|
The following CBME core competencies are covered in this chapter.
|
Tinnitus: Causes, Diagnosis & Treatment
Definition: What is Tinnitus?
The word tinnitus is derived from the Latin word tinnire, which means “to ring.” Tinnitus is the perception of sound in the absence of an external acoustic stimulus. It is a symptom rather than a disease and indicates an underlying disorder affecting the ear, auditory pathway, or, less commonly, the central nervous system.
Patients commonly describe tinnitus as ringing, but the perceived sound may also be buzzing, humming, hissing, roaring, clicking, chirping, whistling, rustling, swishing, machinery noise, or even music. The sound may be heard in one ear, both ears, or within the head and may be continuous or intermittent.
Tinnitus may be unilateral or bilateral. Bilateral tinnitus is more common and is usually associated with age-related or noise-induced hearing loss. However, unilateral tinnitus, especially when accompanied by asymmetric sensorineural hearing loss or neurological symptoms, warrants further evaluation to exclude retrocochlear pathology, such as vestibular schwannoma. Patients often notice that tinnitus becomes more bothersome at night because reduced environmental noise makes the internally generated sound more noticeable.
Although tinnitus is rarely life-threatening, persistent symptoms can significantly impair concentration, sleep, emotional well-being, work performance, and overall quality of life. Therefore, every patient should undergo a systematic evaluation to identify the underlying cause and receive appropriate counselling and evidence-based management.
This chapter provides a comprehensive, CBME-aligned review of tinnitus, covering its classification, causes, pathophysiology, clinical evaluation, red flag features, investigations, MRI indications, treatment options, cognitive behavioural therapy (CBT), tinnitus retraining therapy (TRT), high-yield revision points, viva questions, clinical cases, and NEET PG-style MCQs.
Epidemiology
Approximately 10–15% of adults experience tinnitus, while only 1–2% have severe symptoms affecting quality of life. More than 95% of tinnitus cases are subjective, non-pulsatile tinnitus, which is usually associated with sensorineural hearing loss, particularly presbycusis and noise-induced hearing loss. In contrast, pulsatile tinnitus is a red flag because it often suggests an underlying vascular abnormality until proven otherwise.
The prevalence increases among individuals with:
- Age-related hearing loss
- Occupational noise exposure
- Military personnel
- Factory workers
- Musicians
- Patients receiving ototoxic medications.
Risk Factors of Tinnitus
- Increasing age
- Hearing loss
- Noise exposure
- Ototoxic medications (aminoglycosides, cisplatin, loop diuretics, salicylates)
- Ear diseases. Meniere’s disease, otosclerosis, vestibular schwannoma.
- History of head injuries, cardiovascular disease and hypertension.
- Smoking
- Alcohol intake
- Anxiety
- Temporomandibular joint (TMJ) dysfunction
Pathophysiology of Tinnitus
Understanding the pathophysiology of tinnitus helps explain why many patients continue to hear sounds even when no external sound is present. Normally, sound waves travel through the external ear, middle ear, and cochlea, where they are converted into electrical impulses. These impulses travel via the auditory nerve to the brainstem, thalamus, and finally the auditory cortex, where they are perceived as sound.
In many patients, tinnitus begins after damage to the cochlea, most commonly due to age-related hearing loss, noise exposure, or ototoxic drugs. As a result, the cochlea sends fewer signals to the brain. Instead of simply accepting this reduced input, the brain compensates by increasing the sensitivity (central gain) and spontaneous activity of neurons within the auditory pathway. The brain then interprets this abnormal neural activity as sound, even though no external sound is present.
An easy way to understand this is to compare tinnitus with phantom limb pain. Just as an amputee may continue to feel pain in a missing limb, the brain can continue to perceive sound despite reduced or absent auditory input. Therefore, tinnitus is often described as a phantom auditory perception. This also explains why hearing aids often reduce tinnitus by restoring auditory input and reducing central neural gain.
