Audiometry tests are essential assessments used to evaluate an individual’s hearing capabilities. Various types of audiometry tests are employed, including Pure Tone Audiometry, Speech Audiometry, Bekesy Audiometry, and Impedance Audiometry. Among these, Pure Tone Audiometry (PTA) is considered the gold standard for measuring hearing thresholds.
Pure Tone Audiometry (PTA)
PTA is a subjective test designed to determine the hearing threshold for pure tones, which are sinusoidal waves characterised by a single frequency, amplitude, and phase. Pure Tone Audiometry (PTA) is considered the gold standard for measuring hearing thresholds.
- Instrument: The test utilises an instrument called an audiometer, which is an electronic device that produces pure tones. The intensity of the audiometer can be increased or decreased in 5 dB steps.
- Audiogram: During the test, the threshold intensity for each frequency is measured and recorded in a graphical representation known as an audiogram.
- Components of an Audiometer. An audiometer is composed of several key parts:
- Electronic Oscillator: This component generates pure tones across a range of frequencies, from low to high.
- Intensity Dial: This dial allows the examiner to adjust the threshold intensity of hearing for each tone.
- Headphones: These deliver pure tones of various frequencies to each ear separately via air conduction.
- Bone Conductor: A vibrator placed on the mastoid or forehead to deliver sound via bone conduction
Prerequisites for PTA. For accurate results, PTA should be conducted under specific conditions:
- Sound-Proof Environment: The test should take place in a sound-proof room, with ambient noise levels accepted at less than 35 dB.
- Minimising Distractions: Transient noises, such as sneezing or coughing, should be avoided, as they can interfere with the test results.
- Examiner-Patient Interaction: The patient sits in a soundproof booth while the examiner conducts the audiometry from outside. Communication can occur via intercom or face-to-face to observe the patient’s reactions.
Procedure of PTA. The testing process follows a standardised sequence to ensure reliability. The testing process typically begins with the better ear.
- Air Conduction (AC) Testing: The thresholds for pure tones are measured in the following order: 1000 Hz, 2000 Hz, 4000 Hz, and 8000 Hz, followed by 500 Hz and 250 Hz. If there is a difference of 20 dB or more between contiguous frequencies, inter-octave frequencies (750 Hz, 1500 Hz, 3000 Hz, and 6000 Hz) will also be tested. The procedure is then repeated for the other ear.
- Bone Conduction (AC) Testing: After completing AC testing for both ears, conduct bone conduction testing if an air-bone gap (ABG) is suspected or to confirm sensorineural thresholds. BC thresholds are typically measured at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz. There’s usually no need to retest 1000 Hz for BC if it was the initial AC frequency.
Bracketing Technique (Modified Hughson-Westlake Method)
The bracketing technique, also known as the 10 dB down, 5 dB up method, involves delivering each test signal at an audible level (e.g., 30 dB HL), then reducing the volume in 10 dB steps until the signal becomes inaudible. The volume is then increased in 5 dB increments until the patient can perceive the sound again. Repeat this down-10, up-5 sequence to find the hearing threshold.
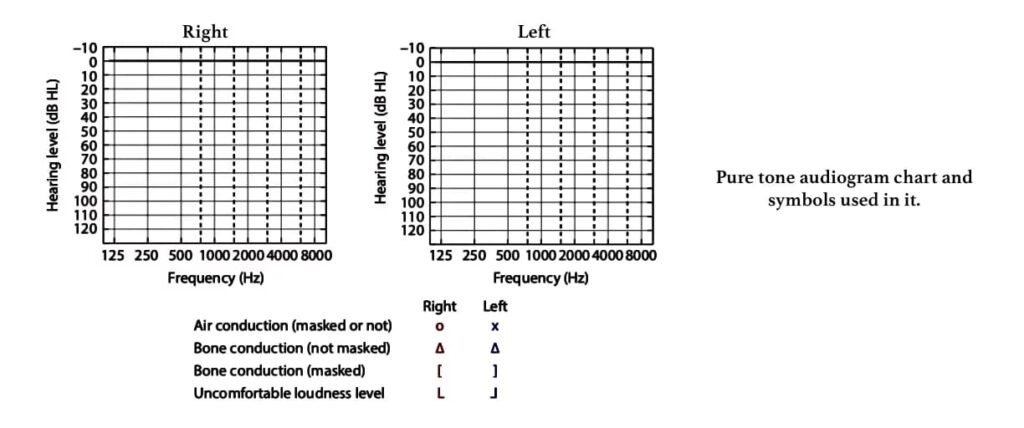
Pure Tone Audiogram is a graphical representation of hearing detection thresholds in each ear across different frequencies.
- X-axis: Represents frequency (Hz), typically ranging from 125 Hz to 8000 Hz.
