Carcinoma of the Oral Cavity
Oral cancer is a major health concern worldwide, with India experiencing a particularly high incidence compared to Western countries. In India, the age-adjusted incidence rate for oral cancer stands at 44.8 per 100,000 males and 23.7 per 100,000 females, compared to just 11.2 per 100,000 in the United States. The majority of these cancers are squamous cell carcinomas, comprising over 90% of cases.
Aetiology of Oral Cavity Cancer
Oral cavity cancers are primarily caused by lifestyle choices and environmental factors. Smoking, tobacco chewing, alcohol consumption, dietary deficiencies, dental sepsis, and infections are key risk factors for the development of oral cancer.
- Smoking. Tobacco use, particularly smoking, is a major contributor, with over 90% of patients having a history of smoking. Tobacco contains over 30 carcinogens, such as polycyclic aromatic hydrocarbons and nitrosamines, which are strongly linked to cancer. Smokers are six times more likely to develop oral cancer than non-smokers. Unique practices like “reverse smoking,” seen in India, where the burning end of a cigarette is placed inside the mouth, significantly increase the risk of cancer in the hard palate. Additionally, pipe and cigar smokers are at higher risk due to the use of dark or air-cured tobacco, which is more carcinogenic than the blond tobacco in cigarettes.
- Tobacco chewing is another prevalent practice, particularly in India, where powdered tobacco mixed with lime is placed in the mouth. Products like chutta, paan, and khaini contribute to carcinoma development due to prolonged exposure to harmful substances. Chewing paan, a mixture of betel leaf, lime, and tobacco, lowers the mouth’s pH, releasing alkaloids from tobacco and areca nut, increasing cancer risk. This habit is associated with alveolobuccal cancer and oral submucous fibrosis, a premalignant condition that causes stiffening of oral tissues.
- Alcohol consumption synergistically further elevates cancer risk, particularly in the upper aerodigestive tract, with heavy drinkers facing up to six times higher risk than non-drinkers. Alcohol acts as a solvent, enhancing the absorption of carcinogens and increasing cellular permeability. Its metabolite, acetaldehyde, causes local cell damage, and chronic alcohol use upregulates cytochrome P450 enzymes, activating procarcinogens.
- Dietary deficiencies, while not definitively linked to cancer, are suspected contributors. Riboflavin (vitamin B2) deficiency, particularly in alcoholics, may increase the risk of oral cancer. Paterson-Brown-Kelly syndrome, involving iron deficiency anaemia, predisposes individuals to cancers of the oral cavity. High intake of fruits and vegetables is associated with a reduced risk of head and neck cancer.
- Poor oral hygiene, dental sepsis, ill-fitting dentures, and chronic irritation from sharp teeth can lead to malignant changes in the oral mucosa. Continuous inflammation and mechanical irritation are significant contributors to oral cancer development.
- Infections also play a role, with viruses such as human papillomavirus (HPV), human immunodeficiency virus (HIV), herpes simplex virus (HSV), and Epstein-Barr virus (EBV) being implicated in the development of head and neck cancers.
Sites of Oral Cancer
Oral cancers can develop in various regions of the oral cavity, each with unique clinical presentations and treatment protocols. The sites for oral cavity cancers include:
- Mucosal Lip
- Buccal Mucosa
- Anterior Two-Thirds of the Tongue
- Hard Palate
- Alveolar Ridges (Upper and Lower)
- Floor of the Mouth
- Retromolar Trigone

Clinical Presentation and Treatment by Site
Oral cancer presents differently depending on the site of the lesion. Treatment varies based on the cancer’s location, stage, and extent of spread.
