|
The following CBME core competencies are covered in this chapter.
|
Sudden Sensorineural Hearing Loss (SSNHL)
Introduction
SSNHL was first described by De Kleyn in 1944. It is an otological emergency. The severity of the hearing loss may vary from mild to total loss, which can be permanent. SSNHL may be accompanied by roaring type tinnitus, or there are incidences of mild transient vertigo, which may also be associated with nausea and vomiting.
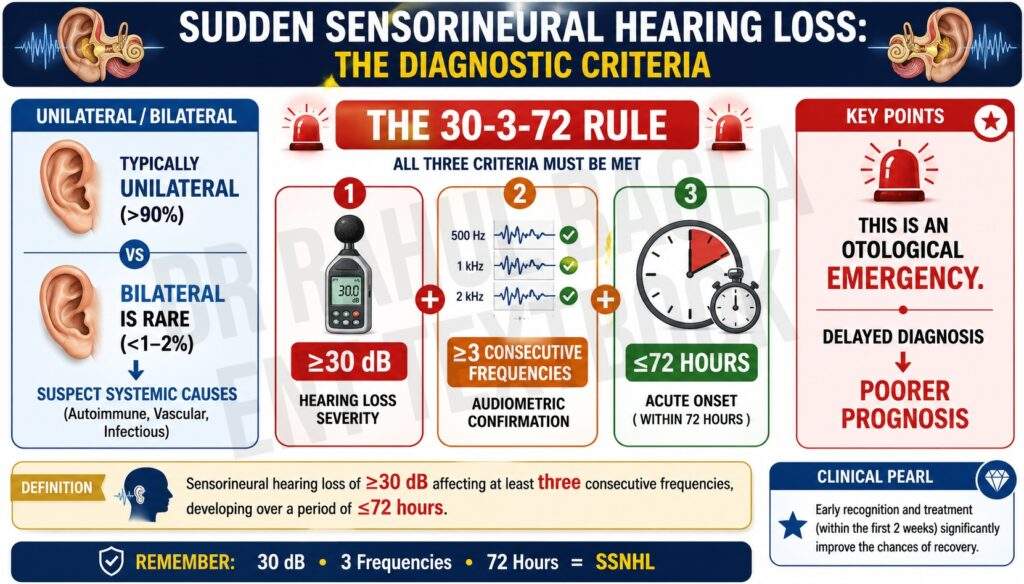
Definition and Diagnostic Criteria
- Sensorineural hearing loss of ≥30 decibels (dB)
- Affecting at least three consecutive frequencies
- Developing over a period of ≤72 hours.
- Typically unilateral (over 90% of cases).
Bilateral SSNHL is rare (<1-2%) and raises suspicion for systemic causes (autoimmune, vascular, infectious).
Epidemiology
SSNHL usually occurs in one ear, and rarely in both ears (about 1% of cases). Though it is rarely seen, it remains clinically significant because it requires urgent diagnosis and management.
Clinical Presentation
Key Symptoms
Patient may present with:
- Sudden onset of hearing loss (often noticed on waking).
- Tinnitus (roaring or buzzing).
- Aural fullness or ear blockage.
- Mild vertigo, nausea or imbalance may be present.
Natural History of SSNHL
Patients first notice their hearing loss on awakening in the morning, with or without associated tinnitus. They often present with a full or blocked ear. It can be unilateral or bilateral. As this is a common and non-specific symptom, it can be underestimated by both patients and clinicians, thus leading to a delay in evaluation and treatment.
Aetiology of SSNHL
Viral infections, vascular obstruction, breaks or rupture in the cochlear membranes have all been described as possible etiologic factors for idiopathic sudden deafness. Perilymph fistulae may occur in the oval or round window as a result of physical trauma such as a blow to the head or ear, barotrauma, acoustic trauma, surgical trauma, chronic ear disease or may occur spontaneously.
