|
The following CBME core competencies are covered in this chapter.
|
Benign Paroxysmal Positional Vertigo (BPPV)
Introduction and Definition
Benign Paroxysmal Positional Vertigo (BPPV) is the most common cause of vertigo. BPPV accounts for ~20–30% of vertigo cases and is the most common peripheral vestibular disorder. It is characterised by brief, intense episodes of rotatory vertigo that are triggered by specific changes in head position relative to gravity. Patients typically experience symptoms when getting out of bed, turning over in bed, bending forward, looking up, or extending the neck. The condition is called “benign” because it does not threaten life, “paroxysmal” because the vertigo comes in sudden, short-lived attacks, “positional” because specific head positions provoke it, and “vertigo” because it causes a false sense of rotational movement.
Epidemiology: BPPV has a female predominance with a female-to-male ratio of approximately 2:1.
Aetiology and Risk Factors
BPPV is classified into idiopathic (primary) and secondary forms.
Idiopathic (50-70% of cases): No identifiable cause. The incidence increases with age due to age-related degeneration of the utricular macula.
Secondary (known) causes include:
- Head trauma (most common secondary cause, often bilateral)
- Viral labyrinthitis or vestibular neuritis
- Meniere’s disease
- Ear surgery (especially stapedectomy or cochlear implantation)
- Prolonged bed rest or immobilisation
- Migraine (particularly in younger patients)
- Inflammatory conditions (e.g., otitis media)
In all these conditions, the common pathological event is the dislodgement of otoconial debris from the utricular macula.
Pathophysiology of BPPV
Otoconia are tiny calcium carbonate crystals that normally reside on the gelatinous membrane of the macula of the utricle and saccule. They add weight to the membrane, helping the otolith organs sense linear acceleration and gravity.
In BPPV, these otoconia become dislodged from the degenerating utricular macula and migrate into one or more of the semicircular canals. Two mechanisms have been described:
- In canalolithiasis, the dislodged otoconial debris floats freely within the semicircular canal.
- In cupulolithiasis, the debris sticks to the cupula, making it sensitive to gravity. In certain head positions, this produces abnormal cupular displacement and stimulates vestibular afferents, resulting in vertigo and nystagmus.
Why the Posterior Semicircular Canal is Most Commonly Involved
The posterior semicircular canal is most commonly involved in BPPV because its anatomy makes it the most favourable canal for otoconial trapping.
- The posterior canal lies in a position such that it becomes the most dependent semicircular canal in both the upright and supine postures. Therefore, gravity easily pulls free otoconia into this canal.
- The posterior canal’s orientation and opening allow particles to enter easily and become trapped, preventing their return to the utricle.
- During rolling movements in bed, otoconia tend to move repeatedly backwards and forward, which further encourages their migration into the posterior canal.
- Once debris enters the posterior canal, its position does not allow easy natural clearance back into the utricle, leading to persistence and recurrence of symptoms.
- The anatomical arrangement of the posterior canal, along with the common crus shared with the anterior canal, also contributes to the tendency of otoconia to settle in this canal.
Pathophysiological sequence
When the head moves into a provocative position (e.g., lying down with the head turned), the free-floating otoconial debris moves within the endolymph due to gravity. Because the debris is three times denser than endolymph, it creates abnormal endolymph flow, deflecting the cupula and stimulating the vestibular afferents. This inappropriate stimulation is interpreted by the brain as head rotation, producing vertigo and characteristic nystagmus.
Clinical Features (Symptoms) of BPPV
Typical features
- Vertigo begins after a latent period of 2–20 seconds
- Episodes may occur with or without nausea
- Vertigo usually lasts less than 1 minute
- Attacks occur in clusters and are triggered exclusively by specific head position changes (e.g., lying down, rolling over in bed, looking up to a high shelf).
- Between episodes, the patient may remain symptom-free or may feel marked unsteadiness (classically described as “walking on pillows”)
Important negative features (help differentiate from central or other peripheral causes):
- No hearing loss, tinnitus, or aural fullness (these suggest Meniere’s disease or labyrinthitis).
- No neurological symptoms like dysarthria, diplopia, or limb ataxia (these suggest central causes).
Diagnosis of BPPV
A typical history is often sufficient to establish the diagnosis. However, the properties of nystagmus during the Dix-Hallpike manoeuvre help confirm BPPV and differentiate it from central positional vertigo.
