Clinical Approach to a Patient with Facial Weakness
Introduction
Facial nerve paralysis is one of the most common neurological presentations encountered in otolaryngology practice. Facial weakness may result from lesions involving the facial nerve anywhere along its course from the cerebral cortex to the terminal extracranial branches. A systematic clinical approach helps differentiate upper motor neuron from lower motor neuron lesions, localise the site of pathology, identify the underlying cause and guide appropriate treatment.
Clinical Presentation of Facial Weakness
The facial nerve palsy (lower motor neuron type) patient presents with the following clinical features on the involved side:
- Facial weakness on one side
- Inability to close eye
- Loss of nasolabial fold
- Bell’s phenomenon (upward and outward rolling of the eyeball on attempted eye closure)
- Posterior auricular pain/otalgia
- Decreased tearing
- Hyperacusis
- Taste disturbances
- Drooling
Presence of associated otologic, neurological or systemic symptoms may help localise the lesion and identify the underlying cause.
Distinguishing Upper Motor Neuron from Lower Motor Neuron Paralysis
The first and most critical step is to determine whether the lesion involves the upper motor neuron (supranuclear) or the lower motor neuron (nuclear or infranuclear). This distinction is made by examining forehead movement.
Bedside test: Ask the patient to raise both eyebrows. In upper motor neuron paralysis, the forehead muscles on the affected side contract normally because the frontalis muscle receives bilateral cortical innervation. In lower motor neuron paralysis, the forehead is completely paralysed.
Table: Differences between upper and lower motor neuron facial paralysis
| Feature | Upper Motor Neuron (Central) | Lower Motor Neuron (Peripheral) |
| Forehead movement | Preserved (Upper face spared) | Paralysed (Entire half of face involved) |
| Lower face | Contralateral weakness | Ipsilateral complete weakness |
| Associated findings | Limb weakness, dysarthria, cognitive deficits | Otalgia, hyperacusis, taste disturbance, vesicles, unable to frown, close the eye, purse the lips or whistle. |
| Common causes | Stroke, brain tumour, multiple sclerosis, intracranial haemorrhage | Bell’s palsy, Ramsay Hunt syndrome, trauma, infection |
Clinical pearl: A patient who can wrinkle their forehead on the affected side suggests a central lesion and requires neurological evaluation and neuroimaging.
Clinically Relevant Anatomy
Understanding the functional anatomy of the facial nerve helps localise the lesion clinically.
| Anatomic Site | Clinical Correlate | Test/Clue |
| Geniculate ganglion | Lacrimation affected | Schirmer’s test |
| Nerve to stapedius | Hyperacusis | Stapedial reflex loss |
| Chorda tympani | Taste loss anterior 2/3 tongue | Electrogustometry |
| Meatal/labyrinthine segment | Vestibulocochlear symptoms | Associated hearing loss/vertigo |
The Facial Nerve Course – Segments
- Intracranial (cisternal) – 24 mm
- Meatal – 8-10 mm
- Labyrinthine – 4 mm (narrowest, most vulnerable)
- Tympanic – 11 mm (most common site of facial canal dehiscence)
- Mastoid – 13 mm (longest)
Labyrinthine segment (0.68 mm diameter) is the narrowest → most vulnerable to compression from oedema → explains why Bell’s palsy can cause a complete block here.
Important Branches of the Facial Nerve
- Greater Superficial petrosal (geniculate ganglion)
- Nerve to stapedius (pyramid level)
- Chorda tympani (vertical segment)
- Posterior auricular + muscular (at stylomastoid foramen)
Surgical anatomy pearl: During mastoidectomy, remember the posterior tympanotomy boundaries:
- Medial = facial nerve
- Lateral = chorda tympani
- Superior = fossa incudis
Localisation of the site of the lesion
Localisation of the site of injury along the course of the facial nerve is achieved by testing the function of its individual branches.
