|
The following CBME core competencies are covered in this chapter.
|
Embryology of the Ear: A Comprehensive Guide for MBBS and ENT PG Students
The development of the ear is a fascinating and intricate process, crucial for understanding various congenital anomalies and clinical presentations in otolaryngology. This chapter, aligned with the CBME curriculum, provides a comprehensive and student-friendly guide to the embryology of the ear, specifically designed for MBBS and ENT PG students preparing for university theory exams, viva questions, practical exams, and NEET PG MCQs. Mastering this topic will strengthen your conceptual clarity and equip you with essential knowledge for your medical career.
Introduction to Pharyngeal Arches and Germinal Layers
The development of the ear is deeply intertwined with the formation of the pharyngeal arches (also known as branchial arches). These structures are fundamental to the embryology of the head and neck, hence their importance in understanding ear development.
(i) Pharyngeal Arches
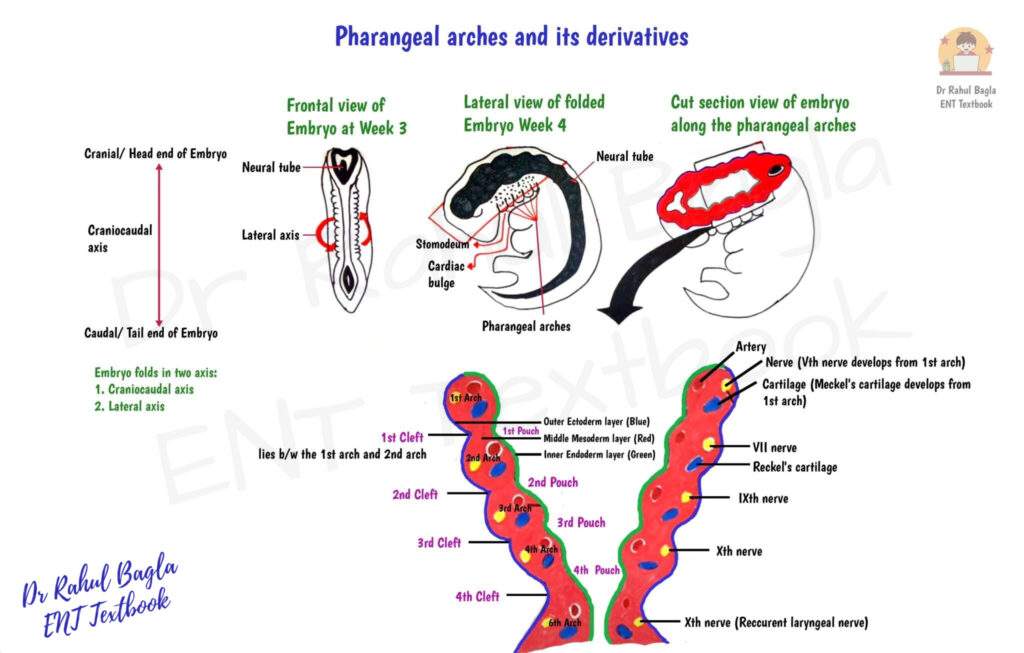
Six pairs of distinct outgrowths, the pharyngeal arches, become apparent around the 4th week of embryonic life. They are located laterally to the stomodeum (primitive mouth) and superior to the cardiac bulge. These arches primarily consist of mesoderm, which is then infiltrated by neural crest cells. Interestingly, the fifth pharyngeal arch appears only briefly before regressing.
Each pharyngeal arch possesses its own dedicated blood supply and nerve supply, emphasising their segmental development. Between adjacent pharyngeal arches, you will find:
- Pharyngeal clefts: These are indentations on the ectodermal (outer) surface.
- Pharyngeal pouches: These are outpouchings on the endodermal (inner) surface.
Both the clefts and pouches play pivotal roles in the formation of various ear structures.
(ii) Germinal Layers
Each pharyngeal arch is composed of three primary germinal layers:
- Endoderm: This innermost layer forms the lining of the pharyngeal arches.
- Ectoderm: This outermost layer forms the external surface of the arches.
- Mesoderm: Situated between the endoderm and ectoderm, this layer forms the structural framework of the arches.
Understanding the contribution of each germinal layer is vital for comprehending the origin of different ear components.
