Disorders of Oesophagus
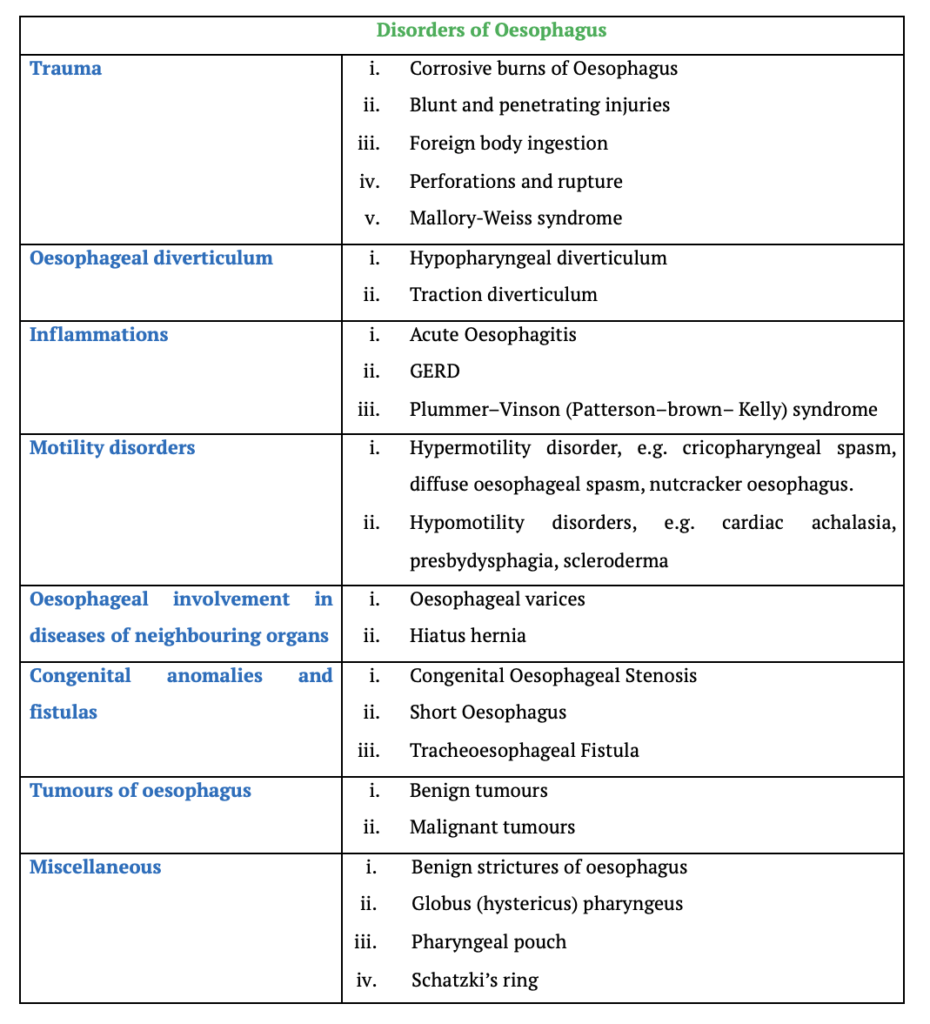
The oesophagus, a muscular tube connecting the lower end of the pharynx to the stomach, is susceptible to various disorders. These conditions can range from inflammatory responses to more severe mechanical injuries or chronic conditions. Understanding the causes, symptoms, diagnosis, and treatments of oesophageal disorders is crucial for both clinical practice and patient care. Below are some of the common disorders of the oesophagus, outlined in detail.
Trauma
1. Corrosive Burns of the Oesophagus
Causes:
Corrosive burns occur when acids, alkalis, or other chemicals are ingested, either accidentally (often in children) or deliberately (in suicide attempts).
Symptoms:
White corrosive crusts and burned areas are found in the mouth and the surrounding area. These burns cause severe pain in the mouth, pharynx, and chest, often accompanied by gagging, vomiting, sialorrhea and respiratory difficulties. Shock becomes progressive, with falling blood pressure and a rising pulse rate, cyanosis and pallor, cold sweats, and circulatory collapse.