Clinical Localization
| Site of lesion | Signs |
| Level of nucleus | May be associated with VIth nerve paralysis |
| Cerebellopontine angle | Identified by the presence of vestibular and auditory defects and involvement of other cranial nerves such as Vth, VIIIth, Xth and XIth. |
| Intratemporal segment | Localised by topodiagnostic tests. Taste disturbance, hyperacusis, and lacrimation abnormalities. |
| Extra-temporal segment in the parotid gland | Affects only the motor functions of the nerve. It may sometimes be incomplete as some branches of the nerve may not be involved in tumour or trauma. |
Topographic Diagnosis (Localisation of the Lesion)
Localising the site of injury along the course of the facial nerve is achieved by testing the function of its individual branches.
Topodiagnostic Tests
| Test | Nerve branch assessed | Technique considerations | Assessment/ Outcome |
| Schirmer’s test | Greater (superficial) petrosal nerve | The eye is gently dried of excess tears or use local anaesthetic drops. A Strip of filter paper is placed in the inferior conjunctival fornix of each eye for 5 minutes, and the patient is asked to close their eyes. The length of the paper moistened is compared between the eyes. | Significant reduction in lacrimation compared to the opposite side suggests a lesion proximal to the geniculate ganglion. |
| Stapedial reflex | Nerve to stapedius muscle | Can be tested by tympanometry. | Reflex is lost when the lesion is above the nerve to stapedius. |
| Electrogustometry | Chorda tympani | The tongue is stimulated electrically to produce a metallic taste, and the two sides are compared. Or a drop of salt or sugar solution placed on one side of the protruded tongue | Threshold of the test is compared between sides. Impairment of taste indicates lesion above the chorda tympani. |
| Salivary flow testing | Chorda tympani | Polythene tubes are placed into both Wharton ducts, and salivary flow (no. of drops) is measured over a minute following a gustatory stimulus (6% citric acid on the anterior part of tongue) | A reduction of 25% or more indicates lesion above the chorda. |
Patterns of Localisation
- Suprageniculate lesion: Abnormal Schirmer’s test; all other tests may be abnormal depending on the exact site.
- Suprastapedial lesion (between geniculate and nerve to stapedius): Normal Schirmer’s, absent stapedial reflex, abnormal taste.
- Infrastapedial lesion (between nerve to stapedius and chorda tympani): Normal Schirmer’s, normal stapedial reflex, abnormal taste.
- Infrachordal lesion (below chorda tympani): Isolated motor paralysis.
Clinical Evaluation
History
The diagnosis can be made based on a thorough history, physical examination and diagnostic testing when required. The time of onset, duration and progression of the disease may indicate its aetiology and determine prognosis. Rapidly progressive or complete paralysis, delayed recovery and recurrent episodes are associated with a poorer prognosis.
History should include:
- Time and mode of onset
- Duration and progression of weakness
- Ear symptoms such as otalgia, otorrhoea, hearing loss or vertigo
- Vesicular eruptions
- Facial/head trauma
- Previous surgery
- Headache or neurological symptoms
- Recurrent episodes
- Associated medical conditions such as diabetes mellitus, pregnancy, autoimmune disorders and malignancy
Physical Examination
A complete head and neck examination should be performed, including detailed otologic and cranial nerve examination.
Examination should assess:
- Degree of facial asymmetry
- Ability to wrinkle forehead
- Eye closure
- Ability to smile, puff out cheeks and whistle
- Bell’s phenomenon
- Vesicles or otorrhoea
- Parotid swelling
- Other cranial nerve involvement
Attempt to localise the exact site of the lesion along the course of the facial nerve, i.e. intracranial, intratemporal or extracranial.
Assessment of Severity: The House–Brackmann Grading System
Once Lower Motor Neuron (Peripheral) paralysis is confirmed, the severity must be documented using a standardised scale. The House–Brackmann system, introduced in 1985, remains the most widely used grading system in clinical practice and research.
