INTRODUCTION OF ADENOIDS
In 1724, Santorini first described the nasopharyngeal lymphoid aggregate, initially terming it Luschka’s tonsil. However, the term “adenoids” was later coined by Wilhelm Meyer in 1870. Fundamentally, the adenoids are a group of subepithelial lymphoid tissue, often referred to as mucosa-associated lymphoid tissue (MALT), situated in the nasopharynx. Importantly, they form an integral part of Waldeyer’s ring, a crucial collection of lymphoid tissue strategically located at the entrance of the upper respiratory and digestive tracts.
FUNCTION OF ADENOIDS
The adenoids play a vital role in a child’s developing immune system, serving as an important immunological organ. Therefore, understanding their functions is paramount.
- Immune System’s First Line of Defence: In young children, the adenoids act as an initial sentinel. They are the first point of contact for inhaled germs or allergens with the body’s immune cells. This early interaction is crucial as it helps to initiate and accelerate the development of natural immunity.
- Antibody Production: As a key component of Waldeyer’s ring, the primary function of the adenoids is to produce important antibodies, particularly IgG and IgA. These antibodies are essential in protecting the body from various infections.
- Developing Immune Memory: Early and repeated exposure to different pathogens through the nasal and oral cavities helps the adenoids “remember” these invaders. This process is critical for building a robust and lasting immune system, ultimately contributing to a child’s long-term immunity.

ANATOMY OF ADENOIDS
The nasopharyngeal tonsil, commonly referred to as the “adenoids,” is located where the roof and posterior wall of the nasopharynx meet. It consists of vertical ridges of lymphoid tissue separated by deep clefts. Remember, among all the tonsils forming Waldeyer’s ring (palatine, lingual, pharyngeal/adenoid, tubal), only the palatine tonsils possess a true fibrous capsule and prominent crypts. This is a frequently asked question in exams.
HISTOLOGY OF ADENOIDS
The surface of the adenoid is covered by three types of epithelium (mixed epithelium):
- Ciliated pseudostratified columnar: This is the predominant type, similar to the respiratory epithelium found elsewhere in the upper respiratory tract. It aids in mucociliary clearance.
- Stratified squamous
- Transitional.
PHYSIOLOGY OF ADENOIDS
Adenoid tissue is already present at birth and undergoes physiological enlargement until about 6-7 years of age. After this point, the size of the adenoids typically plateaus, but the nasopharynx itself continues to increase in size with age. Therefore, while the adenoids may not be actively growing larger, their proportion to the expanding nasopharynx makes them appear comparatively smaller. Subsequently, after the age of 7 years, the adenoid tissue begins a process of atrophy, continuing until puberty (12 years). Regression of this lymphoid tissue then accelerates rapidly after around twenty years of age in most individuals, eventually leading to its almost complete disappearance by the age of twenty. Clinical symptoms related to the adenoids are more common in younger children due to the smaller volume of the nasopharynx and the higher frequency of upper respiratory tract infections.

BLOOD SUPPLY, VENOUS DRAINAGE, LYMPHATICS & NERVE SUPPLY OF ADENOIDS
Blood supply. Adenoids receive their blood supply from:
- Ascending palatine branch of facial artery.
- Ascending pharyngeal branch of external carotid artery.
- Pharyngeal branch of the third part of maxillary artery.
- Ascending cervical branch of inferior thyroid artery of thyrocervical trunk.
Venous drainage is through the internal jugular and facial veins.
Lymphatics from the adenoids drain into upper jugular nodes directly or indirectly via retropharyngeal (nodes of Rouvier) and parapharyngeal nodes.
Nerve Supply: The adenoids receive sensory innervation from Cranial Nerves IX (Glossopharyngeal) and X (Vagus). These nerves carry sensation, and importantly, referred pain to the ear due to adenoiditis is also mediated through them. Therefore, earache can be a presenting symptom of adenoid inflammation.