Diagnostic Criteria of BPPV (Bárány Society, 2015)
For definite BPPV, all of the following must be present:
- Recurrent episodes of positional vertigo are triggered by specific head movements.
- Duration of vertigo <1 minute per episode.
- Characteristic nystagmus on positional testing (Dix-Hallpike or supine roll test).
- No other cause identified.
Positional Tests for Diagnosis of BPPV
1. Dix-Hallpike Test (Gold standard for posterior and anterior canal BPPV)
Procedure:
- The patient sits upright on the examination couch with legs extended and head turned 45° to one side.
- The examiner rapidly brings the patient into the supine position with the head hanging 30° below the horizontal (over the edge of the couch).
- The examiner observes the patient’s eyes for nystagmus and asks about vertigo for at least 30 seconds.
- The patient is then returned to sitting upright, and after recovery (about 30 seconds), the test is repeated with the head turned 45° to the opposite side.
Interpretation (posterior canal BPPV):
- Latency: 2-20 seconds (time for debris to move).
- Nystagmus direction: Upbeating and torsional (the upper pole of the eye beats toward the undermost ear).
- Duration: Less than 60 seconds (typically 10-40 seconds).
- Fatiguability: The nystagmus and vertigo decrease with repeated testing in the same position.
Interpretation (anterior canal BPPV – rare):
- Nystagmus is downbeating and torsional (intorsion of the eye).
- Also elicited on Dix-Hallpike, but may be less reproducible.

2. Supine Roll Test (For horizontal canal BPPV)
Indication: Suspect horizontal canal BPPV when the Dix-Hallpike test produces bilateral nystagmus or when the patient describes vertigo triggered by turning the head while supine (e.g., rolling over in bed).
Procedure:
- The patient lies supine with the head elevated 30 degrees (to bring the horizontal canal into the vertical plane).
- The examiner rapidly turns the patient’s head 90 degrees to one side and holds for 30-60 seconds, observing for horizontal nystagmus.
- The head is returned to the centre and then turned 90 degrees to the opposite side.
Interpretation:
- Geotropic horizontal nystagmus (fast phase beats toward the ground): Indicates canalolithiasis of the horizontal canal. The side with the stronger nystagmus is the affected side.
- Apogeotropic horizontal nystagmus (fast phase beats away from the ground): Indicates cupulolithiasis of the horizontal canal (rare).
Supine Head Roll test
Comparison of BPPV Types
| Feature | Posterior Canal (p-BPPV) | Horizontal Canal (h-BPPV) | Anterior Canal (a-BPPV) |
| Incidence | 85-95% | 5-15% | 1-2% |
| Diagnostic test | Dix-Hallpike | Supine roll test | Dix-Hallpike (straight hanging) |
| Nystagmus direction | Upbeating + torsional (toward undermost ear) | Horizontal (geotropic or apogeotropic) | Downbeating + torsional |
| Latency | 2-20 sec | 2-20 sec | May be shorter or absent |
| Duration | <60 sec | 30-60 sec | <60 sec |
| Fatiguability | Yes | Yes | Variable |
Red Flags (Atypical Features Suggesting Central Cause)
- Nystagmus that is purely vertical or purely torsional (not mixed).
- No latency or immediate onset of nystagmus.
- Duration of nystagmus >1 minute (non-fatiguable).
- Direction-changing nystagmus on Dix-Hallpike.
- Associated neurological signs (ataxia, dysarthria, diplopia, headache).
- Failure to respond to repeated repositioning manoeuvres.
If any red flag is present, consider alternative diagnoses such as central positional vertigo (cerebellar tumour, Arnold-Chiari malformation, multiple sclerosis) and order MRI brain.
Differential Diagnosis of BPPV
| Condition | Key Distinguishing Feature |
| Central positional vertigo | Non-fatiguable nystagmus, >1 min duration, associated with neurological signs |
| Meniere’s disease | Fluctuating hearing loss, tinnitus, aural fullness, episodes lasting hours |
| Vestibular migraine | Headache, photophobia, phonophobia, episodes lasting minutes to hours |
| Orthostatic hypotension | Vertigo only on standing, not on lying down, associated with lightheadedness |
| Cervical vertigo | Neck pain, provoked by sustained neck postures, no nystagmus |
Management of BPPV (Canalith Repositioning Procedures)
The mainstay of treatment is canalith repositioning procedures (CRPs), which use sequential head and body movements to guide the otoconial debris out of the semicircular canal and back into the utricle. Medications (e.g., vestibular sedatives) are not effective for BPPV and should be avoided because they delay natural compensation.
