|
The following CBME core competencies are covered in this chapter.
|
Chronic Rhinitis
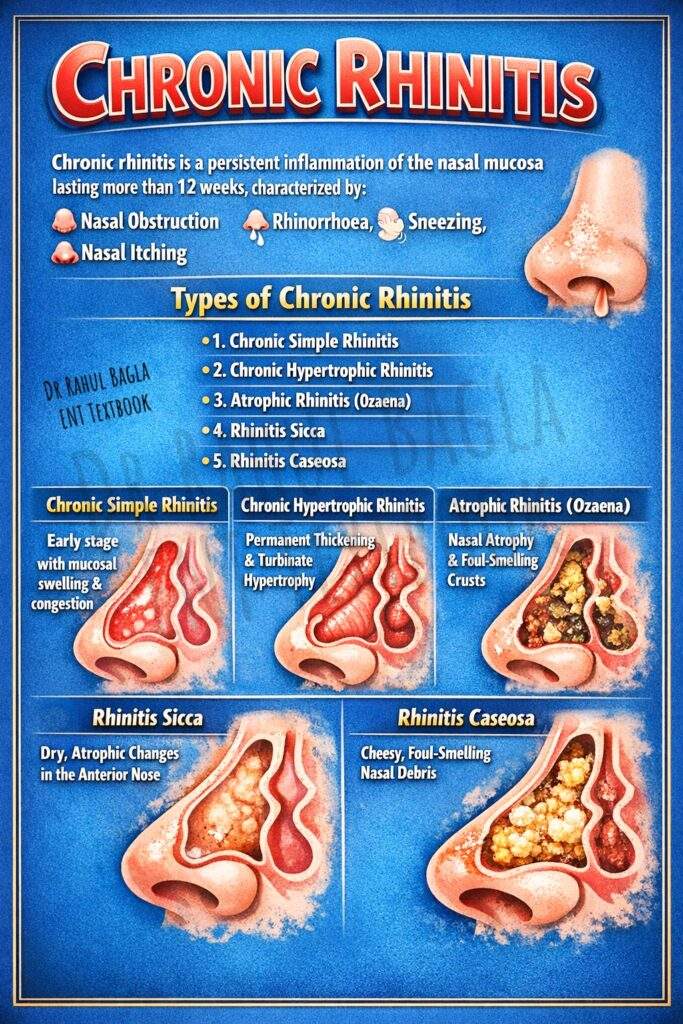
Chronic rhinitis is defined as a persistent inflammation of the nasal mucosa, lasting for more than 12 weeks, characterised by symptoms of nasal obstruction, rhinorrhoea (anterior or posterior), sneezing, and nasal itching. Unlike acute rhinitis, which usually resolves spontaneously, chronic rhinitis progresses slowly and often results from repeated infections, environmental irritation, or structural abnormalities of the nose.
Classification of Chronic Rhinitis
For a conceptual understanding, chronic rhinitis can be broadly classified into specific and non-specific inflammations. This chapter focuses on the latter.
Chronic Non-Specific Rhinitis
- Chronic Simple Rhinitis
- Chronic Hypertrophic Rhinitis
- Chronic Atrophic Rhinitis (Primary & Secondary)
- Rhinitis Sicca
- Rhinitis Caseosa
It is important to remember that these are not always distinct entities but rather represent a progression or spectrum of the same disease process. For instance, simple chronic rhinitis can, over time, progress to hypertrophic rhinitis due to persistent and untreated inflammation.
1. Chronic Simple Rhinitis
Chronic simple rhinitis represents persistent low-grade inflammation of the nasal mucosa, usually resulting from repeated episodes of acute rhinitis. It is considered an early stage in the progression toward chronic hypertrophic rhinitis. It is characterised by vascular engorgement and glandular hyperactivity without permanent tissue thickening.
Aetiology
The condition typically arises from recurrent acute attacks of rhinitis, which fail to resolve completely due to various predisposing factors. These factors can be remembered using the mnemonic NOSE:
- Nasal and Paranasal Factors: Persistent infection due to chronic sinusitis, adenoiditis, or tonsillitis.
- Obstructive Factors: Mechanical obstruction, such as a deviated nasal septum (DNS), synechiae (adhesions), or foreign bodies, which lead to stasis of secretions.
- Systemic and Environmental Factors: Endocrine or metabolic disorders (e.g., hypothyroidism, , excessive intake of carbohydrates and lack of exercise), and chronic irritation from dust, smoke, or cigarette smoking.