Pathology:
- Severity: The extent of oesophageal burns depends on the type, concentration, duration of contact and quantity of the corrosive substance ingested.
- Types of necrosis: Acids cause coagulative necrosis, while alkalis induce liquefactive necrosis, penetrating deeper into the oesophagus. The oesophagus is more severely affected than the stomach in alkaline burns, due to reflex cardiospasm, while acid burns cause more severe damage to the stomach. Alkalies are more destructive and penetrate deep into the layers of the oesophagus. With lye burns, the entire oesophagus and stomach may slough off, causing fatal mediastinitis and peritonitis.
Oesophageal burns usually take the following course:
- Acute necrosis.
- Granulation: Slough separates, leaving a granulating ulcer.
- Stricture formation: Begins two weeks after the injury and can persist for months, leading to progressive dysphagia.
- Late complications such as late or recurrent stenosis and possibly malignant degeneration.
2. Blunt and Penetrating Injuries
- Blunt injuries to the oesophagus, such as those sustained in car accidents, can lead to oesophageal tears. These tears may result in delayed oesophagal-tracheal fistulas, which are characterised by coughing while swallowing.
- Penetrating injuries, usually in the cervical region, can result from sharp force trauma. Treatment depends on the severity, with minor injuries managed conservatively and larger injuries requiring surgical intervention.
3. Foreign body ingestion
4. Perforation or Rupture of the Oesophagus
Causes: Oesophageal perforation, or rupture, may result from:
- Instrumental trauma: This is iatrogenic, often occurring during esophagoscopy or the dilation of oesophageal strictures. Ruptures typically occur just above the upper sphincter or in the lower sphincter near the hiatus.
- Spontaneous rupture: This often follows episodes of vomiting, primarily affecting the lower third of the oesophagus. A classic example is Boerhaave syndrome, where all layers of the oesophagus rupture post-emesis, often associated with chronic vomiting or alcohol abuse.
Symptoms:
Symptoms vary based on the location of the perforation:
- Cervical oesophageal rupture: Pain, fever, difficulty swallowing, local tenderness and surgical emphysema in the neck.
- Thoracic oesophageal rupture: Pain referred to the interscapular region, fever, shock, and signs of pneumothorax (air in the chest cavity). Hamman’s sign (a crunching sound over the heart) may also be present due to air in the mediastinum.
Diagnosis:
Chest and neck X-rays reveal widening of the mediastinum and retrovisceral space, surgical emphysema, pneumothorax, pleural effusion or gas under the diaphragm. Early diagnosis is crucial, as untreated perforation can lead to fatal mediastinitis. All patients complaining of pain in the neck or interscapular region, following an oesophagoscopy, should be suspected of a perforation.
Treatment:
- Stop oral feeding and maintain nutrition through intravenous (IV) fluids.
- Administer IV antibiotics to prevent infection.
- Early cervical perforations may be managed conservatively; drainage is required only if suppuration develops. Retrovisceral space and/or upper mediastinum can be drained through the neck.
- While thoracic perforations is more serious and often require surgical repair, especially if detected within six hours. If diagnosis is delayed, repair is not possible; surgery is then restricted to drainage of the infected area.
5. Mallory-Weiss Syndrome
Mallory-Weiss syndrome involves a tear in the mucosa at the junction between the oesophagus and the stomach, typically following severe retching or vomiting.
Causes:
This syndrome is commonly associated with chronic alcoholism but may also result from conditions like malignant tumors, pregnancy-related vomiting, and other gastrointestinal disorders.
Symptoms:
Symptoms include severe but painless gastrointestinal bleeding, pallor, tachycardia, and sometimes shock.
Treatment:
Most cases resolve spontaneously within 24 to 48 hours, but endoscopic or surgical intervention may be required in severe cases. Rarely, the condition can be fatal.
Oesophageal diverticulum
1. Hypopharyngeal Diverticulum
An oesophageal diverticulum is a pouch that protrudes from the oesophageal wall. The most common type is hypopharyngeal diverticulum, which usually does not cause symptoms but may cause mild respiratory symptoms when the diverticulum is at the level of the carina, retrosternal pressure and attacks of coughing. Twenty percent of cases are combined with hiatus hernia. Diverticula are diagnosed through radiography and endoscopy.