Table: House–Brackmann facial nerve grading system
| Grade | Description | Characteristics |
| I | Normal | Normal function in all areas |
| II | Mild dysfunction | Slight weakness noticeable only on close inspection; complete eye closure with minimal effort; synkinesis may be present |
| III | Moderate dysfunction | Obvious asymmetry but not disfiguring; eye closes completely with effort; synkinesis or contracture evident |
| IV | Moderately severe dysfunction | Obvious weakness and disfiguring asymmetry; incomplete eye closure; normal symmetry at rest |
| V | Severe dysfunction | Barely perceptible motion; asymmetry at rest; incomplete eye closure |
| VI | Total paralysis | No movement whatsoever |
Clinical application: Grade should be recorded at the first visit and repeated weekly. Electrodiagnostic testing is most useful in complete or near complete paralysis (House–Brackmann grade V–VI). Early clinical improvement within 3 weeks predicts favourable recovery.
Temporal Pattern of Onset and Etiological Approach
The time course of paralysis provides invaluable diagnostic information.
- Sudden onset (seconds to minutes): Trauma, cerebrovascular accident, intracranial haemorrhage.
- Acute onset (hours to 72 hours): Bell’s palsy, Ramsay Hunt syndrome.
- Subacute onset (days to weeks): Lyme disease, sarcoidosis, otitis media, Guillain–Barré syndrome.
- Progressive onset (weeks to months): Facial nerve schwannoma, parotid malignancy, metastatic disease.
- Recurrent ipsilateral paralysis: Tumour involving the facial nerve must be excluded by imaging.
- Recurrent contralateral paralysis: Usually benign (Bell’s palsy or Melkersson – Rosenthal syndrome).
Warning signs requiring imaging:
- Progressive weakness lasting >3 weeks
- Absence of recovery by 3–6 months
- Recurrent paralysis on the same side
Common Causes of Facial Weakness
Clinical Classification by Site
| Segment | Common Causes | Important Clues |
| Intracranial/CPA | Acoustic neuroma, meningitis, metastasis | Vth, VIIth, VIIIth, IXth, Xth and XIth C.N. symptoms |
| Intratemporal | Bell’s (most common), Ramsay Hunt, AOM/CSOM, trauma, schwannoma | Otalgia, otorrhea, vesicles |
| Extratemporal | Parotid tumour, trauma | Palpable mass, previous surgery |
Bell’s Palsy
Bell’s palsy is idiopathic acute peripheral facial paralysis. It is the most common cause of lower motor neuron facial paralysis.
Diagnostic Criteria:
- Acute onset (<72 hours), complete or partial unilateral facial weakness
- No identifiable cause after history and examination
- No CNS signs
Important points of bell’s palsy
- Accounts for 60-75% of all peripheral facial palsies
- 80-90% recover fully. Incomplete recovery is more common in patients with complete paralysis at onset.
- Recurrence in 7-12%. Recurrent ipsilateral palsy warrants imaging to exclude a tumour
- Higher risk: Diabetes (4x), pregnancy (3rd trimester)
Treatment:
Treatment is most effective when started within 72 hours.
- Prednisolone 1 mg/kg/day × 7-10 days (taper not proven beneficial per recent RCTs)
- Acyclovir 400 mg five times a day or valacyclovir 1 g three times a day × 7 days. Antiviral therapy may be added in severe paralysis, though benefit is modest.
- Eye Care Protocol: Day: Artificial tears. Night: Lubricating ointment. Tape the closed eye during sleep if closure is incomplete. Refer to ophthalmology if incomplete closure >1 week
Ramsay Hunt Syndrome (Herpes Zoster Oticus)
Ramsay Hunt syndrome results from varicella zoster virus reactivation involving the geniculate ganglion.
Clinical Triad:
- Vesicular rash involving the external auditory canal/pinna/oral cavity
- Severe otalgia (out of proportion)
- Ipsilateral facial palsy
Treatment (different from Bell’s):
- Prednisolone 1 mg/kg/day × 5 days then taper
- Oral valacyclovir 1 g PO 3×/day × 7-10 days
- I.V. Acyclovir 10-15 mg/kg IV q8h × 7 days if severe/immunocompromised.