AETIOLOGY OF ADENOID HYPERTROPHY
Enlarged adenoids often result from repeated inflammation and infection. Several factors contribute to adenoid hypertrophy:
- Recurrent attacks of rhinitis
- Sinusitis
- Chronic tonsillitis.
- Allergy of the upper respiratory tract

CLINICAL FEATURES
Symptoms and signs of adenoid enlargement are influenced not only by the absolute size of the adenoid mass but also by the available space in the nasopharynx. Enlarged and infected adenoids can cause nasal, aural (ear), or general symptoms.
Nasal Symptoms
- Nasal Obstruction: The most common symptom, leading to mouth breathing. Nasal obstruction interferes with feeding or suckling in children, as respiration and feeding cannot occur simultaneously, causing failure to thrive.
- Nasal Discharge: Partly due to choanal obstruction, preventing normal nasal secretions from draining into the nasopharynx, and partly due to associated chronic rhinitis. This often results in a wet, bubbly nose.
- Recurrent Sinusitis: Chronic maxillary sinusitis is commonly associated with adenoids due to persistent nasal discharge and infection. Conversely, primary maxillary sinusitis can lead to infected and enlarged adenoids.
- Epistaxis: Acute inflammation of the adenoids can cause nosebleeds with nose blowing.
- Voice Change: Nasal obstruction leads to a hyponasal voice (rhinolalia clausa), which is devoid of its normal nasal quality. This is a tell-tale sign of nasopharyngeal obstruction.
- Olfaction: Adenoidal hyperplasia may reduce olfactory sensitivity, particularly affecting retronasal smell and taste.
Ear Symptoms
- Tubal Obstruction: An adenoid mass can block the eustachian tube, leading to a retracted tympanic membrane and conductive hearing loss.
- Recurrent Acute Otitis Media: Infections can spread via the eustachian tube, causing recurrent episodes of acute otitis media.
- Chronic Suppurative Otitis Media: This condition may persist in the presence of infected adenoids.
- Otitis Media with Effusion (OME) / “Glue Ear”: Adenoids are a significant cause of OME in children. Fluctuating adenoid sizes can cause intermittent eustachian tube obstruction and, consequently, fluctuating hearing loss.
General Symptoms
- Adenoid Facies: Chronic nasal obstruction and mouth breathing lead to a characteristic facial appearance known as adenoid facies. This is marked by an elongated face, a dull and vacant expression, a persistently open mouth, prominent and crowded upper teeth (prognathism), a hitched-up upper lip, and a pinched-in nose due to disuse atrophy of the alae nasi. Furthermore, the hard palate becomes highly arched because the moulding action of the tongue is lost.
- Apneic Spells / Obstructive Sleep Apnea (OSA): These may occur when there is total or near-total nasal obstruction due to severe adenoid hypertrophy. An apneic spell is clinically defined as the complete cessation of breathing for a minimum duration of 10 seconds. The diagnosis of OSA is often made if a child experiences 30 or more apneic spells in 7 hours of sleep or, more practically for screening, more than 5 apneic spells per hour of sleep (Apnea-Hypopnea Index > 5/hour). OSA due to adenoid hypertrophy can significantly impact a child’s development, behaviour (e.g., hyperactivity, poor concentration), and cardiovascular health.
- Pulmonary Hypertension and Cor Pulmonale: Long-standing nasal obstruction or obstructive sleep apnoea will lead to chronic hypoxia, causing pulmonary vasoconstriction. Over time, this can lead to pulmonary hypertension and, if left untreated, can lead to cor pulmonale.
- Aprosexia: Lack of concentration due to daytime fatigue and irritability.
DIAGNOSIS OF ADENOID HYPERTROPHY
Accurate diagnosis is crucial for appropriate management. A multi-pronged approach is usually employed:
- Clinical Examination:
- Rigid or Flexible Nasopharyngoscopy: This is the gold standard for direct and detailed visualisation of the adenoids and the entire nasopharyngeal space, especially in a cooperative child. Flexible scopes are often preferred in younger children due to better tolerance.