- Infectious Causes. Viral infections are a well-documented cause. It may affect the cochlea (viral endolymphatic labyrinthitis) or the eighth cranial nerve (viral neuronitis). Meningococcal meningitis, Encephalitis, Herpes virus (simplex, zoster, varicella, cytomegalovirus), Mumps, Measles, Human immunodeficiency virus, Lyme disease, Rubella, Syphilis, Toxoplasmosis.
- Vascular Causes. Vasospasm, thrombosis, or embolism of the labyrinthine or cochlear artery. Vasospasm (ie, arterial vasoconstriction) is often due to stress, fatigue, and the emotional state of the patient. Thrombosis and embolism are usually due to arteriosclerosis. Haemorrhage (leukaemia) into the inner ear. They may be associated with diabetes, hypertension, polycythaemia, macroglobinaemia or sickle cell trait.
- Trauma. Noise trauma, barotrauma, head injury, ear operations (stapedectomy), and spontaneous rupture of cochlear membranes (perilymph fistula).
- Autoimmune Causes. Immune-mediated sensorineural hearing loss. Wegener’s granulomatosis, Rheumatoid arthritis, Sjogren’s syndrome, Polyarteritis nodosa, Relapsing polychondritis, Lupus erythematosus, Ulcerative colitis, Autoimmune inner-ear disease (AIED), Cogan’s syndrome, Antiphospholipid syndrome, Sarcoid.
- Neoplastic Causes. Acoustic neuroma. Metastases in the cerebellopontine angle, carcinomatous neuropathy, Leukaemia, Myeloma.
- Ear (otologic) Causes. Meniere’s disease, Cogan’s syndrome, and large vestibular aqueduct.
- Toxic Causes. Ototoxic drugs (Aminoglycoside antibiotics, Loop diuretics, NSAIDs, Salicylates), insecticides, platinum-based chemotherapeutic agents, and general anaesthesia
- Miscellaneous Causes. Multiple sclerosis, hypothyroidism, and sarcoidosis.
- Psychogenic.
Differential Diagnosis of SSNHL
SSNHL must be differentiated from:
- Middle ear infection or disease
- Viral endolymphatic labyrinthitis
- Ototoxicity
- Meniere’s disease
- Trauma
- Bacterial labyrinthitis
- Perilymph fistula
- Retrocochlear lesions (acoustic neuroma)
- Neurological causes, such as cerebrovascular accidents
Evaluation and Investigations
In the majority of cases, there is no cause present (idiopathic). Neurological signs must be elicited if present. Otoscopy helps rule out middle ear disease or infection. Nonetheless, examination and investigation are important to exclude treatable causes.
- Careful history and examination. Rule out possibilities such as middle ear infection or disease, viral endolymphatic labyrinthitis, ototoxicity, Meniere’s disease, trauma, bacterial labyrinthitis, and perilymph fistula, and elicit neurological signs if present.
- Audiological Evaluation. Audiometry must be performed to determine the degree and type of hearing loss. 30-35 dB or more of SNHL in at least three consecutive frequencies occurring over 72 hours or less strongly indicates SSNHL. BERA (Brainstem Evoked Response Audiometry / Auditory Brainstem Response – ABR) can also be done.
- Vestibular tests. It is important to note if vertigo and accompanying nystagmus are present. Fistula test, Fitzgerald-Hallpike caloric test with electronystagmographic monitoring.
- Imaging studies of temporal bones. Magnetic resonance imaging (MRI) scanning to rule out acoustic neuroma, multiple sclerosis and cerebrovascular accidents. Fine-cut contrast CT of the temporal bone is advised if MRI is contraindicated.
- Blood investigations. For autoimmune disease, inflammatory markers and syphilis are required. Blood glucose level for diabetes.
- Exploratory tympanotomy is performed when a perilymph fistula is strongly suspected.
Prognosis
The prognosis is better than is generally supposed. Approximately 50% of patients spontaneously return to normal hearing without any treatment. Spontaneous recovery of normal hearing is more likely to occur if good prognosis factors are present.