Repositioning Manoeuvres for Posterior Canal BPPV
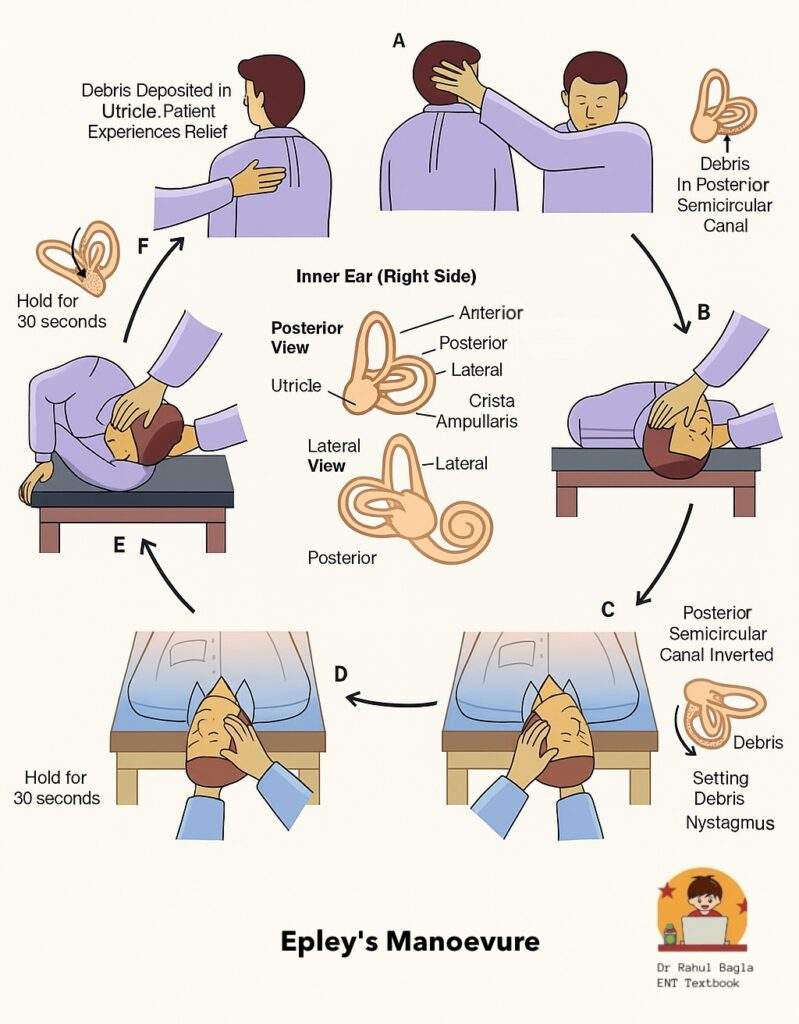
1. Epley Manoeuvre (Canalith Repositioning Procedure – CRP)
Step-by-step (for right-sided p-BPPV):
- Starting position: Patient sits upright on the couch, head turned 45° to the right (affected side).
- Position 1 (Dix-Hallpike): Rapidly lower the patient to supine with head hanging 30° below horizontal. Wait 30-60 seconds until vertigo and nystagmus subside.
- Position 2: Turn the patient’s head 90° to the left (opposite side), keeping the head still extended. Wait 30-60 seconds.
- Position 3: Roll the patient onto the left side by turning the head and body together as a unit, so the patient’s face is now towards the ground (head further turned ~90° left). Wait 30-60 seconds.
- Position 4 (Sitting up): Bring the patient back to sitting upright, while keeping the head turned 45° to the left. Then slowly turn the head forward and drop the chin 20° to neutral.
Post-manoeuvre instructions:
- Advise the patient to remain upright (avoid lying flat) for 48 hours. Postural restrictions are traditionally advised, although many recent studies suggest they may not be mandatory.
- Avoid extreme head movements (looking up, bending forward) for 48 hours.
- Sleep with the head elevated 30-45° using two pillows.
- A soft cervical collar may help restrict neck movements.
Success rate: 80-90% after one manoeuvre; repeated manoeuvres increase success to >95%.
