|
The following CBME core competencies are covered in this chapter.
|
Ménière’s Disease (Idiopathic Endolymphatic Hydrops / Labyrinthine Hydrops)
Introduction
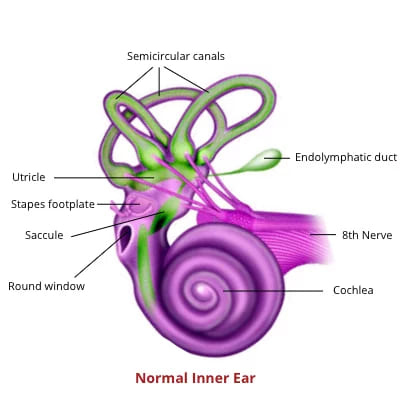
Ménière’s disease is an idiopathic disorder affecting the membranous labyrinth of the inner ear. It was first described by the French physician Prosper Ménière in 1861. The condition is characterised by abnormal accumulation of endolymph within the labyrinth, producing increased hydraulic pressure in the endolymphatic system.
This pressure leads to a classic tetrad of symptoms:
- Recurrent spontaneous episodic vertigo
- Fluctuating or progressive sensorineural hearing loss
- Tinnitus (typically low-pitched roaring)
- A sensation of fullness or heaviness in the ear
Ménière’s disease is often preceded by aural fullness and is frequently accompanied by nausea and vomiting.
Epidemiology
Both sexes are equally affected. The common age group is between the second and sixth decades.
Terminology: Ménière’s Disease vs Ménière’s Syndrome
Meniere’s disease is idiopathic in nature, meaning its exact cause is unknown. In contrast, Meniere’s syndrome occurs secondary to other underlying conditions, such as autoimmune dysfunction, endocrine disorders, syphilis, trauma, electrolyte imbalances, and parasitic infections. These conditions interfere with the normal production or resorption of endolymph.
This distinction is analogous to the differentiation between Bell’s palsy and facial paralysis due to a known cause. Just as Bell’s palsy is not diagnosed if the cause of facial paralysis is known, Meniere’s disease is not diagnosed if the cause of vertigo is known.
Diagnostic Criteria of Meniere’s Disease
The most recent guidelines for the diagnosis of Ménière’s disease were issued in 2015 by the Classification Committee of the Bárány Society, The Japan Society for Equilibrium Research, the European Academy of Otology and Neurotology (EAONO), the Equilibrium Committee of the American Academy of Otolaryngology– Head and Neck Surgery (AAO–HNS) and the Korean Balance Society. It is as follows.

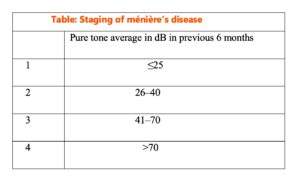
Staging of Ménière’s Disease (Hearing-Based Staging)
The staging system is essential in the diagnosis of certain, definite and probable Meniere’s disease. It is based on the average of pure tone thresholds at 0.5, 1, 2 and 3 kHz (rounded to the nearest whole) of the worst audiogram during 6 months before start of treatment.
Clinical Features of Meniere’s Disease
The clinical presentation of Meniere’s disease is characterised by a combination of vertigo, hearing loss, tinnitus, and aural fullness.
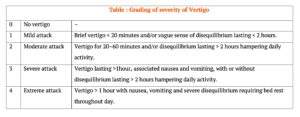
1. Vertigo
This is the hallmark symptom of Meniere’s disease, characterised by sudden, episodic attacks of vertigo that may last from a few minutes to several hours. A commonly used thumb rule is that Ménière’s vertigo lasts between 24 minutes and 24 hours in the majority of cases. Importantly, the patient remains conscious and has no focal neurological deficit during the attack. These episodes are often accompanied by nausea, vomiting, ataxia, nystagmus, abdominal cramps, diarrhoea, cold sweats, pallor, and bradycardia. Some patients may experience warning signs such as aural fullness, changes in tinnitus, or ear discomfort before an attack. During remission periods, patients may report hearing loss, a sense of imbalance, or be asymptomatic.