- External Irritants: Occupational hazards, snuff, and sudden changes in temperature and humidity.
Pathology
In chronic simple rhinitis, the nasal mucosa shows persistent vascular congestion and mild hypertrophic changes. The pathology reveals:
- Vasodilatation: The blood sinusoids, particularly over the turbinates, are distended.
- Glandular Hyperplasia: There is an increase in the number and activity of seromucinous glands and goblet cells, leading to hypersecretion.
- Oedema: The submucosa shows inflammatory oedema.
Crucially, all these changes are reversible if the causative factors are identified and treated early. The mucosa pits on pressure because the underlying stroma is oedematous and not fibrosed.
Clinical Features
- Nasal Obstruction: This is the hallmark symptom. Obstruction often worsens during sleep because venous congestion increases in the dependent nasal cavity. As a result, patients frequently report alternating nasal blockage.
- Nasal Discharge: The discharge is mucoid or mucopurulent, thick, and viscid. It often trickles down the throat as a postnasal drip, leading to a constant desire to clear the throat.
- Headache: A dull, non-localised headache can occur due to swollen turbinates impinging on the nasal septum.
- Examination Findings (Anterior Rhinoscopy) :
- Nasal Mucosa: Dull red or pink in colour, not pale as in allergy.
- Inferior Turbinate: Swollen, but soft and boggy. It pits on pressure with a probe and shrinks dramatically after application of a vasoconstrictor (e.g., 0.1% xylometazoline). This diagnostic feature differentiates it from hypertrophic rhinitis. The middle turbinate may also be swollen and impinge on the septum.
Management
The cornerstone of treatment is reversing the pathology and eliminating causative factors.
1. Treat the Cause: Address underlying factors like sinusitis (with antibiotics), adenoids (surgery), DNS (septoplasty), and allergy. Advise the patient to stop smoking and avoid dusty environments.
2. Medical Therapy:
- Nasal Decongestants: Topical decongestants (e.g., xylometazoline) can provide short-term relief for severe blockage. However, they must not be used for more than 10 days to avoid rhinitis medicamentosa, a condition of rebound congestion.
- Nasal Steroids: Intranasal corticosteroid sprays (e.g., fluticasone, mometasone) are the mainstay of treatment. They reduce inflammation and oedema without the risk of rebound congestion.
- Nasal Saline Irrigations: Alkaline nasal douching helps clear thick, viscid secretions and improves mucociliary clearance.
- Systemic Antibiotics: A short course may be necessary to treat secondary bacterial infection or concurrent sinusitis.
2. Chronic Hypertrophic Rhinitis
This represents the next stage, where persistent, untreated inflammation leads to permanent structural changes due to fibrosis and bony hypertrophy. The changes are more marked on the turbinates.
Aetiology
The causes are largely the same as those of chronic simple rhinitis, but the inflammation is more severe and prolonged. Common causes include recurrent nasal infections, chronic sinusitis, and persistent irritation from smoking or industrial dust. It can also result from long-standing allergic or vasomotor rhinitis.
Pathology
The key pathological shift is from reversible oedema to irreversible fibrosis.
- Mucosa and Submucosa: There is thickening due to fibrosis, cellular infiltration, and hyperplasia of glands.
- Periosteum and Bone: The turbinate bones undergo true hypertrophy.
- Turbinate Changes: The inferior turbinate is most commonly affected. It can be hypertrophied in its entirety or only at specific points: the anterior tip, posterior end (which can block the Eustachian tube), or the inferior border (giving it a mulberry appearance).
Clinical Features
Symptoms:
- Nasal Obstruction: This is the predominant symptom and is typically persistent and bilateral, without the marked alternation seen in simple rhinitis.
- Discharge: The discharge is thick, mucopurulent, and sticky, making it difficult to blow out.
- Other Symptoms: Patients may complain of a sensation of heaviness in the head, dull headache, and transient or persistent hyposmia (reduced smell).
Examination Findings:
- Turbinate Appearance: The turbinates are enlarged and have a firm, nodular feel.
- Probe Test: The mucosa is firm and does not pit on pressure due to underlying fibrosis.
- Response to Vasoconstrictor: There is minimal to no shrinkage after applying a decongestant. This is the single most important clinical sign differentiating it from chronic simple rhinitis.