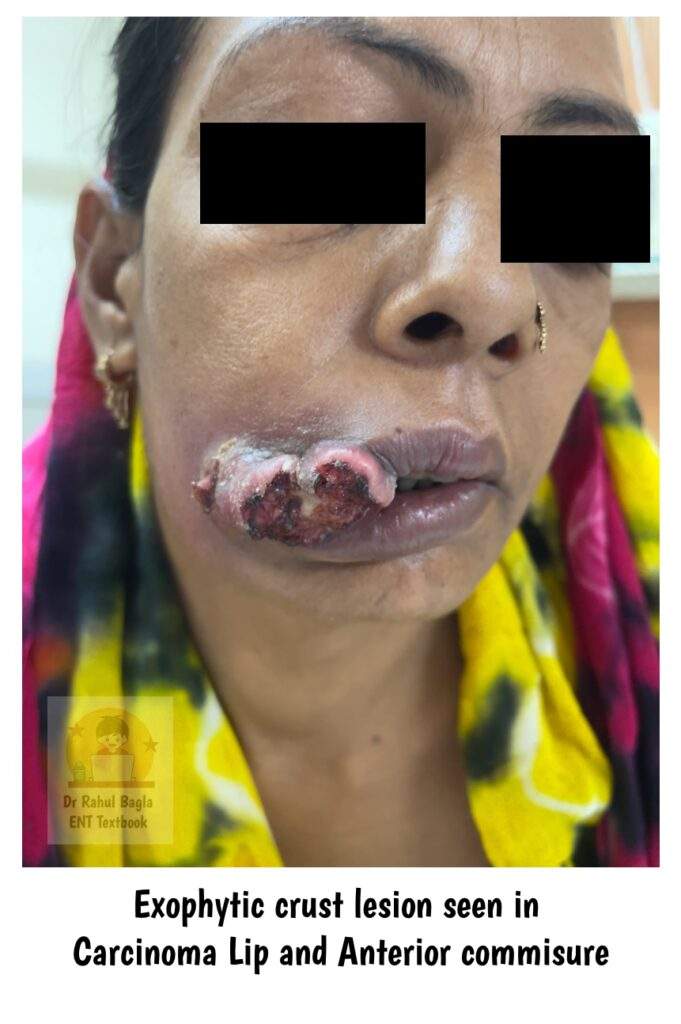
Carcinoma of the Lip
Lip cancer is the most prevalent malignant tumour in the head and neck region, exhibiting clinical behaviour similar to that of skin cancer. Key contributing factors include solar radiation, tobacco smoking, and viral infections. It occurs more frequently in males between the ages of 40 and 70 with male-to-female ratio of 95:5. Tumours predominantly arise in the lower lip (90%), while the upper lip (6-7%) and the oral commissure (3-4%).
- Anatomy. The lips form the anterior boundary of the oral vestibule. They consist of fleshy folds primarily made up of the orbicularis oris muscle, which is externally lined by skin and internally by mucous membrane. The inner surface of each lip is supported by a frenulum, a small fold of tissue that connects it to the gum. Notably, the upper lip has a median vertical groove on its outer surface called the philtrum. Lymphatic drainage of the central part of the lower lip is directed to the submental lymph nodes, while the remainder of the lower lip drains into the submandibular lymph nodes.
- Histological types. The most common histological type of lip cancer is squamous cell carcinoma, followed by basal cell carcinoma and tumours of the minor salivary glands, which generally affect the upper lip.
- Clinical features. Lip cancer usually manifests as an ulcerative or exophytic, crusted lesion. Adjacent areas may show crusting, colour changes, thinning, and various lesions of leukoplakia.
- Investigations. Only advanced stage tumours that are adherent to the mandible require CT or MRI for complete staging and treatment planning.
Treatment. For early-stage lip cancers, both surgical excision and radiation therapy yield similar outcomes. The ideal strategy for managing lip cancer involves simultaneous ablation and reconstruction. The primary goals for lip reconstruction are to maintain sensation, and mobility, prevent drooling, promote speech, and achieve acceptable cosmetic results. Full-thickness skin flaps incorporating skin, muscle, and mucosa are recommended whenever feasible. The repair approach should provide sufficient mucosa near the oral commissure to mitigate contracture risks.
Surgery
-
- Surgery of lower lip
-
- For small defects (less than 1/3rd of the lower lip) – Wedge excision (W-plasty or half W-plasty) can be done.
- For moderate defects (1/3rd to 2/3rd) – Abbe-Estlander flap or Karapandzic flap can be used.
- For large defects (greater than 2/3rd) may require larger cheek flaps or free tissue transfer. The common forms of cheek flap include the bilateral Gillies fan flaps or the Bernard–Webster cheek flap reconstruction.
-
- Surgery of upper lip.
-
- For small defects (less than 1/3rd of the upper lip) – Wedge excision and advancement flaps can be employed.
