|
The following CBME core competencies are covered in this chapter.
|
Eustachian Tube Anatomy
Introduction
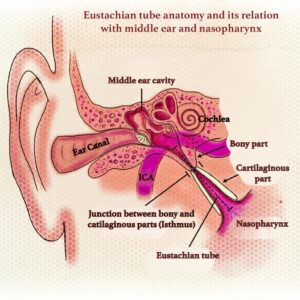
The Eustachian tube (ET) is named after Bartolomeo Eustachius (1520–1574). It is also called the pharyngotympanic tube because it connects the middle ear cavity to the nasopharynx. Structurally, it is a dynamic, trumpet-shaped, mucosa-lined channel, and functionally, it behaves like a physiological valve.
The Eustachian tube remains one of the most clinically relevant structures in otology because its dysfunction explains many common ENT problems such as ear fullness, conductive hearing loss, recurrent otitis media, otitis media with effusion, and barotrauma. Therefore, understanding its anatomy is essential for mastering middle ear diseases in both MBBS and ENT PG university exams.

Functions of the Eustachian tube
The Eustachian tube remains normally closed at rest. However, it opens briefly during swallowing and yawning. Thus, it maintains middle ear health by performing three major functions: ventilation, protection, and drainage.
1. Ventilation (Pressure Equalisation)
The middle ear is a closed, air-filled space lined by mucosa. This mucosa continuously absorbs oxygen, which creates negative pressure. Without a ventilatory channel, the tympanic membrane would retract, resulting in conductive hearing loss. Therefore, the eustachian tube opens periodically – approximately once per minute during wakefulness – to equalise middle ear pressure with atmospheric pressure. This explains why you feel ear pressure during takeoff and landing in an aircraft, and why swallowing or yawning provides relief.
2. Protection (Reflux Prevention)
The nasopharynx contains bacteria, viruses, secretions, and significant sound pressure. The eustachian tube normally remains closed at rest to prevent these from entering the middle ear. Consequently, the tube acts as a functional one-way valve, even though it lacks an anatomical sphincter. When this protective mechanism fails, nasopharyngeal secretions can reflux into the middle ear, leading to acute otitis media.
3. Drainage (Mucociliary Clearance)
The middle ear mucosa produces mucus. This mucus, along with any debris, inflammatory cells, or pathogens, must be cleared toward the nasopharynx. The eustachian tube lining contains ciliated pseudostratified columnar epithelium. These cilia beat directionally toward the nasopharynx, creating a mucociliary transport system. Therefore, the tube allows air to enter and fluid to exit. Any interruption of this clearance mechanism leads to middle ear effusion.
Embryological Origin: Foundation for Congenital Disorders
The Eustachian tube develops from the first pharyngeal pouch (endoderm) during the 4th to 6th week of gestation. The distal part of the pouch expands to form the tubotympanic recess.
- The proximal narrow part becomes the Eustachian tube.
- The distal expanded part becomes the middle ear cavity.
Therefore, congenital abnormalities of the first pouch may cause Eustachian tube anomalies. These anomalies often occur with first branchial arch syndromes, such as:
- Treacher Collins syndrome
- Hemifacial microsomia
In these conditions, the tube may be absent, stenotic, or abnormally oriented, leading to chronic middle ear disease from birth.
Basic Dimensions and Orientation: Adult vs. Infant
In Adults
Length measures 36 mm on average, with a normal range of 31 to 38 mm. The tube runs downward, forward, and medially from the middle ear to the nasopharynx. It forms a 45-degree angle with the horizontal plane. Consequently, gravity actively assists in draining secretions downward toward the nasopharynx. This orientation also means that nasopharyngeal secretions must travel upward against gravity to enter the middle ear, providing natural protection.
In Infants and Young Children
Length measures only 13 to 18 mm at birth, which is about half the adult length. The tube forms only a 10-degree angle with the horizontal plane, making it much more horizontal. As the eustachian tube of infants is wider, shorter and more horizontal, all the protective functions of the ET system are less efficient. This configuration makes drainage less efficient because gravity provides minimal assistance. Furthermore, nasopharyngeal secretions can reflux into the middle ear much more easily because they do not have to travel against a significant gravity gradient. Even the milk goes into the middle ear if the infants are not fed in a head-up position. For these reasons, eustachian tube dysfunction and otitis media are far more common in infants and young children. The tube reaches adult length and orientation by approximately 7 years of age.