Prognosis: Prognosis is poorer than Bell’s palsy because viral inflammation causes greater axonal degeneration (axonotmesis rather than neuropraxia). Approximately 50–70% patients achieve satisfactory recovery despite treatment, while complete recovery rates are lower in patients with complete paralysis at onset.
Malignant Otitis Externa (Skull Base Osteomyelitis)
Seen in: Elderly diabetic, immunocompromised Organism: Pseudomonas aeruginosa (90%) Findings: Severe otalgia. Granulation tissue at the bony-cartilaginous junction
Multiple cranial nerves may become involved in advanced disease. (order of frequency): VII → X → XI → XII → IX → VI → V
Diagnosis:
- CT temporal bone (bony erosion)
- MRI (soft tissue extension, dural involvement)
- Technetium/Gallium scan (follow treatment response)
Treatment (minimum 6 weeks IV): Prolonged antipseudomonal antibiotic therapy is required, commonly using intravenous ciprofloxacin, ceftazidime, piperacillin-tazobactam or combination therapy depending on severity and culture sensitivity.
PET-CT is emerging as the best tool for monitoring treatment response. ESR/CRP monitored weekly – should trend down; if rising after 1 week, suspect resistance or inadequate debridement.
Traumatic Facial Paralysis
Clinical Pattern
- Delayed onset paralysis: Prognosis is usually good recovery with conservative treatment
- Immediate onset of paralysis usually suggests severe nerve injury.
Evaluation
HRCT of the temporal bone should be performed to identify fractures, bony impingement or transection.
Indications for Surgical Exploration
- Immediate complete paralysis
- Displaced bony fragments
- Evidence of nerve transection
- Severe degeneration on electrodiagnostic testing
Surgical Approaches
- Transmastoid approach – tympanic and mastoid segments • Middle cranial fossa approach – labyrinthine and meatal segments
Investigations
Audiological Evaluation
- Pure tone audiometry
- Impedance audiometry, including stapedial reflex testing
Electrodiagnostic Evaluation
Electrodiagnostic tests provide objective information about the degree of nerve degeneration and help predict prognosis. They are most useful between day 4 and day 21 after the onset of complete paralysis.
Electroneuronography (ENoG)
ENoG is the most useful prognostic test. A supramaximal stimulus is delivered to the facial nerve trunk at the stylomastoid foramen, and the evoked compound muscle action potential (CMAP) is recorded from the nasolabial fold. The amplitude on the paralysed side is compared with the normal side.
Interpretation:
- CMAP amplitude <10% of the normal side indicates 90% axonal degeneration.
- Degeneration of >90% occurring within the first 14 days of complete paralysis predicts a poor recovery rate.
- Faster degeneration (within 7 days) carries an even poorer prognosis.
ENoG has no role in the first 72 hours because Wallerian degeneration takes time to develop.
Electromyography (EMG)
EMG records motor unit potentials from the orbicularis oculi and oris muscles. It is useful in chronic cases to plan reanimation procedures.
Findings and their implications:
- Fibrillation potentials: Evidence of Wallerian degeneration, appearing 2–3 weeks after denervation. They indicate intact motor end plates, so nerve substitution procedures may succeed.
- Polyphasic innervation potentials: Early signs of reinnervation, appearing 6–12 weeks before clinical recovery.
- Normal or polyphasic potentials after one year: Ongoing reinnervation; no surgery required.
- Electrical silence: Atrophy of motor end plates and fibrous replacement of muscle. Muscle transposition rather than nerve substitution is needed.
Other Tests (Historical)
- Minimal nerve excitability test: Compares current threshold to elicit minimal muscle contraction. A difference of 3.5 mA or more indicates poor recovery.
- Maximal stimulation test: Reduced or absent response with maximal stimulation suggests nerve degeneration.
These tests are rarely used due to poor accuracy and inter‑observer variation.
Imaging
Indications for MRI:
- Progressive weakness lasting more than three weeks • No recovery after 3–6 months • Recurrent ipsilateral palsy • Associated neurological findings • Suspicion of tumour
Preferred modality: MRI with gadolinium and thin cuts through the internal auditory canal. In Bell’s palsy, enhancement of the geniculate ganglion and labyrinthine segment may be seen and is usually reactive rather than neoplastic.
