|
The following CBME core competencies are covered in this chapter.
|
Evaluation of Hearing Impaired Child
Introduction
Evaluation of a hearing-impaired child aims to identify the type, degree, laterality and cause of hearing loss as early as possible to prevent delays in speech, language and cognitive development. Early diagnosis through Universal Newborn Hearing Screening (UNHS), Otoacoustic Emissions (OAE), Brainstem Evoked Response Audiometry (BERA/ABR) and age-appropriate behavioural hearing tests enables timely rehabilitation with hearing aids, cochlear implants and speech-language therapy. This chapter discusses the causes, clinical evaluation, hearing assessment and investigations of childhood hearing loss according to current ENT practice and the requirements of MBBS, ENT PG, NEET PG, INI-CET and FMGE examinations.
The first five years of life represent the critical period for speech and language development. Therefore, early detection and intervention are essential. Children diagnosed and treated before 6 months of age achieve significantly better speech, language and cognitive outcomes than those diagnosed later.
Because nearly 50% of infants with permanent congenital hearing loss have no identifiable risk factors, selective screening alone is insufficient. Therefore, Universal Newborn Hearing Screening (UNHS) is recommended for all newborns, making early screening and continuous surveillance the most effective strategy for detecting childhood hearing loss and initiating timely intervention.
Goals of Evaluation
The objectives of evaluating a child with hearing loss are to:
- Confirm the presence of hearing loss.
- Determine the type, degree and laterality of hearing loss.
- Identify the underlying cause whenever possible.
- Detect associated syndromic abnormalities.
- Assess speech and language development.
- Plan appropriate rehabilitation, including hearing aids, cochlear implantation and speech therapy.
- Initiate early intervention to optimise communication and overall development.
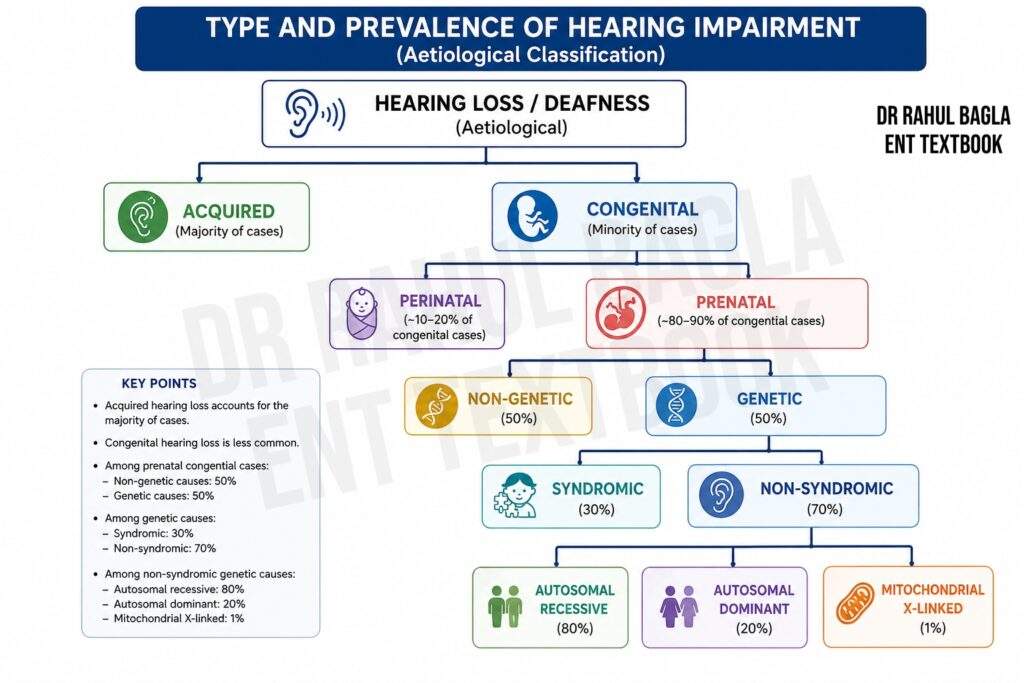
Types and Prevalence of Hearing Impairment
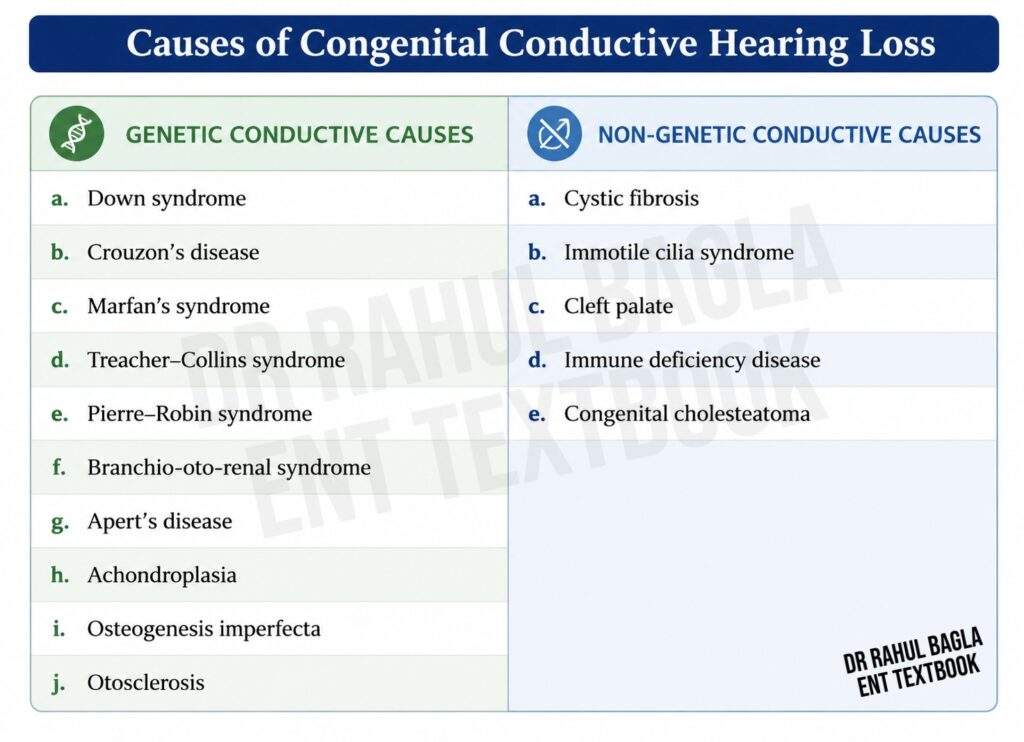
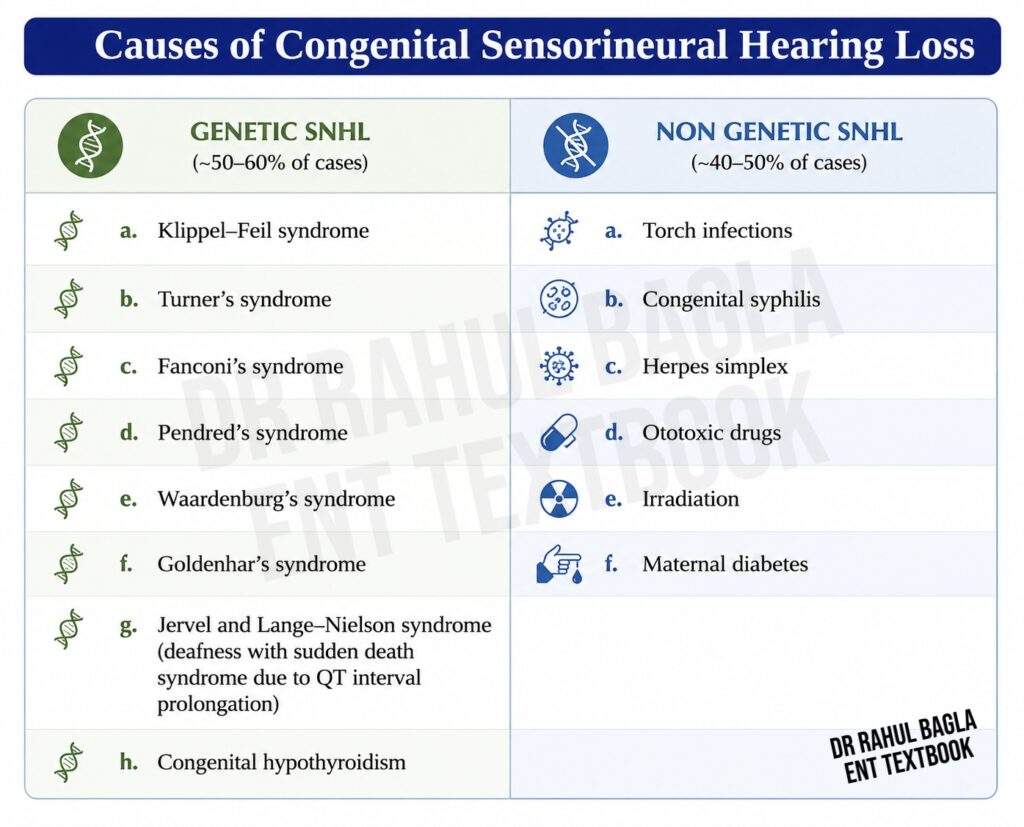
Causes of Congenital Hearing Loss
Definition of Deaf Child
According to the World Health Organisation (WHO), deafness refers to hearing loss severe enough that spoken language cannot be understood through hearing alone, even with amplification.