- For moderate defects (1/3rd to 2/3rd) – Perialar crescentic advancement flap, Reverse Karapandzic free flap, Abbe−Estlander flaps can be used
- For large defects (greater than 2/3rd) – Burrow-Diffenbach flap can be used.
Neck management. Squamous cell carcinoma has a favourable prognosis due to the early presentation, which often remains small and without palpable lymph nodes. Lymph node metastases occur late, with the submental and submandibular nodes being the first to show involvement. The presence of cervical lymph nodes at initial presentation signifies a poor prognosis. Lymph node metastases may require block dissection.
Radiotherapy Techniques. Radiotherapy is effective for early-stage cancers & elderly patients and achieves cure rates comparable to surgery. However, cosmetic results may be less satisfactory than surgical excision. For small tumour’s, external beam therapy with orthovoltage x-ray can be effectively utilized. Brachytherapy with 192-iridium is another option, typically involving multiple sessions within a week for total doses of 40 to 45 Gy. Photodynamic therapy is also viable, employing a sensitizing drug followed by light exposure to induce tumour apoptosis with minimal scarring compared to traditional methods.
Carcinoma of the Buccal Mucosa
The buccal mucosa is a large area that extends from the meeting point of the lips anteriorly to the pterygomandibular raphe posteriorly. It spans from the upper gingivobuccal sulcus to the lower gingivobuccal sulcus, covering the inside of the cheeks. Carcinoma of the buccal mucosa is highly prevalent, second only to tongue cancer, and is observed equally in both sexes. The most common site of origin is the angle of the mouth or the occlusal line where the upper and lower teeth meet. It can also arise in the buccal sulcus, where tobacco or “pan” quid is habitually placed, and may appear in multiple locations due to the extensive area involved.
- Gross Appearance. The lesions associated with buccal mucosa carcinoma can present in various forms, including verrucous, exophytic, or ulceroinfiltrative. The verrucous form often appears as a white papillary growth with significant keratinization. The exophytic type may be accompanied by erythroleukoplakia, while the ulceroinfiltrative type tends to infiltrate deeply into underlying tissues.
- Local Spread. Carcinoma of the buccal mucosa often spreads locally, involving deeper tissues from the submucosa to muscles, subcutaneous fat, and skin. Spread to the buccinator or anterior masseter muscles can lead to trismus (inability to open the mouth fully). Radial spread may involve adjacent structures, including the angle of the mouth, lip, retromolar trigone, and gingivobuccal sulci.
- Lymphatic Spread. Approximately 50% of patients experience lymphatic spread, typically involving the submandibular and upper jugular nodes. In some cases, the cancer may skip the submandibular group and spread directly to the upper jugular nodes.
- Clinical Features. Early stages of buccal mucosa carcinoma are usually asymptomatic. As the disease progresses, symptoms such as pain and bleeding become prominent, particularly when the lesion invades deeply or ulcerates. Advanced cases may present with a fungating mass over the cheek, foul-smelling oral lesions, and trismus due to muscle involvement.
- Histological Types. Squamous cell carcinoma is the most common histological type in buccal mucosa cancer. Tumours may also arise from minor salivary glands, exhibiting histology similar to salivary gland tumours.
- Diagnosis is confirmed through a biopsy, which determines the histological type of the tumour. Proper biopsy depth is essential to assess the extent of invasion, as tumours thicker than 5 mm are more likely to metastasize to the cervical lymph nodes. A computed tomography (CT) scan is used to assess the involvement of bone structures such as the mandible or maxilla and to evaluate the tumour’s extension into surrounding areas like the infratemporal fossa.
Treatment of carcinoma buccal mucosa. The standard treatment for buccal carcinoma primarily involves surgery, with postoperative radiotherapy (PORT) recommended for select patients. Early-stage tumours (T1/T2) are generally resected perorally, while advanced stages (T3/T4) may require more extensive procedures, including facial access incisions and bony resection of the maxilla or mandible. A resection margin of 1 cm is advised, with margins up to 2 cm when skin involvement is present. If imaging or clinical evidence suggests skin involvement, the external skin should be included in the specimen.
Primary site
- Stage I (T1N0): Early-stage tumours are treated with surgical excision alone.
- Stage II (T2N0): Radiotherapy is recommended if there is no bone involvement. If the tumour invades the bone or muscles, surgery, including excision, mandibulectomy, or maxillectomy, is preferred. Reconstruction with skin or mucosal flaps may be necessary.