Diagnostic requirement (symptom-based): At least two definitive episodes of vertigo lasting for at least 20 minutes are required.
Tullio phenomenon
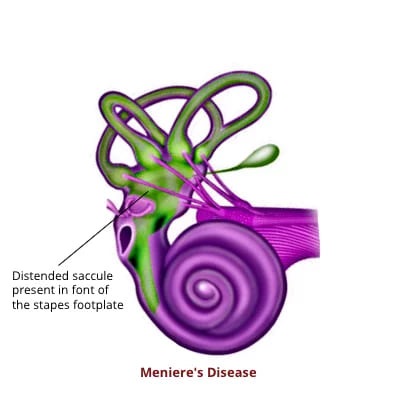
Attacks of vertigo on hearing loud noise, probably due to the distended saccule lying against the stapes footplate. However, this phenomenon is also noticed when there are three functioning windows in the ear, e.g., a fenestration of the horizontal canal in the presence of mobile stapes.
Nystagmus in Ménière’s disease
Nystagmus is seen in all patients and progresses through three phases:
- Irritative phase: beats towards the affected ear
- Paretic phase: beats towards the healthy ear
- Recovery phase: beats again towards the affected ear
Hennebert’s sign
Application of negative pressure to the external auditory canal produces horizontal nystagmus in about 90% of cases due to the proximity of the stapes footplate to a dilated saccule.
2. Fluctuating Hearing Loss
Hearing loss may accompany or precede vertigo. Initially, hearing may be normal during remission phases, but repeated episodes can lead to permanent deafness. Hearing loss typically affects low frequencies first. Patients may complain that music sounds disharmonious.
Associated cochlear phenomena
- Recruitment: sounds become intolerably loud at certain intensities (intolerance to loud sounds), making them poor candidates for hearing aids.
- Diplacusis: difference in pitch perception between ears.
- Dysacusis: difficulty processing sound details due to distortion in frequency or intensity.
- Diplacusis binauralis dysharmonica: perception of the same frequency sound as different pitch in both ears (the affected ear often perceives higher pitch).
3. Tinnitus
This is usually a low-pitched, ocean-like roaring, whistling, or hissing sound. Changes in the intensity and pitch of tinnitus may serve as a warning sign of an impending vertigo attack.
4. Aural Fullness
Patients commonly experience a sensation of fullness. Fullness may be perceived in head and neck as well.
5. Somatopsychic Effects
Common in elderly patients. Patients may develop secondary agoraphobia.
Natural History and Progression (Course of Disease)
Ménière’s disease is often progressive:
- Early stage: fluctuating low-frequency SNHL with episodic vertigo
- Middle stage: worsening hearing loss, persistent tinnitus, recurrent vertigo
- Late stage: hearing loss becomes permanent and flat; vertigo may reduce but imbalance persists
Bilateral involvement may develop in some patients over time.
Aetiology and Risk Factors
A. Proposed Etiological Theories in Ménière’s Disease (Idiopathic)
The exact cause remains unknown, but several associations and theories exist:
- Autoimmune Disorders: Meniere’s disease has been observed in some patients with lupus and rheumatoid arthritis.
- Genetic Factors: Although most cases are sporadic, 5–15% are familial, with an autosomal dominant pattern of inheritance. A possible locus between HLA-C and HLA-A on the short arm of chromosome 6 has been described.
- Viral Infections: The benefit observed from acyclovir therapy in some patients suggests that Herpes simplex virus may play a role. Damage to the endolymphatic sac and duct by viral infections has been suggested. Commonly implicated viruses include herpes simplex type 1 and enterovirus.
- Anatomical Variations: A small vestibular aqueduct and a smaller endolymphatic sac and duct have been proposed as contributing factors.
- Traumatic factors: Trauma may lead to biochemical dysfunction in the membranous labyrinth cells. It may also release debris, which can block the endolymphatic sac and duct.