Table: Infant vs. Adult Eustachian Tube
| Feature | Infant (Birth to 7 years) | Adult (7 years and older) |
| Length | 13–18 mm | 36 mm (31–38 mm) |
| Direction | More horizontal. Forms an angle of 10° with the horizontal. | Forms an angle of 45° with the horizontal |
| Orientation | More horizontal, less gravity-assisted | Downward, forward, medial |
| Angulation at isthmus | No significant angulation | Distinct angulation present |
| Bony to cartilaginous ratio | Bony part relatively longer and wider | Bony part one-third, cartilaginous two-thirds |
| Tubal cartilage rigidity | Flaccid, more collapsible. Retrograde reflux of nasopharyngeal secretions can occur | Comparatively rigid. Remains closed and protects the middle ear from reflux |
| Elastin density at hinge | Less dense, weaker recoil does not efficiently close by recoil | More dense, stronger recoil helps to keep the tube closed by recoil of cartilage |
| Ostmann’s fat pad volume | Smaller in volume | Larger and helps to keep the tube closed |
| Clinical consequence | Higher risk of otitis media and reflux | Lower risk of spontaneous reflux |
Parts of the Eustachian Tube
The tube divides into two distinct parts. Interestingly, the distribution is reversed compared to the external auditory canal, which has an outer cartilaginous part and an inner bony part. The eustachian tube has the bony part laterally and the cartilaginous part medially.
The Bony Part (Lateral, Posterolateral One-Third)
This segment measures approximately 12 mm in length. It begins from the anterior wall of the tympanic cavity, specifically from an area called the protympanum. The bony tympanic end is an oval-shaped opening, measuring 5 × 2 mm, and it is located in the anterior wall of the middle ear, a little above the level of the floor. The bony part is lined by thin cuboidal respiratory epithelium, which has fewer cilia than the cartilaginous part. Importantly, the bony part cannot collapse because it is surrounded by the temporal bone. Therefore, any obstruction in this region is due to mass lesions, granulation tissue, or bony abnormalities, not dynamic collapse.
The Cartilaginous Part (Medial, Anteromedial Two-Thirds)
This segment measures approximately 24 mm in length. It opens at the lateral wall of the nasopharynx, positioned 1 cm behind the posterior end of the inferior turbinate. The structure is remarkable: a single piece of cartilage folds upon itself to create a complex shape. This folding creates a medial lamina, a roof, and part of the lateral lamina. The remaining portion of the lateral lamina is composed of fibrous membrane rather than cartilage. Consequently, the lateral wall is more flexible than the medial wall. The cartilaginous part is lined by respiratory epithelium with abundant goblet cells and cilia, identical to the epithelium of the nasopharynx. Importantly, the cartilaginous part is dynamic – it can open and close, making it the functional part of the tube and the site of most eustachian tube disorders.
Key Anatomical Landmarks
1. The Isthmus: The Narrowest Point
The bony and cartilaginous parts meet at the isthmus. This is the narrowest part of the entire tube, with a diameter of 0.5 mm or less at its most constricted point. Consequently, the isthmus is the most common site of functional obstruction, and even mild mucosal swelling here can cause complete blockage. The isthmus is lined by respiratory epithelium similar to the nasopharynx. During swallowing, the isthmus opens last and closes first, acting as a critical control point for middle ear pressure regulation.
2. Torus Tubarius
The cartilage at the pharyngeal end raises an inverted J-shaped elevation called the torus tubarius. On nasopharyngeal endoscopy, you will find this landmark located 1 to 1.25 cm behind and slightly below the posterior end of the inferior turbinate. Therefore, the torus tubarius serves as a reliable landmark for identifying the eustachian tube opening. Its shape and position are relatively symmetric in healthy individuals.
