|
The following CBME core competencies are covered in this chapter.
|
Noise-Induced Hearing Loss (NIHL)
Introduction
Noise is defined as unwanted or harmful sound that disrupts auditory comfort and poses risks to physiological and psychological health. Noise-induced hearing loss (NIHL) and acoustic trauma are significant, preventable health issues caused by exposure to excessive noise. These conditions are particularly prevalent in occupational settings, such as industries involving loud machinery, gunfire, or motor racing, as well as recreational activities like using personal music devices at high volumes. NIHL is a major occupational hazard, often leading to financial compensation claims for affected employees.
Definition
Noise-Induced Hearing Loss (NIHL) refers to hearing impairment caused by exposure to excessive noise, either gradually over time (chronic exposure) or suddenly due to a single loud impulse sound.
Classification / Types of Noise-Induced Hearing Loss
It can be categorised into two types based on exposure:
- Noise-Induced Hearing Loss (NIHL)
- Acoustic Trauma (Sudden / Impulse Noise)
1. Noise-Induced Hearing Loss (NIHL)
It is caused by chronic exposure to excessive noise, typically in occupational settings. Depending upon the reversibility, the hearing loss is classified into two types:
- Temporary Threshold Shift (TTS): There is temporary hearing loss that recovers within a few days after noise exposure. It is caused by metabolic changes, such as reduced blood flow and cochlear hypoxia. Another hypothesis is that there is bending of hair cells’ stereocilia due to sudden noise exposure.
- Permanent Threshold Shift (PTS): There is permanent, irreversible hearing loss caused by repeated or severe noise exposure. It results from structural damage, including Breakdown of actin filaments in stereocilia, Swelling of inner ear structures, Apoptosis and necrosis of outer and inner hair cells, damage to the basilar membrane, and damage to spiral ganglion cells.
2. Acoustic Trauma (Sudden / Impulse Noise)
It is caused by a single exposure to an extremely intense sound (e.g., explosions, gunfire, or firecrackers), reaching 140–170 db SPL. It results in immediate hearing loss without a preceding temporary threshold shift (TTS). It can cause mechanical damage to the tympanic membrane, ossicles, organ of Corti, Reissner’s membrane, and hair cells, leading to permanent hearing impairment.
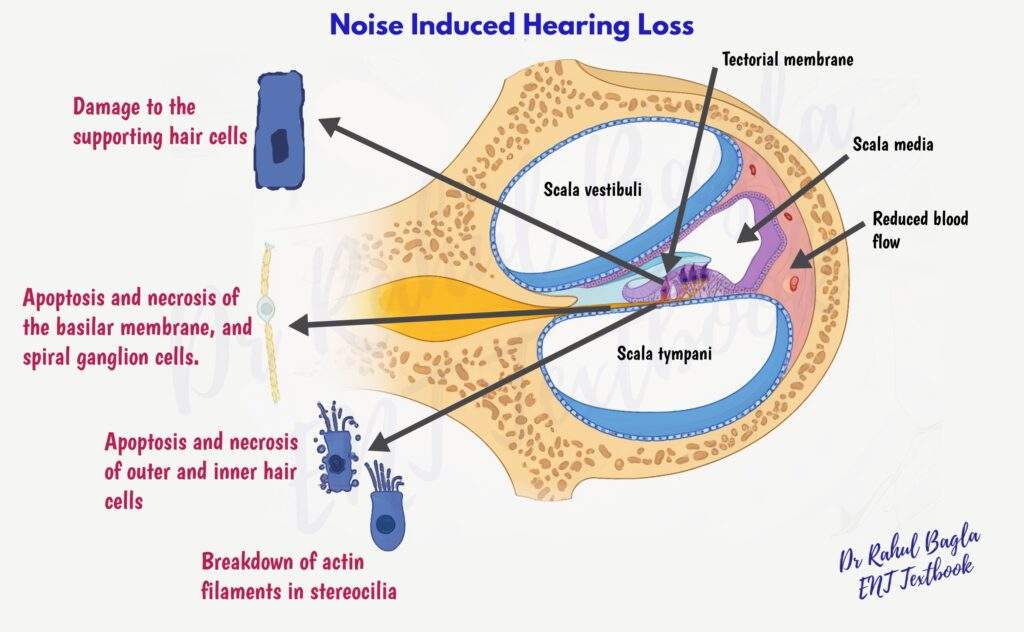
Table: Comparison between NIHL and Acoustic Trauma
| Feature | Temporary Threshold Shift (TTS) | Permanent Threshold Shift (PTS) | Acoustic Trauma |
| Type of Exposure | Short-term/limited exposure | Repeated or prolonged exposure | Single sudden impulse noise |
| Onset | Gradual after exposure | Gradual progressive | Sudden immediate |
| Reversibility | Reversible | Irreversible | Usually irreversible |
