Anatomy and Functions of the Palatine Tonsils
The palatine tonsils, also known as faucial tonsils, are paired, oval-shaped masses of lymphoid tissue that occupy the tonsillar fossa on either side of the oropharynx. Anatomically, they are positioned between the anterior pillar (formed by the palatoglossus muscle) and the posterior pillar (formed by the palatopharyngeus muscle). Though they may look small when viewed through the mouth, their true size runs deeper, stretching into the soft palate, the base of the tongue, and the palatoglossal arch.

Collectively, the palatine tonsils, together with the pharyngeal tonsils (adenoids), lingual tonsils, tubal tonsils, and the diffuse submucosal lymphoid aggregates of the pharynx, constitute Waldeyer’s ring. This lymphoid ring encircles the pharyngeal inlet and serves a critical immunological function, acting as the first line of defence against inhaled or ingested pathogens by facilitating antigen recognition and initiating immune responses.

Histological Structure of palatine tonsils
Histologically, the tonsils consist of dense aggregates of lymphocytes, which are organized into follicles within a connective tissue stroma. The epithelial covering of the tonsils is composed of stratified squamous epithelium, which invaginates deeply into the parenchyma to form numerous crypts. These crypts significantly increase the surface area of the tonsils, thereby enhancing their immunological functions by providing more interaction sites for antigens and lymphoid tissues.
Microbial Flora of the Palatine Tonsils
The microbial environment within the tonsils is highly variable, showing significant differences between surface and core samples. On the surface of diseased tonsils, the most commonly identified pathogen is group A beta-haemolytic streptococcus (GABHS), which is also found in about 40% of asymptomatic individuals. Other microorganisms that inhabit the tonsillar surface include Haemophilus influenzae, Staphylococcus aureus, alpha-haemolytic streptococci, Branhamella species, Mycoplasma, Chlamydia, anaerobes, and various respiratory viruses. In cases of recurrent tonsillitis, Haemophilus influenzae and Staphylococcus aureus, including methicillin-resistant Staphylococcus aureus (MRSA), are often predominant, while beta-haemolytic streptococci are less frequently isolated.
Anatomical Structure of the Palatine Tonsils
The palatine tonsils exhibit distinct anatomical features, with two surfaces—medial and lateral—and two poles—upper and lower.
Medial Surface: The medial surface of the tonsil is lined with nonkeratinizing stratified squamous epithelium, which forms multiple crypts by dipping into the tonsil’s tissue. On average, 12–15 crypts can be observed on this surface. One prominent crypt near the upper part of the tonsil, known as the crypta magna or intratonsillar cleft, represents the ventral part of the second pharyngeal pouch. Secondary crypts often arise from the main crypts, accumulating a cheesy material composed of epithelial cells, bacteria, and food debris, which can be expelled by applying pressure to the anterior pillar.
Lateral Surface: The lateral surface of the tonsil is encapsulated by a fibrous capsule. Between this capsule and the underlying tonsillar bed is a layer of loose areolar tissue, which facilitates easy dissection during a tonsillectomy. This area is also prone to pus accumulation in cases of peritonsillar abscess. Fibres from the palatoglossus and palatopharyngeus muscles attach to the tonsil’s capsule, contributing to its structural support.
Upper Pole: The upper pole of the tonsil extends into the soft palate. A semilunar fold of mucous membrane covers the medial surface of this pole, extending between the anterior and posterior pillars, and enclosing a potential space known as the supratonsillar fossa.
Lower Pole: The lower pole of the tonsil is anchored to the tongue. A triangular fold of mucous membrane extends from the anterior pillar to the lower part of the tonsil, forming the anterior tonsillar space. This region is separated from the tongue by a groove called the tonsillolingual sulcus, which is a potential site for carcinoma development.
Bed of the Tonsil: The bed of the tonsil is formed by the superior constrictor and styloglossus muscles. The glossopharyngeal nerve and an enlarged styloid process, if present, may be closely associated with the lower part of the tonsillar fossa. These structures can be accessed surgically through the tonsil bed following a tonsillectomy. The tonsil is also in close proximity to the facial artery, the submandibular salivary gland, the posterior belly of the digastric muscle, the medial pterygoid muscle, and the angle of the mandible, which are important considerations during surgery.
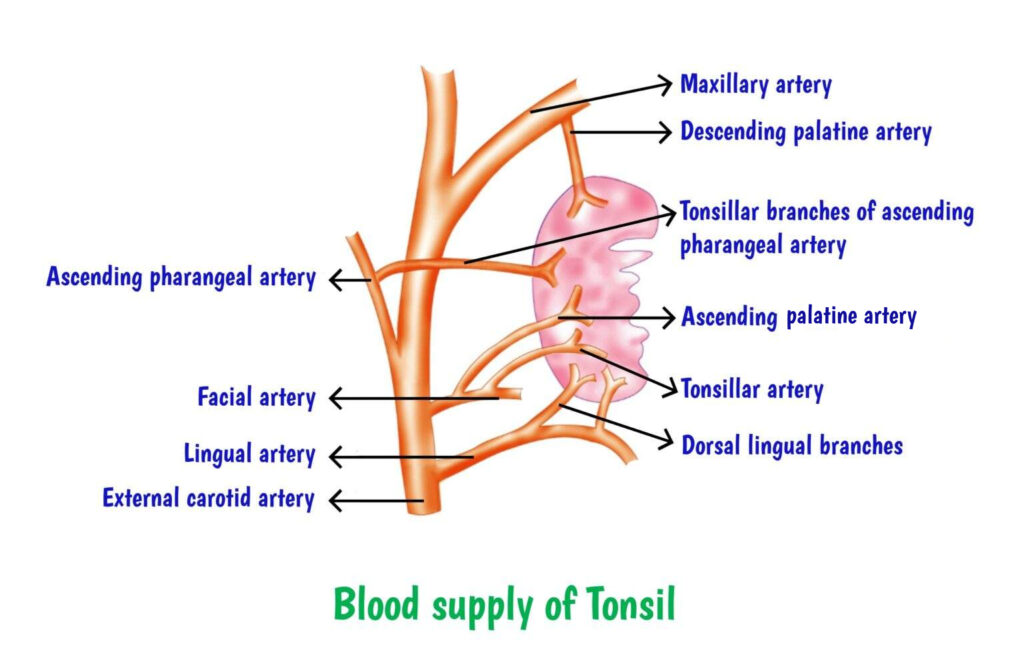
Blood Supply
The palatine tonsils receive their blood supply from five primary arteries:
- The tonsillar branch of the facial artery (the main artery).