Types of Tinnitus
By perception
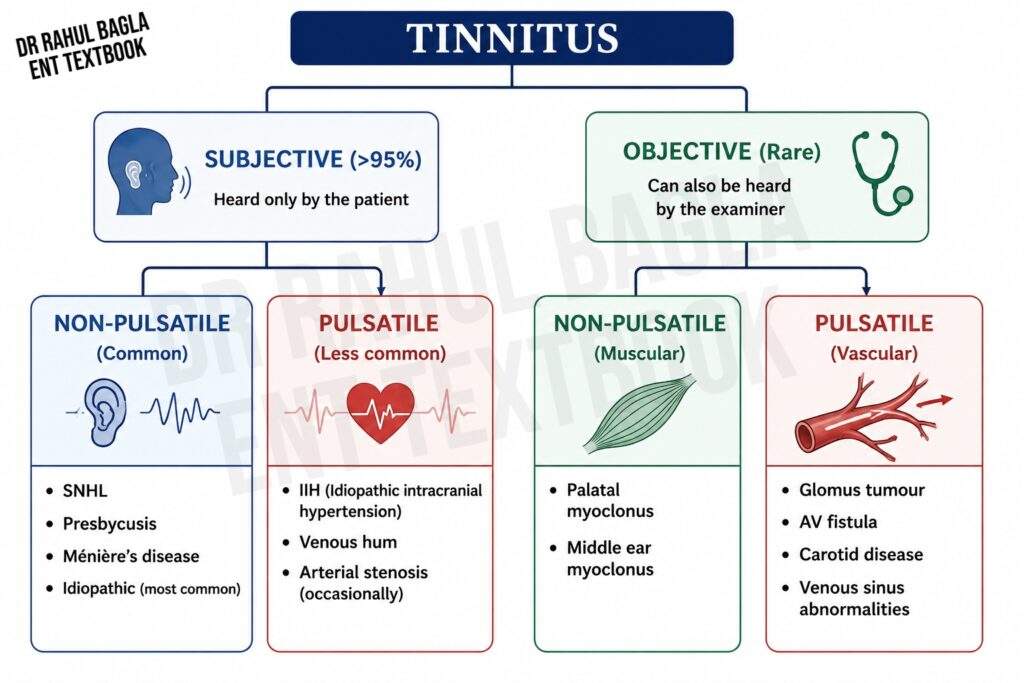
- Subjective tinnitus: Heard only by the patient. Accounts for >95% of cases. Usually associated with hearing loss or cochlear pathology.
- Objective tinnitus: Rare. Can also be heard by the examiner. Usually due to vascular abnormalities or muscular contractions.
By sound character
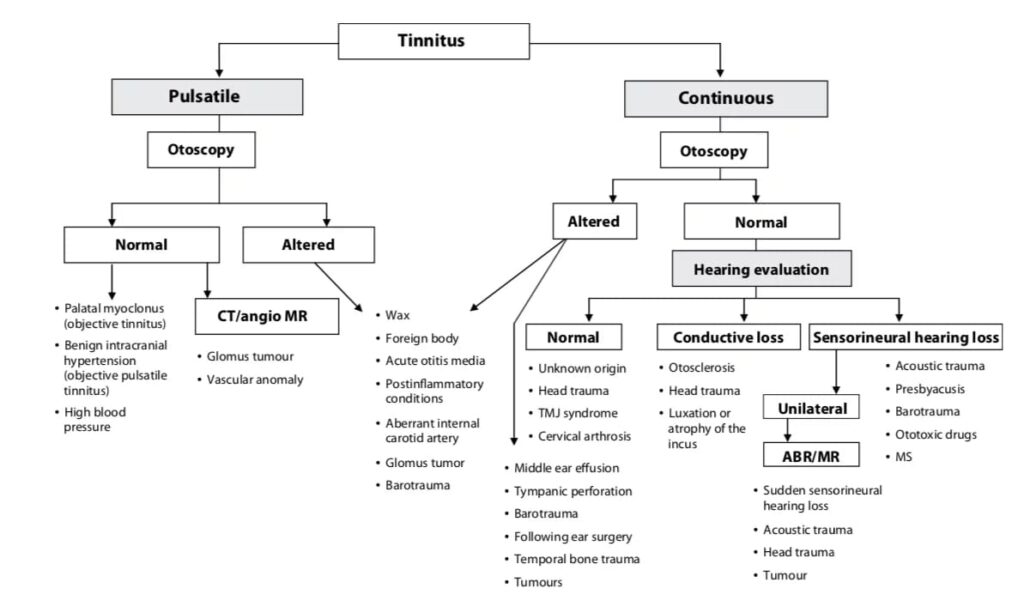
- Pulsatile tinnitus: May be pulse-synchronous or non-pulse-synchronous. Pulse-synchronous tinnitus is usually vascular in origin.
