|
The following CBME core competencies are covered in this chapter.
|
Vestibular Neuritis (Vestibular Neuronitis)
Introduction
Vestibular neuritis is an acute inflammation of the vestibular nerve that causes sudden, severe vertigo without hearing loss. It is one of the most common causes of acute vestibular syndrome and is frequently asked in MBBS, ENT PG, FMGE, INI-CET, and NEET PG examinations. This chapter provides simplified notes, clinical features, investigations, management, MCQs, viva questions, and high-yield revision points for rapid exam preparation.
Definition
Vestibular neuritis (also acute unilateral peripheral vestibulopathy) is a sudden, spontaneous loss of unilateral vestibular function caused by selective inflammation of the vestibular nerve, almost always of viral or post‑viral origin. A key feature of vestibular neuritis is that cochlear function is preserved, meaning there is no hearing loss or tinnitus. This differentiates it from labyrinthitis, where auditory symptoms are present. The disease is the second most common cause of vertigo (after BPPV) and a classic cause of acute sustained vertigo.
Surgical Anatomy
The vestibulocochlear nerve has two components:
- Vestibular nerve: innervates the inner ear’s vestibular system and helps maintain balance.
- Cochlear nerve: supplies the cochlea and is responsible for hearing.
The vestibular nerve arises from bipolar neurons in Scarpa’s (vestibular) ganglion and divides into superior (utricle, anterior & horizontal semicircular canals) and inferior divisions (saccule, posterior canal). The superior division travels through the longer, narrower bony canal of the labyrinthine segment, making it more susceptible to entrapment and ischaemia during inflammation – hence superior vestibular neuritis is far more common.
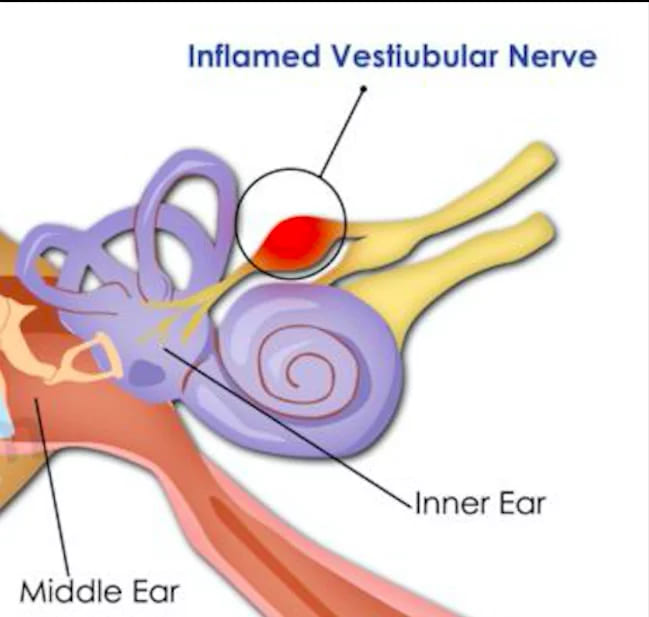
Selective inflammation of the vestibular nerve (branch of the 8th cranial nerve)
Aetiology
The exact cause remains obscure. The suggested causes are:
- Most commonly, it is associated with preceding or accompanying viral infection. It is believed to occur due to the reactivation of a latent virus, herpes simplex virus type 1 (HSV-1), in the vestibular ganglion. Other viruses that can cause isolated peripheral vestibular dysfunction include rubella, cytomegalovirus, Epstein–Barr virus, adenovirus, and influenza types A and B.
- Head trauma may cause acute vestibular loss.
- Vascular and immunological causes.
Pathophysiology
Inflammation of the vestibular nerve leads to a sudden reduction or loss of vestibular input from one side. This creates an imbalance between the vestibular systems of the two ears, producing:
- severe vertigo
- spontaneous nystagmus
- postural imbalance
As the acute inflammation settles, the brain gradually adapts through vestibular compensation, leading to symptom improvement.
Clinical Features
History
- Acute onset (<24 hours, often present on waking) of severe rotational vertigo.
- Vertigo is continuous (not episodic), worst for the first 24-48 hours, then gradually subsides over days to weeks.
- Intense nausea, vomiting, diaphoresis, prostration; patient lies still in bed, fearing movement.
- No hearing loss, tinnitus, or ear fullness (key differentiator from labyrinthitis and Meniere’s).
- No focal neurological symptoms such as diplopia, dysarthria, limb ataxia, or sensorimotor deficit, but this alone does not rule out central pathology.