- Posterior Rhinoscopy: Using a post-nasal mirror to visualise the adenoid mass directly is a classical method, though often challenging in young, uncooperative children.
- Anterior Rhinoscopy: May show signs of rhinitis or purulent discharge.
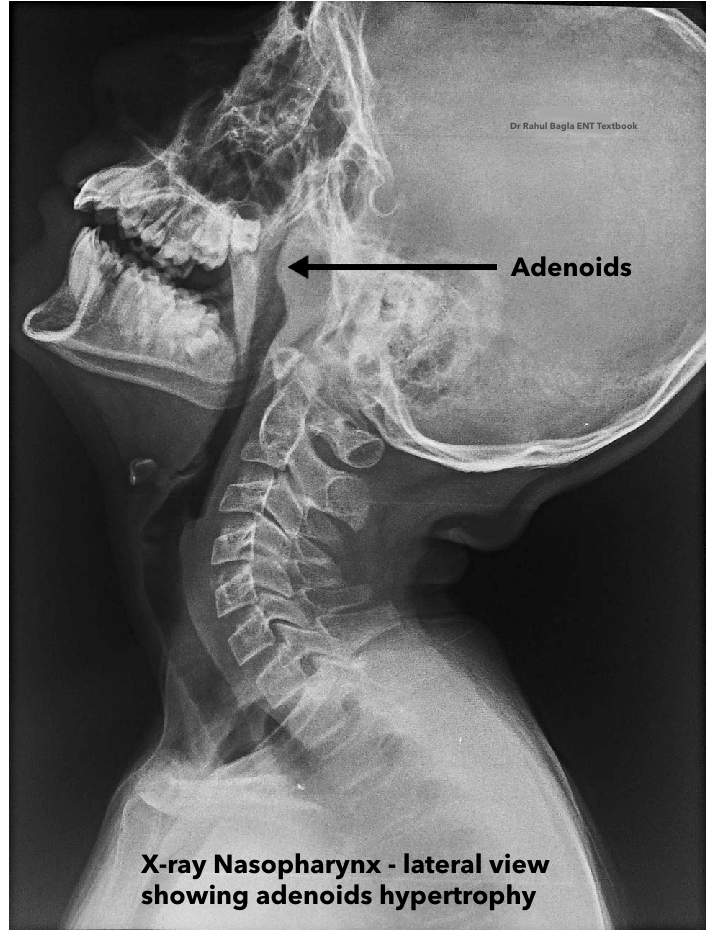
- Radiological Examination:
- Soft tissue lateral view radiograph of the nasopharynx: This is a valuable, non-invasive imaging modality. It can reveal the size of the adenoids and, more importantly, the extent of nasopharyngeal air space compromise.
Important for Viva: An examiner might ask you to differentiate between an enlarged adenoid and an antrochoanal (AC) polyp on a lateral radiograph. Remember this key distinction: in the case of an AC polyp, you will see a column of air present along the posterior and superior walls of the nasopharynx, which is absent with a true adenoid mass. This is because the AC polyp arises from the maxillary sinus and extends into the nasopharynx, leaving an air column around its pedicle.
- Soft tissue lateral view radiograph of the nasopharynx: This is a valuable, non-invasive imaging modality. It can reveal the size of the adenoids and, more importantly, the extent of nasopharyngeal air space compromise.
- Rule Out Other Causes: A thorough nasal examination should always be conducted to meticulously exclude other potential causes of nasal obstruction, as they can mimic adenoid hypertrophy.
DIFFERENTIAL DIAGNOSIS
It is imperative to consider other conditions that can present with similar symptoms, particularly nasal obstruction. These include:
- Choanal atresia: A congenital condition where the posterior nasal passages (choanae) are blocked.
- Foreign bodies in the nose: Commonly seen in children, leading to unilateral nasal obstruction and foul-smelling discharge.
- Nasopharyngeal angiofibroma: A benign, highly vascular tumour predominantly seen in adolescent males, causing recurrent epistaxis and nasal obstruction.