- Non-pulsatile tinnitus: Most commonly associated with sensorineural hearing loss.
The most common presentation of tinnitus is subjective non-pulsatile tinnitus with no associated disease other than presbycusis: this is also known as subjective idiopathic tinnitus. Descriptions of sounds can be in any form, such as humming, whistling, voices, music, or ringing sounds.
Functional (Psychogenic) Tinnitus
It is commonly associated with psychiatric disorders such as anxiety, depression and somatisation. It should be differentiated from auditory hallucinations, in which the patient perceives voices or organised sounds such as music. No structural otological or neurological cause is identified after appropriate evaluation.
Causes of Tinnitus
A. By Perception
| Feature | Subjective Tinnitus (>95%) | Objective Tinnitus (Rare) |
| Definition | Heard only by the patient | Heard by both the patient and the examiner |
| Underlying mechanism | Abnormal activity within the cochlea or auditory pathway; no external sound source | Actual sound is generated within or around the ear |
| Common causes | Otological: Cerumen impaction, Otitis media, Presbycusis, Noise-induced hearing loss, Ménière’s disease, Sudden SNHL, Vestibular schwannoma Metabolic/Endocrine: Vitamin B12 deficiency, Diabetes mellitus, Thyroid disorders, Hyperlipidaemia Neurological: Head injury, Temporal bone fracture, Multiple sclerosis, Brainstem lesions, Stroke Cardiovascular: Hypertension, Hypotension, Anaemia, Cardiac arrhythmias Drugs (Ototoxic): Aminoglycosides, Cisplatin, Loop diuretics, Salicylates, Quinine Psychological: Anxiety, Depression, Stress |
Vascular: Glomus tumour, AV malformation/fistula, Carotid stenosis, Carotid aneurysm, Persistent stapedial artery, Aberrant internal carotid artery, Venous hum, High-riding jugular bulb Muscular: Palatal myoclonus, Middle ear myoclonus (Stapedius/Tensor tympani) Patulous Eustachian tube Mechanical: TM joint clicking, Dental malocclusion |
| Typical sound | Ringing, Buzzing, Hissing, Roaring, Whistling | Pulsating, Clicking, Fluttering, Thumping, Swishing |
| Clinical clue | Usually associated with sensorineural hearing loss | Usually due to vascular or muscular pathology |
B. By Sound Character
| Feature | Pulsatile Tinnitus | Non-pulsatile Tinnitus |
| Definition | Rhythmic sound, often synchronous with heartbeat | Continuous or intermittent non-rhythmic sound |
| Mechanism | Usually caused by vascular abnormalities; occasionally, muscular contractions | Usually due to cochlear or auditory pathway dysfunction |
| Pulse-synchronous causes | Idiopathic intracranial hypertension, Glomus tumour, AV malformation/fistula, Carotid stenosis, Carotid aneurysm, Persistent stapedial artery, Aberrant internal carotid artery, Venous hum, High-riding jugular bulb, Sigmoid sinus abnormalities, Pregnancy, Anaemia, Thyrotoxicosis | — |
| Non-pulse-synchronous causes | Palatal myoclonus, Middle ear myoclonus (Stapedius/Tensor tympani) | Presbycusis, Noise-induced hearing loss, Ménière’s disease, Sudden SNHL, Vestibular schwannoma, Idiopathic tinnitus (most common), Spontaneous otoacoustic emissions, Patulous Eustachian tube |
| Typical sound | Pulsating, Whooshing, Thumping | Ringing, Buzzing, Hissing, Roaring, Whistling |
| Clinical importance | Red flag – vascular causes should be excluded | Most common form; usually associated with sensorineural hearing loss |
Red Flag Features in Tinnitus
The following features require prompt evaluation:
- Unilateral tinnitus
- Pulsatile tinnitus
- Sudden sensorineural hearing loss
- Asymmetric hearing loss
- Associated vertigo or neurological deficits
- Persistent unilateral middle ear effusion
Persistent unilateral tinnitus, particularly when associated with asymmetric sensorineural hearing loss, should raise suspicion for retrocochlear pathology such as vestibular schwannoma and warrants MRI evaluation.