Physical Examination – The Acute Vestibular Syndrome (AVS)
All findings refer to the affected (lesion) side.
1. Spontaneous Nystagmus
- Horizontal‑torsional, beating toward the healthy ear (quick phase away from the lesion).
- Peripheral type: suppressible by visual fixation; increased in darkness or with Frenzel goggles.
- Central nystagmus is often purely vertical or direction‑changing, not suppressed by fixation – a red flag.
2. Head Impulse Test (HIT, Head Thrust Test)
- The examiner rapidly turns the head ~20° while the patient fixates on the examiner’s nose.
- Positive test = catch‑up saccade when head is turned toward the affected side → indicates peripheral vestibular loss on that side.
- This is the single most sensitive bedside marker of peripheral vestibulopathy.
3. Romberg Test – falls or sways toward the side of the lesion.
4. Gait Testing – veers ipsilaterally; severe cases cannot walk.
5. Unterberger (Fukuda stepping test) – rotation >45° toward the affected ear.
Mostly vestibular neuritis is unilateral, but bilateral involvement is also reported. The rotatory chair test (used in combination with VNG or ENG) is the gold standard for the diagnosis of bilateral vestibular loss.
Differential Diagnosis of Acute Sustained Vertigo
| Condition | Key feature | Distinction |
| Vestibular neuritis | Acute vertigo, HIT positive, skew absent | No hearing loss |
| Labyrinthitis | Acute vertigo + sensorineural hearing loss | Audiometry shows SNHL |
| Posterior circulation stroke (PICA/AICA) | Can mimic totally; skew present? HIT may be falsely normal | HINTS, brain MRI with DWI |
| Labyrinthine infarction (AICA) | Acute vertigo + hearing loss ± brainstem signs | MRI/MRA |
| Ménière’s disease | Episodic vertigo (minutes–hours) with fluctuating hearing | Not sustained for days |
| Vestibular migraine | Recurrent, usually with headache/light sensitivity | History, normal HIT interictally |
Take‑home for MBBS: A normal head impulse test in a patient with acute vertigo must raise suspicion of a central (cerebellar) stroke – the “dangerous normal HIT”.
Investigations
For Unilateral Hypofunction (Gold standard)
- Caloric testing (part of VNG): reduced/absent response on the affected side (canal paresis >25%).
- Video Head Impulse Test (vHIT) – shows reduced VOR gain and overt/covert saccades in the plane of the affected canal(s). In superior neuritis, the lateral and anterior canals are involved; the posterior canal is spared.
To differentiate between Superior and Inferior Neuritis
- c‑VEMP (cervical VEMP) – assesses saccular function / inferior vestibular nerve. Absent or reduced in inferior neuritis.
- o‑VEMP (ocular VEMP) – assesses utricular function / superior vestibular nerve. Absent in superior neuritis.
- Pure inferior neuritis is rare (~5%) and presents with normal HIT/calorics (posterior canal spared) but reduced c‑VEMP.
Others
- Pure‑tone audiometry – normal (to rule out labyrinthitis).
- MRI brain with gadolinium – may show enhancement of the vestibular nerve (not required for routine diagnosis). CT/CTA if vascular risk factors and HINTS cluster indicate a central cause.
- Essential in atypical presentations (elderly, vascular risk factors, normal HIT, skew present, severe truncal ataxia).
Management (Phase‑wise)
Phase 1: Acute Suppression (First 1–3 days)
- Vestibular suppressants
- Antihistamines (e.g., dimenhydrinate 50 mg oral/IM, or meclizine 25–50 mg oral)
- Anticholinergics (e.g., scopolamine transdermal patch)
- Antidopaminergics (e.g., prochlorperazine 5–10 mg IM/oral, or metoclopramide for vomiting)
- Antiemetics (ondansetron) for nausea; not primarily vestibulosuppressive.
- Fluids & electrolyte replacement IV if severe vomiting.
- Corticosteroids (level of evidence moderate): Methylprednisolone 100 mg/day × 3 days, then taper over 3 weeks, may improve 1‑year vestibular function if started within <72 hours. Discuss risk–benefit (contraindicated in uncontrolled diabetes, peptic ulcer).
- DO NOT continue suppressants beyond 3 days – they impair central compensation. Encourage early head and eye movements as tolerated.
Phase 2: Vestibular Rehabilitation (from ~day 4 onwards)
- Supervised therapy to retrain gaze stability (gaze stabilisation exercises) and postural control.
- Bedside Cawthorne–Cooksey exercises (graduated eye/head movements, sitting, standing, turning, throwing tasks).
- Gradual return to normal activity; many programs include habituation, adaptation and balance training.
