigo produced by loud noise rather than pressure. It is typically associated with labyrinthine fistula, superior canal dehiscence syndrome and post-fenestration surgery.
4. Romberg’s Test and Sharpened Romberg Test
These tests assess static balance by challenging proprioceptive and vestibular inputs, especially when visual input is removed.
Method
- The patient removes shoes and stands with feet together, arms by their side. The examiner must stand close by for safety.
- First, the patient stands quietly with eyes open. This allows visual compensation.
- Then, the patient stands with eyes closed. With visual input lost, the vestibular and proprioceptive systems are put to a greater test.
- If the patient can perform this without significant sway, proceed to the Sharpened Romberg Test: The patient stands in a heel-to-toe position (tandem stance), with one foot directly in front of the other. Arms are folded across the chest.
Interpretations
- Peripheral Vestibular Lesions: The patient sways and tends to fall towards the side of the lesion, especially with eyes closed. Inability to perform the sharpened Romberg test strongly indicates vestibular impairment.
- Central Vestibular Disorders: Patients often exhibit swaying or instability even with their eyes open, indicating a more profound and often multisensory balance deficit.
- A “wooden soldier” fall (straight backward without correction) is frequently non-organic or psychogenic.
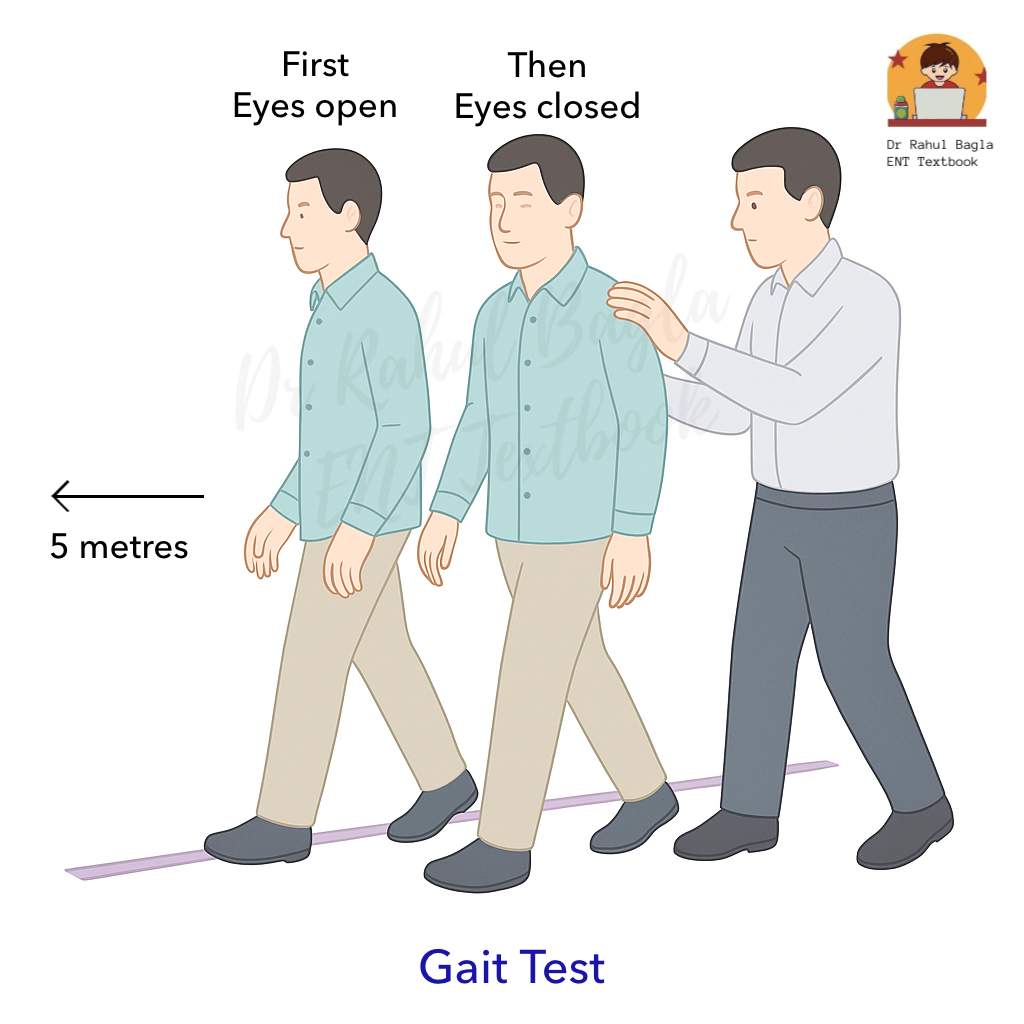
5. Gait Test
Method
The patient is asked to walk along a straight line in normal speed for 5 metres to a fixed point, first with eyes open and then closed. The examiner walks alongside to prevent the person from falling over and hurting himself.