- Stage III and IV: Advanced stages require tumour resection and reconstruction using skin or myocutaneous flaps, followed by radiotherapy. If lymph nodes are palpable, neck dissection is performed.
Neck Management. Regional spread typically involves ipsilateral level I and II lymph nodes. Comprehensive neck dissection is required for patients with palpable lymphadenopathy or pathological nodes. In cases with pathological nodes limited to level I, selective neck dissection (SND) from level I–III may be performed. Tumours larger than T2 or thicker than 5 mm warrant elective neck dissection for optimal disease control.
Carcinoma of the Oral Tongue
Carcinoma of the oral tongue primarily involves the anterior two-thirds of the tongue and is most commonly diagnosed in men aged between 50 and 70 years. However, cases in younger individuals and females are increasingly recognized, due to the rising prevalence of alcohol consumption among women. Among patients diagnosed with tongue cancer, approximately 70% report significant usage of both tobacco and alcohol as contributing factors. In some cases, oral tongue carcinoma can develop from pre-existing conditions such as leukoplakia, chronic dental ulcers, or syphilitic glossitis.
- Anatomy and Site of Origin. The oral tongue is defined as the freely mobile anterior two-thirds of the tongue and is demarcated from the base of the tongue by the circumvallate papillae located posteriorly. It is subdivided into several parts: the tip, dorsum, lateral borders, and ventral surface. The ventral and lateral surfaces connect with the floor of the mouth and are lined with nonkeratinizing stratified squamous epithelium. In contrast, the dorsum and tip of the tongue are covered by specialized gustatory mucosa, characterized by thick, primarily keratinized epithelium. Beneath the mucosal lining, the intrinsic muscles of the tongue, along with four pairs of extrinsic muscles (genioglossus, hyoglossus, styloglossus, and palatoglossus), provide functional support.
- Site. The most common sites for tumour development in the oral tongue are the middle of the lateral border and the ventral aspect (undersurface). Only 4-5% occur at the tip or on the dorsum of the tongue.
- Gross Appearance. Clinically, carcinoma of the oral tongue may present in various forms. Patients may observe exophytic lesions resembling papillomas, or they might identify nonhealing ulcers characterized by rolled edges, a greyish-white shaggy base, and induration. Furthermore, a submucosal nodule may be present along with induration of the surrounding tissue, indicating the progression of the disease.
- Local Spread. Carcinoma of the oral tongue can exhibit local spread, primarily infiltrating deep into the lingual musculature leading to complications such as ankyloglossia, a condition characterized by restricted tongue movement. Additionally, it may extend to adjacent structures, including the floor of the mouth, the alveolus and the mandible.
- Lymphatic Spread. In terms of lymphatic spread, carcinoma of the oral tongue is known to metastasize to various regional lymph nodes. The submandibular and upper jugular lymph nodes are commonly involved, particularly when the originates from the lateral border of the tongue. Tumours located at the tip of the tongue may spread to the submental lymph nodes and the jugulo-omohyoid group. It is also important to note that lymph node involvement can occur bilaterally or contralateral.
- Histopathology and Diagnostic Investigations. Majority of oral tongue carcinomas are squamous cell type, with most tumours categorized as well to moderately differentiated. Accurate assessment of tumour thickness is crucial for determining appropriate management strategies, particularly concerning the neck. Tumour thickness can be effectively evaluated using intraoral sonography. Biopsy techniques should aim to include both the deep margin of the tumour and the peripheral mucosa to know the tumour depth and facilitate histological grading, which is essential for assessing the risk of cervical metastasis.
Clinical features. The clinical presentation of oral tongue carcinoma can vary significantly depending on the stage of the disease.
- Painless Early Lesions: In the initial stages, lesions may be painless and remain asymptomatic for extended periods, leading to delayed diagnosis.
- Localized Pain: As the disease progresses, patients may experience localized pain at the site of the ulcer, which can indicate invasive growth or irritation.
- Referred Pain: Patients may also report pain in the ipsilateral ear. This phenomenon occurs due to shared innervation between the tongue, supplied by the lingual nerve, and the ear, innervated by the auriculotemporal nerve, both of which are branches of the mandibular division of the trigeminal nerve.
- Presence of a Lump: The formation of a palpable lump within the mouth can often signify the presence of a and warrants further investigation.