- Allergic Reactions: Certain food triggers may exacerbate symptoms. The presence of IgG and IgA in cells of the endolymphatic sac supports this hypothesis. Circulating immune complexes can damage the blood vessels of the endolymphatic sac and stria vascularis.
- Vascular Factors: Endolymphatic hydrops impairs inner ear blood flow autoregulation, leading to venous congestion. The combination of hydrops and venous congestion may cause vertigo.
- Sympathetic Overactivity: This can lead to spasm of the internal auditory artery, resulting in deafness and vertigo.
- Endocrine and Metabolic Factors: Approximately 4% of Meniere’s disease cases are due to hypothyroidism, which may require thyroid replacement therapy.
B. Causes of Secondary Endolymphatic Hydrops (Ménière’s Syndrome)
Secondary hydrops may occur due to:
- Abnormal metabolic and endocrine states
- Developmental insult
- Syphilis
- Chronic otitis media (COM)
- Viral infection
- Autoimmunity
- Otosclerosis
- Abnormal fluid balance
- Leukaemia
- Otic capsule diseases (otosclerosis, Paget’s disease)
- Post-stapedectomy
- Congenital or acquired syphilis
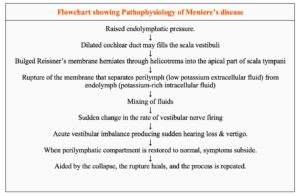
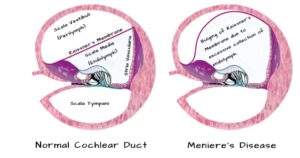
Pathophysiology of Meniere’s Disease
The underlying pathology in Ménière’s disease is excessive accumulation of endolymph within the membranous labyrinth, leading to its distension and rupture. Distension is always seen in the cochlear duct and, in most cases, also involves the saccule. The utricle is less commonly involved. Rupture causes mixing of endolymph and perilymph, disrupting ionic composition and inner ear function.
Schuknecht Theory
Schuknecht proposed that rupture of the membranous labyrinth allows potassium-rich endolymph to mix with perilymph, causing depolarisation and inactivation of nerve cells. This produces decreased cochlear and vestibular function and symptoms of a Ménière attack. When the membrane heals, the attack subsides.
Other proposed mechanisms include: (PG Level)
- Perisaccular fibrosis
- Atrophy of the endolymphatic sac
- Loss of epithelial integrity
- Hypoplasia of the vestibular aqueduct
- Narrowing of the endolymphatic duct lumen
Mechanisms leading to hydrops
- Increased Production of Endolymph: Endolymph is produced by the stria vascularis, and its overproduction can lead to hydrops.
- Reduced Absorption of Endolymph: Normally, endolymph is absorbed in the endolymphatic sac. Any disruption in this process can contribute to fluid build-up.
- Combination of Both: In some cases, both increased production and reduced absorption may occur, exacerbating the condition.
Variants of Ménière’s Disease (Atypical Ménière)
Meniere’s disease can present in various forms, often classified based on the predominant symptoms and the specific areas of the inner ear affected. Understanding these variants is crucial for accurate diagnosis and treatment. Below are the common variants of Meniere’s disease:
1. Tumarkin’s Otolithic Crisis (Drop attacks)
Clinical Presentation: Patients experience sudden episodes of being forcefully pushed to the ground without warning, often described as a “drop attack.” These episodes occur without loss of consciousness, vertigo, or hearing loss, distinguishing them from typical Meniere’s disease attacks.
Pathophysiology: The underlying mechanism involves the deformation of the otolithic membrane in the utricle or saccule, caused by fluctuations in endolymphatic pressure. This deformation disrupts the normal functioning of the otolith organs, leading to the sudden loss of postural control.
Treatment: Intratympanic injection of gentamicin is commonly used. Gentamicin is vestibulotoxic and helps in reducing the frequency of these crises by partially ablating the vestibular function.