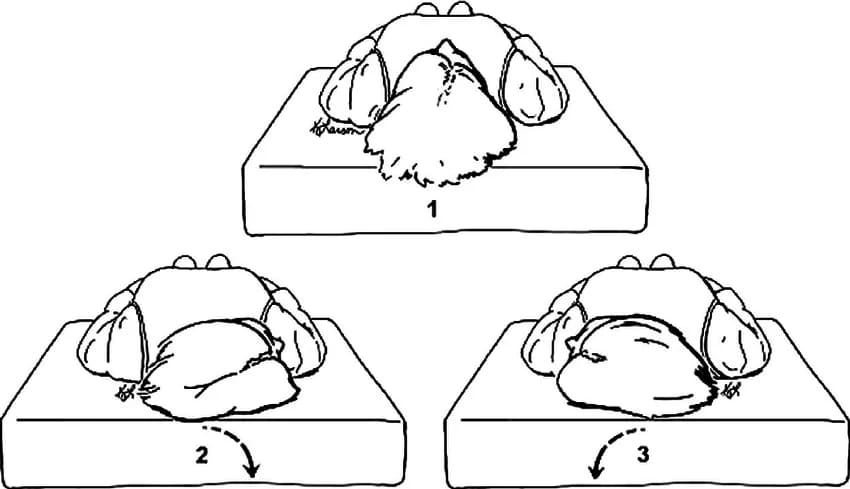
2. Semont Liberatory Manoeuvre (for p-BPPV)
Step-by-step (for right-sided p-BPPV):
- Patient sits upright on the couch, head turned 45° to the left (towards the healthy side).
- Rapidly move the patient to lie down on the right (affected) side, keeping the head turned 45° left. Hold for 1 minute (or until vertigo subsides).
- Without pausing, rapidly swing the patient 180° to lie down on the left side (face now towards the ground), keeping the head in the same 45° left rotation. Hold for 1 minute (or until symptoms subside).
- Slowly bring the patient back to sitting upright.
Success rate: 80-90% after one or two manoeuvres. This manoeuvre is more likely to induce severe vertigo but is highly effective.
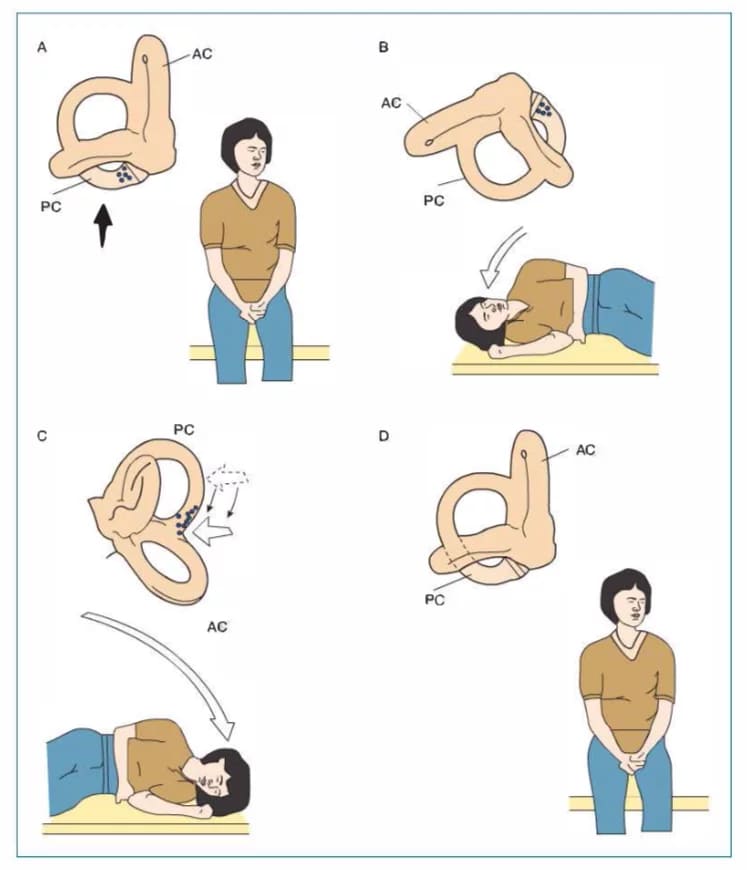
Semont’s liberatory manoeuvre
3. Brandt-Daroff Habituation Exercises (Home exercises)
Procedure: The patient performs a series of side-lying positions at home, 5 repetitions, 3 times daily. This is not a repositioning manoeuvre but rather promotes habituation (reduction of vertigo over time). It is less effective than Epley or Semont and is no longer a first-line treatment, but it can be offered to patients who cannot tolerate clinic-based manoeuvres.