Treatment:
Surgical removal is indicated only if symptoms are severe or complications such as ulceration, bleeding, or malignancy are suspected.
2. Traction Diverticula
Traction diverticula are caused by scar tissue from paraoesophageal or paratracheal lymph node inflammation. The diverticula are visible on radiographs as an inverted cone arising from the wall, usually located in the middle third of the oesophagus. These diverticula often go unnoticed and usually require no treatment unless symptoms are severe and require removal.
Inflammations
1. Acute Oesophagitis
Causes:
It is an acute inflammation of the oesophagus, often caused by:
- Ingestion of hot liquids.
- Ingestion of caustic or corrosive agents (such as chemicals).
- Trauma from swallowing foreign bodies or during esophagoscopy.
- Fungal infections like moniliasis (especially from oral thrush).
- Systemic disorders such as pemphigus.
Symptoms:
Patients typically experience dysphagia (difficulty swallowing), a burning sensation behind the sternum (retrosternal), and occasionally, haematemesis (vomiting blood).
Diagnosis:
Diagnosis is based on the patient’s history, X-ray imaging, and esophagoscopy (an endoscopic examination of the oesophagus).
2. Gastro-oesophageal reflux
Gastro-oesophageal reflux disease (GERD) occurs when the lower oesophageal sphincter (LES) weakens, allowing stomach contents to flow back into the oesophagus. This leads to symptoms like substernal pain, heartburn and regurgitation, especially after meals or when lying down. GERD is common, with 20% of adults experiencing weekly episodes and 10% experiencing daily symptoms. Though most cases are mild, complications such as oesophagitis, oesophageal strictures, or cancer may develop in severe cases.
Risk factors for GERD include hiatal hernia, smoking, obesity, pregnancy and alcohol. Medications like anticholinergic, beta-adrenergic drugs and calcium-channel blockers may also worsen symptoms. Diagnosis primarily relies on a detailed medical history, as physical exams may not reveal the condition. Persistent cases may require esophagogastroscopy or 24-hour pH monitoring to confirm the diagnosis.
The treatment consists of:
- Avoid smoking, alcohol, and trigger foods (chocolates, mints and carbonated drinks).
- Elevate the head of the bed at night.
- Avoiding food at least 3 hours before bedtime.
- Take antacids or H2 receptor antagonists, e.g. cimetidine and ranitidine
- Drugs that increase the tone of the lower oesophagal sphincter, e.g. metoclopramide.
- In severe or complicated cases, proton pump inhibitors (e.g., omeprazole)
- Antireflux surgery, e.g. Nissen’s fundoplication may be necessary to strengthen the LES and prevent further reflux.
3. Plummer–Vinson Syndrome (Patterson–Brown–Kelly Syndrome)
Plummer–Vinson syndrome is characterised by a combination of dysphagia, iron-deficiency anaemia, glossitis, angular stomatitis, koilonychia (spoon-shaped nails), and achlorhydria. The condition leads to atrophy of the alimentary tract mucous membranes and predominantly affects women over the age of 40.
Diagnosis: Barium swallow and oesophagoscopy reveal a web in the post-cricoid region, caused by subepithelial fibrosis. Approximately 10% of patients with this syndrome develop post-cricoid carcinoma, and there is an increased risk of carcinoma in the tongue, buccal mucosa, pharynx, oesophagus, and stomach.
Treatment: Correction of anaemia is the first step, achieved through oral or parenteral iron supplementation, and associated B12 and B6 deficiencies must also be addressed. Dilatation of the oesophageal web can be performed using bougies.
Motility disorders
Hypermotility disorders
1. Cricopharyngeal Spasm. It is a condition where the upper oesophageal sphincter (cricopharyngeus muscle) fails to relax properly due to fibrosis or muscle spasm. This junction between the pharynx and oesophagus experiences incoordination between relaxation and the simultaneous contraction of the pharynx. Common causes include cerebrovascular accidents, Parkinson’s disease, bulbar polio, multiple sclerosis, and muscular dystrophies.