Indications of HRCT temporal bone:
- Temporal bone trauma • Cholesteatoma • Malignant otitis externa • Bony erosion or fractures
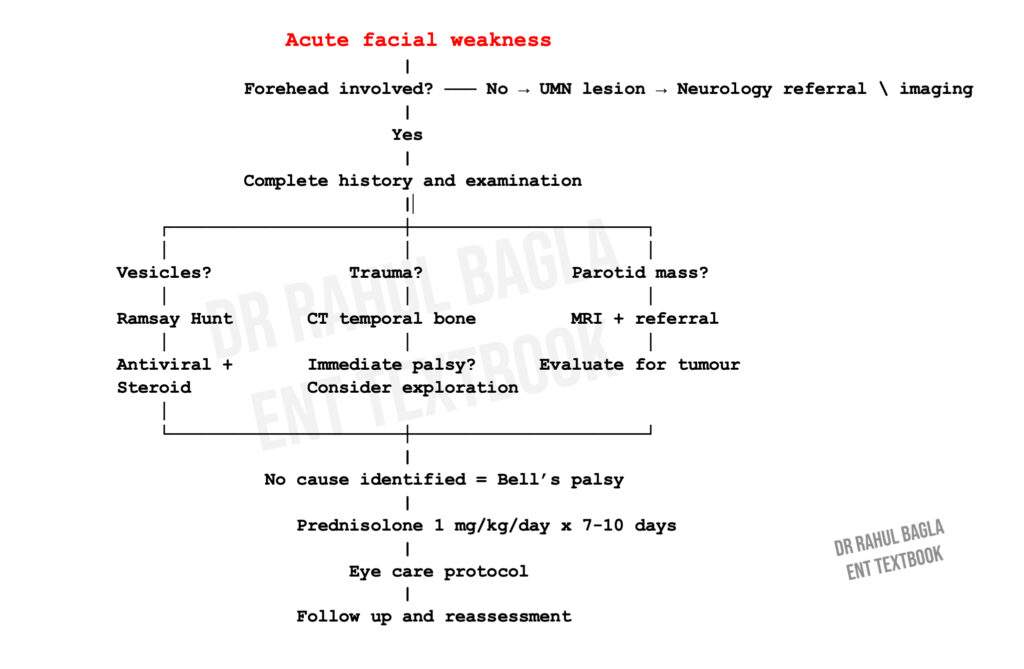
Management Principles
Initial Clinical Algorithm
Surgical Reanimation of the Chronic Facial Paralysis
For patients with long‑standing facial paralysis (more than 12–18 months) and no clinical or electromyographic evidence of reinnervation, surgical reanimation may be considered. The choice of procedure depends on the availability of the proximal nerve stump, the status of the distal facial muscles (assessed by EMG), and the patient’s goals (static tone versus dynamic smile).
Nerve substitution procedures (when motor end plates are intact):
- Hypoglossal‑facial anastomosis: The hypoglossal nerve is divided and anastomosed to the distal facial nerve stump. The patient learns to activate facial muscles by moving the tongue. Synkinesis/mass movement is common. The classic technique causes significant tongue hemiatrophy; the “jump” graft technique (partial hypoglossal to facial) reduces morbidity.
- Nerve grafting (sural nerve): Used when a gap exists between the proximal and distal stumps. Recovery is good only if the graft is placed in a well‑vascularized bed and there is no distal muscle fibrosis.
Muscle transposition procedures (when motor end plates are atrophic):
- Temporalis transfer: The anterior half of the temporalis muscle is detached, turned down, and sutured to the orbicularis oris and zygomaticus. It provides static support and a voluntary smile when the patient clenches the jaw.
- Masseter transfer: Similar principle using the masseter muscle.
Free flap reanimation (gracilis muscle): The gracilis muscle is harvested with its nerve (obturator) and vascular pedicle. It is inset into the face, and the nerve is coapted to the contralateral facial nerve (for spontaneous smile) or to the masseteric nerve (for voluntary smile). This is the gold standard for smile reanimation in young, motivated patients.