Development of the External Ear
The external ear, comprising the pinna (auricle) and the external auditory canal, is the most visible part of the ear and undergoes significant development during the embryonic period.
1. Development of the Pinna (Auricle)
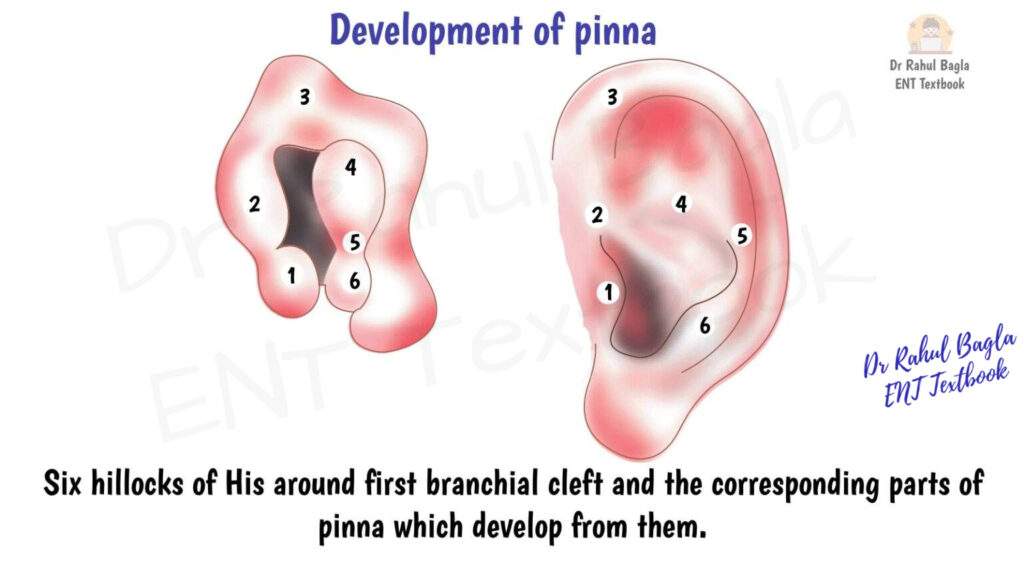
The pinna begins to form around the 6th week of embryonic life from six small prominences or tubercles collectively known as the hillocks of His. These hillocks emerge around the first pharyngeal cleft.
- The first pharyngeal arch gives rise to the first hillock.
- The second pharyngeal arch forms the remaining five hillocks.
Specifically, the first hillock forms the tragus, while the rest of the pinna develops from the fusion of the other hillocks. The incisura terminalis marks the line of separation between the first and second hillocks. These hillocks gradually fuse to create the characteristic shape of the pinna.
Clinical Correlation: Incomplete or improper fusion of these hillocks can lead to developmental anomalies such as preauricular sinuses or cysts. These are often found anterior to the crus of the helix, typically between the tragus and the helix. By the 20th week of gestation, the auricle achieves its adult configuration and migrates from a lower position to a more lateral and cranial location on the head.
2. Development of the External Auditory Canal (EAC), Tympanic Membrane, and Eustachian Tube
The external auditory canal (EAC) and portions of the tympanic membrane develop from the first pharyngeal cleft, while the Eustachian tube arises from the first pharyngeal pouch.
- The first pharyngeal cleft invaginates inward to form the anlage of the external auditory canal.
- Conversely, the first pharyngeal pouch invaginates inward to form the Eustachian tube.
The tympanic membrane (eardrum) forms where the inward invagination of the first pharyngeal cleft meets the outward expansion of the first pharyngeal pouch. Consequently, the tympanic membrane is a unique structure, deriving from all three germinal layers:
- Ectoderm: Forms the outer epidermal layer.
- Mesoderm: Contributes to the fibrous middle layer.
- Endoderm: Forms the inner mucosal layer.
Around the 16th week, cells from the bottom of the ectodermal cleft proliferate to form a solid meatal plug. This plug subsequently undergoes recanalization, creating the lumen of the ear canal. This process typically starts from the deepest part of the canal, near the tympanic membrane, and progresses outwards. Therefore, an important clinical implication is that conditions like atresia of the outer part of the ear canal can occur, while the deeper meatus develops normally. The external ear canal is generally fully developed by the 28th week of gestation.