| Main Mechanism | Metabolic exhaustion, hypoxia | Structural damage, apoptosis | Mechanical disruption |
| Hair Cell Damage | Functional disturbance | Outer & inner hair cell death | Severe hair cell rupture |
| Audiogram | Temporary dip | Permanent notch & progression | Sudden severe SNHL / mixed loss |
| Examples | Short loud music exposure | Factory worker, industrial exposure | Firecracker, explosion, gunfire |
Aetiology / Common Sources of Noise Exposure
Noise exposure may occur from:
- Occupational Sources: Loud machinery industries, Gunfire exposure, Motor racing industries.
- Recreational Sources: Personal music devices at high volume, Concerts and music shows, Firecrackers
Factors Influencing Hearing Damage (Risk Factors)
- Frequency of Noise: Sounds in the 2–3 kHz range are most damaging.
- Intensity and Duration: Hearing damage correlates directly with the intensity and duration of noise exposure – sounds under 80 dB(A) are safe, while exposure above 130 dB(A) can cause immediate damage.
- Continuous vs. Interrupted Noise: Continuous noise is more harmful than intermittent noise.
- Individual Susceptibility: Genetic factors, pre-existing ear diseases, and systemic conditions (e.g., diabetes, cardiovascular disease) increase vulnerability.
- Predisposing Factors: Smoking, blue eye colour, recreational drug use, and exposure to ototoxic agents.
Clinical Features
- Symptoms: Most patients report a gradual-onset bilateral sensorineural hearing loss, frequently accompanied by tinnitus or hyperacusis. A history of prolonged exposure to loud noise (occupational/recreational) is common. With acoustic trauma cases, we often see sudden unilateral hearing loss accompanied by otalgia, imbalance, and acute stress reactions.
- Examination: Local ear examination may appear normal in chronic exposure (NIHL) or show injury to the tympanic membrane and ossicles in cases of acoustic trauma.
Diagnosis (Hearing Tests)
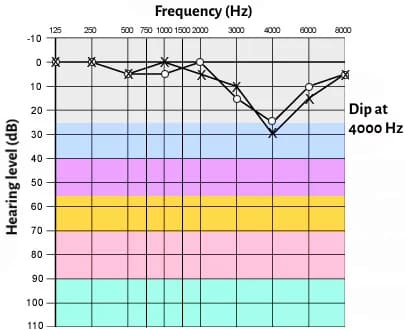
1. Pure-Tone Audiometry (PTA): It is the gold standard test for diagnosis. There is a classic 4–6 kHz notch with preservation of lower and mid frequencies. The notch is symmetrical in both ears, with some recovery at 8 kHz. The notch deepens as noise exposure increases. However:
- Not all audiograms showing a notch at 4000 Hz are due to NIHL
- Not all NIHL presents the typical 4000 Hz notch
2. Tympanometry: Normal middle ear function (unless tympanic membrane/ossicles are damaged).
3. Speech Audiometry: Assesses functional hearing loss.
4. Advanced Tests
- Otoacoustic emissions (OAE): measure outer hair cell function
- Auditory brainstem response (ABR): helps identify retrocochlear pathologies such as acoustic neuroma
5. Additional Tests
- SISI test: effectively identifies cochlear pathology (recruitment) and helps differentiate cochlear from retrocochlear lesions. The acoustic reflex test is more reliable for detecting non-organic hearing loss.