Eye closure procedures:
- Gold weight implantation: A gold weight is sutured to the tarsal plate deep to the levator palpebrae. Gravity assists eye closure.
- Palpebral spring: A stainless steel spring is inserted to actively close the eye. Rarely used today.
- Tarsorrhaphy: Permanent or temporary partial closure of the eyelids.
Decision Algorithm for Chronic Palsy (>12-18 months)
No recovery after 12–18 months
|
EMG
|
┌─────────┴─────────┐
| |
Motor end plates No motor end plates
intact present
| |
Nerve procedures Muscle transfer
Table: Common Procedures Summary
| Procedure | Indication | Outcome | Success Rate |
| Nerve graft (sural) | Gap <3 cm, healthy bed | Tone, some movement | 60-70% HB III-IV |
| Hypoglossal-facial jump | No proximal stump | Tone, mass movement | 70-80% improvement |
| Temporalis transfer | Long-standing, no motor end plates | Static + dynamic correction | Reliable smile |
| Gold weight implant | Incomplete eye closure | Eye closure | 90% satisfaction |
Prognosis
| Condition | Complete Recovery Rate | Poor Prognostic Factors |
| Bell’s palsy | 80–90% | Age >60 years, complete paralysis at onset, absent stapedial reflex, postauricular pain, dry eye, abolished taste |
| Ramsay Hunt syndrome | Approximately 50–70% achieve satisfactory recovery with treatment. | Complete paralysis at onset, age >60 years |
| Traumatic palsy (delayed) | Excellent | — |
| Traumatic palsy (immediate) | Variable | Bony impaction, nerve transection |
Sequelae and Complications of Facial Paralysis
Peripheral facial paralysis due to any cause may result in any of the following complications:
1. Incomplete Recovery. Facial asymmetry is not completely resolved. It results in persistent tears in the affected eye due to incomplete eye closure, difficulty in speaking clearly, involuntary drooling of saliva and difficulty in drinking and eating, leading to psychological and social stigma.
2. Exposure Keratitis. Due to incomplete closure of the eye, tear film from the cornea evaporates, causing dryness, foreign body sensation, blurring of vision, exposure keratitis and corneal ulcer. Treatment of exposure keratitis is:
- Frequent use of eye drops (containing hydroxypropyl cellulose, hydroxypropyl methylcellulose or polyvinyl) should be used during the daytime, whilst at night, the eye should be taped closed after putting thicker ointments containing petroleum, mineral oil or lanolin.
- Corneal protection with lubrication and patching.
- Use of large-lens sunglasses.
- Patients should be instructed to close the eye gently with clean hands to avoid corneal abrasion.
- Patients having long-term facial nerve palsy are advised to close their eyes manually using a finger, as well as attempting to stretch the upper lid in order to prevent shortening caused by the unopposed action of the levator palpebrae superioris muscle.
- Temporary tarsorrhaphy may also be indicated. Eye closure can also be improved by using gold-weight implants sutured to the tarsal plate deep to the levator palpebrae muscle.
3. Crocodile tears (Gustatory Lacrimation). During recovery from facial nerve paralysis, regenerating parasympathetic fibres destined for the salivary glands may become misdirected and supply the lacrimal gland instead. Therefore, while eating food, instead of developing salivation, the patient develops paroxysmal ipsilateral shedding of tears (lacrimation). Treatment options are botulinum toxin injection into the lacrimal gland and sectioning of the greater superficial petrosal nerve or tympanic neurectomy.
4. Frey’s Syndrome (Gustatory Sweating). It commonly occurs following parotid surgery or injury to the auriculotemporal nerve. The overlying sweat glands get aberrant reinnervation from postganglionic parasympathetic neurons, resulting in flushing and sweating over the parotid area, instead of salivation during mastication.