Phase 3: Prognosis and Chronic Management
- 80–90% recover full daily function within 6 weeks.
- Detailed canal recovery: central compensation masks residual canal paresis; caloric/vHIT may remain abnormal.
- ~15–30% develop chronic dynamic visual disturbance (oscillopsia on head movement) and persistent subjective dizziness (PPPD).
- Follow‑up at 1, 3, 6 months; if incomplete recovery, consider tailored VRT, psychological support, and, rarely, vestibular implant research setting.
———— End of the chapter ————
High-Yield Points for NEET PG and University Exams
- Vestibular neuritis has no hearing loss (labyrinthitis has hearing loss).
- The head impulse test is positive toward the affected side (catch-up saccade).
- A normal head impulse test in acute vertigo suggests a central stroke until proven otherwise.
- Superior neuritis is far more common than inferior neuritis due to a longer bony canal.
- Nystagmus beats toward the healthy ear (away from the lesion) and is suppressed by fixation.
- Corticosteroids started within 72 hours may improve long-term recovery (evidence level moderate).
- Vestibular suppressants should not exceed 3 days (they impair central compensation).
- Vestibular rehabilitation is the mainstay of chronic management.
- MRI brain is indicated only for atypical cases or suspected central causes.
- cVEMP tests the inferior nerve (saccule); oVEMP tests the superior nerve (utricle).
NEET PG-Style MCQs
- A 45-year-old woman awakens with severe spinning dizziness, nausea, and vomiting, but she reports normal hearing. Examination shows horizontal nystagmus beating to the right and a positive head impulse test to the left. What is the most likely diagnosis? A. Labyrinthitis B. Vestibular neuritis C. Ménière’s disease D. Cerebellar stroke.
- In vestibular neuritis, the head impulse test is positive when the head is turned toward which side? A. The healthy side B. The affected side C. Either side equally D. Superior direction only.
- A 60-year-old diabetic patient presents with acute vertigo for 6 hours. The head impulse test is normal, and nystagmus is vertical. What should you do next? A. Start vestibular suppressants B. Discharge with prochlorperazine C. Order emergent MRI brain D. Perform caloric testing.
- Which investigation remains normal in vestibular neuritis but abnormal in labyrinthitis? A. vHIT B. Caloric test C. Pure tone audiometry D. cVEMP.
- Why is superior vestibular neuritis more common than inferior neuritis? A. Inferior nerve lacks blood supply B. Superior nerve travels through a longer, narrower bony canal C. HSV-1 selectively infects the utricle D. Inferior nerve is not myelinated.
- A patient with acute vertigo has a positive head impulse test, horizontal nystagmus suppressed by fixation, and no skew deviation. This pattern indicates: A. Central lesion B. Peripheral lesion C. Psychogenic vertigo D. Orthostatic hypotension.
- How long should vestibular suppressants be continued in vestibular neuritis? A. 7 days B. 2 weeks C. 3 days maximum D. Until symptoms resolve completely.
- A patient with vestibular neuritis continues to have imbalance and visual blurring with head movements after 3 months. What is the best next step? A. Repeat course of steroids B. Continue prochlorperazine C. Vestibular rehabilitation therapy D. Intratympanic gentamicin.
- Which test assesses the function of the inferior vestibular nerve and saccule? A. oVEMP B. cVEMP C. Caloric test D. vHIT.
- A 70-year-old hypertensive man presents with acute vertigo, left-sided limb ataxia, and dysarthria. The head impulse test is normal bilaterally. Most likely diagnosis: A. Vestibular neuritis B. Labyrinthitis C. Posterior circulation stroke D. Benign paroxysmal positional vertigo.
Answers: 1: B. 2: B. 3: C. 4: C. 5: B. 6: B. 7: C. 8: C. 9: B. 10: C.
Clinical Case Scenarios for Viva and Practical Exams
Case 1. A 35-year-old teacher wakes up unable to get out of bed because the room is spinning violently. She vomited three times. She denies any hearing change or ear ringing. On examination, she has left-beating horizontal nystagmus that reduces when she focuses on a target. The head impulse test to the right shows a corrective saccade. The Romberg test shows sway toward the right. Most likely diagnosis: Right-sided vestibular neuritis. Best next step: Symptomatic treatment with prochlorperazine for 1 to 2 days, IV fluids, and consider oral methylprednisolone if within 72 hours. What will you advise? Avoid prolonged suppressants, start early head movements, and follow up for vestibular rehabilitation.