In clinical practice, children with profound sensorineural hearing loss (>90 dB HL) who fail to develop speech are considered deaf children. The older terms deaf-mute and deaf and dumb are now considered outdated and should be avoided because many deaf children can develop intelligible speech following early diagnosis and appropriate rehabilitation.
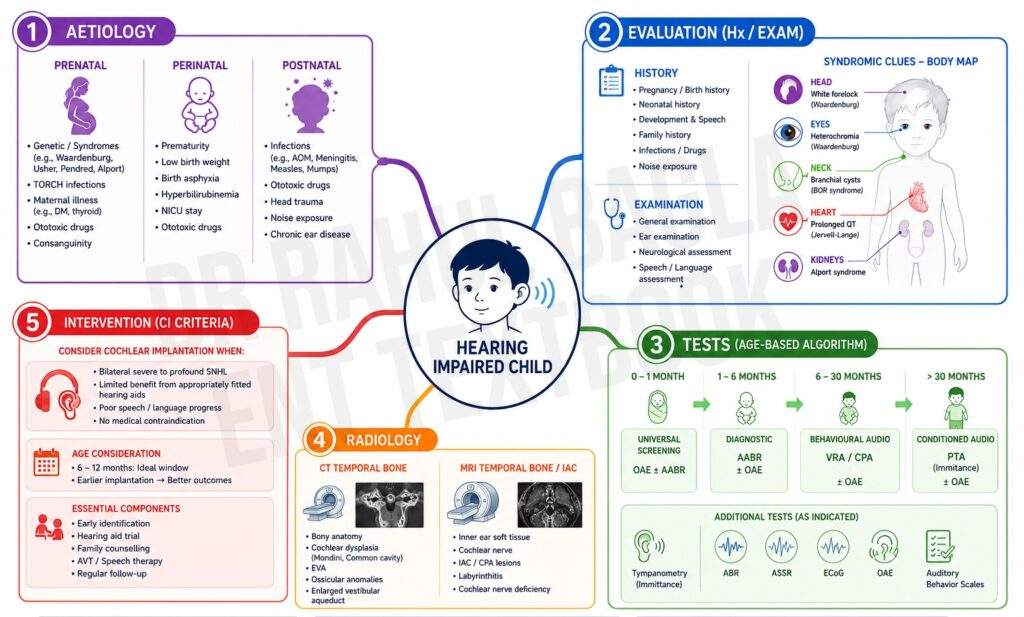
Aetiology
Childhood hearing loss may occur before birth (prenatal), during birth (perinatal) or after birth (postnatal).
Classification of Childhood Hearing Loss According to Time of Onset
- Prenatal (before birth)
- Perinatal (during birth and neonatal period)
- Postnatal (after birth)
A. Prenatal causes
Prenatal causes may be related to genetic abnormalities in the infant or maternal factors affecting the developing fetus during pregnancy.
Genetic abnormalities in the infant
Congenital hearing loss may result from genetic or non-genetic abnormalities affecting the inner ear. The anomalies may involve the bony labyrinth, membranous labyrinth, or both, and may occur as isolated (non-syndromic) abnormalities or as part of a syndrome.