- Malignant tumours of the nasopharynx: Particularly of mesenchymal origin (e.g., rhabdomyosarcoma) in children, or nasopharyngeal carcinoma (rare in children) which can cause unilateral nasal obstruction, ear symptoms, and cranial nerve palsies.
- Dental causes: Positional anomalies of the teeth and malocclusion, while often secondary to adenoid facies, can sometimes be part of a broader syndrome or have primary dental origins.
TREATMENT
Conservative Management
For mild symptoms, conservative approaches are often effective:
- Breathing exercises: To encourage nasal breathing.
- Decongestant nasal drops (short-term): To reduce nasal swelling and improve airflow. However, prolonged use should be avoided due to the risk of rhinitis medicamentosa.
- Nasal saline irrigation: Helps to clear mucus and reduce inflammation.
- Antihistamines or intranasal corticosteroids: For coexistent nasal allergy, these can significantly alleviate the condition by reducing allergic inflammation and associated adenoid swelling.
Surgical Management
Adenoidectomy🔗 is the indicated treatment for marked symptoms or when conservative measures fail. It’s important to remember that adenoidectomy is often performed in combination with other procedures, addressing the full scope of a child’s condition.
- Adenotonsillectomy: In cases where both enlarged tonsils and adenoids are causing issues, such as obstructive sleep apnea (OSA) or recurrent infections, both are removed in a combined procedure.
- Adenoidectomy with Myringotomy and Grommet Insertion: Adenoid hypertrophy is a significant contributor to otitis media with effusion (OME), also known as “glue ear.” Therefore, if the child has bilateral serous otitis media causing hearing loss, a myringotomy (a small incision in the eardrum) is performed to drain the fluid, followed by the insertion of a grommet (a tiny ventilation tube) to prevent fluid from re-accumulating. This combined procedure is very common and highly effective.
———— End of the chapter ————
High-Yield Points for Revision
- Discovery: Santorini (Luschka’s tonsil, 1724); Meyer (adenoids, 1870).
- Location: Roof and posterior wall of nasopharynx.
- Waldeyer’s Ring Components: Palatine, Lingual, Pharyngeal (Adenoid), Tubal tonsils.
- Unique Tonsil Feature: Only palatine tonsils have a true fibrous capsule and prominent crypts.
- Epithelium of Adenoids: Mixed: Ciliated pseudostratified columnar (most common), stratified squamous, transitional.
- Physiological Enlargement: Up to 6-7 years; atrophy after 7 years, nearly disappears by 20.
- Blood Supply Mnemonic (APMPA): Ascending Palatine, Maxillary (Pharyngeal branch), Pharyngeal (Ascending), Ascending Cervical.
- Referred Pain to Ear: Via CN IX (Glossopharyngeal) and CN X (Vagus).
- Most Common Symptom: Nasal obstruction and mouth breathing.
- Voice Change: Hyponasal voice (rhinolalia clausa).
- Adenoid Facies Features: Open mouth, dull expression, crowded upper teeth, high-arched palate, pinched nose.
- Gold Standard Diagnosis: Nasopharyngoscopy (flexible or rigid).
- Radiological View: Lateral soft tissue view of nasopharynx.
- Key Differential Diagnosis: Nasopharyngeal angiofibroma (adolescent males, epistaxis).
- OSA Definition (Children): >5 apneic spells/hour of sleep (Apnea-Hypopnea Index).
- Serious Complications: Pulmonary hypertension, cor pulmonale.
MCQs
Test your knowledge with these practice questions!