2. Cochlear Hydrops
Clinical Presentation: This variant involves symptoms solely related to cochlear dysfunction, such as hearing loss and tinnitus, but without vertigo. The absence of vertigo differentiates cochlear hydrops from classic Meniere’s disease.
Pathophysiology: The condition is caused by a blockage at the level of the ductus reuniens, which connects the cochlear duct and the saccule. This blockage prevents the spread of endolymphatic hydrops from the cochlea to the vestibular system, resulting in isolated cochlear symptoms.
3. Vestibular Hydrops
Clinical Presentation: Patients experience episodic vertigo without accompanying cochlear symptoms like hearing loss or tinnitus. This variant highlights the exclusive involvement of the vestibular system.
Pathophysiology: Similar to other forms of hydrops, vestibular hydrops result from endolymphatic pressure changes, but these affect only the vestibular apparatus. The cochlear function remains unaffected, leading to vertigo as the sole symptom.
4. Lermoyez Syndrome
Clinical Presentation: Lermoyez syndrome is essentially Meniere’s disease with a reversed sequence of symptom onset. Patients first notice a deterioration in hearing, which is later followed by episodes of vertigo. In some cases, vertigo is followed by a temporary improvement in hearing.
Pathophysiology: The mechanisms are similar to those of classic Meniere’s disease, involving fluctuating endolymphatic pressure. However, the order in which symptoms appear is reversed, possibly due to differing rates of fluid buildup and pressure changes within the cochlear and vestibular systems.
5. Delayed Hydrops
Clinical Presentation: Delayed hydrops may present after a period of normal inner ear function, often following an episode of viral, bacterial, or spirochetal infection. Patients may experience hearing loss, tinnitus, and vertigo, sometimes years after the initial infection.
Pathophysiology: This variant is thought to result from latent or chronic infections that cause inflammation and subsequent endolymphatic hydrops. The delayed onset of symptoms may be due to a slow, progressive accumulation of endolymph or scarring in the inner ear structures.
Clinical Examination
1. Otoscopy: The findings are usually normal, but pneumo-otoscopy of the affected ear may elicit symptoms.
2. Nystagmus: The quick component of nystagmus is directed toward the normal ear.
3. Tuning Fork Tests: These tests often reveal sensorineural hearing loss.
- Weber Test: Sound is lateralized to the better ear.
- Rinne Test: The test is positive, indicating that air conduction is better than bone conduction.
- Absolute Bone Conduction: This is reduced in the affected ear.
4. Neurologic Examination: This is essential to differentiate Meniere’s disease from other conditions that can present with vertigo, such as stroke, migraine, or brainstem compression.
Differential Diagnosis
| Condition | Features |
| Vestibular migraine | Migraine features, shorter vertigo (5 min-4 hrs), normal hearing |
| Vestibular schwannoma | Progressive unilateral HL, no fluctuation, ABR abnormal |