- Both bony + membranous labyrinth affected: Mondini dysplasia, Michel aplasia, Common cavity deformity
- Membranous labyrinth affected: Scheibe dysplasia, Alexander dysplasia, Bing-Siebenmann dysplasia
- Isolated inner ear malformations: Enlarged vestibular aqueduct, Cochlear nerve aplasia, Semicircular canal malformations
Anomalies Affecting Both Bony and Membranous Labyrinths
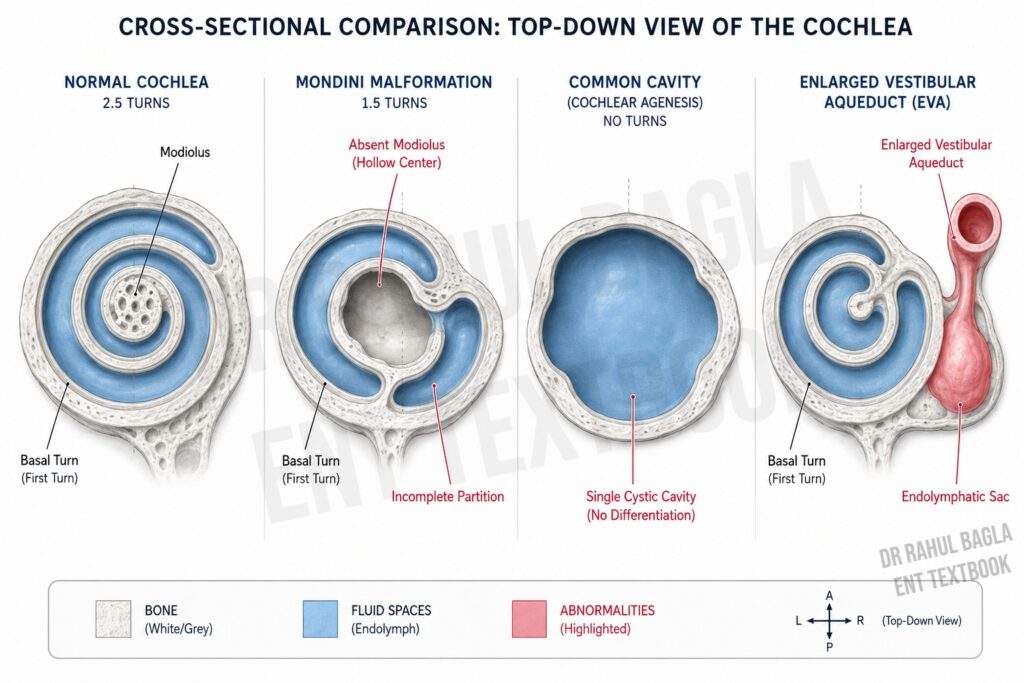
Mondini Dysplasia: Mondini dysplasia is the commonest congenital malformation involving both the bony and membranous labyrinth. It is usually bilateral but may also be unilateral. It may occur in isolation or be associated with syndromes such as Enlarged Vestibular Aqueduct Syndrome, Pendred syndrome, Klippel-Feil syndrome, Waardenburg syndrome and Treacher Collins syndrome.
Characteristic abnormalities include:
-
- Cochlea has only 1½ turns instead of the normal 2½ turns.
- Basal turn is usually the only well-developed turn.
- Absence of osseous spiral lamina leading to incomplete partition of scala vestibuli and scala tympani.
- Partial or complete absence of the modiolus.
Michel Aplasia: Michel aplasia is the most severe congenital inner ear malformation. There is complete absence of both the bony and membranous labyrinth, and the petrous temporal bone may also be underdeveloped. Although the external and middle ears are usually normal, hearing aids and cochlear implantation are ineffective because no functional inner ear is present.
Common Cavity Deformity: The cochlea and vestibule fail to differentiate and form a single common cavity. This malformation causes severe to profound sensorineural hearing loss.
Anomalies Primarily Affecting the Membranous Labyrinth
Scheibe Dysplasia (Cochleosaccular Dysplasia): Scheibe dysplasia is the commonest membranous labyrinth anomaly seen in congenitally deaf children. It is usually inherited as an autosomal recessive non-syndromic disorder. The bony labyrinth and the utricle with semicircular canals remain normal, whereas:
-
- Cochlea and saccule are markedly dysplastic.