Assessment of a Patient
History
- Tinnitus: Unilateral/ Bilateral, Constant/ Intermittent – If intermittent, duration & frequency of episodes, aggravating or relieving factors.
- H/o Hearing loss, discharge or ear surgery, loud sound, giddiness, ototoxic drugs, head trauma or any other systemic illness.
- Personal history: Smoking, alcohol, caffeine intake and use of ototoxic medications.
- Occupational History.
- Family history of hearing loss.
- Sleep disturbance and its effect on quality of life.
Clinical examination
- Inspection of the ears to look for any congenital anomalies or scars indicating trauma or surgery.
- Look for tympanic membrane perforation, middle ear effusion/fluid, cholesteatoma or any vascular lesion.
- Tuning fork tests.
- Cranial nerves examination.
- Auscultation of the neck, temporal and mastoid regions for bruits (vascular lesions) is required in cases of pulsatile tinnitus.
- Examine the temporomandibular joint and cervical spine in selected patients.
Investigations
- Pure Tone Audiometry: To assess the type and degree of hearing loss.
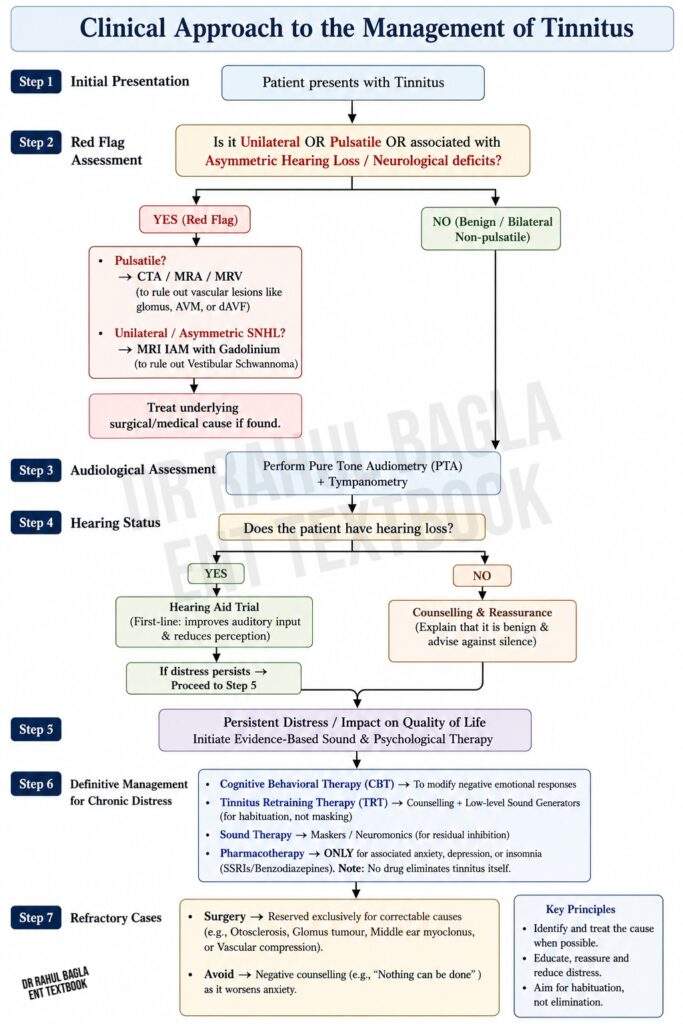
- MRI: MRI with gadolinium contrast of the internal auditory canals and brain is indicated in patients with unilateral tinnitus, asymmetric sensorineural hearing loss or neurological deficits to exclude vestibular schwannoma and other retrocochlear pathology. Routine imaging is not recommended in patients with bilateral, non-pulsatile tinnitus associated with symmetrical hearing loss and a normal neurological examination.