Interpretation
In the case of recent vestibular hypofunction, with eyes closed, the patient tends to deviate to the affected side.
6. Tandem Gait Test
Method
The patient is asked to take 10 heel-to-toe steps in a straight line at normal speed with arms folded on the chest, first with eyes open and then closed. The examiner walks alongside the patient for safety reasons and looks out for deviation towards the side of the lesion.
With the eyes open, this primarily tests cerebellar function as the visual components compensate for chronic vestibular and proprioceptive deficits. However, tandem walking with closed eyes is a good test of vestibular function, assuming that the visual and proprioceptive functions are intact.
Interpretation
- Peripheral Vertigo: Patients may exhibit some impaired balance but can usually still walk.
- Central Vertigo: Patients with central lesions often cannot walk or even stand without falling, highlighting a more severe imbalance.
7. Unterberger Stepping Test (Fukuda Stepping Test)
This test identifies the tendency of patients with vestibular imbalance to turn while walking, indicating the side of the lesion.
Method
The patient is asked to march on the spot 50 times with the arms extended and eyes closed. Repetition of the test is essential for consistency.
Interpretation
- Positive test: Rotational movement towards the side of the lesion by >30–45° or displacement forward/backward >50 cm.
- Unilateral paralytic labyrinthitis: Rotates to the side of the lesion.
- Irritative lesions (e.g., early Ménière’s): May rotate away from the lesion side or be unable to perform the test.
8. Past-pointing Test
Past pointing means the movement of a pointing finger that goes beyond the intended mark. This is called overshooting and is a manifestation of dysmetria (inability to control the range of motion).
Method
The patient stands in front of the clinician. The clinician extends his arms and points both of his index fingers approximately 15cm (6 inches) apart. The patient is asked to lift both arms over the head and then bring the arms down to touch his index fingers to the clinician’s index fingers.
Interpretation
- Normally, the patient can perform the test without difficulty.
- Vestibular Disease: Patients have difficulty lining up with the clinician’s fingers and will consistently “past-point” (overshoot) towards the side of the vestibular lesion.
- Clinical Correlation: Importantly, the direction of past-pointing, falling during Romberg, the slow component of nystagmus, and the turn in the Unterberger test all point towards the side of the vestibular lesion.
Laboratory Tests for Vestibular Functions
These tests help confirm diagnosis and allow objective, quantitative evaluation of peripheral vestibular function and the vestibular-ocular reflex.
1. Video Head Impulse Test (vHIT)
Principle
vHIT tests the vestibulo-ocular reflex using rapid, unpredictable head impulses (150–200°/s). Infrared camera goggles record eye movement.
Normal gain is approximately 0.8–1.2.
Corrective saccades indicate abnormal vestibular function:
- Overt saccades (visible after impulse)
- Covert saccades (occur during impulse)
Method
- Patient fixates on a target 1.5 m away.
- Examiner gives unpredictable, small-amplitude, high-velocity head turns in the horizontal plane, then vertical planes (for anterior and posterior canals).
- vHIT goggles record head and eye movements.
Interpretation
- Low gain with corrective saccades → ipsilateral semicircular canal dysfunction (horizontal, anterior, or posterior – individually testable).
- Bilateral low gain → bilateral vestibulopathy.