| TIA/vertebrobasilar insufficiency | Focal neuro deficits, vascular risk factors |
| Vestibular paroxysmia | Brief (seconds) vertigo, responds to carbamazepine |
| Recurrent unilateral vestibulopathy | Vertigo only, no hearing symptoms |
Investigations
Investigations aim to:
- Confirm cochleovestibular involvement
- Exclude secondary hydrops and retrocochlear pathology
A. Metabolic and Screening Tests (to exclude secondary causes)
- CBC
- Random blood sugar
- ESR
- Serum urea
- Serum electrolytes
- VDRL and TPHA
- Thyroid function tests
- Lipid profile
B. Cochlear Function Tests
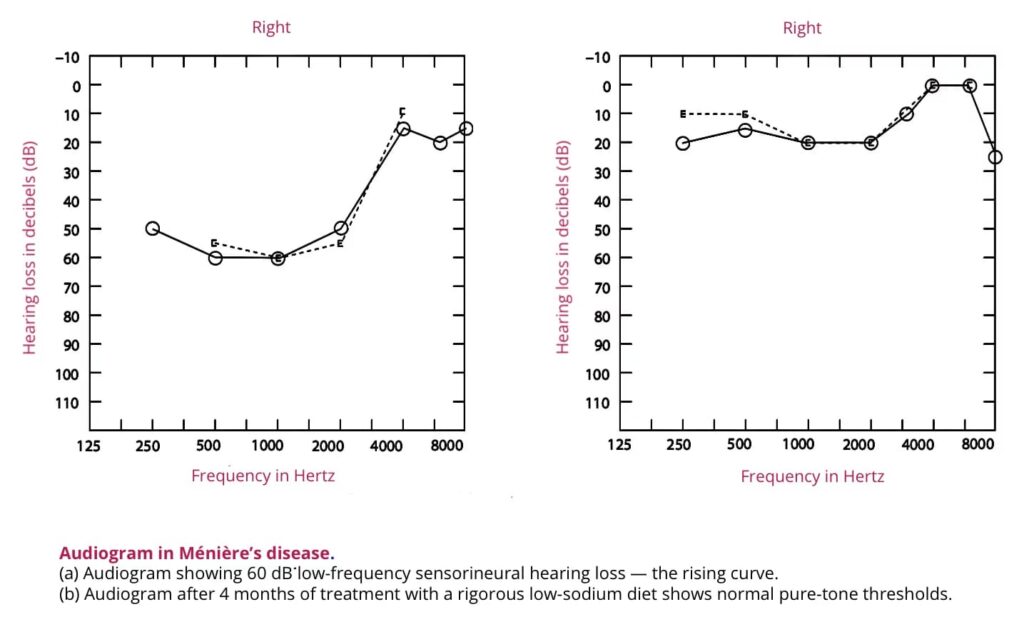
1. Pure Tone Audiometry (PTA): In the early stages of Meniere’s disease, low-frequency sensorineural hearing loss is recorded, producing a rising curve on the audiogram. Later, as higher frequencies become involved, the curve may become tent-shaped or falling type, eventually flattening in advanced stages.
2. Glycerol Test (Dehydration Test): This test involves the oral administration of glycerol, a dehydrating agent, along with an equal amount of water and lemon juice. This reduces endolymphatic pressure and may lead to improvements in hearing. The test has both diagnostic and prognostic value and is often combined with electrocochleography. Positive test suggests reversibility and benefit from diuretics.
Positive glycerol test:
- Improvement of 10 dB in two or more adjacent octaves
- Gain of 10% in speech discrimination score within 1–2 hours
- Improvement in tinnitus and aural fullness
3. Speech Audiometry: Speech discrimination score ranges from 55% to 85%. Discrimination worsens during and immediately after attacks. There is no rollover phenomenon. It helps rule out retrocochlear lesions.
4. ABLB Test: The alternate binaural loudness balance test demonstrates recruitment.
5. Auditory Brainstem Response (ABR/BERA): Hydrops increases scala media pressure, causing basilar membrane stiffening, resulting in decreased wave V latency.
6. Electrocochleography (ECoG): This electrophysiological test measures the ratio of summating potential (SP) to action potential (AP) through either transtympanic or extratympanic methods. In Meniere’s disease, the SP/AP ratio is elevated due to basilar membrane distention toward the scala tympani. Normally, the SP/AP ratio is 30%; in Meniere’s disease, it is raised. The test is most accurate during an acute episode.
7. Caloric Test: This test often shows a decreased response and canal paresis on the diseased side in 75% of cases. In some instances, directional preponderance to the healthy side or a combination of canal paresis and directional preponderance may be observed.
C. Vestibular Function Tests
1. Romberg and Unterberger Stepping Test: Positive in ~30% cases.
2. Caloric Test: Shows reduced response (canal paresis) on the affected side in ~75%. Directional preponderance may be seen.
3. Furosemide Test (Vestibular Glycerol Test): Diuretic administration may improve vestibular symptoms.
4. Vestibular Evoked Myogenic Potential (VEMP): Useful for saccular function. Low amplitude cVEMP may be found in the affected ear.