Good prognosis factors:
- Early treatment.
- If the recovery phase starts within 2 weeks. The shorter the delay between the onset of SSNHL and the onset of recovery, the better the prognosis for complete recovery.
- Young age patients below 40 years.
- No history of vertigo.
- An Audiogram showing mild hearing loss with the involvement of low and mid frequencies.
Poor prognosis factors:
- Late treatment.
- If the recovery phase starts after 2 weeks.
- Old patients above 60 years.
- History of vertigo.
- An audiogram shows severe to profound hearing loss with the involvement of high frequencies. A downward-sloping audiogram is associated with a poorer prognosis.
Treatment of SSNHL
Treatment depends on identifying a cause, but most idiopathic cases require empirical therapy. Therefore, early treatment is the most important step.
First-Line Treatment
- Bed rest.
- Steroid therapy. Prednisolone 40–60 mg (1 mg/kg/day, up to a maximum of 60 mg daily) in a single morning dose for 1 week and then tapered off in 3 weeks. Steroids are anti-inflammatory and relieve oedema. They have been found useful in idiopathic sudden hearing loss of moderate degree. The treatment is based on the maximum adrenal output of hydrocortisone (cortisol), which is 200–300 mg/day during stress.
Adjunctive/Supportive Therapies
- Inhalation of carbogen (5% CO2+ 95% O2). It increases cochlear blood flow and improves oxygenation.
- A low-salt diet and a diuretic. It is empirical and has the same benefit as in cases of Meniere’s disease.
- Low molecular weight dextran. It decreases blood viscosity. It is contraindicated in cardiac failure and bleeding disorders.
- Vasodilator drugs. Historically used, but not routinely recommended in current guidelines due to limited evidence of efficacy.
Second-Line / Salvage Therapies
- Hyperbaric oxygen therapy. Hyperbaric oxygen therapy (HBOT) delivers 100% oxygen to a patient at a pressure greater than 1 atmosphere. This increases the concentration of oxygen in labyrinthine fluids and improves cochlear function. Therapy typically involves multiple sessions of 1–2 hours over days to weeks. HBOT is an expensive and time-consuming intervention that is available only in selected centres.
- Intratympanic (IT) steroid therapy. It raises the local concentration of steroids in cochlear fluids. The main advantage of IT treatment is the reduction in systemic corticosteroid side effects. Dexamethasone and solumedrol (methylprednisolone sodium succinate) are the most commonly used IT steroids. Most studies quote doses of 10–24 mg/mL dexamethasone and 30–40 mg/mL solumedrol. Higher concentrations may have better outcomes. Adverse effects with IT steroids are infrequent but include pain, transient dizziness, infection, persistent tympanic membrane perforation, a possible vasovagal episode during injection, and the need for repeat visits. The main risk appears to be a persistent tympanic membrane perforation at the injection site.
———— End of the chapter ————
High-Yield Points for Quick Revision
- SSNHL = ≥30 dB SNHL over 3 contiguous frequencies within 72 hrs.
- Most cases are idiopathic.
- Early treatment improves outcomes.
- MRI is mandatory to rule out acoustic neuroma.
- Steroids are the mainstay of therapy.
- IT steroids and HBOT are useful second-line options.
MCQs NEET PG & University Exam
- Which of the following is NOT a known cause of SSNHL? A. CMV infection B. Acoustic neuroma C. Otosclerosis D. Perilymph fistula Answer: C. Otosclerosis. Explanation: Otosclerosis causes progressive CHL, not SSNHL.
- What is the most important first investigation in suspected SSNHL? A. CT scan B. Audiometry C. Tympanometry D. VDRL Answer: B. Audiometry. Explanation: Confirms type and severity of hearing loss.