- Lymphadenopathy: Enlarged lymph nodes in the neck often accompany the condition, indicating lymphatic spread and necessitating evaluation of nodal involvement.
- Advanced Symptoms: Late-stage features of the disease may include dysphagia (difficulty swallowing), obstacles in protruding the tongue, slurred speech, and bleeding from the mouth. These symptoms often reflect significant burden and involvement of critical anatomical structures.
Treatment. The primary objectives in the treatment of oral tongue carcinoma involve treating the tumour itself, managing any neck disease associated with nodal metastasis, and preserving as much function of the tongue as possible. Surgical resection remains the gold standard, with the recommended practice being to resect the tumour with a 1 cm margin in three dimensions.
- For small tumours classified as T1N0, surgical resection and radiotherapy yield comparable outcomes.
- Tumours classified as T2N0 may also be effectively treated through radiotherapy, which includes the neck nodes to eliminate potential micrometastases, or through surgical excision accompanied by prophylactic neck dissection.
- Advanced-stage tumours (stage III or IV) require a combination of surgery and postoperative radiotherapy, as concurrent treatment enhances outcomes relative to standalone modalities.
Efforts to preserve the tip of the tongue during surgery are essential to maintaining optimal postoperative function while ensuring adequate oncological margins. Specific surgical approaches may include hemiglossectomy, which might incorporate portions of the floor of the mouth, segmental or hemimandibulectomy, along with block dissection of neck nodes, often referred to as the “commando operation.”
- Neck management. Typically, tumours of the oral tongue metastasize initially to levels I and II, with lateral tongue tumours frequently spreading directly to level II nodes. Although involvement of level V nodes is rare in the absence of positive findings in levels I–IV, level IV nodes can still be affected. Thus, it is critical to perform dissections of levels I–IV during elective neck procedures.
- Postoperative Radiotherapy. Postoperative radiation therapy (PORT) is advised for patients with positive margins, multiple cervical node involvement, extracapsular spread in the neck, advanced-stage tumours, perineural spread, or tumours characterized by thickness greater than 9–10 mm.
Carcinoma of Hard Palate
Hard palate carcinoma is rare, comprising only 1% to 3% of oral cancers. Risk factors include tobacco and alcohol use, with a unique link to reverse smoking—a practice particularly common among women in certain regions of India. The disease affects both sexes equally, with most cases occurring in individuals in their sixth or seventh decade of life.
- Anatomy. The hard palate, a part of the maxilla, is located within the maxillary alveolus and merges with the alveolar mucosa. It contains minor salivary glands in its submucosa, with around 33% of palatal tumours originating from these glands. It is innervated by branches of the maxillary division of the trigeminal nerve, and lymphatic drainage primarily occurs via the submandibular lymph nodes.
- Histological types. Tumours may be either squamous cell or glandular in origin, with the latter more common. Glandular tumours arise from minor salivary glands and may include adenoid cystic, mucoepidermoid, or adenocarcinomas.
- Clinical features. Patients often present with pain, ulceration, dental mobility, or ill-fitting dentures. Advanced cases may lead to infraorbital paraesthesia, trismus, or nasal obstruction. Most cases present at stages I or II, though cervical lymphadenopathy is seen in about 8% of patients, with 27% showing occult metastases.
- Investigations. CT and MRI are essential for evaluating tumour extension into the maxillary antrum. Nasal endoscopy is also recommended to assess the extent of the tumour.
Treatment.
- Surgical Management. Smaller tumours are resected along with the underlying bone via a peroral approach, while larger lesions require partial maxillectomy. The surgical defect in the palate, left after excision of the growth, is closed by a suitable prosthesis.
- Neck management. Cervical metastasis is seen in 35% of patients with hard palate or maxillary carcinoma, warranting consideration of elective neck dissection for T2 lesions or larger.
- Postoperative Management. Postoperative radiotherapy is recommended for T3 or greater disease, particularly when positive margins, perineural invasion, or multiple cervical nodes with extracapsular spread are observed.
Carcinoma of Retromolar Trigone
Carcinoma of the retromolar trigone is a rare type of oral cancer, accounting for 6–7% of oral carcinomas. It is more common in older males and may originate at this site or spread from nearby areas like the gingiva, floor of mouth, buccal mucosa, palatine arch, oropharynx, masticator space, involving the medial pterygoid, masseter, temporalis, mandibular branch of the trigeminal nerve. Patients often present with advanced-stage disease (stage III/IV) and symptoms such as pain, trismus, otalgia, and lingual paraesthesia.