D. Radiology
1. MRI Posterior Fossa / Internal Auditory Canal: This imaging study is essential to rule out acoustic neuromas or other cerebellopontine angle lesions in the absence of contraindications to MRI.
2. Delayed Gadolinium-Enhanced MRI: Intravenous gadolinium contrast is administered four hours before MRI, or intratympanic gadolinium is given 24 hours before MRI. This imaging technique serves as a biomarker to differentiate between the perilymphatic and endolymphatic spaces, as gadolinium loads into the perilymphatic space without entering the endolymph in a healthy inner ear.
Treatment of Meniere’s Disease
A. Management of Acute Attack
- Reassurance and rest: Head elevated; minimise head movements.
- Vestibulosuppressants (doses for adults):
- Prochlorperazine: 10 mg IV/IM/rectally for acute vertigo; or 5–10 mg TDS orally.
- Cinnarizine: 25–50 mg TDS orally.
- Promethazine hydrochloride: 25 mg orally/IM every 12 hours.
- Transdermal scopolamine: 1.5 mg patch every 72 hours.
- Diazepam: 2–5 mg IV/IM/orally; Lorazepam: 1–2 mg orally/IM/IV.
- Vasodilator: Betahistine (where available) 16 mg TDS
B. Preventive Medical
General Advice
- Anxiety management: Relaxation exercises and yoga are encouraged.
- Smoking cessation: Nicotine induces vasospasm; advise cessation.
- Dietary restrictions: Low-salt (≤2 g/day), caffeine-free diet.
- Activity modifications: Avoid flying, diving, or working at heights.
- Hydration: Avoid excessive water intake.
Management of Chronic Phase
- Vestibulosuppressants/antiemetics: Prochlorperazine 10 mg TDS orally for 2 months, then 5 mg TDS for 1 month.
- Diuretics: If vestibulosuppressants and vasodilators are ineffective. First-line: Hydrochlorothiazide 25 mg daily. Alternative: Acetazolamide 250 mg BID orally (or 500 mg extended-release daily). Both reduce episode frequency; monitor electrolytes and potassium.
- Vasodilator: Betahistine 8–16 mg TDS orally increases labyrinthine blood flow and is commonly used.
- Allergen elimination: Identifying and eliminating allergens that trigger attacks may be beneficial.
C. Refractory Cases (Intratympanic Gentamicin / Steroids)
- Intratympanic steroid injections: If medical treatments fail, repeated intratympanic injections of dexamethasone are indicated. Dexamethasone 4 mg/mL, 0.5–1.0 mL injected via tympanic membrane, repeated weekly for 2–4 weeks.
- Intratympanic gentamicin: For disabling vertigo unresponsive to steroids. Low-dose regimen: 26.4 mg/mL, 0.5–0.8 mL (one to three injections). Gentamicin, a vestibulotoxic drug, can control vertigo in 60-80% of patients but may lead to sensorineural hearing loss as a long-term complication.
D. Surgical Treatment
Indicated for 10–20% of patients with intractable vertigo refractory to medical therapy. The procedures have been divided into:
- Procedures with hearing and vestibular preservation.
- Procedures with hearing preservation and vestibular ablation.
- Procedures with hearing and vestibular ablation.
Hearing and vestibular preservation
- Endolymphatic sac decompression: The sac is opened medially into the subarachnoid space or the mastoid cavity. This surgical fistula is kept patent by inserting a silastic sheet. The preservation of hearing and vestibule is achieved.
- Intratympanic steroids with a grommet: Ventilation tube permits repeated steroid delivery.
- Tenotomy of Tensor Tympani and Stapedial Tendons: This procedure can relieve symptoms by reducing the impact of increased cochlear pressure. (obsolete)
- Sacculotomy: Puncturing the cochlear duct to drain it into the perilymph, which helps alleviate symptoms. (obsolete)
Hearing preservation, vestibular ablation
- Intratympanic gentamicin with grommet (dose as above).
- Vestibular nerve section: Selective section of the vestibular nerve via retrolabyrinthine or middle fossa approach (>90% effective).