- Cochlear nerve and inferior vestibular nerve may be hypoplastic.
- Organ of Corti may be absent.
Alexander Dysplasia: Alexander dysplasia primarily affects the basal turn of the membranous cochlea, producing high-frequency sensorineural hearing loss. As lower frequencies remain preserved, hearing aids often provide useful benefit.
Bing-Siebenmann Dysplasia: This rare anomaly involves complete absence or severe dysplasia of the membranous vestibular labyrinth while the cochlea remains relatively normal.
Specific Isolated Inner Ear Malformations
Enlarged Vestibular Aqueduct (EVA): It is defined as an enlargement of the vestibular aqueduct greater than 1.5 mm, associated with dilatation of the endolymphatic sac. It is best demonstrated on HRCT Temporal Bone, while MRI best demonstrates the dilated endolymphatic sac.
Clinical features include:
-
- Progressive sensorineural hearing loss
- Early childhood onset
- Fluctuating hearing loss
- Episodic vertigo
- Perilymphatic fistula in some cases
Cochlear or Vestibular Nerve Aplasia: Complete absence or hypoplasia of the cochlear or vestibular nerve results in profound hearing loss and may also produce balance disturbances.
Semi-circular Canal Malformations: These commonly involve the superior or lateral semicircular canals and present with vestibular dysfunction, delayed motor milestones and balance impairment.
Maternal Factors
Factors affecting the developing foetus during pregnancy.
- Infections. Toxoplasmosis, rubella, cytomegaloviruses, herpes type 1 and 2 and syphilis. Remember the mnemonic, TORCHES.
- Drugs. Streptomycin, gentamicin, tobramycin, amikacin, thalidomide, quinine or chloroquine.
- Radiation during the first trimester.
- Other factors. Nutritional deficiency, Alcohol intake, diabetes, toxaemia and thyroid deficiency.
B. Perinatal Causes
Perinatal causes occur during birth or the early neonatal period and can significantly impact the auditory system. Key causes include:
- Anoxia causes damage to the cochlear nuclei and may lead to haemorrhage into the inner ear. Common risk factors include placenta previa, prolonged labour and umbilical cord complications (cord around the neck or prolapsed cord), leading to fetal anoxia.
- Prematurity and Low Birth Weight. Babies born before term or with a birth weight less than 1,500 g (3.3 lb) are at a higher risk of auditory damage due to underdeveloped systems.
- Birth Injuries. Birth injuries such as those caused by forceps delivery can lead to intracranial haemorrhage, with blood extravasation into the inner ear, affecting hearing.
- Neonatal Jaundice. Bilirubin levels exceeding 20 mg% can damage the cochlear nuclei, leading to sensorineural hearing loss.
- Neonatal Meningitis and Sepsis. These infections can severely damage the auditory system, leading to hearing loss.
- Time Spent in Neonatal ICU. Prolonged stays in the neonatal intensive care unit (NICU) often expose infants to risk factors like infections, mechanical ventilation, and ototoxic medications.
- Ototoxic Drugs. Drugs used to treat neonatal meningitis or septicemia, such as aminoglycosides, can damage the inner ear, causing irreversible hearing loss.
C. Postnatal Causes
Postnatal causes occur after birth and can be categorised into genetic and non-genetic origins:
- Genetic Causes. Genetic factors contribute to familial progressive sensorineural deafness or syndromes like Alport Syndrome, Klippel-Feil Syndrome, and Hurler Syndrome. Though genetic, these conditions may manifest later in childhood or adulthood.
- Non-Genetic Causes. Postnatal non-genetic causes are similar to those in adults but often have distinct characteristics in children:
- Viral Infections. Infections such as measles, mumps, varicella, and influenza can damage the cochlear structures, leading to hearing loss.
- Meningitis and Encephalitis. These infections can cause inflammation and damage to the auditory nerves or pathways, resulting in hearing loss.
- Secretory Otitis Media. Chronic middle ear infections can lead to conductive or sensorineural hearing loss if untreated.
- Ototoxic Drugs. Medications such as aminoglycosides and chemotherapeutic agents used postnatally can cause auditory damage.