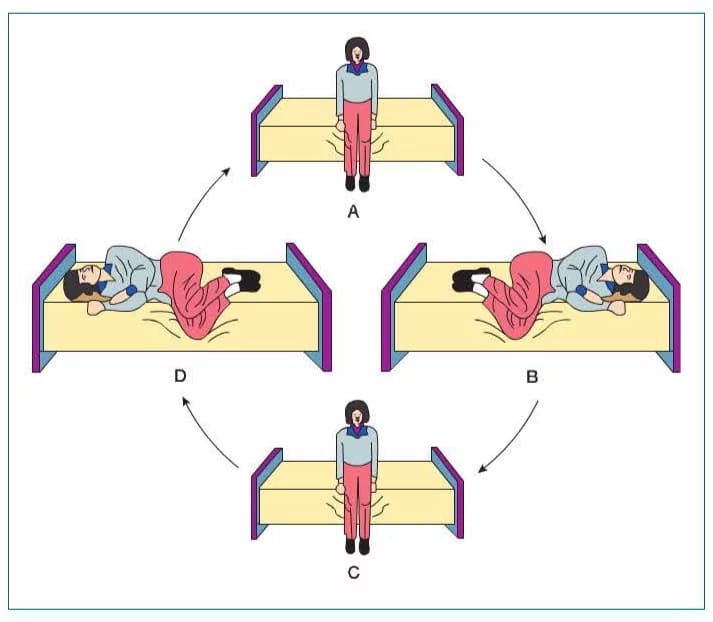
Brandt–Daroff positional exercises
Repositioning Manoeuvres for Horizontal Canal BPPV
1. For geotropic h-BPPV (canalolithiasis) – Barbecue (Lempert) Manoeuvre (for right-sided)
Step-by-step procedure:
- Patient lies supine with head elevated 30°.
- Turn head 90° to the right (affected side). Wait 30-60 seconds.
- Turn head 90° to the centre. Wait 30-60 seconds.
- Turn head 90° to the left (unaffected side). Wait 30-60 seconds.
- Roll the patient onto the left side (90° further, so head and body turn together). Wait 30-60 seconds.
- Roll the patient onto the stomach (prone) with head still turned left. Wait 30-60 seconds.
- Roll back to supine and slowly sit up.
Alternative: Forced prolonged position – The patient lies on the unaffected side (affected ear up) for 12 hours overnight. This is simpler but less effective.
2. For apogeotropic h-BPPV (cupulolithiasis) – Gufoni manoeuvre or reverse barbecue
These are more advanced manoeuvres; PG students should know that apogeotropic horizontal BPPV responds better to the Gufoni manoeuvre (patient sits, then lies quickly to the unaffected side, then turns head 45° towards the floor). Surgical options (canal plugging) are rarely needed.
Repositioning Manoeuvre for Anterior Canal BPPV
1. Modified Epley manoeuvre
The same as the standard Epley but the initial Dix-Hallpike position is held with the head straight (no turn) or the patient is positioned with the face up and chin tucking. Alternative: Perform a deep Dix-Hallpike (head hanging >30°) and then rapidly bring the patient upright.
Surgical Treatment
Indicated in <1% of refractory cases
| Procedure | Principle | Complications |
| Posterior canal occlusion (plugging) | The canal is surgically occluded, preventing endolymph movement, so debris no longer stimulates the cupula | Hearing loss (risk ~5%), persistent imbalance |
| Singular neurectomy | Sectioning the nerve to the posterior canal ampulla | Hearing loss, facial nerve injury (rare) |
Surgery is reserved for patients with intractable, debilitating symptoms lasting >6 months despite repeated CRP trials (at least 3-4 sessions).