Development of the Middle Ear Cleft
The middle ear cleft is a complex air-filled space comprising the Eustachian tube, tympanic cavity, attic, antrum, and mastoid air cells. Its development is crucial for sound conduction.
The entire middle ear cleft, including the Eustachian tube, tympanic cavity, attic, antrum, and mastoid air cells, develops from the endoderm of the tubotympanic recess. This recess arises primarily from the first pharyngeal pouch and, to a lesser extent, from the second pharyngeal pouch.
Development of the Ossicles
The three tiny bones of the middle ear—the malleus, incus, and stapes—are critical for sound transmission and have distinct embryological origins:
- The malleus and incus are derived from the cartilage of the first pharyngeal arch (Meckel’s cartilage).
- The stapes, with the exception of its footplate and annular ligament, develops from the cartilage of the second pharyngeal arch (Reichert’s cartilage).
- The footplate of the stapes and its annular ligament originate from the otic capsule, the cartilaginous precursor of the bony labyrinth.
The middle ear is considered completely developed at the time of birth. The Eustachian tube and tympanic cavity are generally formed by 8 months gestation, while the epitympanum and mastoid antrum are also well-developed by birth.

Development of the Inner Ear
The inner ear, responsible for both hearing and balance, has a distinct and early developmental pathway, starting as early as the 3rd week of fetal life.
The development of the inner ear begins around the 3rd week of fetal life and is largely completed by the 16th week.
1. Membranous Labyrinth
The formation of the membranous labyrinth, which houses the sensory organs of hearing and balance, involves a series of invaginations and differentiations:
- Otic Placode: Development commences with the formation of a thickened area of external ectodermal epithelium called the otic placode.
- Otic Pit: As the embryo grows, this placode invaginates (folds inward) to form the otic pit.
- Otic Vesicle (Otocyst): Eventually, the otic pit separates from the external ectoderm, forming a distinct, closed structure known as the otic vesicle or otocyst.
The otic vesicle, entirely derived from ectoderm, subsequently differentiates into two main parts:
- Dorsal Utricular Portion (Pars Superior): This portion forms the vestibular system, which includes the utricle, semicircular canals, and the endolymphatic tube. It develops earlier than the pars inferior.
- Ventral Saccular Portion (Pars Inferior): This portion forms the hearing system, including the cochlear duct (with the organ of Corti) and the saccule.
By the 20th week of gestation, the cochlea (containing the organ of Corti) is fully developed, enabling the fetus to perceive sounds within the womb. This early development of hearing is a fascinating aspect, often referenced in cultural narratives.

2. Bony Labyrinth
Surrounding the developing otic vesicle is the mesoderm, which thickens to form the otic capsule. This otic capsule undergoes a process of differentiation:
- Cartilaginous Framework: The otic capsule initially forms the cartilaginous framework of the inner ear.
- Ossification: This cartilaginous framework subsequently ossifies to become the bony labyrinth.
This cartilage also ossifies to form the petrous part of the temporal bone, which encases and protects the delicate structures of the internal ear.