- Trauma, including temporal bone fractures, middle ear surgery, or perilymphatic fistulas, can lead to hearing impairment.
- Noise-Induced Hearing Loss. Exposure to loud sounds during childhood or adolescence can cause permanent damage to the hair cells in the cochlea.
- Neonatal Jaundice and Meningitis. Unresolved neonatal jaundice and meningitis remain significant contributors to sensorineural hearing loss even postnatally.
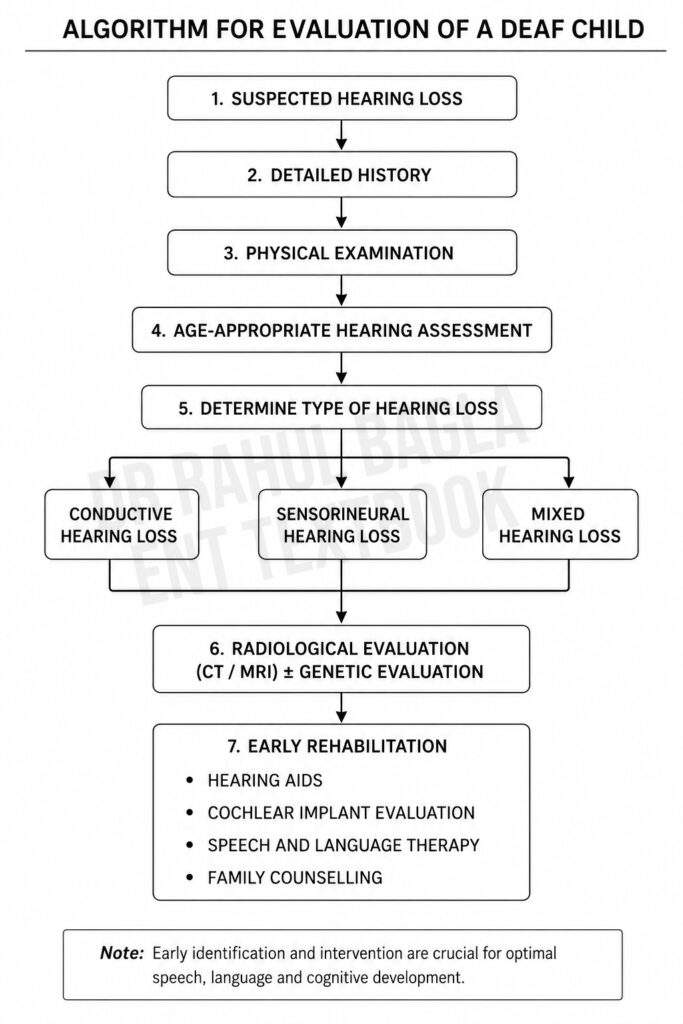
Evaluation of a deaf child
The evaluation consists of:
- Comprehensive history
- Physical examination
- Age-appropriate hearing assessment
- Radiological investigations
- Additional investigations when indicated
1. Comprehensive history taking
A detailed history of the prenatal, perinatal or postnatal period is the foundation for determining the cause of hearing loss.
- Antenatal History: Ask about: i. Maternal infections (TORCHES) ii. Maternal illnesses (diabetes, hypertension or hypothyroidism) iii. Ototoxic drug exposure iv. Radiation exposure v. Alcohol or substance abuse vi. Pregnancy-related complications
- Perinatal History: Ask about: i. Prematurity ii. Birth weight below 1500 g (3.3 lb) iii. Birth asphyxia or delayed crying iv. NICU admission (>48 hours) v. Mechanical ventilation vi. Neonatal jaundice requiring exchange transfusion vii. Neonatal meningitis or septicemia viii. Birth trauma
- Postnatal History: Ask about: i. Delayed speech and language development ii. Developmental milestones iii. Ear discharge or recurrent ear infections iv. Viral illnesses (measles, mumps) v. Meningitis or encephalitis vi. Head injury vii. Noise exposure viii. Ototoxic medications ix. Previous hearing assessment or hearing aid use x. Immunization status
- Family History: Ask about: i. Childhood hearing loss ii. Consanguineous marriage iii. Family members using hearing aids or cochlear implants iv. Syndromic disorders associated with hearing loss
Risk Factors for Permanent Congenital Hearing Loss
Look for: i. NICU stay for more than 48 hours ii. Family history of early childhood deafness iii. Craniofacial anomalies (e.g. cleft palate) iv. Prenatal infections (TORCHES) v. Birth weight below 1500 g (3.3 lb) vi. Exposure to ototoxic medications vii. Bacterial meningitis viii. Hyperbilirubinemia (severe jaundice) ix. Low Apgar score (0–4 at 1 minute or 0–6 at 5 minutes) x. Genetic syndromes associated with hearing loss
Developmental and Functional Assessment
Assessment should also include developmental milestones beyond hearing alone. Delayed speech and language development is often the earliest manifestation of significant hearing loss. Gross motor delay may suggest associated vestibular dysfunction, while poor academic performance or behavioural problems may indicate late-onset or progressive hearing impairment. Vision should also be assessed because dual sensory impairment significantly affects language development and rehabilitation.