- Which of the following tonsils forming Waldeyer’s ring possesses a true fibrous capsule and prominent crypts? A) Lingual tonsil B) Tubal tonsil C) Pharyngeal tonsil (Adenoid) D) Palatine tonsil
- A 5-year-old child presents with chronic mouth breathing, dull facial expression, and a high-arched palate. This characteristic appearance is known as: A) Treacher Collins syndrome B) Adenoid facies C) Pierre Robin sequence D) Crouzon syndrome
- The primary sensory nerve supply to the adenoids, which also mediates referred pain to the ear in adenoiditis, is derived from: A) Facial nerve (CN VII) B) Trigeminal nerve (CN V) C) Glossopharyngeal nerve (CN IX) and Vagus nerve (CN X) D) Hypoglossal nerve (CN XII)
- Physiological enlargement of adenoid tissue typically occurs until what age? A) 2-3 years B) 6-7 years C) 10-12 years D) 15-18 years
- Which of the following is considered the gold standard for direct visualization and diagnosis of adenoid hypertrophy? A) Soft tissue lateral view radiograph of the nasopharynx B) Digital palpation of the postnasal space C) Rigid or flexible nasopharyngoscopy D) Anterior rhinoscopy
- A 7-year-old boy presents with recurrent episodes of acute otitis media (4 episodes in the last 6 months) and a persistent conductive hearing loss. Which of the following is the most likely contributing factor related to adenoids? A) Adenoid abscess B) Adenoid atrophy C) Tubal obstruction due to adenoid hypertrophy D) Nasopharyngeal angiofibroma
- Which of the following is NOT a typical component of the mixed epithelium covering the surface of the adenoid? A) Ciliated pseudostratified columnar B) Stratified squamous C) Simple cuboidal D) Transitional
- A child diagnosed with Obstructive Sleep Apnea (OSA) due to adenoid hypertrophy is likely to present with which of the following general symptoms? A) Cor pulmonale in early stages B) Decreased incidence of upper respiratory tract infections C) Aprosexia and poor school performance D) Weight gain due to increased appetite
- Which arterial branch is typically not a primary blood supply to the adenoids? A) Ascending palatine branch of facial artery B) Ascending pharyngeal branch of external carotid artery C) Superficial temporal artery D) Pharyngeal branch of maxillary artery
- A 4-year-old child with chronic nasal obstruction and mouth breathing is suspected of having enlarged adenoids. Which radiological investigation is most commonly used to assess the size of the adenoids and the extent of nasopharyngeal airway compromise? A) CT scan of paranasal sinuses B) MRI of the nasopharynx C) Soft tissue lateral view radiograph of the nasopharynx D) Chest X-ray
MCQ Answers and Explanations
- D) Palatine tonsil: Only palatine tonsils have a true fibrous capsule and prominent crypts, a key distinguishing feature.
- B) Adenoid facies: This is the classic description of the characteristic facial changes associated with chronic nasal obstruction due to adenoid hypertrophy.
- C) Glossopharyngeal nerve (CN IX) and Vagus nerve (CN X): These cranial nerves provide sensory innervation to the adenoids and mediate referred pain.
- B) 6-7 years: Adenoids physiologically enlarge until about 6-7 years before starting to atrophy.
- C) Rigid or flexible nasopharyngoscopy: Direct visualisation using a scope offers the most detailed and accurate assessment.
- C) Tubal obstruction due to adenoid hypertrophy: Enlarged adenoids can block the Eustachian tube, leading to negative middle ear pressure, effusion, and recurrent infections.
- C) Simple cuboidal: The adenoid surface is covered by ciliated pseudostratified columnar, stratified squamous, and transitional epithelium, not simple cuboidal.
- C) Aprosexia and poor school performance: Chronic sleep deprivation from OSA leads to daytime fatigue, irritability, and difficulty concentrating (aprosexia), affecting academic performance. Cor pulmonale is a late complication.
- C) Superficial temporal artery: The superficial temporal artery is a branch of the external carotid artery, supplying the temporal region, not the adenoids. The other options are documented blood supplies.
- C) Soft tissue lateral view radiograph of the nasopharynx: This is the most common and cost-effective radiological method to assess adenoid size and the airway space.
Clinical-Based Questions (Practical & Viva Scenarios)
These questions prepare you for real-world patient encounters and examiner queries.
- Case Scenario: A 6-year-old boy is brought to your ENT OPD with complaints of chronic mouth breathing, snoring loudly at night, and recurrent ear infections for the past year. His mother also reports that he often seems tired during the day and has difficulty concentrating in school. On examination, you notice an open mouth posture, a dull expression, and prominent upper incisors.