Case 2. A 68-year-old diabetic, hypertensive male presents with acute vertigo, slurred speech, and double vision. He also reports mild left ear hearing loss. The head impulse test is normal to both sides. Nystagmus is bidirectional. Most likely diagnosis: Posterior circulation stroke (AICA territory) with labyrinthine infarction. Best next step: Immediate non-contrast CT head followed by MRI brain with DWI. Do not give vestibular suppressants without imaging.
Case 3. A 25-year-old medical student has an episode of severe vertigo lasting 3 days, which resolved completely. One month later, he has no symptoms, but caloric testing shows 40% right canal paresis. Most likely diagnosis: Previous right vestibular neuritis with central compensation. Explanation: Clinical recovery does not require normal caloric tests. No further treatment needed unless symptoms recur.
FAQ’s in Viva
- What is the difference between vestibular neuritis and labyrinthitis? Vestibular neuritis affects only the vestibular nerve, causing vertigo without hearing loss, whereas labyrinthitis affects both vestibular and cochlear nerves, causing vertigo with sensorineural hearing loss and tinnitus.
- Can vestibular neuritis recur? Recurrence is rare (less than 5% of cases). If vertigo recurs frequently, consider alternative diagnoses such as Ménière’s disease or vestibular migraine.
- Is the head impulse test always positive in vestibular neuritis? Yes, during the acute phase (first few days). After central compensation develops, the head impulse test may become less prominent, but is often still detectable with vHIT.
- Do steroids really work in vestibular neuritis? Current evidence shows moderate benefit. Steroids started within 72 hours may improve long-term vestibular recovery, but they do not significantly reduce acute symptom duration.
- How long does vertigo last in vestibular neuritis? Severe rotational vertigo lasts 24 to 72 hours, followed by gradual improvement over days to weeks. Complete compensation takes up to 6 weeks in most patients.
- Can a normal head impulse test ever be safe? No. In acute continuous vertigo, a normal head impulse test is a red flag for central stroke until proven otherwise. Always investigate further.
- What should I tell a patient with vestibular neuritis about returning to work? Most patients return to non-hazardous work in 2 to 4 weeks. Pilots, heavy machine operators, and construction workers require a formal vestibular assessment before return.
———— End ————
Download full PDF Link:
Vestibular Neuritis Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Gordon B. Hughes, Myles L. Pensak, H. B. Broidy. Textbook of Clinical Otology.
- Mario Sanna. Textbook of Color Atlas of Endo-Otoscopy Examination–Diagnosis–Treatment.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Vestibular neuritis notes for MBBS students, Vestibular neuritis symptoms and treatment, Vestibular neuritis vs labyrinthitis difference, Acute vestibular syndrome diagnosis, Head impulse test in vestibular neuritis, HINTS examination explained, Caloric test vestibular neuritis interpretation, Video head impulse test vHIT vestibular neuritis, Vestibular neuritis management guidelines, Vestibular neuritis steroid treatment evidence, Cawthorne Cooksey exercises vestibular rehabilitation, Vestibular neuritis NEET PG MCQs, Vestibular neuritis viva questions and answers, Vestibular neuritis differential diagnosis table, Vestibular neuritis duration of symptoms, Superior vestibular neuritis vs inferior vestibular neuritis, cVEMP and oVEMP in vestibular neuritis, Posterior circulation stroke vs vestibular neuritis, Dangerous normal head impulse test, Vestibular neuritis CBME ENT notes, Vestibular neuritis exam oriented summary, Vestibular neuritis quick revision points, Vestibular neuritis flowchart for diagnosis, Vestibular neuritis clinical case scenarios, Vestibular neuritis prognosis and recovery time, Persistent postural perceptual dizziness PPPD after neuritis, Vestibular neuritis treatment in emergency, ENT vestibular disorders revision notes, Vertigo causes and differentiation for MBBS, Acute vertigo approach for NEET PG, Vestibular neuritis notes for MBBS, Vestibular neuronitis CBME curriculum, Acute vestibular syndrome hints exam, Head impulse test positive meaning, Difference between neuritis and labyrinthitis, Vestibular neuritis NEET PG MCQs, Superior vs Inferior vestibular neuritis, cVEMP and oVEMP explained, Vestibular neuritis treatment guidelines 2025, Central vertigo red flags, Vestibular rehabilitation exercises cawthorne cooksey, ENT PG vestibular disorders summary, Acute vertigo approach for university exam, Vestibular neuritis prognosis and PPPD, Scarpa ganglion herpes simplex, Corticosteroids in vestibular neuritis evidence, Video head impulse test interpretation, Caloric testing canal paresis, Posterior circulation stroke mimics, Vertigo algorithm for medical students.
THANKS