Hearing and vestibular ablation
- Transmastoid labyrinthectomy: Complete destruction of the inner ear; reserved for intractable vertigo with severe-to-profound hearing loss.
———— End of the chapter ————
High-Yield Points
- Ménière’s disease is due to endolymphatic hydrops.
- Vertigo lasts 20 min to 24 hours (key differentiator).
- Hearing loss is fluctuating low-frequency SNHL initially.
- Definite Ménière’s requires audiometrically proven SNHL (Bárány 2015).
- Tinnitus is typically low-pitched roaring.
- Aural fullness often precedes attacks.
- ECoG shows raised SP/AP ratio.
- Caloric test shows canal paresis on affected side in most cases.
- Vestibular migraine mimics Ménière’s but hearing is usually normal.
- BPPV vertigo lasts seconds, Ménière lasts hours.
- Intratympanic steroids preserve hearing, gentamicin risks hearing loss.
- Vestibular nerve section controls vertigo (>90%) with hearing preservation.
- Labyrinthectomy is reserved for poor hearing with intractable vertigo.
- Tumarkin drop attacks occur without LOC.
- Ménière’s syndrome means secondary hydrops due to identifiable cause.
NEET PG Style MCQs
- Ménière’s disease is caused by: A. Perilymphatic fistula B. Endolymphatic hydrops C. Otolith degeneration D. Vestibular nerve tumor.
- Vertigo in Ménière’s disease typically lasts: A. Seconds B. 20 minutes to 24 hours C. 2–3 days D. Continuous for weeks.
- The earliest audiogram pattern in Ménière’s disease is: A. High frequency SNHL B. Low frequency SNHL (rising curve) C. Conductive hearing loss D. Normal audiogram always.
- Bárány 2015 criteria for definite Ménière’s disease requires: A. At least one episode of vertigo B. Audiometrically documented SNHL C. MRI evidence of hydrops mandatory D. Positive Dix-Hallpike test.
- The most typical tinnitus in Ménière’s disease is: A. Pulsatile tinnitus B. High-pitched ringing C. Low-pitched roaring D. Clicking tinnitus.
- Electrocochleography in Ménière’s disease shows: A. Reduced SP/AP ratio B. Increased SP/AP ratio C. Absent wave I only D. Normal SP/AP always.
- Caloric testing in Ménière’s disease commonly shows: A. Increased response on affected side B. Canal paresis on affected side C. Normal response always D. Bilateral hyperactive labyrinth.
- Intratympanic gentamicin controls vertigo by: A. Cochlear stimulation B. Vestibular ablation C. Middle ear ventilation D. Increasing endolymph production.
- Tumarkin otolithic crisis is best described as: A. Sudden hearing improvement after vertigo B. Drop attacks without loss of consciousness C. Continuous positional vertigo D. Vertigo triggered by loud sound only.
- Definitive surgical option for Ménière’s disease with profound hearing loss and intractable vertigo is: A. Labyrinthectomy B. Stapedotomy C. Myringoplasty D. Tympanoplasty type III.
Answers: 1: B. 2: B. 3: B. 4: B. 5: C. 6: B. 7: B. 8: B. 9: B. 10: A.
Clinical Case Scenarios
Case 1
A 42-year-old female has recurrent episodic vertigo lasting 3 hours, associated with low-pitched roaring tinnitus and aural fullness in the left ear. Hearing fluctuates between attacks. Most likely diagnosis: Definite Ménière’s disease. Best initial investigation: Pure tone audiometry. Best first-line long-term management: Low salt diet + betahistine ± diuretics.
Case 2
A 35-year-old male has vertigo episodes lasting 20–30 seconds triggered by turning in bed. There is no tinnitus or hearing loss. Most likely diagnosis: BPPV. Best bedside test: Dix-Hallpike maneuver. Best treatment: Epley maneuver.
Case 3
A 50-year-old woman has episodic vertigo lasting 2 hours with photophobia and migraine headache. Hearing is normal on audiometry. Most likely diagnosis: Vestibular migraine. Best management: Migraine prophylaxis and trigger avoidance.