- Normal gain but saccades (especially covert) → partial deficit.
- Normal vHIT in acute vestibular syndrome → suggests central cause (e.g., posterior circulation stroke) – this is part of the HINTS examination.
Advantages over caloric
Tests high-frequency range (2–5 Hz) – more physiological; tests all six semicircular canals individually; not affected by TM perforation; portable systems allow bedside use.
2. Caloric Test
The caloric test checks how well each ear’s balance system (labyrinth) is working by making changes in temperature in the external auditory canal through hot or cold water. The caloric test induces nystagmus (involuntary eye movements). The advantage of the test is that it evaluates each ear separately, unlike rotational tests (which test both ears together). If the induced vertigo is similar to one patient’s experience, it proves the labyrinthine origin of vertigo. However, some patients may not tolerate the induced vertigo and discomfort.
Principle
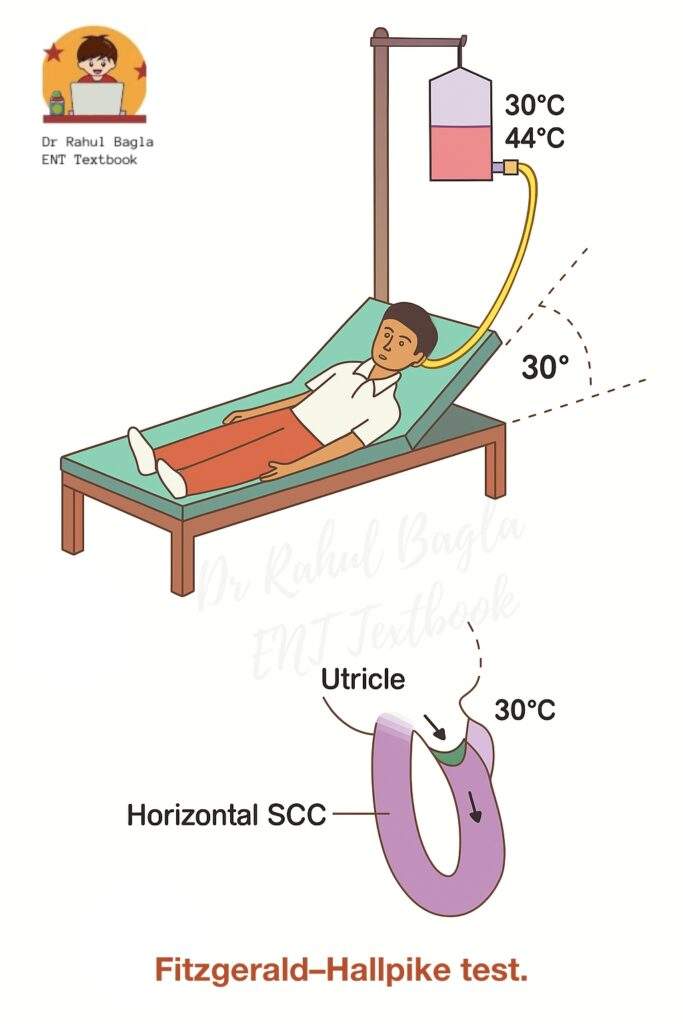
Irrigation with water at 30 or 44°C (37 ± 7°C) for 40 seconds is the standard procedure. A 5-minute interval between consecutive irrigations allows the temporal bone temperature to normalize.
- Hot Water (44°C): Heats the endolymph in the horizontal semicircular canal. The heated endolymph becomes less dense, rises, and creates a flow towards the ampulla, deflecting the cupula. This simulates a head rotation to the irrigated side (same side), producing nystagmus with the fast phase to the irrigated side.
- Cold Water (30°C): Cools the endolymph, making it denser. It sinks, creating a flow away from the ampulla. This simulates a head rotation to the opposite side, producing nystagmus with the fast phase to the opposite side.
Mnemonic: COWS (Cold Opposite, Warm Same)
- Cold water/air induces nystagmus with a fast phase to the Opposite side.
- Warm water/air induces nystagmus with a fast phase to the Same side.