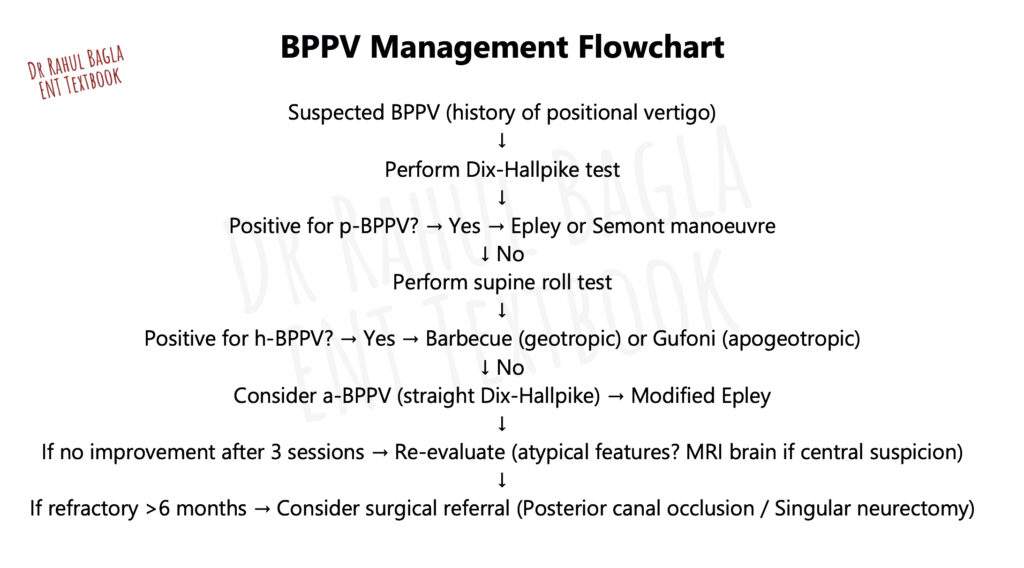
BPPV Management Flowchart
———— End of the chapter ————
High Yield Points
- BPPV is the most common cause of peripheral vertigo.
- Vertigo is brief (<1 min), intense, rotatory, and triggered by head position change.
- Common triggers: getting out of bed, rolling in bed, looking up, bending forward.
- Most common canal involved: Posterior semicircular canal (85–95%).
- Pathogenesis: dislodged otoconia from utricle enter semicircular canals.
- Most common mechanism: canalolithiasis (free-floating debris).
- Typical BPPV features: latency 2–20 sec, duration <60 sec, fatiguable nystagmus.
- No hearing loss/tinnitus/aural fullness (helps differentiate from Ménière’s disease).
- Gold standard diagnostic test: Dix–Hallpike manoeuvre.
- Posterior canal BPPV nystagmus: upbeating + torsional (towards undermost ear).
- Horizontal canal BPPV test: Supine Roll test (geotropic = canalolithiasis, apogeotropic = cupulolithiasis).
- Treatment of choice: Epley manoeuvre (posterior canal), Barbecue manoeuvre (horizontal canal); surgery is rarely needed.
NEET PG Style MCQs
- BPPV most commonly involves which semicircular canal: A. Anterior B. Posterior C. Horizontal D. Superior.
- Gold standard diagnostic test for posterior canal BPPV is: A. Caloric test B. Romberg test C. Dix-Hallpike test D. Head impulse test.
- Nystagmus in posterior canal BPPV is typically: A. Downbeating vertical B. Horizontal geotropic C. Upbeating torsional D. Pure torsional.
- Most common mechanism of BPPV is: A. Labyrinthitis B. Cupulolithiasis C. Canalolithiasis D. Endolymphatic hydrops.
- In BPPV, vertigo episodes usually last: A. Few seconds to <1 minute B. 1–2 hours C. 6–12 hours D. 1–2 days.
- Supine roll test is primarily used to diagnose: A. Posterior canal BPPV B. Horizontal canal BPPV C. Anterior canal BPPV D. Ménière’s disease.
- Geotropic horizontal nystagmus on roll test indicates: A. Central vertigo B. Cupulolithiasis C. Canalolithiasis D. Vestibular schwannoma.
- Treatment of choice for posterior canal BPPV is: A. Vestibular sedatives B. Epley manoeuvre C. Caloric irrigation D. Labyrinthectomy.
- Which of the following is a red flag for central positional vertigo: A. Latency of 5 seconds B. Fatiguable nystagmus C. Nystagmus lasting >1 minute D. Vertigo on rolling in bed.