Treatment
Management aims to relieve nasal obstruction by reducing the size of the turbinates while preserving as much normal mucosa as possible.
1. Conservative Medical Management: A trial of intranasal steroids may be given for early hypertrophic changes, but the response is often poor.
2. Surgical Reduction of Turbinates: Various surgical options exist, and the choice depends on the type and site of hypertrophy.
- For Soft Tissue Hypertrophy:
- Submucosal Diathermy (SMD) : A needle electrode is inserted into the submucosa of the turbinate, delivering heat to cause coagulation and scarring, thereby reducing the soft tissue bulk.
- Cryosurgery: Freezing the turbinate tip to cause necrosis and shrinkage.
- Radiofrequency Ablation (RFA) / Coblation: A modern, minimally invasive technique that uses radiofrequency energy to create controlled submucosal tissue destruction, preserving the mucosal surface.
- Laser Assisted Turbinoplasty: Using a laser (e.g., diode or CO2) to vaporise a strip of the turbinate.
- For Bony Hypertrophy:
- Partial Turbinectomy: Surgical excision of the hypertrophied part (anterior end, inferior border, or posterior end).
- Submucous Resection of Turbinate Bone: This is an excellent procedure that removes the hypertrophied bone but preserves the overlying mucosa, thus maintaining its physiological function. It is the preferred method for bony hypertrophy.
- Surgical Tip: Excessive or total turbinectomy should be strictly avoided as it can lead to empty nose syndrome, a debilitating condition characterised by paradoxical nasal obstruction, crusting, and dryness.
Compensatory Hypertrophic Rhinitis
This is a unique phenomenon seen in cases of marked deviated nasal septum (DNS) . When the septum deviates significantly to one side, the nasal cavity on the other (wider) side becomes roomy. To protect this wider cavity from the ill effects of excessive airflow, drying, and crusting, the inferior and middle turbinates on that side undergo hypertrophy. This is nature’s attempt to narrow the airway and is therefore a physiological response, not a pathological one. Consequently, these hypertrophic changes are not reversible with septoplasty alone and often require concurrent reduction (turbinoplasty) at the time of surgery.
3. Atrophic Rhinitis (Ozaena)
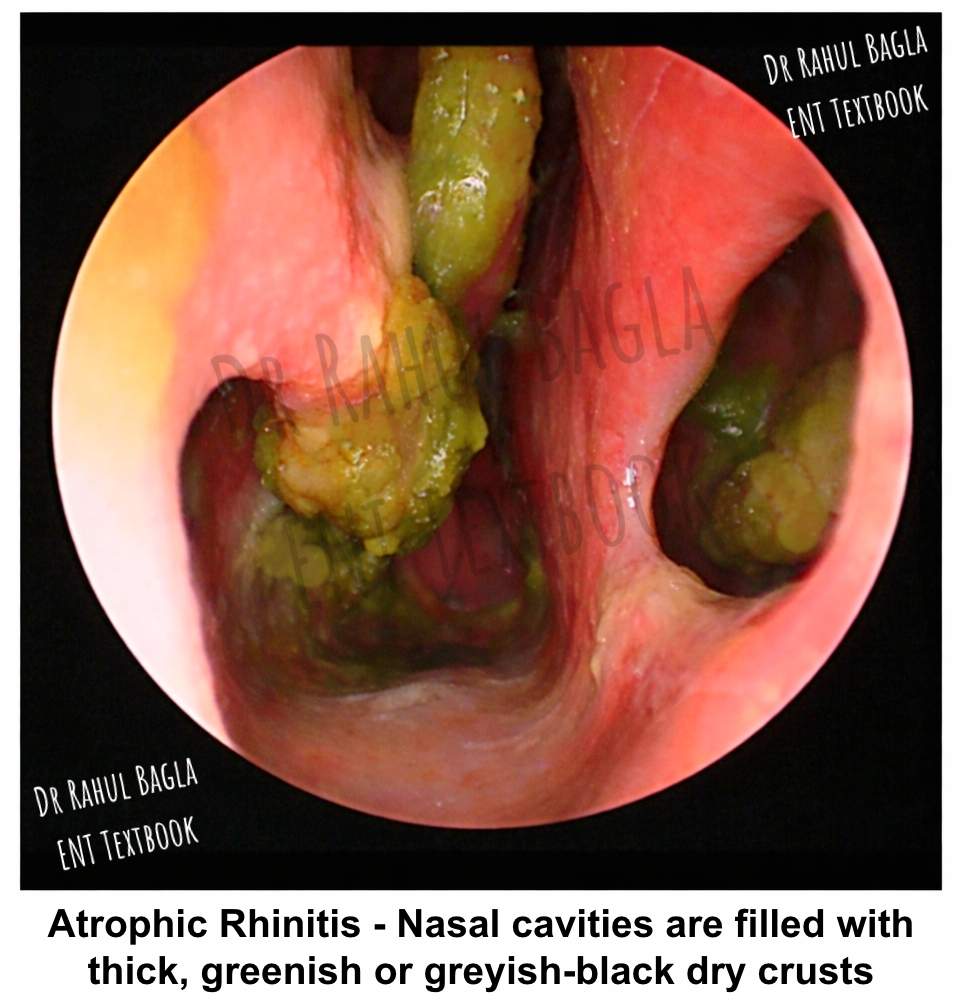
Atrophic rhinitis is a distinct and chronic condition characterised by progressive atrophy of the nasal mucosa, submucosa, and turbinate bones. This results in a roomy nasal cavity that is paradoxically full of foul-smelling crusts. The term Ozaena is used for the classic, fetid form of primary atrophic rhinitis.