Methods
The caloric test is typically performed using one of three primary methods.
- Modified Kobrak Test
- Fitzgerald-Hallpike Bi-thermal Caloric Test
- Cold-air Caloric (Dundas Grant’s) Test.
A. Modified Kobrak Test (Quick Office Procedure)
The Modified Kobrak Method is a quick in-office procedure that precisely controls temperature to stimulate the ear, typically using a small volume of water or air for a localised effect.
Method.
- The patient sits with their head tilted 60 degrees backwards. This position places the horizontal semicircular canal in a vertical orientation.
- The ear is irrigated with ice water for 60 seconds, starting with a small volume and gradually increasing it if there’s no response:
- Begin with 5 mL of ice water.
- If no response, increase to 10 mL, then 20 mL, and finally 40 mL.
Interpretation.
- Normal Response: A normal response is the presence of nystagmus (involuntary eye movements) beating toward the opposite ear when 5 mL of ice water is used.
- Hypoactive Labyrinth: If nystagmus is only observed with increased volumes of water (between 5 mL and 40 mL), it suggests the labyrinth (inner ear balance organ) is hypoactive (underactive).
- Dead Labyrinth: If there is no nystagmus even after irrigating with 40 mL of ice water, it indicates a dead labyrinth.
B. Fitzgerald-Hallpike Bi-thermal Caloric Test:
Method.
- The patient reclines on the couch at 30 degrees (so that horizontal SCC comes in a vertical position).
- Examine both ears for wax or tympanic membrane (TM) perforations. (If TM is perforated, use air instead of water).
- Alternatively, irrigate each ear with water at 30°C and 44°C for 40 seconds.
- Observe and record the nystagmus (duration, amplitude, frequency) using electronystagmography (ENG) or videonystagmography (VNG). The total time is recorded from the start of irrigation to the end of nystagmus and charted on a calorigram.
- If no nystagmus is elicited, repeat the test with 20°C water for 4 minutes before concluding a “dead labyrinth.”
Interpretations (Most Common Findings): Both canal paresis and directional preponderance must be greater than 15-20% to be clinically significant.
- Canal Paresis (CP): One ear is weaker
- Definition: The response (measured as nystagmus duration) to both cold & warm is much less on one side than on the opposite side. It reflects the weak function of the ipsilateral labyrinth, vestibular nerve, or vestibular nuclei.
- Calculation: [(RC + RW) – (LC + LW)]
% CP = _____________________________________ x 100
(RC + RW + LC + LW)
where R/L = Right/Left ear, C/W = Cold/Warm irrigation response). - Commonly seen in Meniere’s disease, vestibular schwannoma, post-labyrinthectomy, or vestibular nerve section.
- Directional Preponderance (DP): Nystagmus is stronger in one direction
- Definition: The total duration of nystagmus beating in one direction is significantly greater than the nystagmus beating in the opposite direction.
- Calculation: [(RW + LC) – (LW + RC)]
% DP = ____________________________________ x 100
(RC + RW + LC + LW)
(where R/L = Right/Left ear, C/W = Cold/Warm irrigation response for respective beating direction). - Clinical Significance: This can be seen in both central and peripheral lesions. DP towards the side of a central lesion, and away from the side of a peripheral lesion (due to an irritative lesion). Further investigations (e.g., BERA, CT/MRI) are required for differentiation and localisation. If nystagmus is 25–30% or more on one side, it indicates directional preponderance.
- Specific Patterns:
- CP + Contralateral DP: Commonly seen in Meniere’s disease.
- CP + Ipsilateral DP: Often seen in acoustic neuroma.
- No nystagmus at all: Indicates a dead labyrinth or bilateral hypofunction
C. Cold-air Caloric (Dundas Grant’s) Test. Cold air is introduced into the ear by pouring ethyl chloride into the Dundas grant tube, which is a coiled copper tube wrapped in cloth. This test is used when there is a perforation in the eardrum.
3. Rotational Tests
The rotational chair tests horizontal canal VOR. Useful when caloric is contraindicated (TM perforation, children) or to assess bilateral loss.