- Tympanometry with acoustic reflex: evaluates middle ear function
- Tone decay test: provides valuable information about neural adaptation in suspected retrocochlear disorders.
Characteristic Audiogram Pattern: 4–6 kHz Notch
Why the 4 kHz Dip?
The anatomical location of the 4 kHz area of the basilar membrane corresponds to that area of the basal turn (of the cochlea). It is more susceptible to damage due to:
- The anatomical rigidity makes it prone to torsion and vascular injuries.
- Reflex contraction of intratympanic muscles in response to loud sounds shifts the sound towards higher frequencies.
- Increased resonance of the external auditory canal at this frequency.
Differential Diagnosis
| Condition | Key Clinical Clue | Audiogram Pattern / Differentiating Feature |
| Presbycusis | Elderly patient, gradual progression | Bilateral high-frequency down-sloping loss (no classic notch) |
| Ototoxic drug-induced hearing loss | History of aminoglycosides, cisplatin, loop diuretics | Bilateral high-frequency SNHL, often rapidly progressive |
| Meniere’s disease | Vertigo + fluctuating hearing loss + tinnitus | Low-frequency SNHL initially |
| Acoustic neuroma | Unilateral/asymmetric SNHL, poor speech discrimination | Retrocochlear features; ABR abnormal |
| Malingering | Inconsistent symptoms, suspicious behaviour | Poor correlation between PTA and objective tests |
Preventive Measures and Hearing Conservation
1. Prevention (Industrial and Occupational)
For Industrial Workers
- Pre-employment and annual audiograms: for early detection
- Noise regulation: limit exposure to ≤115 dB (continuous/intermittent) and avoid impulse noise >140 dB
- Training programs: educate workers on NIHL risks and prevention
- Job rotation: shift workers to non-noisy areas periodically
Hearing Protection Devices (HPDs)
- Earplugs: attenuate 15–30 dB (optimal for 3–5 kHz)
- Earmuffs: provide 30–40 dB attenuation (effective across 500 Hz–8 kHz)
- Combined use: earplugs + earmuffs offer >40 dB protection
- Active noise reduction: electronic devices that cancel ambient noise, especially effective for low-frequency sounds (e.g., in aircraft)
2. Prevention of Personal Noise Trauma
- Volume control: Keep music player volume low (≤60% of maximum volume for ≤60 minutes/day at ≤60 dB)
- Headphone choice: Use noise-cancelling, muff-type headphones instead of earbuds
- Regular breaks: Take breaks from headphone use to allow ear recovery
- Early consultation: Seek ENT advice if tinnitus or hearing loss occurs
Legislation and Permissible Noise Levels (India)
1. Ministry of Labour, Govt. of India, Model Rules under Factories Act:
- Permissible Exposure Limit (PEL): 90 dB (A) for 8 hours/day (5 dB rule of time-intensity states that “any rise of 5 db noise level will reduce the permitted noise exposure time to half.).
- Impulse Noise: No exposure above 115 dB (A)or impulse noise above 140 dB (A) is allowed.
2. Noise Pollution (Regulation and Control) Rules 2000: The Ministry of Environment and Forest, Govt of India, has defined permissible limits of noise for various zones or areas. According to which silence zone is 100 m around the premises of hospitals, nursing homes, educational institutions and courts. Loudspeakers are prohibited between 10:00 PM and 6:00 AM.
3. Environment Protection Rules 2006: Manufacture, sale and use of firecrackers generating sound levels above 125 db (AI) or 145 db (C) pk from a distance of 4 m from the point of bursting are not permitted. [dB (AI) = A-weighted impulse sound pressure level in decibels; dB (C) pk = C-weighted peak sound pressure in decibels].
4. Permissible Noise Levels (Central Pollution Control Board, India):
- Industrial Areas: 75 dB (day), 70 dB (night).
- Residential Areas: 55 dB (day), 45 dB (night).
- Commercial Areas: 65 dB (day), 55 dB (night).