2. Diffuse Oesophageal Spasm. It is characterised by strong, ineffective, non-peristaltic contractions of the oesophagus while the sphincter’s relaxation remains normal. Patients may experience dysphagia (difficulty swallowing), odynophagia (painful swallowing), and substernal chest pain that mimics angina. Diagnostic tests such as a barium swallow may reveal segmented oesophageal spasms resembling a “rosary bead” or “corkscrew” oesophagus. Manometry shows normal sphincter relaxation with non-peristaltic waves. Treatment includes dilation of the lower oesophagus, and severe cases may require surgical myotomy.
3. Nutcracker Oesophagus. It presents with strong, high-amplitude oesophageal contractions that remain peristaltic, unlike diffuse oesophageal spasm where the contractions are non-peristaltic. This condition causes symptoms like dysphagia and substernal pain. While the contractions are powerful, they maintain their coordinated peristaltic nature, differentiating it from other hypermotility disorders.
Hypomotility disorders
1. Cardiac Achalasia. Cardiac Achalasia is characterised by the absence of peristalsis in the oesophagus and a high resting pressure in the lower oesophageal sphincter (LES), which fails to relax during swallowing. This condition leads to food retention in the oesophagus, resulting in a dilated oesophagus, or megaoesophagus, particularly in children. It typically affects individuals aged 30–50 but can also occur in children. The cause is the degeneration or absence of ganglion cells (myenteric plexus of Auerbach) in the oesophageal wall, similar to Chagas disease in South America, caused by Trypanosoma cruzi.
Symptoms include dysphagia (difficulty swallowing), more pronounced with liquids than solids, and regurgitation of food, particularly at night. Diagnosis is made through barium swallow (showing a “rat tail” or “bird-beak” appearance), manometric studies (revealing high pressure in the LES and failure to relax), and endoscopy to rule out carcinoma or stricture.
The primary treatment is Heller’s myotomy, where the LES is surgically cut to relieve obstruction. In cases unfit for surgery, pneumatic dilation is an alternative, using a dilator or balloon to expand the LES. Complications include oesophageal perforation, especially if carcinoma is present. Long-term medical treatment is generally ineffective, and recurrences may require repeat interventions.
2. Presbydysphagia refers to swallowing difficulties in the elderly, affecting all swallowing stages. Age-related changes include weakened mastication, reduced laryngeal elevation, prolonged pharyngeal and oesophageal transit times, and ineffective peristalsis. Though common in healthy elderly individuals, these changes may lead to swallowing issues when compounded by illness or weakness.
3. Scleroderma. Scleroderma, including CREST syndrome (Calcinosis, Raynaud’s phenomenon, oesophageal involvement, sclerodactyly, and telangiectasia), is a progressive connective tissue disorder. It results in the replacement of smooth muscle cells with collagen fibres, leading to fibrosis. The oesophagus, particularly the lower two-thirds, is commonly affected, leading to poor peristalsis and severe gastro-oesophageal reflux disease (GORD).
Oesophageal involvement in diseases of neighbouring organs
1. Oesophageal Varices. Theses are swollen blood vessels in the oesophagus, often caused by portal hypertension, leading to severe bleeding (hematemesis) and tarry stools. These varices develop due to obstructed blood flow, commonly from cirrhosis, hepatitis, or tumours. Diagnosis is confirmed through flexible esophagoscopy, which is more accurate than radiography. Treatment involves emergency blood replacement, controlling bleeding with devices like the Sengstaken–Blakemore tube, and, in some cases, a portal venous shunt or obliteration of varices using laser or sclerosing agents.
2. Hiatus Hernia. It occurs when part of the stomach moves into the chest through the oesophageal opening of the diaphragm. It is common in patients over 40 and exists in two forms:
- Sliding hernia, where the stomach moves in line with the oesophagus, often causes reflux oesophagitis, which may give rise to ulceration and stenosis. Haematemesis may occur. It is caused by raised intra-abdominal pressure.
- Paraesophageal hernia, where part of the stomach, along with its peritoneal covering, passes up into the thorax by the side of the oesophagus. The gastro-oesophageal junction still remains below the diaphragm, and the angle between the oesophagus and stomach is maintained. There is no reflux oesophagitis in this type of hernia. The main symptom is dyspnoea on exertion due to the position of the stomach in the thorax, and sometimes bleeding.