Method
Patient sits in a motorised, computer-controlled chair (Barany’s revolving chair) with head tilted 30° forward, immobilised. Two modes:
- Sinusoidal rotation (0.05–1 Hz)
- Velocity step (impulsive) – abrupt increase from stationary to 60–90°/s
Nystagmus is recorded via VNG. Both labyrinths are tested simultaneously – cannot lateralise the lesion.
Interpretation
| Response | Disorder |
| Bilateral reduced or absent | Bilateral vestibular failure (ototoxicity, post-meningitis, idiopathic) |
| Asymmetric response or directional preponderance | Unilateral vestibular disorder (less sensitive than caloric) |
| Loss of VOR suppression | Central disorder (cerebellar/brainstem) |
4. Vestibular Evoked Myogenic Potentials (VEMPs)
Principle
Loud clicks or tone bursts (500–1000 Hz, 95–105 dB nHL) stimulate otolith organs, producing a reflex electromyographic response.
| Test | Structure Tested | Nerve | Recording Site | Reflex |
| cVEMP (cervical) | Saccule | Inferior vestibular nerve | Tonically contracted sternocleidomastoid (ipsilateral) | Vestibulo-collic |
| oVEMP (ocular) | Utricle | Superior vestibular nerve | Extraocular muscles – contralateral inferior oblique | Vestibulo-ocular |
Method (cVEMP)
Patient lies supine, head elevated and turned to the opposite side to activate SCM. Surface electrodes on the SCM belly and sternum. Clicks are presented via insert earphones. Response is a positive-negative biphasic waveform (p13-n23).
Interpretation
- Absent/reduced amplitude → Saccule/utricle dysfunction (e.g., Ménière’s, ototoxicity, vestibular neuritis involving inferior/superior nerve)
- Enhanced amplitude (low threshold) → Superior canal dehiscence syndrome or third window lesion
- Prolonged latency → Central involvement (multiple sclerosis, brainstem lesion)
- Interaural amplitude asymmetry ratio >30–40% → Unilateral otolith dysfunction
In Ménière’s disease, cVEMP amplitude may be reduced in late stages but can be enhanced during an acute attack. Combined caloric (horizontal canal) + VEMP (otolith) helps dissect which part of the labyrinth is involved.
5. Videonystagmography (VNG) – replaces ENG
Principle
Infrared cameras record eye movements. Includes multiple subtests:
- Spontaneous & gaze-evoked nystagmus
- Positional & positioning tests (Dix-Hallpike, Roll)
- Optokinetic nystagmus
- Saccade and pursuit testing
- Caloric test (core component)
Electronystagmography (ENG) using electrodes is now obsolete – it cannot record torsional movements and is prone to artefacts.
6. Optokinetic Test
This test diagnoses central lesions.
Principle
Repetitive visual patterns (moving stripes or a striped curtain) induce optokinetic nystagmus – slow phase following the target, fast phase resetting.
Method
Patient looks straight ahead while a drum with vertical stripes moves slowly in both directions. Results are analysed.
Interpretation
- Normal: Nystagmus with a slow component in the direction of moving stripes.
- Abnormal (asymmetric or absent): Brainstem, cerebral, or other central disorders.
7. Posturography (Computerised Dynamic Posturography, CDP)
Principle
Force plate measures body sway under varying sensory conditions (fixed or sway-referenced support and/or visual surround). Quantifies the patient’s ability to use vestibular, visual, and proprioceptive inputs for balance.
Method (Sensory Organisation Test – SOT)
Six conditions progressively eliminate or distort visual and proprioceptive inputs. The “sway-referenced” support moves with the patient’s centre of gravity, removing reliable proprioceptive cues.
Interpretation
- Identifies which sensory system is deficient (vestibular, visual, proprioceptive).
- Vestibular loss pattern: Normal sway with eyes open on fixed support; marked sway when both vision and proprioception are distorted (condition 5 or 6).
- Malingering: Non-physiological patterns (e.g., excessive sway only in easy conditions).
- Uses: Medico-legal documentation, vestibular rehabilitation planning, and monitoring progression.