Management / Treatment
- Hearing Protection: Further noise exposure should be minimised using ear protection devices in the form of earplugs or earmuffs. It reduces the further risk of NIHL.
- Hearing Aids: Beneficial for managing severe, permanent hearing loss, though they cannot restore lost hearing. Cochlear implants are used for profound hearing loss unresponsive to hearing aids.
- Medical management: Corticosteroids (e.g., prednisolone) are the mainstay of medical management for acute acoustic trauma, ideally started within 24–48 hours. Some studies have explored the use of piracetam as an adjunct, but the evidence is limited, and it is not widely recommended as first-line therapy.
- Tinnitus Management: Tinnitus Retraining Therapy (TRT) combines cognitive counselling and sound therapy, showing improvement in 60-70% of patients.
- Hyperacusis Management: Similar to tinnitus, using sound therapy and counselling.
- Acoustic Shock: Requires psychological treatment.
Nonauditory Effects of Noise
- Sleep disturbances lead to chronic fatigue and stress.
- Hypertension and tachycardia
- Annoyance and irritability.
- Decreased performance at work and memory loss.
- Mood disturbances and behavioural changes
Other related terminologies
1. Early Onset Presbycusis: It is premature age-related hearing loss, typically occurring earlier than expected due to cumulative noise exposure from childhood. Chronic exposure to loud sounds can damage the cochlea, leading to early degeneration of hair cells and auditory structures.
2. Socioacusis (Non-Occupational Noise-Induced Hearing Loss): Hearing loss caused by non-occupational noise exposure, often from recreational or lifestyle activities.
Common Sources:
- Loud Music: Concerts, music shows, and personal entertainment devices (e.g., headphones, earbuds) played at high volumes.
- Open Vehicles: Motorcycles, snowmobiles, all-terrain vehicles, and Formula One racing cars.
Clinical Findings:
- High-Frequency SNHL: Audiometric testing reveals a characteristic dip at 4–6 kHz.
- Tinnitus: Often accompanies hearing loss.
- Hyperacusis: Increased sensitivity to certain sound frequencies.
———— End of the chapter ————
High-Yield Points for Quick Revision
- NIHL is preventable. Focus on protection and awareness.
- Types: Temporary Threshold Shift (TTS) is reversible (metabolic changes), Permanent Threshold Shift (PTS) is irreversible (structural damage, e.g., hair cell apoptosis).
- Acoustic Trauma: Single, intense exposure (>140 dB SPL), immediate damage (e.g., TM perforation, ossicle damage), no preceding TTS.
- Most Damaging Frequencies: 2–3 kHz range.
- Safe Limit: Sounds below 80 dB(A) are generally safe. Immediate damage above 130 dB(A).
- Diagnosis Gold Standard: Pure Tone Audiometry (PTA) showing a 4–6 kHz notch (bilateral, symmetrical, with recovery at 8 kHz).
- Reasons for 4 kHz Notch: Basal turn rigidity, muscle reflex shifting sound energy, external auditory canal resonance.
- Hearing Protection Devices (HPDs): Earplugs (15-30 dB), Earmuffs (30-40 dB), Combined (>40 dB).
- Indian Regulations (Key numbers to remember):
- PEL: 90 dB(A) for 8 hours (Factories Act).
- 5 dB Rule: Halves exposure time for every 5 dB rise.
- Firecracker Limit: >125 dB(AI) or 145 dB(C) pk from 4m distance prohibited.
- Silence Zone: 100m around hospitals/schools.
- Night time loudspeaker ban: 10 PM to 6 AM.
- Nonauditory Effects: Sleep disturbance, hypertension, annoyance, decreased performance.
- Socioacusis: NIHL from non-occupational/recreational sources.
- Mnemonic for Personal Noise Prevention (60-60-60 Rule): ≤60% maximum volume for ≤60 minutes per day at ≤60 dB.
MCQ’s NEET PG-style
Practice these questions to reinforce your learning and prepare for competitive exams.