- Most common secondary cause of BPPV is: A. Otitis media B. Head trauma C. Cholesteatoma D. Otosclerosis.
Answers with Explanations
1: B. Posterior canal is most commonly affected due to dependent position.
2: C. Dix-Hallpike is the gold standard for posterior canal BPPV.
3: C. Posterior canal BPPV produces upbeating torsional nystagmus.
4: C. Canalolithiasis is the commonest mechanism.
5: A. BPPV attacks are brief and typically last less than 1 minute.
6: B. Roll test diagnoses horizontal canal BPPV.
7: C. Geotropic nystagmus indicates canalolithiasis.
8: B. Epley manoeuvre is first-line for posterior canal BPPV.
9: C. Persistent nystagmus >1 minute suggests central cause.
10: B. Head trauma is the most common secondary cause.
Clinical Case Scenarios
1. Case 1
A 55-year-old woman develops brief spinning vertigo lasting 20 seconds when she turns to the right side in bed. There is no hearing loss or tinnitus. Dix-Hallpike produces upbeating torsional nystagmus on the right.
Most likely diagnosis: Right posterior canal BPPV,
Best test: Dix-Hallpike test,
Best management: Epley manoeuvre
2. Case 2
A 42-year-old man complains of severe vertigo when rolling in bed. Dix-Hallpike produces horizontal nystagmus on both sides. Supine roll test produces geotropic horizontal nystagmus, stronger on the right.
Most likely diagnosis: Right horizontal canal BPPV (canalolithiasis),
Best test: Supine roll test,
Best treatment: Barbecue (Lempert) manoeuvre
3. Case 3
A 60-year-old patient has positional vertigo, but Dix-Hallpike produces immediate downbeating nystagmus lasting more than 1 minute with no fatigue.
Most likely diagnosis: Central positional vertigo,
Best next step: MRI brain (posterior fossa evaluation),
Reason: Persistent downbeating nystagmus is a red flag
4. Case 4
A 70-year-old bedridden patient develops recurrent brief vertigo attacks after a prolonged hospital stay. Dix-Hallpike is positive for posterior canal BPPV.
Most likely cause: Secondary BPPV due to prolonged immobilisation,
Best management: Epley manoeuvre with vestibular rehabilitation advice.
FAQs in Viva
- Q: What is the most common cause of BPPV? A: Dislodged otoconia from the utricle that enter semicircular canals.
- Q: Which canal is most commonly involved in BPPV? A: Posterior semicircular canal.
- Q: What is the gold standard test for BPPV? A: Dix-Hallpike manoeuvre.
- Q: What is the typical duration of BPPV vertigo? A: Less than 1 minute.
- Q: What is the treatment of choice for posterior canal BPPV? A: Epley manoeuvre.
- Q: What does geotropic nystagmus indicate in roll test? A: Horizontal canal canalolithiasis.
- Q: When should MRI brain be ordered in positional vertigo? A: When red flags suggest central positional vertigo.
———— End ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Gordon B. Hughes, Myles L. Pensak, H. B. Broidy. Textbook of Clinical Otology.
- Mario Sanna. Textbook of Color Atlas of Endo-Otoscopy Examination–Diagnosis–Treatment.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Supine head roll test, Epley’s manoeuvre, Semont’s liberatory manoeuvre, Brandt–daroff positional exercises, BPPV, Semont’s liberatory, BPPV diagnostic scoring system, Understanding the BPPV Diagnostic Scoring System: A Comprehensive Guide, Canal switch in BPPV, Exploring Canal Switch Phenomenon in BPPV: Causes and Management, BPPV and arterial stiffness correlation, Investigating the Link Between BPPV and Arterial, Otolin-1 levels in BPPV patients, The Role of Otolin-1 Levels in Diagnosing BPPV, BPPV in stroke patients, Managing BPPV in Stroke Patients: Challenges and Strategies, BPPV recurrence prevention strategies, Effective Strategies to Prevent BPPV Recurrence, BPPV and vitamin D deficiency, Is There a Connection Between BPPV and Vitamin D Deficiency?, BPPV treatment in elderly patients, Tailoring BPPV Treatment for Elderly Patients: Best Practices, BPPV and vestibular rehabilitation therapy, The Role of Vestibular Rehabilitation Therapy in BPPV Management, BPPV misdiagnosis cases, Common BPPV Misdiagnoses and How to Avoid Them