- Y-axis: Represents hearing level (dB HL), with lower (negative) dB values indicating better hearing and higher dB values indicating poorer hearing.
- Symbols: Standardized symbols denote air conduction (AC) and bone conduction (BC) for each ear (e.g., Red ‘O’ for Right AC, Blue ‘X’ for Left AC; Red ‘<‘ for Right BC unmasked, Blue ‘>’ for Left BC unmasked; Red ‘[‘ for Right BC masked, Blue ‘]’ for Left BC masked).
Masking is the process of introducing a noise (a masker) to the non-test ear to prevent it from hearing the sound intended for the test ear. This is important, especially when there’s a significant difference in hearing between the two ears.
- Principle: When a sound is presented to one ear, it can cross over (transcranially) to the opposite cochlea if it’s loud enough. This phenomenon is called cross-hearing or transcranial transmission. The amount of sound energy lost as it travels from one ear to the other is called interaural attenuation (IA).
- Masking for Bone Conduction (BC) Tests:
- Masking the non-test ear is always required in all bone conduction tests.
- Why? Because bone-conducted signals vibrate the entire skull, stimulating both cochleae simultaneously, regardless of where the bone conductor is placed. Therefore, to ensure you are measuring the bone conduction of only the test ear, the non-test ear must be masked with a narrow band noise.
- Masking for Air Conduction (AC) Tests: However, for air conduction tests, a continuous masking noise (or masker) is required only when the interaural hearing difference (AB gap) exceeds 40 dB or more (when using supra or circum-aural headphones), or 55 dB or more (when using insert earphones). This is done to avoid transcranial transmission/ interaural attenuation/ cross-hearing and accurately measure hearing in each ear.
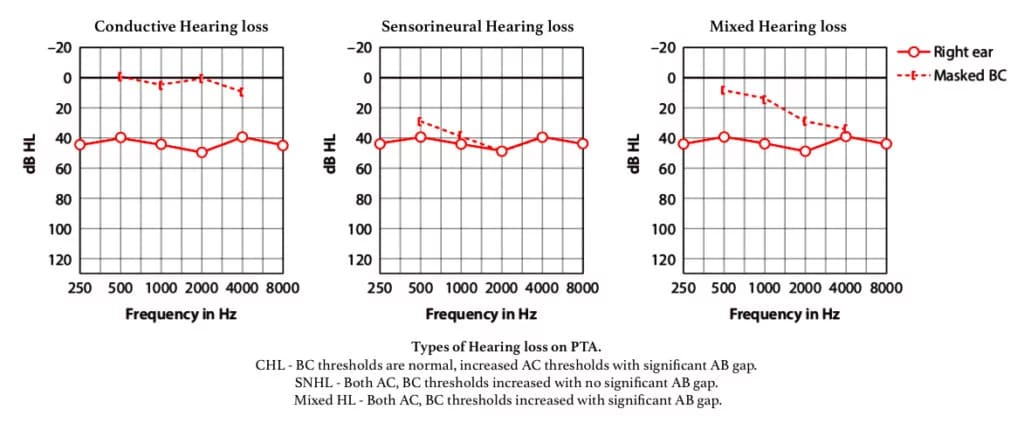
Interpretation of PTA Results. The results of PTA can indicate different types of hearing loss:
- Conductive Hearing Loss: Identified when there is a difference of more than 10 dB between air conduction and bone conduction thresholds at any frequency. The bone conduction thresholds are within normal limits (or near normal, ≤ 20 dB HL),
- Sensorineural Hearing Loss: Identified when bone conduction thresholds are raised above 20 dB HL. There is no significant air-bone gap (typically ≤ 10 dB).
- Mixed Hearing Loss: Occurs when bone conduction thresholds are raised above 20 dB HL, accompanied by a significant air-bone gap (ABG).
Utilisation of PTA. PTA serves multiple purposes in audiology:
- Determining Hearing Loss: It helps identify the type, degree, and configuration (shape of the audiogram, e.g., sloping, flat) of hearing loss. The air conduction pure tone audiogram primarily measures the degree of hearing loss, while the bone conduction audiogram differentiates between conductive and sensorineural hearing loss.
- Medicolegal Assessment: PTA can confirm the degree of hearing impairment for legal and insurance purposes.
- Hearing Aid Prescription: The audiogram is crucial for accurately prescribing hearing aids.
- Speech Reception Threshold: PTA also assists in determining the speech reception threshold of the subject.
Disadvantages of PTA. Despite its advantages, PTA has some limitations:
- Subjectivity: The test results are based on the patient’s responses, which can introduce variability.
- Potential for Malingering: Results may be inaccurate if the patient is feigning hearing loss.
- Age Considerations: The test may yield unreliable results in children under the age of seven, as it depends on cognitive development and cooperation.
———— End of the chapter ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/