- A 35-year-old factory worker presents with a gradual onset of bilateral hearing loss and tinnitus. His audiogram shows a symmetrical dip at 4 kHz with recovery at 8 kHz. Which of the following is the most likely diagnosis? A) Presbycusis B) Otosclerosis C) Noise-induced hearing loss D) Meniere’s disease
- Which of the following noise exposure levels can cause immediate and irreversible hearing damage? A) 70 dB(A) B) 85 dB(A) C) 110 dB(A) D) 140 dB(A)
- Temporary Threshold Shift (TTS) is characterised by: A) Permanent structural damage to outer hair cells B) Immediate, irreversible hearing loss C) Hearing loss that recovers within a few days after noise exposure D) Mechanical damage to the tympanic membrane
- According to the Ministry of Labour, Govt. of India, Model Rules under Factories Act, what is the Permissible Exposure Limit (PEL) for noise for an 8-hour workday? A) 75 dB(A) B) 80 dB(A) C) 90 dB(A) D) 100 dB(A)
- The characteristic “notch” in noise-induced hearing loss is typically seen at which frequency range on a pure-tone audiogram? A) 500 Hz to 1 kHz B) 1 kHz to 2 kHz C) 4 kHz to 6 kHz D) 8 kHz to 10 kHz
- Which of the following is considered a non-auditory effect of chronic noise exposure? A) Tinnitus B) Hyperacusis C) Hypertension D) Diplacusis
- A single exposure to an extremely intense sound, such as an explosion, causing immediate hearing loss, is termed: A) Temporary Threshold Shift B) Socioacusis C) Acoustic Trauma D) Early Onset Presbycusis
- Which factor is least likely to influence the extent of hearing damage from noise exposure? A) Frequency of noise B) Intensity of noise C) Individual’s blood group D) Duration of noise exposure
- A 100-meter radius around hospitals, nursing homes, and educational institutions is designated as a “Silence Zone” according to which Indian legislation? A) Environment Protection Rules 2006 B) Ministry of Labour, Model Rules under Factories Act C) Noise Pollution (Regulation and Control) Rules 2000 D) Bureau of Indian Standards (BIS) Guidelines
- The 5 dB rule of time-intensity in noise exposure regulations implies that if the noise level increases by 5 dB, the permitted noise exposure time will: A) Double B) Remain the same C) Be reduced to half D) Be reduced by 5 hours
MCQ Answers and Explanations:
- C) Noise-induced hearing loss. The classic 4 kHz notch, bilateral presentation, and history of occupational exposure strongly point to NIHL.
- D) 140 dB(A). Exposure above 130 dB(A), especially impulse noise above 140 dB(A), can cause immediate and permanent damage (acoustic trauma).
- C) Hearing loss that recovers within a few days after noise exposure. TTS is a temporary physiological change, not permanent structural damage.
- C) 90 dB(A). This is the standard Permissible Exposure Limit for an 8-hour workday in industrial settings in India.
- C) 4 kHz to 6 kHz. The characteristic “notch” or “dip” in NIHL audiograms is consistently found in this high-frequency range, with the deepest point often at 4 kHz or 6 kHz.
- C) Hypertension. Tinnitus and hyperacusis are auditory effects. Hypertension is a well-documented non-auditory (physiological) effect of chronic noise exposure. Diplacusis is also an auditory phenomenon.
- C) Acoustic Trauma. Acoustic trauma is specifically defined as immediate hearing loss due to a single, intense sound event.
- C) Individual’s blood group. While genetic factors and pre-existing conditions can influence susceptibility, an individual’s blood group is not currently recognized as a factor influencing the extent of noise-induced hearing damage.
- C) Noise Pollution (Regulation and Control) Rules 2000. This legislation specifically designates and regulates silence zones.
- C) Be reduced to half. This is a fundamental principle in occupational noise exposure regulations, emphasizing the exponential increase in risk with increasing sound intensity.
Clinical-Based Questions
1. Scenario: A 50-year-old male, working as a heavy machinery operator for 25 years without consistent hearing protection, complains of gradually worsening hearing, especially in noisy environments, and persistent high-pitched ringing in both ears. He denies vertigo or ear discharge. On examination, both tympanic membranes are normal.