3. Fossa of Rosenmüller
Behind the torus tubarius lies a recess called the fossa of Rosenmüller (also known as the lateral pharyngeal recess). This is a critical landmark because it is the most common site for nasopharyngeal carcinoma to originate. Therefore, any asymmetry, fullness, or irregularity in this area on endoscopy should raise immediate suspicion for malignancy and prompt biopsy. The fossa of Rosenmüller is also a common site for retained adenoid tissue after adenoidectomy and can accumulate debris in patients with chronic rhinosinusitis.
4. Tubal Tonsil (of Gerlach)
Above the torus tubarius, lymphoid tissue forms the tubal tonsil, also called Gerlach’s tonsil. During childhood, this tonsil can hypertrophy significantly. Consequently, enlarged tubal tonsils can compress the eustachian tube opening from above, leading to obstructive eustachian tube dysfunction. This is one reason why adenoidectomy (removal of nasopharyngeal lymphoid tissue) improves eustachian tube function in children – the procedure often includes removal of the tubal tonsil as well. In adults, the tubal tonsil typically atrophies, but it may persist and cause symptoms.
Note:
The Adenoid-Eustachian Tube Connection: The adenoid pad is located directly on the posterior wall of the nasopharynx, near the torus tubarius. When the adenoid hypertrophies, it can mechanically obstruct the pharyngeal opening of the eustachian tube. Additionally, the adenoid serves as a bacterial reservoir, promoting biofilm formation and recurrent otitis media. This explains why adenoidectomy is an effective treatment for chronic otitis media with effusion in children, even when the adenoid is not large enough to cause nasal obstruction.

Applied Anatomy and Clinical Correlations
The Eustachian tube is directly involved in many middle ear pathologies. Therefore, understanding its anatomy is essential for clinical ENT.
1. Otitis Media in Children. Children frequently develop otitis media because their tubes are shorter, wider, and more horizontal. As a result, secretions from the nasopharynx enter the middle ear easily and cause infection.
2. Adenoid Hypertrophy and Tubal Blockage. Enlarged adenoids or hypertrophied tubal tonsil tissue can obstruct the pharyngeal opening. Consequently, the patient develops:
- Ear blockage,
- Recurrent otitis media,
- Otitis media with effusion.
3. Cleft Palate and Muscle Dysfunction. In a cleft palate, tensor veli palatini does not function effectively. Therefore, the tubal opening becomes defective, resulting in chronic middle ear effusion and conductive hearing loss.
4. Patulous Eustachian Tube. With increasing age, a reduction in Ostmann’s fat pad volume may cause abnormal patency of the tube. This condition is called a patulous Eustachian tube, in which the tube remains open instead of closed.
5. Barotrauma During Flying and Diving. The Eustachian tube equalises middle ear pressure during altitude changes. If it fails to open properly, negative pressure develops and causes pain, retraction, and barotrauma.
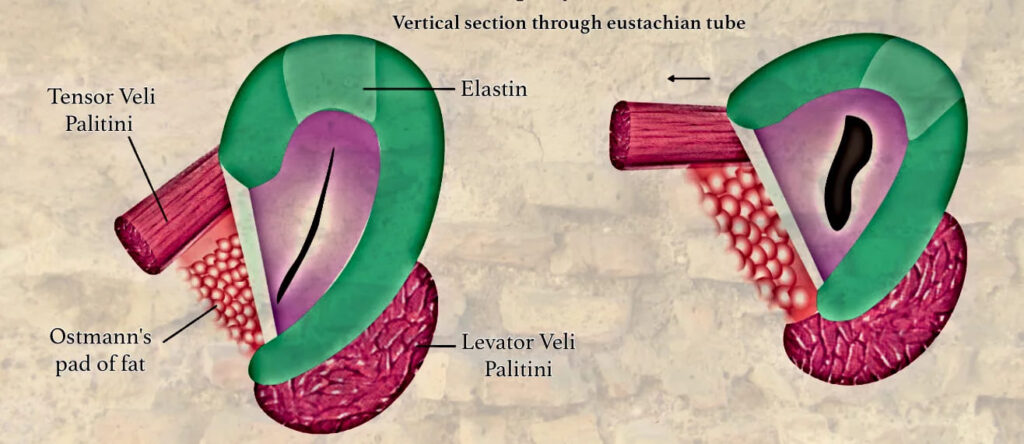
Eustachian Tube Dynamic “Valve” Mechanism
The cartilaginous tube is normally closed at rest. It opens transiently during swallowing, yawning, or sneezing. The closure is maintained by:
- Intrinsic Elastic Recoil: The “Elastin Hinge” – It is a zone, rich in elastin fibres and is situated in the roof at the junction of the medial and lateral lamina. By its recoil, it keeps the tube closed when the dilator muscle of ET (tensor veli palatini) is not in action.