- a) What is your most likely diagnosis?
- Answer: Adenoid hypertrophy with associated Obstructive Sleep Apnea (OSA) and Otitis Media with Effusion/Recurrent Acute Otitis Media.
- b) What specific physical examination findings would you look for to support your diagnosis?
- Answer: Adenoid facies (elongated face, open mouth, dull expression, high-arched palate, crowded teeth, pinched nose), evidence of mouth breathing, nasal discharge, retracted tympanic membrane or fluid level in the middle ear (on otoscopy), and possibly nasal obstruction on anterior rhinoscopy.
- c) What investigations would you order to confirm your diagnosis and assess the severity?
- Answer: Flexible nasopharyngoscopy (gold standard for direct visualisation), soft tissue lateral view radiograph of the nasopharynx (to assess adenoid size and airway space), impedance audiometry (tympanometry) to assess middle ear status (looking for Type B or C tympanogram), and potentially polysomnography (sleep study) if OSA severity needs objective quantification.
- d) Outline your management plan for this child.
- Answer: Given the significant symptoms (OSA, recurrent ear infections, impact on school), adenoidectomy is strongly indicated. If there’s associated OME, a myringotomy with grommet insertion would also be performed concurrently. Post-operatively, educate parents on expected recovery and potential for continued improvement in symptoms. Address any co-existing allergic rhinitis with nasal corticosteroids.
- a) What is your most likely diagnosis?
- Viva Question: “Doctor, can you explain the concept of ‘referred pain’ in the context of adenoiditis and its anatomical basis?”
- Answer: “Yes, sir/ma’am. Referred pain to the ear in adenoiditis is a common clinical symptom. The anatomical basis lies in the shared sensory innervation of the adenoids and the ear. The adenoids receive sensory innervation primarily from the glossopharyngeal nerve (CN IX) and the vagus nerve (CN X). The glossopharyngeal nerve also supplies the middle ear (Jacobson’s nerve) and the Eustachian tube. Similarly, the auricular branch of the vagus nerve (Arnold’s nerve) supplies the external auditory canal. When the adenoids are inflamed, noxious stimuli are transmitted via these nerves. Due to the convergence of afferent nerve fibres from both the nasopharynx and the ear in the brainstem, the brain misinterprets the origin of the pain, perceiving it as coming from the ear. Thus, adenoid inflammation can manifest as otalgia without primary ear pathology.”
- Clinical Tip: “When examining a child with suspected adenoid hypertrophy, what is a crucial differential diagnosis you must consider, especially if there’s unilateral epistaxis in an adolescent male?”
- Answer: “A crucial differential diagnosis, particularly in an adolescent male with unilateral nasal obstruction and recurrent epistaxis, is Nasopharyngeal Angiofibroma. This is a benign but highly vascular tumor originating from the nasopharynx, which can grow significantly and cause severe bleeding. It’s vital to consider this to avoid a catastrophic haemorrhage if a biopsy is performed without proper pre-operative planning.”
FAQ’s in Viva
- What are adenoids?
- Adenoids are a collection of lymphoid tissue (similar to tonsils) located at the back of the nose (nasopharynx), part of the immune system’s first line of defence.
- What are the common symptoms of enlarged adenoids?
- Common symptoms include chronic mouth breathing, nasal obstruction, snoring, recurrent ear infections, and sometimes a characteristic “adenoid facies.”
- How are enlarged adenoids diagnosed?
- Diagnosis typically involves clinical examination, flexible nasopharyngoscopy for direct visualisation, and a soft tissue lateral view X-ray of the nasopharynx.
- Can adenoid hypertrophy cause sleep problems?
- Yes, significant adenoid hypertrophy can lead to Obstructive Sleep Apnea (OSA), causing snoring, restless sleep, daytime fatigue, and difficulty concentrating.
- Is adenoidectomy a common surgery in children?