Aetiology
Atrophic rhinitis is broadly divided into primary and secondary types.
Primary Atrophic Rhinitis (Unknown aetiology)
The exact cause remains unknown, but several theories exist, remembered by the mnemonic HERNIA:
- Hereditary: Familial tendency has been observed.
- Endocrine: Onset at puberty, female preponderance, and spontaneous remission after menopause suggest a hormonal link.
- Racial: More common in White and Asian races; rare in equatorial Africa.
- Nutritional: Deficiency of iron, vitamins A, D, or E, often associated with low socioeconomic status, may play a role.
- Infective: Various organisms like Klebsiella ozaenae (Perez bacillus), Coccobacillus foetidus ozaena, Proteus, and Diphtheroids are found. However, they are now considered secondary invaders responsible for the foul smell rather than the primary cause.
- Autoimmune: An autoimmune process causing chronic vasculitis and tissue destruction is a strong hypothesis. Evidence of endarteritis and periarteritis in mucosal vessels supports this.
Secondary Atrophic Rhinitis
This form has a clear, identifiable cause, such as:
- Iatrogenic: Excessive and radical surgery of the nose or sinuses (e.g., excessive turbinectomy).
- Granulomatous Diseases: Conditions like Wegener’s granulomatosis (GPA) , tuberculosis, syphilis, leprosy, and scleroma.
- Radiation: Post-radiotherapy for sinonasal malignancies.
- Trauma: Severe facial trauma damaging the nasal mucosa.
Pathology
The histopathological hallmarks include:
- Epithelial Metaplasia: The normal ciliated columnar respiratory epithelium transforms into non-keratinised squamous epithelium.
- Vascular Changes: Obliterative endarteritis and periarteritis of terminal arterioles lead to decreased vascularity and ischaemic atrophy of the mucosa and glands.
- Glandular Atrophy: There is a marked decrease in the number and size of mucus glands.
- Bony Resorption: The turbinate bones undergo progressive resorption, leading to grossly patent nasal cavities.
- Sinus Development: Paranasal sinuses are often small and underdeveloped (micro-sinuses) with thick bony walls.
Clinical Features
- Demographics: Classically affects females, starting around puberty.
- Symptoms:
- Foul Smell (Foetor): The patient emits a characteristic, offensive smell from the nose and mouth. Paradoxically, the patient is unaware of this smell due to severe anosmia caused by atrophy of the olfactory mucosa. This is known as “Merciful Anosmia”. The foul smell makes the patient a social outcast.
- Nasal Obstruction: Despite having wide nasal cavities, the patient complains of obstruction. This is due to the large crusts blocking the airway and the loss of sensory nerve endings, which normally sense the airflow.
- Epistaxis: Minor bleeding occurs when crusts are dislodged.
- Other Symptoms: Atrophic changes can extend to the pharynx (atrophic pharyngitis) and larynx (atrophic laryngitis), causing dryness of the throat and hoarseness of the voice. Conductive deafness can occur due to Eustachian tube blockage by crusts or by extension of the pathology.
- Signs (Anterior Rhinoscopy) :
- Crusting: The nasal cavities are filled with thick, greenish or greyish-black dry crusts. Removing them may cause bleeding.