- Diagnosis: What is your working diagnosis, and what specific hearing test would be critical to confirm it?
- Audiogram Expectation: Describe the expected audiometric findings for this patient.
- Management: Outline your initial management plan.
- Viva Tips: The examiner asks, “How would you counsel this patient regarding their condition?”
Answer:
- Diagnosis: Noise-induced hearing loss (NIHL). The history of prolonged occupational noise exposure, gradual bilateral hearing loss, and tinnitus are highly suggestive.
- Critical Hearing Test: Pure Tone Audiometry (PTA) is critical to confirm.
- Audiogram Expectation: The audiogram would likely show a bilateral, symmetrical sensorineural hearing loss (SNHL) with a characteristic “notch” or “dip” at 4 kHz or 6 kHz, and some recovery at 8 kHz. Lower frequencies might be relatively preserved initially.
- Management:
-
- Mandatory Hearing Protection: Emphasize immediate and consistent use of appropriate hearing protection (earplugs and/or earmuffs) at work and in other noisy environments to prevent further progression.
- Audiological Assessment: Refer for comprehensive audiological evaluation, including PTA, speech audiometry, and OAEs, to precisely quantify the hearing loss and assess outer hair cell function.
- Hearing Aids: Counsel on the benefits and fitting of hearing aids as the primary rehabilitative measure.
- Tinnitus Management: Discuss options for tinnitus management, such as sound therapy, TRT, or counseling.
- Occupational Health Referral: Advise referral to an occupational health specialist for workplace assessment and potential compensation.
-
Viva Tips (Patient Counselling): “Mr. [Patient’s Name], based on your history of working with loud machinery for many years and our initial findings, it appears you have noise-induced hearing loss. This is a common condition that occurs when the delicate structures in your inner ear get damaged by prolonged exposure to loud sounds. Unfortunately, this type of hearing loss is generally permanent, meaning we cannot reverse the damage. However, we can certainly prevent it from getting worse and significantly improve your ability to hear and communicate. The most important step now is to use hearing protection diligently whenever you are in noisy environments. We will also perform more detailed hearing tests to determine the exact extent of your loss and discuss options like hearing aids, which can amplify sounds and make your daily life much easier. We can also explore strategies to manage your tinnitus.”
2. Scenario: A young adult presents to the emergency department with sudden, severe hearing loss and ringing in their right ear immediately after a firecracker exploded very close to them. They also report mild ear pain but no bleeding.
- Diagnosis: What is the most appropriate immediate diagnosis?
- Examination & Test: What key finding would you look for on otoscopy, and what single most relevant hearing test would you order immediately?
- Initial Management: What is the immediate medical management to optimize hearing recovery?
Answer:
- Diagnosis: Right Acoustic Trauma. The sudden, severe hearing loss immediately after an intensely loud impulse noise (firecracker) is characteristic.
- Examination & Test:
- Key Otoscopic Finding: You would specifically look for a tympanic membrane perforation (hole in the eardrum), which is common with acoustic trauma due to mechanical forces. You would also check for hemotympanum.
- Relevant Hearing Test: Immediate Pure Tone Audiometry (PTA) to quantify the sudden hearing loss and determine its type (usually SNHL, but can be mixed if TM/ossicles are damaged).
-
Initial Management:
-
- Steroids: High-dose oral corticosteroids (e.g., Prednisolone) for 7-10 days, ideally started within 24-48 hours of onset, to reduce inflammation and potentially improve cochlear recovery. Intratympanic steroids may also be considered.
- Absolute Noise Protection: Advise strict avoidance of any further noise exposure.
- Tympanic Membrane Management: If perforated, advise against ear irrigation and refer for ENT follow-up; most traumatic perforations heal spontaneously.
- Counselling: Provide reassurance and explain the nature of acoustic trauma.
3. Scenario: During a practical ENT exam, you are presenting a case of a patient with suspected NIHL. The examiner asks, “Explain the ‘5 dB rule’ related to noise exposure in industrial settings.”
- Explanation: Provide a clear, concise explanation of the 5 dB rule and its practical implications.