- Yes, adenoidectomy is one of the most common surgical procedures performed in children, primarily indicated for persistent symptoms like chronic obstruction or recurrent infections impacting quality of life.
- Do adenoids grow back after surgery?
- While uncommon, adenoid tissue can occasionally regrow after adenoidectomy, especially if the removal was incomplete or if performed in very young children.
- What is “adenoid facies”?
- Adenoid facies is a characteristic facial appearance caused by chronic mouth breathing due to enlarged adenoids, featuring an open mouth, dull expression, high-arched palate, and crowded upper teeth.
———— End ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page:https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Juvenile Angiofibroma. https://www.entlecture.com/juvenile-angiofibroma/
- Please read. Tumours of Hypopharynx . https://www.entlecture.com/tumours-of-the-hypopharynx/
- Please read. Anatomy of Oesophagus. https://www.entlecture.com/anatomy-of-oesophagus/
Keywords: Learn everything about adenoids in ENT for MBBS and ENT PG exams, including anatomy, functions, clinical features, viva questions, NEET PG MCQs, and treatment. Includes diagrams, mnemonics, and high-yield points. ENT topics for NEET PG, MBBS ENT notes, ENT viva questions, Adenoids anatomy, Adenoid hypertrophy symptoms, Adenoidectomy indications, Obstructive sleep apnea in children, Waldeyer’s ring, Adenoid facies explanation, Otitis media with effusion adenoids, Nasal obstruction in children, Adenoids diagnosis, Adenoids treatment, CBME ENT curriculum, Medical education ENT, ENT quick revision, Clinical ENT cases, ENT exam preparation, Adenoid anatomy for MBBS students, Adenoids location in nasopharynx, Adenoid function in immune system, Histology of adenoid tissue in nasopharynx, Blood and nerve supply of adenoid tonsil, Adenoid growth regression with age, Adenoid hypertrophy symptoms in children, Adenoid facies features exam notes, Adenoid MALT tissue functions, Nasopharyngeal tonsil clinical anatomy, Adenoid lymphatic drainage nodes, Referred ear pain in adenoiditis mechanism, Adenoid hypertrophy management ENT, Adenoidectomy indications and contraindications, Adenoid vs tonsil histology differences, Adenoid regression age 15 to 20 years, Clinical features of adenoid hypertrophy, Adenoid nerve supply, glossopharyngeal vagus, Adenoid hypertrophy, OME conductive hearing loss, Adenoid facies description pediatric ENT, What are adenoids and their function, Symptoms of swollen adenoids in children, Adenoidectomy recovery tips for parents, Natural remedies for enlarged adenoids, Adenoids and breathing problems in kids, Adenoid-related ear infections treatment, Adenoids vs tonsils: key differences, When do adenoids need to be removed, Adenoid issues and sleep apnea connection, How to diagnose adenoid problems at home, Adenoids explained: symptoms, treatments, and when to seek help, Swollen adenoids in children: causes and effective remedies, Everything you need to know about adenoidectomy recovery, The role of adenoids in your child’s health: what to watch for, Natural remedies for enlarged adenoids: a parent’s guide, Adenoids and sleep apnea: how they’re connected, Adenoids vs. Tonsils: understanding the differences and care tips, When should adenoids be removed? Signs and expert advice, Common myths about adenoids debunked: what parents should know, How to diagnose and manage adenoid issues at home, The nasopharyngeal tonsil, commonly referred to as the “adenoids,” is located where the roof and posterior wall of the nasopharynx meet, adenoidectomy recovery tips, natural remedies for swollen adenoids, adenoid hypertrophy in adults, adenoids and sleep apnea connection, endoscopic adenoid removal procedure, adenoid-related ear infections in children, diet after adenoid surgery, adenoid regrowth symptoms, adenoid biopsy procedure details, adenoid cystic carcinoma prognosis
Consize, thorough and well explanatory. Very helpful for us as UG students
Thank you, Dr Rahul!
Best book for complete explanation of each topic of ENT. Each and every concept has been explained so well.