5. Synkinesis (Simultaneous movement). It occurs due to abnormal regeneration of facial nerve fibres, which aberrantly innervate adjacent groups of facial muscles, causing unwanted facial movement. It usually occurs following surgery or surgical repair of the facial nerve. The patient may experience eye closure during a smile and laugh, or while closing the eye, there is twitching of the corner of the mouth. Treatment options are physical therapy, botulinum toxin, and surgery.
6. Tics and Spasms. These are involuntary twitching of the eye and facial muscles on one side of the face, occurring as a result of faulty regeneration of fibres following nerve injury.
7. Contractures. Due to prolonged facial palsy, the facial muscles get contracted and become atrophic. Shortening of the facial muscles affects the movements of the face. Usually, no facial asymmetry is visible during the rest position. But sometimes the affected side of the face may appear slightly lifted, and the eye may appear smaller as compared to the other eye.
Summary: Key Points for Examination Revision
Bedside differentiation:
- Forehead involved = suggests peripheral (LMN) → ENT cause
- Forehead spared = suggest central (UMN) → Neurology cause
Bell’s palsy essentials:
- Most common cause (60–75%)
- Diagnosis of exclusion
- Treat with prednisolone 1 mg/kg/day × 7–10 days (start within 72 hours)
- Eye care is the priority
- 80–90% recover completely
Red flags requiring imaging:
- Progressive weakness >3 weeks
- No recovery by 3–6 months
- Recurrent ipsilateral palsy
- Associated neurological findings
Ramsay Hunt vs Bell’s:
- Ramsay Hunt: vesicles + severe pain + worse prognosis → mandatory antiviral + steroid
- Bell’s: no vesicles → steroid ± antiviral
Malignant otitis externa:
- Elderly diabetic + severe otalgia + granulation tissue at bony‑cartilaginous junction
- Pseudomonas aeruginosa
- Treat with IV antipseudomonal antibiotics for 6+ weeks
ENoG timing:
- Days 4–14 after the onset of complete paralysis
- 90% degeneration within 14 days → poor prognosis
Traumatic palsy:
- Delayed onset → conservative (good prognosis)
- Immediate onset → CT for bony fragment; explore if present
———— End of the Chapter ————
High-Yield Points
- Forehead sparing indicates UMN lesion.
- Bell’s palsy is the most common cause of LMN facial paralysis.
- The labyrinthine segment is the narrowest part of the facial canal.
- Hyperacusis indicates lesion proximal to nerve to stapedius.
- Ramsay Hunt syndrome presents with vesicles, otalgia, and facial palsy.
- ENoG is most useful between day 4 and day 14.
- More than 90% degeneration on ENoG predicts poor prognosis.
- Eye care is the most important supportive treatment.
- Recurrent ipsilateral palsy requires MRI.
- Delayed traumatic facial palsy has good prognosis.
NEET PG Style MCQs
- Forehead sparing in facial paralysis suggests: A. Bell’s palsy B. Upper motor neuron lesion C. Ramsay Hunt syndrome D. Parotid tumor
- The narrowest segment of the facial canal is: A. Tympanic segment B. Mastoid segment C. Labyrinthine segment D. Meatal segment
- Hyperacusis occurs due to paralysis of: A. Tensor tympani B. Stapedius C. Buccinator D. Orbicularis oculi
- The most common cause of lower motor neuron facial paralysis is: A. Stroke B. Bell’s palsy C. Acoustic neuroma D. Cholesteatoma
- Vesicles in the external auditory canal with facial palsy suggest: A. Bell’s palsy B. Ramsay Hunt syndrome C. Malignant otitis externa D. Acoustic neuroma
- Best timing for ENoG is: A. First 24 hours B. Day 4–14 C. After 6 weeks D. After 6 months
- Hyperacusis indicates lesion proximal to: A. Chorda tympani B. Greater superficial petrosal nerve C. Nerve to stapedius D. Stylomastoid foramen
- Recurrent ipsilateral facial palsy requires: A. Observation B. MRI evaluation C. Oral antibiotics D. Mastoidectomy
- Bell’s palsy treatment is most effective if started within: A. 24 hours B. 48 hours C. 72 hours D. 1 week
- The best prognostic electrodiagnostic test in facial palsy is: A. EMG B. ENoG C. Schirmer’s test D. Audiometry
Answers
1: B. 2: C. 3: B. 4: B. 5: B. 6: B. 7: C. 8: B. 9: C. 10: B.