Diagnosis is typically through a barium swallow. Treatment may be surgical to reduce the hernia and repair the diaphragm. Conservative management includes lifestyle changes like raising the head while sleeping, avoiding smoking, reducing obesity, using antacids or proton pump inhibitors and attention to the causes that raise intra-abdominal pressure.
Congenital anomalies and fistulas
1. Congenital Oesophageal Stenosis. It primarily affects the middle and distal oesophagus. Usually asymptomatic, severe cases may cause failure to thrive and regurgitation, often becoming apparent when infants start solid foods. Symptoms include dysphagia, coughing, and vomiting. Diagnosis is through radiography and endoscopy, with treatment options like bougienage or endoscopic laser removal of webs.
2. Short Oesophagus. It is a rare congenital condition, often debated as a true entity or a form of congenital hiatus hernia. It involves a shortened oesophagus with an intra-thoracic stomach. Affected infants present with failure to thrive, and symptoms are similar to reflux oesophagitis. Diagnosis is made using contrast radiography and endoscopy. Treatment is difficult and may involve surgical procedures similar to those for reflux esophagitis.
3. Tracheoesophageal Fistula. It is a congenital or acquired connection between the oesophagus and trachea, sometimes accompanied by atresia. Symptoms include choking, dyspnea, cyanosis, and recurrent aspiration pneumonia. Diagnosis is confirmed through contrast radiography and endoscopy, with inability to pass an NG tube in newborns being a strong indicator. Treatment involves surgical separation and reconstruction of the trachea and oesophagus, either through a cervical or thoracic approach ,depending on the fistula’s location.
Neoplasms of the Oesophagus
1. Benign tumours. They are rare, with leiomyoma being the most common (two-thirds) of all benign cases. It arises from the smooth muscle in the oesophageal wall. It causes dysphagia when it grows beyond 5 cm. Diagnosis is through barium swallow and endoscopy, but biopsy is avoided due to the risk of perforation. Treatment involves enucleation of the tumour via thoracotomy. Other benign neoplasms include mucosal polyps, lipomas, fibromas, and haemangiomas, which are treated with surgical excision.
2. Malignant tumours, primarily oesophageal carcinoma, have a higher incidence in regions like China, Japan, and India, where lifestyle factors such as smoking, alcohol consumption, and tobacco chewing contribute significantly. Squamous cell carcinoma accounts for 93% of cases, with adenocarcinoma seen mainly in the lower oesophagus. The cancer can spread through direct invasion, lymphatic spread, or the bloodstream, potentially affecting nearby organs such as the trachea, lungs, or liver.
Clinical features of oesophageal cancer include early symptoms like substernal discomfort and progressive dysphagia, which initially affects solid foods but later extends to liquids. Weight loss and emaciation follow, with pain often indicating advanced disease. Aspiration pneumonia can result from laryngeal paralysis or fistula formation.
Diagnosis is made using barium swallow, oesophagoscopy for biopsy, and CT scans to evaluate metastases. Treatment for upper oesophageal cancer is primarily radiotherapy due to the complexity of surgery in this region. Surgery is the preferred option for cancer in the lower oesophagus, where the affected segment can be excised with a portion of the stomach. Palliative care options for advanced cases include oesophageal intubation, gastrostomy, or laser surgery to maintain a food channel. Chemotherapy is reserved for palliative care in advanced or widespread disease.
The prognosis for oesophageal carcinoma is poor, with a five-year survival rate of only 5–10%.
Miscellaneous Causes of Oesophageal Conditions
1. Benign Strictures of the Oesophagus. Benign oesophageal strictures typically occur due to damage to the oesophageal muscular layer. Several factors contribute to the formation of these strictures:
-
- Burns from ingestion of corrosive substances or hot fluids.
- Trauma is caused by impacted foreign bodies, surgical instruments, or external injuries.
- Ulceration due to reflux oesophagitis.
- Infections such as diphtheria or typhoid cause ulceration.
- Postoperative anastomotic sites.
- Congenital strictures, usually occur in the lower third of the oesophagus.