- Extrinsic Tissue Pressure: Ostmann’s Pad of Fat – It is a mass of fatty tissue located in the inferolateral aspect of the eustachian tube that most likely aids in closing the tube. Therefore, it protects the middle ear from the retrograde flow of nasopharyngeal secretions. Ostmann’s fat pad decreases in volume with an increase in age, leading to a patulous eustachian tube.
Muscles of the Eustachian Tube System
These muscles are the “motors” that actively open the tube.
| Muscle | Primary Action | Origin | Insertion | Nerve Supply | Role in ET Function |
| Tensor Veli Palatini (TVP) | Primary dilator of ET | Scaphoid fossa of medial pterygoid plate, cartilage of ET, spine of sphenoid | Forms palatine aponeurosis (soft palate) | Mandibular nerve (V3) via medial pterygoid branch | Contraction pulls the lateral lamina (fibrous membrane) downwards and laterally, opening the lumen like a pulley. Most important for active opening |
| Levator Veli Palatini (LVP) | Elevates soft palate | Petrous apex, inferior surface of ET cartilage | Soft palate (blends with contralateral muscle) | Pharyngeal plexus (cranial nerves IX, X, XI) | Elevates the medial cartilaginous lamina and rotates the torus tubarius medially, aiding in opening. Its action is more palatal than tubal |
| Salpingopharyngeus | Elevates pharynx | Inferior part of cartilaginous ET | Blends with palatopharyngeus in pharyngeal wall | Pharyngeal plexus (IX, X) | Minor role. May help stabilize/open the pharyngeal end |
| Tensor Tympani | Dampens loud sounds (acoustic reflex) | Bony canal above ET, cartilaginous ET | Neck of malleus | Mandibular nerve (V3) | Not a direct dilator. Its connection suggests a role in middle ear pressure regulation during ET opening |
During activities like swallowing or yawning, the simultaneous contraction of the Tensor veli palatini and Levator veli palatini allows air to pass through the ET, equalizing middle ear pressure with atmospheric pressure. The tube closes passively due to the elastic recoil of the elastin hinge cartilage and deformation of Ostmann’s fat pad. Dysfunction of these muscles, as seen in conditions like cleft palate or neuromuscular disorders, can lead to Eustachian tube dysfunction (ETD), causing symptoms such as ear fullness, hearing loss, and recurrent otitis media. Proper functioning of these muscles is essential for maintaining middle ear pressure, particularly during altitude changes or upper respiratory infections.
Vascular Supply
- Arterial Supply: Ascending pharyngeal artery (main), middle meningeal artery, artery of pterygoid canal.
- Venous Drainage: Pterygoid venous plexus.
- Lymphatic Drainage: Retropharyngeal and deep cervical nodes.
———— End of the chapter ————
High-Yield Points
- Eustachian tube connects the middle ear to the nasopharynx.
- It stays closed at rest and opens during swallowing/yawning.
- Functions: ventilation, protection, drainage.
- Adult length: 36 mm, infant length: 13–18 mm.
- Adult angle: 45°, infant angle: 10°.
- Tube runs downward, forward, and medially.
- Bony part: 12 mm, cartilaginous part: 24 mm.
- Isthmus is the narrowest part (≤0.5 mm).
- Cartilaginous part is the functional valve and a common site of dysfunction.
- Tensor veli palatini is the main dilator muscle.
- Closure occurs due to the elastin hinge and Ostmann fat pad.