Anatomy. The retromolar trigone is a small triangular area located immediately posterior to the last molar tooth on the medial upper surface of the body of the mandible. It covers the anterior surface of the ascending ramus of the mandible. The base of the retromolar trigone lies posterior to the last molar, and its apex is situated adjacent to the tuberosity of the maxilla. This area is bordered by the buccal mucosa on the outside and the anterior tonsillar pillar on the inside. Since the retromolar mucosa is not subjected to the pressures of chewing, it is covered by a lining mucosa with nonkeratinizing stratified squamous epithelium, similar to the tissue found in the buccal mucosa. The buccal branch of the mandibular division of the trigeminal nerve supplies the sensory nerves in this area. Lymph from this region drains into the submandibular and deep cervical lymph nodes on the same side.
Treatment depends on the extent of the disease, with wide surgical excision and block dissection being common. Surgery is typically combined with radiotherapy or chemo-radiotherapy, as radiotherapy alone is associated with higher recurrence rates and lower disease-free survival.
Surgical margins.
The goal of surgical resection in cancer treatment is to achieve complete removal of the tumour, as inadequate clearance can lead to higher local recurrence rates and worse long-term outcomes. During the procedure, continuous reassessment of margins, both visually and by palpation, is crucial. While resection margins of up to 2 cm are advocated for some head and neck cancers, they can cause significant functional and cosmetic deficits. A 1 cm three-dimensional margin is considered acceptable for oral and oropharyngeal tumours. Guidelines suggest margins of over 5 mm as clear, 1–5 mm as close, and less than 1 mm as positive. Larger tumours, perineural spread, and cervical metastasis are linked to a higher likelihood of failing to achieve clear margins. Postoperative radiotherapy (PORT) is recommended for patients with positive or close margins, but even with PORT, recurrence rates remain higher compared to cases where adequate clearance is achieved during surgery.
———— End of the chapter ————
Download full PDF Link:
Carcinoma of the Oral Cavity Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Juvenile Angiofibroma. https://www.entlecture.com/juvenile-angiofibroma/
- Please read. Tumours of Hypopharynx . https://www.entlecture.com/tumours-of-the-hypopharynx/
- Please read. Anatomy of Oesophagus. https://www.entlecture.com/anatomy-of-oesophagus/
Keywords: What are the Risk Factors for Oral Cavity Carcinoma? Signs and Symptoms of Oral Cancer, Comprehensive Guide to Oral Cavity Carcinoma, Treatment Guidelines for Oral Cancer Prognosis of Oral Cancer, How to Diagnose Oral Cancer, Oral Cancer Examination, Risk Factors for Oral Cancer, Oral Cancer Biopsy Procedure, Early Detection of Oral Cavity Cancer, W-plasty, Abbe-Estlander flap or Karapandzic flap, Gillies fan flaps or the Bernard–Webster cheek flap, Perialar crescentic flaps, Burrow-Diffenbach flap, Oral cavity carcinoma, Mouth cancer diagnosis, Oral cancer treatment, Risk factors for oral carcinoma, Symptoms of oral cavity cancer, Stages of oral cancer, Oral squamous cell carcinoma, Early signs of carcinoma in the oral cavity, Best treatments for oral cavity carcinoma, How to prevent mouth cancer naturally, Survival rates for oral squamous cell carcinoma, Oral cancer screening methods and tools, Difference between oral carcinoma and mouth ulcers, Role of HPV in oral cavity carcinoma development, User Intent and Natural Language Focus: What is oral cavity carcinoma and how is it treated?, Can oral cancer be cured completely? , Causes and prevention of oral cancer, How to recognize early symptoms of oral carcinoma? , Advanced therapies for oral squamous cell carcinoma, Tobacco and oral cancer risk, Head and neck cancer overview, Oral cancer awareness campaigns, Surgical options for mouth cancer, Chemotherapy for carcinoma in the oral cavity, Understanding Carcinoma of the Oral Cavity: Symptoms, Treatments, and Prevention, Learn about oral cavity carcinoma, including its causes, early symptoms, treatment options, and how to lower your risk effectively.