- Roomy Nasal Cavities: After crust removal, the nasal cavities appear abnormally wide. The turbinates are atrophied to small ridges, allowing a direct view of the posterior wall of the nasopharynx (“patulous nasal cavity”). Septal perforation and dermatitis of the nasal vestibule may be present.
- Mucosa: The nasal mucosa is pale, thin, and glazed.
- External Deformity: A saddle-nose deformity may be present in long-standing cases.
Prognosis
The disease is chronic and tends to persist for years. However, there is a natural tendency for it to burn out and recover spontaneously by middle age, often after menopause.
Treatment
A complete cure is often difficult to achieve, especially in primary cases. Therefore, treatment is primarily palliative and aims to:
- Remove crusts and foul smell.
- Reduce crust formation.
- Atrophy of the mucosa.
The management can be divided into medical and surgical approaches.
Medical Treatment (Palliative)
1. Nasal Irrigation (Douching): The first and most important step. The nose is irrigated with a warm alkaline solution, made by dissolving a teaspoonful of powder containing soda bicarbonate 1 part (28.4 g), sodium biborate 1 part (28.4 g), sodium chloride 2 parts (56.7 g) in 280 mL of clean water. The solution is run through one nostril and comes out from the other. It loosens the crusts and removes thick tenacious discharge. Care should be taken to avoid pushing the fluid into the sinuses and eustachian tube. Initially, irrigations are done two or three times a day, but later, once every 2 or 3 days is sufficient. Hard crusts may be difficult to remove by irrigation. They are first loosened and then mechanically removed with forceps or suction.
2. Nasal Drops to Retain Moisture:
- 25% Glucose in Glycerine: Applied after douching. It acts as a hygroscopic agent, retaining moisture, and the glucose inhibits the growth of proteolytic bacteria (by forming lactic acid), thereby reducing the foul smell.
- Kemicetine Anti-Ozaena Solution: Contains Chloramphenicol (antibiotic), Oestradiol, and Vitamin D. It helps combat infection and improve vascularity.
- Oestradiol in arachis oil can also be used as nasal drops. It helps to increase the vascularity of the nasal mucosa and the regeneration of seromucinous glands.
3. Systemic Therapy:
- Vasodilators: Priscol (Tolazoline) or Nicotinic acid given orally may help improve vascularity.
- Potassium Iodide: Given orally to stimulate nasal secretions.
- Streptomycin: 1g/day for 10 days can be effective against Klebsiella, reducing crusting and odour.
4. Placental Extract: Submucosal injections were used historically to promote regeneration, but this is largely abandoned due to the risk of transmitting infections like HIV.
Surgical Treatment
Surgical options are considered when medical management fails. The principle behind most surgeries is to narrow the excessively patent nasal cavity, thereby reducing crusting caused by the drying effect of rapid airflow.
1. Young’s Operation (Nostril Closure): This involves raising vestibular skin flaps and suturing them together to completely close one or both nostrils. The nasal cavity is closed for 6 months to a year, allowing the mucosa to rest, regenerate, and become healthy. In a Modified Young’s operation, a small 3mm hole is left for breathing and endoscopic examination.
2. Procedures to Narrow the Nasal Cavity:
- Wilson’s Operation: Submucosal injection of Teflon paste into the inferior turbinate and lateral wall to narrow the cavity.
- Lautenslauger’s Operation: This is a major procedure involving osteotomy and medial displacement of the lateral nasal wall.
- Implants: Insertion of cartilage, bone, or synthetic materials (Plastipore) under the mucoperiosteum of the floor and lateral wall.
Unilateral Atrophic Rhinitis
This condition can occur on the wider side of a nose with an extreme deviation of the nasal septum. The excessive unidirectional airflow leads to drying and secondary atrophic changes on that side.
4. Rhinitis Sicca
Rhinitis sicca is considered a milder, localised form of atrophic rhinitis. The atrophic changes are not diffuse but confined to the anterior part of the nasal cavity, particularly the anterior nasal septum.
Aetiology. It is commonly associated with:
- Environmental Factors: Working in hot, dry, and dusty environments (e.g., bakers, mill workers).
- Nutritional Factors: Anaemia and nutritional deficiencies.
Pathology. There is localised metaplasia of the normal ciliated epithelium to stratified squamous epithelium, along with decreased activity of the seromucinous glands in the anterior nasal cavity. The posterior part of the nasal cavity remains normal.