Limitations
Does not lateralise or identify specific canal/otolith involvement.
8. Cupulometry (Historical)
A technique using graded angular acceleration to test cupula function. Involved measuring the duration of post-rotatory nystagmus after sudden stops from different speeds. No longer used in clinical practice – replaced by rotational chair and vHIT.
9. Galvanic Test (Historical)
A small electrical current (0.5–2 mA) applied behind the ears stimulates the vestibular nerve, producing nystagmus and postural deviation. Abnormally reduced response suggests a nerve lesion. Rarely used now – largely replaced by vHIT and VEMP.
Cerebellar Function Tests
“These tests help differentiate cerebellar ataxia from vestibular imbalance.”
- Asynergia (abnormal finger-nose test). The patient touches the tip of his nose with his forefinger and then touches the clinician’s finger, held within the reach of the outstretched arm of the patient. The test is repeated as fast as the patient can. The position of the clinician’s finger can be changed to make the test more sensitive. Patients having cerebellar dysfunction will not be able to touch the nose on the first attempt (dysmetria). The reason is that intention tremors are more pronounced as the hand approaches the face.
- Dysmetria (inability to control range of motion). i.e. movements are incorrect in range, direction and force. The movements may overshoot their intended mark (hypermetria) or fall short of it (hypometria).
- Adiadochokinesia (inability to perform rapid alternating movements). e.g. supination and pronation of the forearm or patting the palm of one hand to the palm and back of the other hand.
- Rebound phenomenon (inability to control movement of extremity when opposing forceful restraint is suddenly released). When the patient attempts to do a movement against resistance, and if the resistance is suddenly removed, the limb moves forcibly in the direction towards which the effect was made. This is called the rebound phenomenon. It is due to the absence of the breaking action of antagonistic muscles.
———— End of the chapter ————
High-Yield Points for Quick Revision
- Vestibular system maintains balance by integration of vestibular, visual, and proprioceptive input.
- Vestibular system follows a push–pull mechanism; unilateral loss causes spontaneous nystagmus.
- Vestibular nystagmus has slow phase (pathological) and fast phase (corrective).
- Nystagmus direction is named by fast phase, but falling occurs toward slow phase (weak side).
- Peripheral nystagmus is unidirectional and suppressed by fixation; central nystagmus is not suppressed.
- Dix-Hallpike is the gold standard test for posterior canal BPPV.
- Peripheral positional nystagmus shows latency, short duration, and fatiguability.
- Fistula test becomes positive in cholesteatoma erosion of lateral SCC; false positive is Hennebert sign.
- vHIT tests high-frequency vestibular function and all six semicircular canals.
- Caloric test evaluates low-frequency horizontal SCC function and tests each ear separately.
- Caloric test interpretation depends on canal paresis (CP) and directional preponderance (DP).
- Rotational chair tests both labyrinths together and is useful in bilateral vestibular failure.
- VEMP evaluates otolith organs: cVEMP for saccule and oVEMP for utricle.
- Posturography helps in vestibular rehabilitation planning but cannot lateralise lesions.
Practical Tips for Viva and Clinical Exam Scenarios
- Presenting a Case: When presenting a patient with vertigo, always start with the onset, duration, and associated symptoms (hearing loss, tinnitus, neurological deficits). This immediately points towards peripheral vs. central causes. Example Viva Question: “A patient presents with sudden onset, severe rotatory vertigo lasting minutes, associated with nausea but no hearing loss. What’s your top differential and how do you confirm it?” (Answer: BPPV, confirmed by Dix-Hallpike).
- Performing Dix-Hallpike: Always warn the patient about inducing vertigo. Maintain eye contact to observe nystagmus, and have a clear understanding of its characteristics. Practice the smooth movement.
- Differentiating Nystagmus: Examiners frequently ask about differentiating peripheral from central nystagmus. Memorise the table and be ready to explain each feature with a clinical example.
- Caloric Test Interpretation: Understand the calculation for Canal Paresis and Directional Preponderance, and their clinical significance. Be prepared to explain the COWS mnemonic.