Case 4
A 55-year-old male has disabling Ménière’s disease with recurrent vertigo despite low salt diet, diuretics, and intratympanic steroids. Hearing is still serviceable. Best next step: Intratympanic gentamicin or vestibular nerve section depending on hearing preservation plan.
Frequently Asked Questions in Viva
- What is Ménière’s disease? Ménière’s disease is an idiopathic inner ear disorder caused by endolymphatic hydrops leading to episodic vertigo, fluctuating SNHL, tinnitus, and aural fullness.
- How long does vertigo last in Ménière’s disease? Vertigo usually lasts between 20 minutes and 24 hours, which is a key diagnostic clue.
- What is the most common audiogram finding in early Ménière’s disease? Early disease shows low-frequency sensorineural hearing loss producing a rising audiogram curve.
- How is Ménière’s disease different from vestibular migraine? Ménière’s disease typically causes fluctuating hearing loss, whereas vestibular migraine usually has normal hearing and migraine features.
- What is the role of electrocochleography in Ménière’s disease? ECoG supports diagnosis by showing an increased SP/AP ratio due to endolymphatic hydrops.
- What is Tumarkin crisis in Ménière’s disease? Tumarkin crisis is a sudden drop attack without loss of consciousness caused by otolithic dysfunction.
- What is the best treatment for refractory Ménière’s disease? Intratympanic steroids are tried first, and intratympanic gentamicin is used for disabling vertigo if steroids fail.
———— End ————
Download full PDF Link:
Meniere’s Disease Best Lecture Notes Dr Rahul Bagla ENT Textbook
Download PPT
Meniere’s Diseases Best PPT Notes Lectures Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Ménière’s disease notes for MBBS students, Ménière’s disease symptoms and treatment, Ménière’s disease Bárány 2015 criteria explained, Ménière’s disease staging AAO-HNS, Ménière’s disease differential diagnosis table, Ménière’s disease vs vestibular migraine differences, Ménière’s disease vs BPPV comparison, Ménière’s disease pathophysiology Schuknecht theory, Endolymphatic hydrops explanation for students, Ménière’s disease audiogram low frequency SNHL, Electrocochleography SP AP ratio Ménière’s disease, Glycerol test positive criteria Ménière’s disease, Caloric test findings in Ménière’s disease, VEMP test in Ménière’s disease, Intratympanic gentamicin dose Ménière’s disease, Intratympanic steroid injection Ménière’s disease, Endolymphatic sac decompression surgery indications, Vestibular nerve section for Ménière’s disease, Labyrinthectomy indications in Ménière’s disease, Tumarkin otolithic crisis drop attacks notes, Lermoyez syndrome Ménière’s disease variant, Cochlear hydrops vs Ménière’s disease, Vestibular hydrops diagnosis and treatment, Ménière’s disease NEET PG MCQs with answers, Ménière’s disease viva questions ENT, Ménière’s disease CBME ENT exam guide, Ménière’s disease high yield points, Ménière’s disease management flowchart, Ménière’s disease investigation checklist, Ménière’s syndrome secondary endolymphatic hydrops causes, Ménière’s disease MRI delayed gadolinium hydrops imaging, Ménière’s disease revision summary ENT, Ménière’s disease case presentation in viva, Ménière’s disease short notes for university exams,
Nice book with extraordinary illustrations
Diagrams are really good and easily reproducible
Simple and to the point details about the topics..
V.nice collection of informations
Thanks
thank you for making ENT easy to understand
Mind blowing explanation Sir👏👏
Nice content with easy explanation
Good book for ENT. Easy to understand and learn.
“This book is a game-changer for ENT preparation—crisp concepts, clinically relevant points, and exactly what a student needs to excel in exams.”
Best and simplest book of ENT for proff as well and NEET PG Point of view
The pedagogical warmth of this book is unmatched- it doesn’t just teach ENT, it makes you fall in love with it.
Thanks