- Fossa of Rosenmüller is the common site of nasopharyngeal carcinoma.
- Children develop otitis media due to a short, wide, horizontal tube.
NEET PG Style MCQs
- The main function of the Eustachian tube is to: A. Produce cerumen B. Equalise middle ear pressure C. Conduct sound waves D. Maintain cochlear function
- The Eustachian tube remains normally closed at rest mainly to: A. Improve hearing B. Prevent reflux of nasopharyngeal secretions C. Increase mucus production D. Prevent ossicular fixation
- The average length of the Eustachian tube in adults is: A. 18 mm B. 24 mm C. 36 mm D. 45 mm
- The narrowest part of the Eustachian tube is: A. Torus tubarius B. Cartilaginous end C. Isthmus D. Tympanic opening
- The most important muscle responsible for opening the Eustachian tube is: A. Levator veli palatini B. Tensor veli palatini C. Salpingopharyngeus D. Tensor tympani
- The Eustachian tube in infants is predisposed to otitis media mainly because it is: A. Longer and narrower B. More vertical C. Shorter, wider and horizontal D. Completely closed at birth
- Ostmann’s fat pad mainly helps in: A. Opening the tube B. Closing the tube C. Producing mucus D. Protecting ossicles
- The fossa of Rosenmüller is clinically important because it is: A. Site of tubal opening B. Commonest site for nasopharyngeal carcinoma C. Narrowest part of tube D. Site of tympanic membrane attachment
- The Eustachian tube develops from: A. First pharyngeal pouch B. Second pharyngeal cleft C. Fourth pharyngeal arch D. Otic placode
- The cartilaginous part of the Eustachian tube is important because: A. It cannot collapse B. It is the functional opening-closing segment C. It forms the tympanic cavity D. It has no mucosa
Answers: 1: B. 2: B. 3: C. 4: C. 5: B. 6: C. 7: B. 8: B. 9: A. 10: B.
Clinical Case Scenarios
1. Case 1. A 6-year-old child has recurrent ear discharge and hearing loss. Nasal endoscopy shows enlarged adenoids near the torus tubarius. Most likely pathology: Obstructive Eustachian tube dysfunction causing otitis media, Best management: Adenoidectomy with treatment of middle ear disease,
2. Case 2. A 28-year-old patient complains of severe ear pain during airplane landing. Swallowing temporarily relieves symptoms. Most likely diagnosis: Eustachian tube dysfunction with barotrauma tendency, Best explanation: Failure of pressure equalisation due to poor tubal opening,
3. Case 3. A child with cleft palate develops persistent conductive hearing loss and middle ear effusion. Most likely cause: Tensor veli palatini dysfunction causing poor ET opening, Best next step: Manage cleft palate and middle ear effusion appropriately,
4. Case 4. A 55-year-old patient has autophony and hears his own breathing loudly. Symptoms worsen after weight loss. Most likely diagnosis: Patulous Eustachian tube, Best explanation: Reduced Ostmann fat pad leading to persistent tube opening,
Frequently Asked Questions in Viva
- What are the three functions of the Eustachian tube?
- What is the narrowest part and why is it important?
- Why do children get otitis media more commonly?
- Which muscle is the primary opener of ET?
- What is the importance of fossa of Rosenmüller?
- What is Ostmann’s fat pad and what happens when it decreases?
- Describe the bony and cartilaginous parts with length.
———— End ————
Download full PDF Link:
Eustachian Tube Anatomy Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Eustachian tube anatomy, Pharyngotympanic tube structure, Eustachian tube function, Eustachian tube parts, Eustachian tube location, Eustachian tube histology, Eustachian tube embryology, Eustachian tube dysfunction, Understanding the Anatomy and Function of the Eustachian Tube, A Comprehensive Guide to the Structure of the Pharyngotympanic Tube, Exploring the Components and Location of the Eustachian Tube, The Role of the Eustachian Tube in Middle Ear Health, Anatomical Insights into Eustachian Tube Dysfunction, Bony and cartilaginous parts, Ostman pad of fat, Isthmus, Difference between young and adult eustachian tube, Eustachian Tube Anatomy