- Safety First: In balance tests like Romberg’s and Gait test, emphasise standing close to the patient to prevent falls, as patient safety is paramount.
- “Why this test?”: For each test, be ready to explain its principle, what it measures, and why it’s clinically relevant. For example, “Why use VEMP when we have caloric tests?” (Answer: VEMP assesses otoliths and neural pathways, while caloric tests assess horizontal semicircular canals).
NEET PG Style Multiple Choice Questions
- Suppression of nystagmus by optic fixation is most suggestive of: A. Central lesion B. Peripheral vestibular lesion C. Cerebellar tumour D. Psychogenic vertigo.
- Dix-Hallpike test is most useful for diagnosing: A. Vestibular neuritis B. Ménière’s disease C. BPPV D. Acoustic neuroma.
- In caloric test, warm water irrigation produces nystagmus beating to: A. Opposite side B. Same side C. Vertical direction D. No response.
- Canal paresis in the Fitzgerald-Hallpike caloric test indicates: A. Stronger response from one labyrinth B. Weakness of one labyrinth C. Central lesion only D. Bilateral vestibular failure.
- A false positive fistula test seen in Ménière’s disease is called: A. Tullio phenomenon B. Hennebert sign C. Alexander sign D. Brown sign.
- vHIT mainly assesses: A. Low-frequency vestibular function B. High-frequency vestibular function C. Otolith organs only D. Visual reflex only.
- Which test best evaluates saccule function? A. Caloric test B. Rotational chair test C. cVEMP D. Optokinetic test.
- Posturography is mainly useful for: A. Lateralising labyrinth lesion B. Measuring hearing threshold C. Planning vestibular rehabilitation D. Diagnosing otosclerosis.
- Downbeat nystagmus most strongly suggests: A. Peripheral lesion B. Central lesion C. Ménière’s disease D. BPPV.
- Normal vHIT in acute vestibular syndrome strongly suggests: A. Peripheral vestibular neuritis B. Central cause like stroke C. BPPV D. Perilymph fistula.
MCQ Answers
1: B. 2: C. 3: B. 4: B. 5: B. 6: B. 7: C. 8: C. 9: B. 10: B.
Clinical-Based Questions
1. Case 1
A 45-year-old woman has brief episodes of spinning vertigo lasting 20–30 seconds when turning in bed. Dix-Hallpike produces torsional upbeating nystagmus after 5 seconds latency.
Most likely diagnosis: Posterior canal BPPV.
Best confirmatory test: Dix-Hallpike manoeuvre.
Best treatment: Epley manoeuvre (canalith repositioning).
2. Case 2
A 55-year-old man with chronic unsafe CSOM develops vertigo on pressing the tragus. He also reports ear discharge and hearing loss.
Most likely diagnosis: Labyrinthine fistula due to cholesteatoma.
Best bedside test: Fistula test.
Best next step: HRCT temporal bone and surgical management.
3. Case 3
A 60-year-old diabetic presents with acute severe vertigo and vomiting. He has spontaneous nystagmus, but vHIT shows normal gain without corrective saccades.
Most likely diagnosis: Posterior circulation stroke (central acute vestibular syndrome).
Best next step: MRI brain with diffusion-weighted imaging.
Most important bedside concept: HINTS examination.
4. Case 4
A 50-year-old patient complains of chronic imbalance and oscillopsia. Caloric testing shows absent response bilaterally, and rotational chair test shows reduced response.
Most likely diagnosis: Bilateral vestibular failure (often ototoxicity).
Best investigation to confirm functional loss: Rotational chair test + vHIT.
Best management: Vestibular rehabilitation therapy.
Frequently Asked Questions in Viva
- Q: What are the main differences between peripheral and central vertigo? A: Peripheral vertigo is typically sudden, severe, episodic, associated with nausea/vomiting, and often accompanied by auditory symptoms, while central vertigo is usually insidious, milder, constant, and associated with other neurological signs but rarely auditory symptoms.