Table: Embryology of Ear Timeline
| Week | Events |
|---|---|
| WEEK 3 | • Inner Ear Begins: Thickening of surface ectoderm forms the Otic Placode. (Initial blueprint for hearing/balance) • Concept: Origin of inner ear is ECTODERM. |
| WEEK 4 | • Otic Placode invaginates to form the Otic Pit. • Pharyngeal Arches (6 pairs) develop (1st, 2nd crucial for ear). • 1st Pharyngeal Pouch starts expanding (future Eustachian tube/Middle ear). • 1st Pharyngeal Cleft starts invaginating (future External Auditory Canal). • Concept: Beginnings of all three ear parts are visible. |
| WEEK 5 | • Otic Pit detaches from surface ectoderm, forms Otic Vesicle (Otocyst). (Inner ear's selfcontained unit). • Otic Vesicle differentiates into: Dorsal Utricular Portion (future vestibular system: utricle, semicircular canals) Ventral Saccular Portion (future auditory system: cochlea, saccule) |
| WEEKS 6-12 | • Pinna (Auricle) development starts (Week 6):Six Hillocks of His appear around 1st pharyngeal cleft. • 1st Hillock (1st arch) forms Tragus. Remaining 5 Hillocks(2nd arch) form rest of Pinna. • Clinical: Improper fusion > Preauricular sinus/cyst. • Ossicles begin to form: Malleus & Incus: From 1st pharyngeal arch (Meckel's cartilage). Stapes (Head & Crura: From 2nd pharyngeal arch (Reichert's cartilage). Stapes Footplate & Annular Ligament: From Otic Capsule. Otic Capsule (mesoderm) surrounds otic vesicle, begins to ossify (forms bony labyrinth). |
| WEEK 16 | • Inner Ear is Largely Complete. • External Auditory Canal (EAC): Cells from bottom of 1st cleft form solid Meatal Plug (Temporary blockage). |
| WEEK 20 | • Cochlea is fully developed and functional. (Fetus capable of hearing). • Pinna achieves adult shape and migrates to final position. |
| WEEKS 21-28 | • EAC Recanalization: Meatal plug dissolves, creating lumen of EAC. (Starts from medial, progresses laterally). • EAC is fully developed by Week 28. • Clinical: Incomplete recanalization > Atresia of outer EAC. |
| AT BIRTH | • Middle Ear Cleft (Eustachian tube, tympanic cavity, antrum) is fully developed. • All ear structures are generally complete, though mastoid air cells continue to pneumatize postnatally. |
Table: Summary of Ear Development
Understanding the origins of different ear components is critical for clinical correlations. Here’s a concise summary:
| Ear Part | Embryological Origin | Germ Layer(s) Involved | Key Structures Formed |
|---|---|---|---|
| External Ear | |||
| Pinna (Auricle) | Six Hillocks of His (1st & 2nd pharyngeal arches) | Ectoderm, Mesoderm | Tragus (1st hillock), Helix, Antihelix, Concha, Lobe |
| External Auditory Canal | 1st pharyngeal cleft | Ectoderm | Outer part of EAC, Meatal plug recanalization |
| Tympanic Membrane | Junction of 1st pharyngeal cleft & 1st pharyngeal pouch | Ectoderm, Mesoderm, Endoderm | Eardrum (outer, middle fibrous, inner layers) |
| Middle Ear | |||
| Eustachian Tube | 1st pharyngeal pouch | Endoderm | Connects middle ear to nasopharynx |
| Tympanic Cavity, Attic, Antrum, Mastoid Air Cells | Tubotympanic recess (1st & part of 2nd pharyngeal pouches) | Endoderm | Air-filled spaces of middle ear and mastoid |
| Malleus & Incus | 1st pharyngeal arch (Meckel's cartilage) | Mesoderm | Ossicles for sound conduction |
| Stapes (Head & Crura) | 2nd pharyngeal arch (Reichert's cartilage) | Mesoderm | Ossicle for sound conduction |
| Stapes (Footplate & Annular Ligament) | Otic capsule | Mesoderm | Connects stapes to inner ear |
| Inner Ear | |||
| Membranous Labyrinth | Otic vesicle (from otic placode) | Ectoderm | Cochlea, Saccule, Utricle, Semicircular Canals, Endolymphatic Duct |
| Bony Labyrinth | Otic capsule (surrounding otic vesicle) | Mesoderm | Petrous part of temporal bone, bony channels of inner ear |
———–End of the Chapter———–
High-Yield Points for NEET PG and University Exams
- Pharyngeal arches: Six pairs, 1st and 2nd are most relevant to ear. 5th arch regresses.
- Hillocks of His: Six tubercles form the pinna. 1st hillock (1st arch) forms the tragus; others (2nd arch) form rest of pinna.
- Preauricular sinus/cyst: Result of improper fusion of Hillocks of His.
- Tympanic membrane: Unique with all three germ layers (ectoderm, mesoderm, endoderm).
- External auditory canal atresia: Often occurs in the outer part due to incomplete recanalization of the meatal plug.
- Middle ear cleft: Derived from 1st and 2nd pharyngeal pouches.
- Malleus & Incus: Formed from 1st pharyngeal arch. Mnemonic: My Internal Meatus is In First (Meckel’s) arch.
- Stapes (except footplate): Formed from 2nd pharyngeal arch. Mnemonic: Second Stapes.