Clinical Features and Diagnosis: The primary symptom is dysphagia, starting with difficulty swallowing solids and progressing to liquids. In cases of complete obstruction, patients may experience regurgitation and coughing. Malnutrition is common due to difficulty in swallowing. A barium swallow is typically used to confirm the diagnosis, while oesophagoscopy helps rule out malignancy.
Treatment: Treatment involves prograde dilation using bougies under direct vision with an oesophagoscope. Repeated dilations are often necessary. If dilation is unsuccessful, a gastrostomy can be performed to bypass the inflamed region and allow feeding. Surgical intervention, such as excision of the strictured segment and reconstruction using the stomach, colon, or jejunum, may be required in severe cases.
2. Globus Pharyngeus. Globus pharyngeus, often referred to as “Globus sensation,” is a functional disorder where patients experience a persistent sensation of a lump or foreign body in the throat. This sensation is more pronounced between meals and should not be confused with true dysphagia. Patients often express concerns about throat cancer.
Clinical Considerations: It is essential to conduct a thorough examination of the pharynx, larynx, and base of the tongue, as well as flexible nasal endoscopy and barium swallow, to rule out any inconspicuous lesions in the hypopharynx or oesophageal malignancies. In the absence of any organic cause, reassurance is the primary treatment.
3. Pharyngeal Pouch. A pharyngeal pouch, also known as Zenker’s diverticulum or hypopharyngeal diverticulum, is a condition where the pharyngeal mucosa herniates through a weak point in the pharyngeal wall. This weakness occurs between two parts of the inferior constrictor muscle: the oblique fibers of the thyropharyngeus muscle and the horizontal fibers of the cricopharyngeus muscle. The area between these muscles forms a triangular region called Killian’s dehiscence, which is particularly vulnerable to herniation. The pharyngeal pouch usually develops in the midline of the pharynx and expands to one side, most commonly the left. It is thought to result from uncoordinated swallowing movements or spasms of the cricopharyngeal sphincter, though the exact cause remains unclear. This condition typically affects individuals over the age of 60.
Clinical Features: Patients present with dysphagia that worsens after several swallows as the pouch fills with food, exerting pressure on the oesophagus. Symptoms may include a gurgling sound on swallowing, regurgitation of undigested food, and aspiration pneumonia. Long-standing cases may lead to malnutrition and, rarely, carcinoma. In some cases, there is a noticeable swelling on the left side of the neck.
Diagnosis and Treatment: Barium swallow reveals the size and location of the pouch. During a laryngoscopy, pooling of saliva may be observed, and the “rising tide” sign, where small amounts of swallowed liquid rise back up from the postcricoid region, may be noted. Occasionally, a soft, compressible swelling is visible in the anterior triangle of the neck, indicating the presence of the pouch. Treatment options include excision of the pouch combined with cricopharyngeal myotomy through a cervical approach. In debilitated patients, Dohlman’s procedure or endoscopic laser treatment may be employed to divide the partition between the pouch and oesophagus.
4. Schatzki’s Ring. Schatzki’s ring, also known as the lower oesophageal ring, is a narrowing at the squamocolumnar junction of the oesophagus. It typically occurs in individuals over the age of 50 and may be associated with hiatal hernia.
Symptoms and Treatment: Patients often experience intermittent dysphagia and, in some cases, bolus obstruction. Treatment involves oesophageal dilatation to relieve the obstruction.
———— End of the chapter ————
Download full PDF Link:
Disorders of Oesophagus Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Juvenile Angiofibroma. https://www.entlecture.com/juvenile-angiofibroma/
- Please read. Tumours of Hypopharynx . https://www.entlecture.com/tumours-of-the-hypopharynx/
- Please read. Anatomy of Oesophagus. https://www.entlecture.com/anatomy-of-oesophagus/
Keywords: Oesophagus, Corrosive burns, Foreign body ingestion, Perforations and rupture, Mallory-Weiss syndrome, GERD, Plummer–Vinson syndrome, cardiac achalasia, Oesophageal varices, Hiatus hernia, Tracheoesophageal Fistula, Globus pharyngeus, Pharyngeal pouch, Schatzki’s ring.