- Tympanometry and stapedial reflexes are done to diagnose any middle ear pathology present, such as tensor tympani or stapedial myoclonus.
- Otoacoustic emissions (OAE): Performed when cochlear pathology is suspected.
- Auditory brainstem response (ABR/BERA): Performed when retrocochlear pathology is suspected.
- CTA/MRA/MRV: Performed in patients with pulsatile tinnitus when a vascular cause is suspected.
- Blood investigations: Performed only when clinically indicated (e.g. anaemia, thyroid dysfunction or metabolic disorders).
Management
1. Identify and treat the underlying cause
2. Psychological: Education, reassurance, counselling and cognitive behavioural therapy (CBT) are the most effective evidence-based interventions for reducing tinnitus-related distress. Patients are taught habituation strategies and advised to avoid negative counselling (e.g. “nothing can be done”), which increases anxiety. Biofeedback may benefit selected patients.
3. Medical: No medication has been consistently shown to eliminate tinnitus. Benzodiazepines or antidepressants (particularly SSRIs) may be prescribed only for associated anxiety, depression or sleep disturbance rather than for tinnitus itself.
4. Complementary medicine regimes: Ginkgo biloba, combination supplements, acupuncture, aromatherapy, ear candles, hypnotherapy, meditation, reflexology, tai chi and yoga sessions are utilised as relaxation techniques. Current evidence does not support the routine use of Ginkgo biloba, acupuncture or dietary supplements for tinnitus treatment.
5. Devices to mask tinnitus
- Hearing aids. In patients with hearing loss, hearing aids often reduce the perception of tinnitus by improving auditory input.
- Tinnitus maskers resemble hearing aids and deliver continuous low-level broadband noise (white noise or narrowband noise) to partially or completely cover the patient’s perception of tinnitus. Some patients may experience residual inhibition—a temporary reduction or suppression of tinnitus following exposure to the masking sound—, but this is variable and not the primary mechanism of action. Maskers are particularly useful in patients with normal hearing or those who do not benefit from hearing aids.
- The Tinnitus instrument combines a hearing aid and a masker in a single device.
- Novel sound device. Neuromonics is a sound therapy device that delivers music of a large dynamic range with peaks and troughs. The tinnitus sound is audible in troughs.
6. Tinnitus retraining therapy
- Tinnitus retraining therapy aims to achieve habituation, thereby reducing both the emotional and attentional responses to tinnitus so that it is no longer consciously perceived as bothersome. TRT does not eliminate the tinnitus itself.
- Helps people to manage the impact of tinnitus on their day-to-day life.
- Therapy consists of Counselling and Sound therapy. Patient is exposed to environmental sounds, music, radio, television, or the use of hearing aids (in case he suffers from hearing loss). In general, he should avoid a silent environment. To produce external sound for habituation, sound generators are used, which produce continuous low-level, broadband noise for at least 8 h a day. Sound, here, is used not for masking the tinnitus but is adjusted to remain at a low level, for habituation. TRT needs a long period of 18–24 months but gives a significant improvement in more than 80% of patients.
7. Surgery
Surgery has no role in routine subjective tinnitus. It is reserved for selected patients with surgically correctable causes such as vestibular schwannoma, otosclerosis, middle ear myoclonus, glomus tumours, arteriovenous malformations, dural arteriovenous fistulas or, rarely, vascular compression syndromes requiring microvascular decompression.
Summary table
| Tinnitus Subtype | Key Feature | Investigation | Management |
| Subjective, non-pulsatile | Most common; associated with hearing loss | Pure-tone audiometry (PTA) | Hearing aids, Cognitive behavioural therapy (CBT), Tinnitus retraining therapy (TRT) |
| Subjective, unilateral | Red flag; suspect retrocochlear pathology | MRI of the internal auditory meatus (MRI IAM) | Treat the underlying cause |
| Pulsatile | Synchronous with pulse; usually vascular in origin | CT angiography (CTA), MR angiography (MRA), MR venography (MRV) | Treat the underlying vascular lesion |
| Objective | Audible to the examiner | Auscultation ± targeted imaging | Treat the underlying cause (e.g. glomus tumour, myoclonus) |
———— End of the chapter ————
High Yield Points
- Subjective, non-pulsatile tinnitus accounts for more than 95% of cases and is most commonly associated with sensorineural hearing loss (especially presbycusis).