- What is the standard steroid dose for idiopathic SSNHL? A. 5 mg/kg/day B. 1 mg/kg/day C. 60 mg once weekly D. 10 mg daily Answer: B. 1 mg/kg/day
- A 65-year-old male presents with sudden hearing loss and vertigo. Which of the following predicts poor prognosis? A. Age <40 year B. No vertigo C. Mid-frequency loss D. Downward-sloping audiogram Answer: D. Downward-sloping audiogram
- SSNHL is defined as loss of how many decibels in how many frequencies? A. 30 dB in 2 frequencies B. 40 dB in 3 frequencies C. 30 dB in 3 frequencies D. 20 dB in 3 frequencies Answer: C. 30 dB in 3 frequencies
- Which test best helps in diagnosing retrocochlear causes of SSNHL? A. BERA B. Pure tone audiometry C. Tympanometry D. Rinne’s test Answer: A. BERA
- Intratympanic injection in SSNHL is given to avoid: A. Delayed diagnosis B. MRI scan C. Systemic steroid side effects D. Vertigo Answer: C. Systemic steroid side effects
- HBOT in SSNHL improves outcome by: A. Decreasing ICP B. Increasing oxygenation of inner ear C. Clearing infection D. Lowering BP Answer: B. Increasing oxygenation of inner ear
- Commonest cause of idiopathic SSNHL: A. Acoustic neuroma B. CMV C. Vascular insult D. Unknown Answer: D. Unknown
- MRI in SSNHL is done to exclude: A. Otitis media B. Meniere’s disease C. Vestibular schwannoma D. Otitis externa Answer: C. Vestibular schwannoma
Clinical Case Scenarios
Case 1: A young woman wakes up with left-sided hearing loss. She has no vertigo. Audiometry shows 35 dB SNHL in 3 frequencies.
- Diagnosis: SSNHL.
- Management: Start systemic steroids. MRI brain recommended.
Case 2: A 60-year-old diabetic male presents after 1 week of right-sided hearing loss and vertigo. Audiogram: severe loss with high-frequency dip.
- Poor Prognosis Factors: Age >60, vertigo, high-frequency involvement.
- Management: Systemic and IT steroids; consider HBOT.
Case 3: A scuba diver presents with sudden left ear hearing loss and tinnitus. No middle ear effusion.
- Suspected Diagnosis: Perilymph fistula.
- Management: Audiometry + MRI. Consider exploratory tympanotomy.
Case 4: Patient with Meniere’s disease has a sudden worsening of hearing.
- Diagnosis: Acute exacerbation of Meniere’s or overlapping SSNHL.
- Management: Low-salt diet, diuretic, steroids.
FAQs in Viva
- What is sudden sensorineural hearing loss (SSNHL)? Sudden SNHL is a rapid loss of hearing (≥30 dB in 3 frequencies) within 72 hours.
- Is SSNHL reversible? Yes, especially if treated early. Up to 50% recover spontaneously.
- What is the most common cause of SSNHL? Most cases are idiopathic; exact cause remains unknown.
- Why is MRI recommended in SSNHL? MRI is used to rule out vestibular schwannoma and other retrocochlear pathologies.
- How are steroids used in SSNHL treatment? Prednisolone 1 mg/kg/day for 7 days, tapered over 2–3 weeks.
- Can SSNHL affect both ears? Rarely. Only ~1% of cases are bilateral.
- Is hearing loss permanent in SSNHL? It can be, especially with delayed treatment or poor prognostic factors.
———— End ————
Download full PDF Link:
SSNHL Sudden Sensorineural Hearing Loss Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Sudden Sensorineural Hearing Loss, Sudden Hearing Loss, Sudden Deafness, Unilateral Sudden Hearing Loss, Idiopathic Sudden Sensorineural Hearing Loss, SSNHL Treatment, SSNHL Recovery, SSNHL Causes, SSNHL Symptoms, Sudden Sensorineural Hearing Loss treatment, malformation of the inner ear, head injury, prolonged exposure to loud noise, Medical emergency