Speech audiometry. (Assessing Hearing Ability and Speech Comprehension). Speech audiometry is an essential tool for evaluating a patient’s hearing ability and understanding of spoken words. The results of this test are plotted on a graph. The test is also useful for detecting retrocochlear pathology and non-organic hearing loss.
- Speech Reception Threshold (SRT): Also known as the Speech-awareness threshold (SAT), SRT is the lowest speech intensity at which a patient can correctly repeat or detect 50% of the words.
- Procedure: The test involves delivering recorded tapes or monitored voice of spondee words (two-syllable words with equal stress on each syllable, such as “pancake,” “hardware,” “playground”) through headphones or speakers in a soundproof room. The intensity of these words is varied in 5 dB steps until the patient correctly identifies half of them.
- Interpretation and Reliability: For a normal adult, the SRT should be within 10 dB of the pure tone average (500, 1000, and 2000 Hz). An SRT that is better than the pure tone average by more than 10 dB suggests functional hearing loss or an unreliable pure tone audiogram.
- Speech Discrimination Score (SDS):
- Also known as the speech recognition or word recognition score, SDS measures the patient’s ability to understand speech clearly.
- A list of 25 to 50 phonetically balanced words (single-syllable words such as “pin,” “sin,” “day,” “bus”) is presented to each ear separately at 30–40 dB above the patient’s SRT using pre-recorded material.
- The percentage of words correctly identified by the patient is recorded.
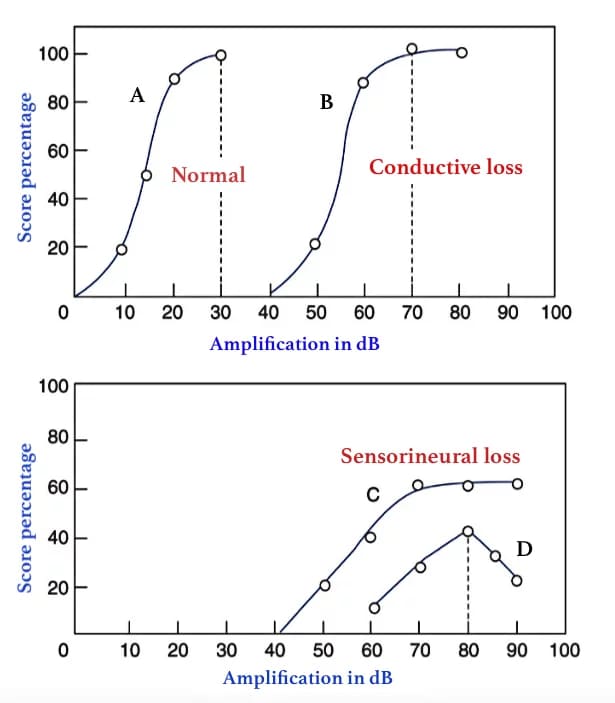
- In normal hearing and conductive hearing loss, a high score of 90–100% is typical.
Table : Ability to understand speech and its relation to speech discrimination (SD) score. A list of 50 PB words is presented and the number correctly heard is multiplied by 2 the number
| SD score | Ability to understand speech |
| 90–100% | Normal (Excellent) |
| 76–88% | Slight difficulty (Good) |
| 60–74% | Moderate difficulty (Fair) |
| 40–58% | Poor |
| <40% | Very poor |
Interpretation of Speech Discrimination Scores
- Conductive Hearing Loss: Patients typically show improved recognition scores when the speech signal intensity is increased.
- Sensorineural Hearing Loss: Patients usually do not show improved recognition scores with increased intensity because louder sounds can distort the speech signal.
- Retrocochlear Pathology: Patients may exhibit a reduction in recognition scores with increased intensity, known as the “rollover” effect, which suggests a lesion in the eighth cranial nerve. In this scenario, as speech intensity increases beyond a certain level, the word recognition score declines rather than stabilizing as it does in cochlear sensorineural hearing loss.
Performance Intensity Function for PB Words
- PB Max: It is beneficial to plot PB scores against various speech intensity levels to determine the maximum score (PB max) a person can achieve, rather than using a single suprathreshold intensity of 30–40 dB above the SRT. The intensity at which PB max is achieved is noted, and the maximum volume of a hearing aid should be set below this level.
Benefits of speech audiometry :
- To measure the speech reception threshold which determines actual disability & not hearing impairment.
- To differentiate organic from nonorganic(functional) hearing loss.
- To find the intensity at which a hearing aid/cochlear implants fits and assessing rehabilitation outcome.
- To differentiate a cochlear from a retrocochlear sensorineural hearing loss.
———— End of the chapter ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/