- The ascending pharyngeal artery from the external carotid artery.
- The ascending palatine artery is a branch of the facial artery.
- The dorsal linguae branches of the lingual artery.
- The descending palatine branch of the maxillary artery.
Venous and Lymphatic Drainage
Venous blood from the tonsils drains into the paratonsillar vein, which subsequently joins the common facial vein and the pharyngeal venous plexus. Lymphatic drainage passes through the superior constrictor muscle and into the upper deep cervical lymph nodes, particularly the jugulodigastric (tonsillar) node located below the angle of the mandible.
Nerve Supply
The sensory innervation of the tonsils is provided by the lesser palatine branches of the sphenopalatine ganglion, which is associated with the trigeminal nerve (CN V), and the glossopharyngeal nerve (CN IX).
Immunological Functions of the Tonsils
The palatine tonsils play a pivotal role in the immune system, being composed of lymphoid tissue with germinal centres located immediately beneath the mucosa. Both T- and B-lymphocytes are present within the tonsils, with B-lymphocytes predominating. These lymphocytes contribute to both cell-mediated and humoral immune responses, despite the tonsils’ lack of afferent lymphatics. B-cells within the tonsils can synthesize specific antibodies, including immunoglobulin IgG and IgA plasma cells, in response to antigens. The tonsils’ interaction with allergens in the upper respiratory tract enhances local immunity and contributes to the development of systemic immunity.
Mechanisms of Tonsillar Defence
The palatine tonsils function as a crucial defence mechanism against pathogens such as viruses, bacteria, and other antigens that enter the body through inhalation or ingestion. Their immunological role is executed through two primary mechanisms:
- Local Immunity: The surface area of the tonsils and adenoids is increased by the presence of multiple crypts and folds. The specialized epithelium of the tonsils contains M-cells, which act as antigen-processing cells. These cells facilitate the interaction between antigenic material and subepithelial lymphoid follicles. Within these follicles, B-cells can differentiate into plasma cells, producing antibodies that neutralize pathogens. Additionally, macrophages within the tonsils phagocytose bacteria and viruses, thereby managing low-dose antigens and chronic infections.
- Surveillance Mechanism: The tonsils also function as sentinels, identifying foreign antigens and alerting the immune system for a broader response. When exposed to a high dose of antigens, B-cells in the tonsillar germinal centres proliferate and undergo hyperplasia, entering the bloodstream. This triggers a complex immune response involving antigen-processing cells, memory cells, dendritic cells, macrophages, T-helper cells, and T-suppressor cells. The antibodies produced by plasma cells tag antigens for destruction by neutrophils and other phagocytes and also enhance macrophage activity in capturing antigens.
Clinical Considerations
The palatine tonsils are most active during childhood, particularly between the ages of 4 and 10 years. After puberty, they undergo a process of involution, which leads to a decrease in B-cell production and a relative increase in the ratio of T-cells to B-cells. Despite concerns, the removal of the tonsils (tonsillectomy) does not impair the integrity of the immune system or increase susceptibility to diseases such as poliovirus or Hodgkin’s disease. However, tonsillectomy should be performed only based on specific medical indications, as the tonsils play an essential role in immune defence during childhood.
———— End of the chapter ————
Download full PDF Link:
Palatine Tonsils Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Juvenile Angiofibroma. https://www.entlecture.com/juvenile-angiofibroma/
- Please read. Tumours of Hypopharynx . https://www.entlecture.com/tumours-of-the-hypopharynx/
- Please read. Anatomy of Oesophagus. https://www.entlecture.com/anatomy-of-oesophagus/
Keywords: Anatomy and Functions of the Tonsils, Histological Structure, Microbial Flora, Blood Supply, Venous and Lymphatic Drainage of Palatine Tonsils, Bed of Tonsils, Anatomy of palatine tonsils explained, Functions of palatine tonsils in immune system, Role of palatine tonsils in fighting infections, Structure and location of palatine tonsils, Palatine tonsils and their role in immunity, Differences between palatine and lingual tonsils, How palatine tonsils protect the throat, Palatine tonsils lymphatic function, Importance of palatine tonsils in children, Anatomy and functions of palatine tonsils: a detailed guide, How palatine tonsils play a key role in your immune system, Understanding the structure and role of palatine tonsils, The immune functions of palatine tonsils: what you need to know, Palatine tonsils: guardians of the throat and immune defenders, Why palatine tonsils are important for immunity in children, Palatine tonsils vs lingual tonsils: key differences explained, Exploring the lymphatic functions of palatine tonsils, Palatine tonsils: location, structure, and immune role overview