- Pulsatile tinnitus is vascular until proven otherwise.
- Red flags: Unilateral tinnitus, pulsatile tinnitus, asymmetric sensorineural hearing loss, sudden sensorineural hearing loss, and associated neurological deficits.
- Investigation of choice for unilateral tinnitus with asymmetric SNHL: MRI of the internal auditory meatus (IAM) with gadolinium to exclude vestibular schwannoma.
- Investigation of choice for pulsatile tinnitus: CTA, MRA, or MRV, depending on the suspected vascular lesion.
- Cognitive behavioural therapy (CBT) has the strongest evidence for reducing tinnitus-related distress.
- Tinnitus retraining therapy (TRT) combines counselling with sound therapy to achieve habituation; it does not eliminate tinnitus.
- No medication has been consistently shown to cure chronic subjective tinnitus.
- Routine imaging is not recommended for patients with bilateral non-pulsatile tinnitus, symmetrical hearing loss, and a normal neurological examination.
MCQ’s
- The most common type of tinnitus is: A. Objective pulsatile tinnitus B. Subjective non-pulsatile tinnitus C. Objective non-pulsatile tinnitus D. Pulsatile vascular tinnitus.
- The strongest risk factor for developing tinnitus is: A. Diabetes mellitus B. Sensorineural hearing loss C. Chronic otitis media D. Smoking.
- A 52-year-old patient presents with unilateral tinnitus and asymmetric sensorineural hearing loss. The most appropriate investigation is: A. X-ray mastoid B. CT temporal bone C. MRI of the internal auditory meatus (IAM) with gadolinium D. Tympanometry.
- Pulsatile tinnitus should primarily raise suspicion of: A. Cochlear otosclerosis B. Vascular pathology C. Presbycusis D. Noise-induced hearing loss.
- Which of the following is an example of objective tinnitus? A. Presbycusis B. Glomus tumour C. Noise-induced hearing loss D. Ménière disease.
- Which investigation is recommended as the first-line hearing assessment in most patients with tinnitus? A. Brainstem Evoked Response Audiometry (BERA) B. Pure Tone Audiometry (PTA) C. Otoacoustic Emissions (OAE) D. Electrocochleography.
- The most effective evidence-based treatment for reducing tinnitus-related distress is: A. Ginkgo biloba B. Betahistine C. Cognitive behavioural therapy (CBT) D. Corticosteroids.
- Which statement regarding tinnitus retraining therapy (TRT) is TRUE? A. It eliminates tinnitus completely B. It combines counselling with sound therapy to promote habituation C. It is useful only in objective tinnitus D. It usually produces complete relief within 2 weeks.
- Which one of the following is NOT considered a red flag in tinnitus? A. Pulsatile tinnitus B. Sudden sensorineural hearing loss C. Bilateral tinnitus associated with symmetrical age-related hearing loss D. Unilateral tinnitus with asymmetric hearing loss.
- Which of the following drugs is well known to cause ototoxic tinnitus? A. Amoxicillin B. Metformin C. Gentamicin D. Omeprazole.
Answers: 1: B. 2: B. 3: C. 4: B. 5: B. 6: B. 7: C. 8: B. 9: C. 10: C.
———— End ————
Download full PDF Link:
Tinnitus Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Ringing, buzzing, hissing, or clicking sounds in head, Tinnitus retraining therapy (TRT), Biofeedback, Noise Complaints, Tinnitus, Tinnitus cause, Tinnitus cure, Tinnitus sound, Tinnitus treatment, Tinnitus home treatment, Tinnitus causes and remedies, Natural tinnitus relief, Tinnitus management tips, Tinnitus and sleep problems, How to stop ringing in ears naturally, Tinnitus diet recommendations, Tinnitus stress connection, Tinnitus treatment exercises, Home remedies for tinnitus, Tinnitus prevention techniques, Chronic tinnitus symptoms, Vitamins for tinnitus relief, Yoga for tinnitus sufferers, Tinnitus sound therapy guide, Understanding pulsatile tinnitus