- Stapes footplate & annular ligament: Derived from otic capsule.
- Inner ear: Completely formed by 16 weeks, derived from ectoderm (otic placode/vesicle).
- Bony labyrinth: Formed from the mesodermal otic capsule.
- Independence of Ear Development: Malformations in one part of the ear (e.g., external ear) do not necessarily affect the other parts (middle or inner ear), allowing for normal function in some regions despite abnormalities in others. This is a common viva question.
MCQ’s NEET PG-Style
Test your understanding with these multiple-choice questions, typical of what you might encounter in the NEET PG exam.
- Which of the following structures is derived from the first pharyngeal arch? a) Stapes b) Incus c) Footplate of stapes d) Otic capsule
- The external auditory canal is formed primarily from the: a) First pharyngeal pouch b) Second pharyngeal pouch c) First pharyngeal cleft d) Second pharyngeal cleft
- The tympanic membrane is unique because it is derived from: a) Ectoderm only b) Mesoderm and endoderm only c) Ectoderm, mesoderm, and endoderm d) Endoderm only
- Malformations like preauricular sinuses are a result of improper fusion of: a) Pharyngeal pouches b) Pharyngeal clefts c) Hillocks of His d) Otic placode
- The membranous labyrinth of the inner ear is derived from the: a) Mesoderm b) Endoderm c) Ectoderm d) Neural crest cells
- Which part of the stapes is derived from the otic capsule? a) Head b) Crura c) Footplate d) Obturator foramen
- Recanalization of the meatal plug forms the: a) Eustachian tube b) Inner ear c) External auditory canal d) Middle ear cavity
- By what gestational age is the cochlea fully developed, allowing for fetal hearing? a) 8th week b) 12th week c) 16th week d) 20th week
- The middle ear cleft primarily develops from the: a) First pharyngeal cleft b) First and second pharyngeal pouches c) Otic vesicle d) Hillocks of His
- If a child presents with external auditory canal atresia, which part of the canal is most likely to be affected due to embryological development? a) Deepest part near the tympanic membrane b) Entire length of the canal c) Outer part of the canal d) Only the cartilaginous portion
MCQ Answers and Explanations
- b) Incus. Explanation: The malleus and incus are derived from the first pharyngeal arch (Meckel’s cartilage). The stapes (except footplate) is from the second arch, and the footplate is from the otic capsule.
- c) First pharyngeal cleft. Explanation: The first pharyngeal cleft invaginates to form the external auditory canal. The first pharyngeal pouch forms the Eustachian tube.
- c) Ectoderm, mesoderm, and endoderm. Explanation: The tympanic membrane is unique as it’s formed at the junction of the first cleft (ectoderm) and first pouch (endoderm), with mesoderm contributing to its fibrous layer.
- c) Hillocks of His. Explanation: Preauricular sinuses or cysts result from incomplete fusion of the six hillocks of His that form the pinna.
- c) Ectoderm. Explanation: The membranous labyrinth develops from the otic placode, which is a thickening of the surface ectoderm, subsequently forming the otic vesicle.
- c) Footplate. Explanation: The footplate of the stapes and its annular ligament are derived from the otic capsule, unlike the rest of the stapes which comes from the second pharyngeal arch.
- c) External auditory canal. Explanation: The meatal plug, a temporary structure in the developing external auditory canal, recanalizes to form the definitive canal.
- d) 20th week. Explanation: The cochlea, including the organ of Corti, is fully developed by the 20th week, allowing the fetus to perceive sounds.
- b) First and second pharyngeal pouches. Explanation: The middle ear cleft, including the Eustachian tube, tympanic cavity, and mastoid air cells, develops from the tubotympanic recess, which is derived from the first and partly the second pharyngeal pouches.
- c) Outer part of the canal. Explanation: Recanalization of the meatal plug typically proceeds from medial to lateral. Therefore, if recanalization is incomplete, the outer part of the canal is most susceptible to atresia.
Clinical-Based Questions for Practical Exams and Viva
These scenarios will help you apply your embryological knowledge to common clinical presentations.
- Scenario: A 4-year-old child is brought to the ENT clinic with a small, dimple-like opening anterior to the tragus of the left ear, which occasionally discharges a small amount of whitish fluid. There is no associated pain or fever.