Clinical Features
- Symptoms: The primary symptoms are excessive crusting and epistaxis (nosebleeds) when the crusts are dislodged.
- Signs: Examination reveals dry crusts on the anterior part of the nasal septum. When these crusts fall off, they may expose an underlying ulcer on the septal mucosa. In advanced and neglected cases, this can deepen to form a septal perforation.
Treatment
- Medical: Iron and multivitamin supplements are given to correct any underlying deficiency.
- Local: Nasal douching with saline is highly effective in softening and removing crusts. Lubricating ointments can be applied to the nasal vestibule.
5. Rhinitis Caseosa
Rhinitis caseosa, also known as nasal cholesteatoma (a misnomer), is a rare, chronic inflammatory condition characterised by the accumulation of a foul-smelling, cheesy, yellowish-white material in the nasal cavity and sinuses.
Aetiology and Pathology
The exact cause is unclear, but it is believed to result from suppurative inflammation with obstruction to the outflow of discharge. The obstruction can be due to a foreign body (e.g., rhinolith), a deviated nasal septum, or hypertrophied turbinates. The stagnant discharge becomes infected, leading to granulation tissue formation and accumulation of keratinous debris, cholesterol crystals, and fat. This mass gradually expands, causing pressure erosion of the nasal walls and even bone invasion.
Clinical Features
- Presentation: It is usually unilateral and more common in young adults.
- Symptoms: Patients present with unilateral nasal obstruction, foul-smelling purulent discharge, headache, and sometimes facial swelling.
- Signs: Anterior rhinoscopy reveals the nasal cavity filled with a whitish, cheesy, offensive-smelling debris. The underlying mucosa may show areas of granulation.
Diagnosis and Management
- Diagnosis: It is primarily clinical. A CT scan is essential to rule out sinus involvement, bone erosion, and to differentiate it from malignancy or fungal sinusitis.
- Treatment: The cornerstone of management is complete removal of all caseous material under endoscopic guidance. Once the debris is evacuated, a patent sinus ostium is established for drainage. Underlying causes, like a rhinolith or DNS, should be addressed. The prognosis is excellent with complete clearance.
——– End of the Chapter——–
NEET PG–Style MCQs
Answers
-
B
-
B
-
B
-
B
-
C
-
B
-
B
-
B
-
B
-
A
Frequently Asked Questions in Viva
- What is chronic rhinitis? Chronic rhinitis is persistent inflammation of nasal mucosa lasting more than 12 weeks.
- What causes foul smell in atrophic rhinitis? Secondary bacterial infection and crust decomposition produce the foul odor.
- What is merciful anosmia? Patients cannot smell their own nasal odor due to olfactory mucosal atrophy.
- What is the treatment of hypertrophic rhinitis? Turbinate reduction surgery such as submucosal diathermy or turbinectomy.
- Why is turbinate preservation important? Excessive removal causes dryness and crusting.
——– End——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Chronic rhinitis notes for MBBS, Chronic rhinitis ENT lecture, Atrophic rhinitis pathology, Hypertrophic rhinitis treatment, Rhinitis medicamentosa management, Chronic rhinitis classification CBME, Chronic rhinitis NEET PG questions, Ozaena clinical features, Merciful anosia meaning, Nasal obstruction differential diagnosis, Chronic simple rhinitis vs hypertrophic rhinitis, Types of rhinitis in ENT, ENT PG exam preparation rhinitis, Chronic rhinitis MCQ, Rhinitis surgery indications, Deviated nasal septum complications, Nasal turbinate hypertrophy management, Empty nose syndrome causes, Nasal douching solution composition, Posterior nasal nerve ablation, Chronic rhinitis notes for MBBS students, Chronic rhinitis ENT exam guide, Chronic rhinitis symptoms causes treatment ENT, Types of chronic rhinitis explained for medical students, Hypertrophic rhinitis vs simple rhinitis difference, Atrophic rhinitis ozaena notes for NEET PG, Chronic rhinitis mnemonics ENT revision, Chronic rhinitis MCQs with answers ENT, Chronic rhinitis CBME curriculum ENT notes, Chronic rhinitis viva questions ENT exam, Atrophic rhinitis merciful anosmia explanation, Turbinate hypertrophy ENT exam notes, Rhinitis sicca causes symptoms treatment, Rhinitis caseosa ENT notes summary, Chronic rhinitis clinical features diagnosis treatment ENT.