- Q: Why is the Dix-Hallpike maneuver important in diagnosing vertigo? A: The Dix-Hallpike maneuver is crucial because it is the gold-standard test to diagnose Benign Paroxysmal Positional Vertigo (BPPV), the most common cause of recurrent vertigo, by reproducing the patient’s symptoms and eliciting characteristic nystagmus.
- Q: How does the caloric test help distinguish between unilateral and bilateral vestibular hypofunction? A: The caloric test evaluates each ear separately; a significantly reduced response from one ear indicates unilateral hypofunction (canal paresis), whereas absent responses from both ears suggest bilateral hypofunction or a “dead labyrinth.”
- Q: What is the significance of “fatiguability” in nystagmus observed during vestibular testing? A: Fatiguability means the nystagmus and vertigo decrease or disappear with repeated testing in the same provocative position, which is a key distinguishing feature of peripheral vestibular lesions, particularly BPPV.
- Q: Can vestibular function tests be performed in children? A: Yes, many vestibular function tests can be adapted for children; for instance, rotational tests are generally better tolerated by children than caloric tests, which can be uncomfortable.
- Q: What is the role of VEMPs in evaluating dizziness? A: VEMPs specifically assess the function of the otolith organs (saccule and utricle) and their neural pathways, providing valuable information for diagnosing conditions like Meniere’s disease or superior canal dehiscence syndrome, which are not directly tested by caloric or rotational tests.
- Q: Why is it important to differentiate between peripheral and central causes of dizziness? A: Differentiating between peripheral and central causes is critical because central causes often indicate more serious neurological conditions (e.g., stroke, tumor) requiring urgent and distinct management compared to more benign peripheral vestibular disorders.
———— End ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: This chapter provides a complete, exam-oriented understanding of vestibular function tests, including bedside examination, instrumental evaluation, interpretation tables, mnemonics, MCQs, and clinical case scenarios, making it sufficient as a standalone resource for MBBS and ENT postgraduate preparation. Master Vestibular Function Tests for NEET PG and Viva, Vestibular Function Tests Notes with MCQs (ENT CBME), Learn Dix Hallpike and Caloric Test Easily, Vestibular Function Tests Simplified for MBBS Students, Vestibular Function Tests Exam Guide by Dr Rahul Bagla, High-Yield Vestibular Tests with Tables and Mnemonics, vHIT vs Caloric Test Explained for ENT Exams, Vestibular Function Tests Complete Revision Notes, Vestibular Function Tests MCQs and Viva Questions, Vestibular Function Tests for MBBS and ENT PG, Vestibular function tests notes for MBBS, Vestibular function tests for NEET PG, Vestibular tests ENT viva questions, Vestibular function tests CBME ENT, Nystagmus examination ENT notes, Peripheral vs central nystagmus difference, Dix Hallpike manoeuvre steps, Dix Hallpike test interpretation, BPPV diagnosis Dix Hallpike, Roll test for horizontal canal BPPV, Fistula test ENT cholesteatoma, Hennebert sign meaning, Tullio phenomenon ENT, Romberg test vestibular lesion, Sharpened Romberg test interpretation, Unterberger stepping test Fukuda test, Past pointing test vestibular lesion, Caloric test ENT explanation, COWS mnemonic caloric test, Fitzgerald Hallpike caloric test formula, Canal paresis calculation ENT, Directional preponderance meaning ENT, vHIT test ENT explanation, Video head impulse test gain meaning, vHIT vs caloric test difference, Rotational chair test vestibular evaluation, VEMP test ENT notes, cVEMP vs oVEMP difference, VEMP interpretation superior canal dehiscence, Posturography dynamic posturography ENT, Computerised dynamic posturography sensory organisation test, ENG vs VNG difference, Optokinetic nystagmus test ENT, Vestibular neuritis tests, Ménière disease vestibular tests, Acoustic neuroma caloric test findings, Bilateral vestibular failure diagnosis, Vestibular rehabilitation posturography, Vestibular system physiology notes, ENT dizziness investigation summary, Vestibular function test MCQs with answers, Vestibular function test mnemonics and revision, Vestibular tests exam guide Dr Rahul Bagla,
Just Excellent *
Thanks Sir