- Questions:
- What is the likely diagnosis based on its location and presentation?
- What is the embryological basis for this condition?
- What advice would you give the parents regarding this condition?
- Questions:
- Scenario: During a routine pediatric examination, you notice that a newborn has a very small, underdeveloped pinna (microtia) on one side. On otoscopy, the external auditory canal appears completely absent (atresia). You are unable to visualize the tympanic membrane.
- Questions:
- Given the embryological development, what is the most likely status of the middle and inner ear in this child? Explain your reasoning.
- Why is it important to investigate the inner ear in such cases, even if it’s often normal?
- What immediate management steps would you consider for this child, focusing on hearing?
- Questions:
- Scenario: A 6-month-old infant is undergoing evaluation for recurrent middle ear infections. The pediatrician notes a history of abnormal facial nerve development on the affected side.
- Questions:
- Considering the embryological origins, what specific middle ear structures might be affected if there is a primary anomaly of the second pharyngeal arch?
- What is the likely nerve involved in this scenario, and what is its embryological relationship to the pharyngeal arches?
- Questions:
Frequently Asked Questions in Viva
Here are some common questions about ear embryology, optimised for Google Rich Snippets:
- Q: What are the Hillocks of His, and what do they form? A: The Hillocks of His are six small prominences, derived from the first and second pharyngeal arches, that fuse to form the pinna (auricle) of the external ear.
- Q: Which germ layer forms the membranous labyrinth of the inner ear? A: The membranous labyrinth, including the cochlea and semicircular canals, is derived from the ectoderm, specifically from the otic placode and subsequently the otic vesicle.
- Q: Are malformations in one part of the ear (e.g., external ear) always associated with malformations in other parts (middle or inner ear)? A: No, the development of the outer, middle, and inner ear occurs largely independently; therefore, malformations in one part do not necessarily affect the others, although syndromic conditions can involve multiple parts.
- Q: What is the embryological origin of the malleus and incus? A: The malleus and incus, two of the ossicles in the middle ear, are derived from the cartilage of the first pharyngeal arch (Meckel’s cartilage).
- Q: When does the inner ear development get completed? A: The inner ear development begins in the 3rd week of fetal life and is largely completed by the 16th week, with the cochlea fully developed by 20 weeks.
- Q: Why is the tympanic membrane considered unique in its embryological origin? A: The tympanic membrane is unique because it is formed by contributions from all three germinal layers: ectoderm (outer layer), mesoderm (fibrous middle layer), and endoderm (inner layer).
Practical Tips for Viva and Clinical Exam Scenarios
- Be precise with numbers: Examiners love to ask about specific weeks of development (e.g., “When does the inner ear complete development?”). Know your 3rd, 4th, 6th, 16th, 20th, and 28th weeks.
- Connect structures to arches/pouches/clefts: This is fundamental. “Pinna – Hillocks of His – 1st and 2nd arches.” “EAC – 1st cleft.” “Eustachian Tube – 1st pouch.” “Malleus/Incus – 1st arch.” “Stapes – 2nd arch.”
- Clinical correlations are key: When asked about embryology, always try to link it to a clinical condition. For example, improper hillock fusion leads to preauricular sinuses. Incomplete meatal plug recanalization leads to EAC atresia. This shows application of knowledge.
- Mnemonic power: Use mnemonics like “MI FIrst” for Malleus/Incus from First arch.
- “Why is this important?”: This is a common viva question. For ear embryology, it’s important because it explains congenital anomalies (atresia, microtia, sinuses), helps predict associated conditions (e.g., facial nerve palsy with 2nd arch anomalies), and guides management (e.g., audiological assessment in atresia).
- Diagram description: Practice describing the formation of the otic placode, pit, and vesicle verbally or by drawing a simple diagram. This helps solidify understanding.
———— End of the chapter ————
Download full PDF Link:
Embryology of Ear Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
“An incredible resource!”
Thank you so much, Dr. Rahul, for making complex topics so accessible. Your textbook is a lifesaver during exam season.
Final Year MBBS Student, Dow Medical College, Pakistan
Grateful for your feedback, Dr. Ayesha. I’m happy the content eases your exam prep.
Thanks