Clinical Case Scenarios
- Case 1. A 40-year-old diabetic male develops sudden onset right-sided facial weakness with inability to close the eye. Forehead movements are absent. No vesicles are seen. Most likely diagnosis: Bell’s palsy. Best treatment: Prednisolone within 72 hours with aggressive eye care.
- Case 2. A 55-year-old woman presents with severe otalgia, vesicular eruptions in the external auditory canal, and ipsilateral facial paralysis. Most likely diagnosis: Ramsay Hunt syndrome. Best management: Steroid plus antiviral therapy.
- Case 3. A 70-year-old hypertensive patient develops sudden facial weakness with preserved forehead movement and hemiplegia. Most likely diagnosis: Upper motor neuron facial palsy due to stroke. Best next step: Urgent neuroimaging.
- Case 4. A patient develops delayed facial paralysis after temporal bone trauma. Most likely prognosis: Good recovery with conservative treatment.
Frequently Asked Questions in Viva
- What is the most common cause of facial nerve paralysis? Bell’s palsy is the most common cause of lower motor neuron facial paralysis.
- How do you differentiate UMN and LMN facial palsy? Forehead sparing suggests UMN lesion, while complete facial involvement suggests LMN lesion.
- Why does hyperacusis occur in facial nerve palsy? Hyperacusis occurs due to paralysis of the stapedius muscle.
- When should MRI be performed in facial paralysis? MRI is indicated in progressive weakness, recurrent palsy, or absence of recovery.
- What is the best prognostic test in Bell’s palsy? Electroneuronography (ENoG) is the best prognostic test.
- What is the classical triad of Ramsay Hunt syndrome? Severe otalgia, vesicular rash, and facial paralysis.
- Why is eye care important in facial palsy? Incomplete eye closure may lead to exposure keratitis and corneal ulceration.
———— End ————
Download full PDF Link: Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck surgery.
- W. Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Salah Mansour, Textbook of Comprehensive and Clinical Anatomy of the Middle Ear.
- Susan Standring, Gray’s Anatomy.
- Orlando Guntinas-Lichius, Textbook of Facial Nerve Disorders and Diseases: Diagnosis and Management.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Learn the complete clinical approach to facial weakness for MBBS and ENT PG students. Covers Bell’s palsy, Ramsay Hunt syndrome, facial nerve anatomy, localisation, investigations, management, MCQs, viva tips, CBME revision notes, and NEET PG high-yield concepts. Clinical Approach To Facial Weakness Notes, Facial Nerve Paralysis ENT Notes, Bell’s Palsy Management For MBBS, Facial Nerve Palsy CBME Guide, LMN Vs UMN Facial Palsy Differences, Facial Nerve Anatomy For NEET PG, Bell’s Palsy MCQs With Answers, Ramsay Hunt Syndrome Notes, Facial Weakness Clinical Examination, Facial Nerve Palsy Viva Questions, Facial Nerve Paralysis Revision Notes, Facial Palsy Treatment Guidelines 2026, ENT Facial Nerve Paralysis Summary, Facial Weakness Diagnosis Algorithm, House Brackmann Grading System Notes, Facial Nerve Lesions Explained, Facial Palsy Clinical Cases For Viva, Facial Paralysis Practical Examination Guide, Facial Nerve Palsy Mnemonics, Facial Weakness ENT PG Preparation, Bell’s Palsy Steroid Treatment Notes, Ramsay Hunt Syndrome MCQs, Facial Nerve Topodiagnostic Tests, Schirmer Test In Facial Palsy, Hyperacusis Facial Nerve Lesion, Electroneuronography ENoG Notes, EMG In Facial Paralysis, Facial Weakness Differential Diagnosis, Facial Nerve Paralysis High Yield Points, ENT CBME Facial Nerve Chapter.