Fractures of Temporal Bone. Temporal bone is very thick and hard structure located in the base of the skull. Skull base has multiple foramina, increasing susceptiblity to traumatic injury. Temporal bone contains important structures like facial nerve, labyrinth, CN VIII, ossicles, carotid artery, jugular vein etc. Any or all structures can get involve in fractures of temporal bone.
Aetiology.
- Motor vehicle accident
- Fall from height
- Physical assaults
- Gunshot wound
- Any trauma causing head, maxillofacial and spine injuries.
Types of fractures.
Its depends on the direction of fracture with respect to the long axis of petrous temporal bone
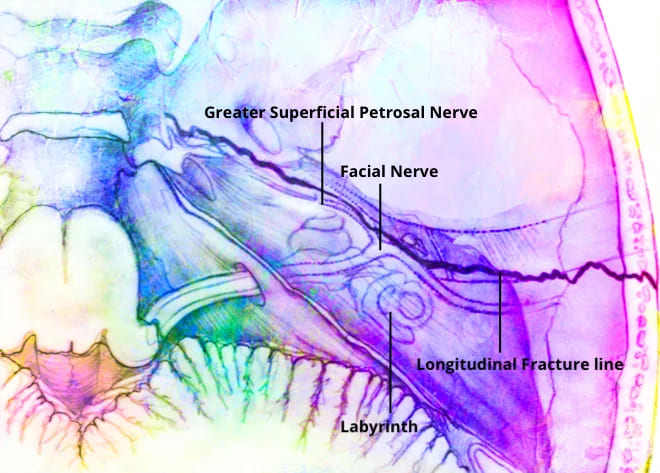
- Longitudinal. Runs parallel to long axis of petrous temporal bone. Starts at squamous part of temporal bone to end at foramen lacerum. Typically, it starts at the squamous part of temporal bone, runs through the roof of the external ear canal and middle ear towards the petrous apex and to the foramen lacerum.
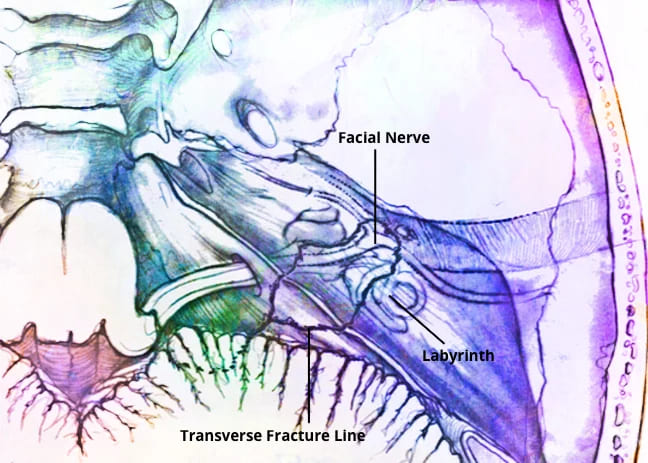
- Transverse. Runs perpendicular to the petrous temporal bone. It runs across the axis of petrous. Starts at foramen magnum or jugular foramen towards the foramen spinosum. Typically, it begins at the foramen magnum and passes through occipital bone, jugular fossa and petrous pyramid, ending in the middle cranial fossa. It may pass medial, lateral or through the labyrinth.
- Mixed (oblique). Having one or more features of both above fractures.
Further complications that should be considered are CSF leak, meningitis, meningocoele from tegmen involvement, and vascular injury to the carotid canal or jugular fossa. Delayed complications can include labyrinthine ossificans and post-traumatic cholesteatoma.
Cause of facial nerve paralysis in temporal bone fracture:
- Oedema.
- Stretching
- Intraneural hemorrhage.
- Compression by a bony spicule.
- Dehiscence of nerve.
- Transection of nerve.
Investigations.
High resolution CT Temporal bone. To know about:
- Type and direction of fracture
- Involvement of otic capsule
- Any associated complications.
Treatment of facial nerve paralysis. It depends upon time of onset of facial palsy following injury.
- Delayed onset paralysis. Treatment is same as Bell palsy and palsy almost always recovers.
- Immediate onset paralysis. Require urgent exploration.
- Facial nerve decompression
- Re-Anastomosis Of Cut Ends
- Cable Nerve Graft.
Differences between Longitudinal and Transverse Fractures
| Longitudinal | Transverse | |
| Incidence | Seen in 80% cases | Seen in 20% cases, but more common in children |
| Type of injury | Parietal blow, lateral blow over mastoid region | Occipital or frontal blow |
| Fracture line | Runs parallel to long axis of petrous temporal bone.Starts at squamous part of temporal bone toend at foramen lacerum | Runs perpendicular to the petrous temporal bone. Starts from foramen magum or jugular foramen towards the foramen spinosum |
| Injury to external and middle ear | present | Absent |
| Bleeding from ear | Common, due to injury to tegmen andtympanic membrane | Absent because tympanic membrane is intact. |
| Haemotympanum | Absent | Haemotympanum may be seen |
| Cerebrospinal fluid otorrhoea | Present, often mixed with blood and usually it is temporary. | Absent or unmanifested |
| Structures injured | Tympanic membrane , ossicles and tegmen | Labyrinth or CN VIII |
| Type of Hearing loss | Conductive, SNHL can also occur due to concussion but is not common. | Sensorineural |
| Vertigo | Less often; due to concussion | Severe, due to injury to labyrinth or CN VIII |
| Incidence of Facial paralysis | Seen in 20% cases, delayed onset. | Seen in 50% cases. Immediate onset. |
| Site of injury | Nerve is injured in tympanic segment, distal to geniculate ganglion | Injury to nerve in meatal or labyrinthine segment proximal to geniculate ganglion. |
| Skull base foramen | Ovale | Spinosum, lacerum |
———— End of the chapter ————
Download full PDF Link:
Fractures of Temporal bone Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Longitudinal fracture, Transverse fracture, Mixed fracture, Facial nerve injury, Management, Diagnosis, Prognosis, Fractures of Temporal Bone, Temporal bone fracture imaging techniques, Advanced Imaging Techniques for Diagnosing Temporal Bone Fractures, Otic capsule sparing vs disrupting fractures, Comparing Otic Capsule Sparing and Disrupting Temporal Bone Fractures, Temporal bone fracture management guidelines, Comprehensive Management Guidelines for Temporal Bone Fractures, Facial nerve injury in temporal bone fractures, Assessing and Treating Facial Nerve Injuries Resulting from Temporal Bone Fractures, Hearing loss after temporal bone trauma, Understanding Hearing Loss Following Temporal Bone Trauma, Cerebrospinal fluid leak in temporal bone fractures, Identifying and Managing CSF Leaks in Temporal Bone Fractures, Temporal bone fracture classification systems, An Overview of Classification Systems for Temporal Bone Fractures, Complications of temporal bone fractures, Recognizing and Managing Complications Arising from Temporal Bone Fractures, Temporal bone fracture rehabilitation exercises, Effective Rehabilitation Exercises Post-Temporal Bone Fracture, Temporal bone fracture case studies, In-Depth Case Studies on Temporal Bone Fracture Management