- Practical Tip: How would you advise a safety officer based on this rule?
Answer:
- Explanation: “Sir/Madam, the ‘5 dB rule of time-intensity’ is a fundamental principle in occupational noise exposure regulations. It states that for every increase of 5 dB in noise level, the permissible exposure time for workers must be halved. This rule reflects the non-linear relationship between noise intensity and the risk of hearing damage – a small increase in decibels represents a significant increase in sound energy. For example, if the Permissible Exposure Limit (PEL) is 90 dB(A) for 8 hours, then 95 dB(A) is only allowed for 4 hours, 100 dB(A) for 2 hours, and so on.”
- Practical Tip (Advice to Safety Officer): “Based on this rule, Mr./Ms. Safety Officer, you must understand that even a seemingly small increase in machinery noise can drastically reduce the safe working hours for your employees. Therefore, you should:
- Prioritise noise reduction at the source wherever possible.
- Implement strict monitoring of noise levels across all shifts.
- Ensure appropriate hearing protection devices are available and consistently used by all workers.
- Actively manage exposure durations for workers in high-noise areas through job rotation or scheduled breaks, strictly adhering to the 5 dB rule calculations to prevent cumulative damage.”
Frequently Asked Questions in Viva
These FAQs are optimised for Google Rich Snippets, offering concise and direct answers.
- What is noise-induced hearing loss (NIHL)? NIHL is a type of hearing impairment caused by prolonged or intense exposure to loud sounds, leading to damage to the delicate structures of the inner ear.
- What is the difference between Temporary Threshold Shift (TTS) and Permanent Threshold Shift (PTS)? TTS is a temporary and reversible hearing loss that recovers within days after noise exposure, whereas PTS is a permanent and irreversible hearing loss due to structural damage from repeated or severe noise exposure.
- Why does noise-induced hearing loss often show a “notch” at 4-6 kHz on an audiogram? The 4-6 kHz region of the cochlea is particularly vulnerable to noise damage due to its anatomical rigidity, the filtering effect of the middle ear muscles, and resonance in the external auditory canal.
- What are the primary preventive measures for noise-induced hearing loss in industrial settings? Key measures include pre-employment and annual audiograms, noise regulation, worker training, job rotation, and consistent use of hearing protection devices like earplugs and earmuffs.
- What is “acoustic trauma”? Acoustic trauma is immediate hearing loss caused by a single exposure to an extremely intense sound, such as an explosion or gunfire, which can result in mechanical damage to ear structures.
- What non-auditory effects can noise have on health? Beyond hearing loss, chronic noise exposure can lead to sleep disturbances, hypertension, irritability, decreased work performance, and mood disturbances.
- What is “Socioacusis”? Socioacusis refers to hearing loss resulting from non-occupational noise exposure, commonly from recreational activities like loud music, concerts, or motorsports.
———— End ————
Download the full PDF Link:
Noise Induced Trauma Best Lecture Notes Dr Rahul Bagla ENT Textbook
Download PPT:
Noise Induced Hearing Loss Best PPT Notes Lectures Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Noise induced trauma, Noise-induced hearing loss (NIHL), Acoustic trauma, Hearing loss from loud noise, Sound-induced hearing damage, Noise-related ear damage, Sensorineural hearing loss, Exposure to loud noise, Industrial noise hearing loss, Occupational hearing damage, Recreational noise-induced hearing loss, Ear trauma due to sound, Causes of noise-induced hearing loss, Symptoms of noise-induced ear trauma, Prevention of noise-related hearing damage, Treatment for noise-induced hearing loss, Noise levels causing hearing damage, Hearing protection from loud noise, Auditory trauma, Noise exposure hearing damage, Decibel damage to ears Hearing sensitivity and noise, Loud sound ear injury, High-decibel ear trauma, Temporary threshold shift (TTS), Permanent threshold shift (PTS), Cochlear damage from noise, Inner ear damage due to sound exposure, Noise-induced cochlear trauma, Effects of noise pollution on hearing, Hearing loss prevention tips, Best ear protection for noise, Noise safety and hearing health, Risk of hearing loss in noisy environments