Recognition of Hearing Loss
- Infants: Suspect hearing loss if the infant: i. Does not startle to loud sounds ii. Sleeps undisturbed despite loud noise iii. Does not turn towards sound by 6 months iv. Does not babble by 6 months
- Older Children: Suspect hearing loss if the child: i. Has delayed speech and language development ii. Has defective or unclear speech iii. Frequently asks for repetition iv. Increases television volume excessively v. Has poor school performance vi. Appears inattentive or is incorrectly labelled as intellectually disabled
Any child with these features should undergo immediate audiological evaluation.
2. Physical examination
- General Examination: Look for: i. Craniofacial abnormalities ii. Microtia or anotia iii. External auditory canal atresia iv. Cleft palate v. Branchial cysts or sinuses vi. White forelock vii. Heterochromia iridis viii. Facial asymmetry ix. Pigmentary abnormalities suggesting syndromic deafness
- Otological Examination: Perform otoscopy to identify: i. Impacted wax ii. Foreign body iii. Congenital canal stenosis or atresia iv. Tympanic membrane perforation v. Middle ear effusion vi. Cholesteatoma vii. Congenital middle ear anomalies. Many of these causes produce conductive hearing loss, which may be reversible.
- General Systemic Examination: Examine for abnormalities involving: i. Eyes ii. Thyroid gland iii. Heart iv. Kidneys v. Nervous system
3. Age-appropriate hearing assessment
Age-appropriate hearing assessment is performed to determine the type, degree, laterality and site of lesion. The choice of test depends on the child’s developmental age, and combines objective (OAE, ABR, impedance) and behavioural methods. These are described in detail under “Methods of Hearing Assessment in Infants and Children.”
4. Radiological Investigations
Radiological imaging is indicated in children with congenital, profound or unexplained sensorineural hearing loss, particularly when cochlear implantation is being considered.
- Computed Tomography (CT) Temporal Bone: CT scan provides an excellent assessment of the bony labyrinth and is useful for detecting Mondini deformity, Common cavity, Enlarged vestibular aqueduct, Cochlear ossification or Ossicular abnormalities.
- Magnetic Resonance Imaging (MRI): MRI provides superior visualisation of soft tissues and is useful for assessing Cochlear nerve aplasia or hypoplasia, Internal auditory canal, Membranous labyrinth, Brainstem abnormalities or Auditory pathway lesions. MRI is mandatory before cochlear implantation because it confirms the presence of the cochlear nerve and excludes cochlear nerve aplasia.
5. Additional Investigations when indicated
Additional investigations should be performed when syndromic or hereditary hearing loss is suspected. These include:
- Genetic testing (especially GJB2 (Connexin-26) mutation analysis)
- Electrocardiography (Jervell and Lange-Nielsen syndrome)
- Ophthalmological examination (Usher syndrome)
- Renal evaluation (Alport syndrome)
- Thyroid function tests (Pendred syndrome)
- Cytomegalovirus (CMV) testing in selected infants
When to Consider Cochlear Implant Evaluation? Children should be referred for cochlear implant assessment when they have:
- Bilateral severe-to-profound sensorineural hearing loss
- Limited benefit from appropriately fitted hearing aids
- Intact cochlear nerve and suitable cochlear anatomy
- No medical contraindication for surgery
Earlier implantation is associated with superior speech and language outcomes.
Methods of Hearing Assessment in Infants and Children
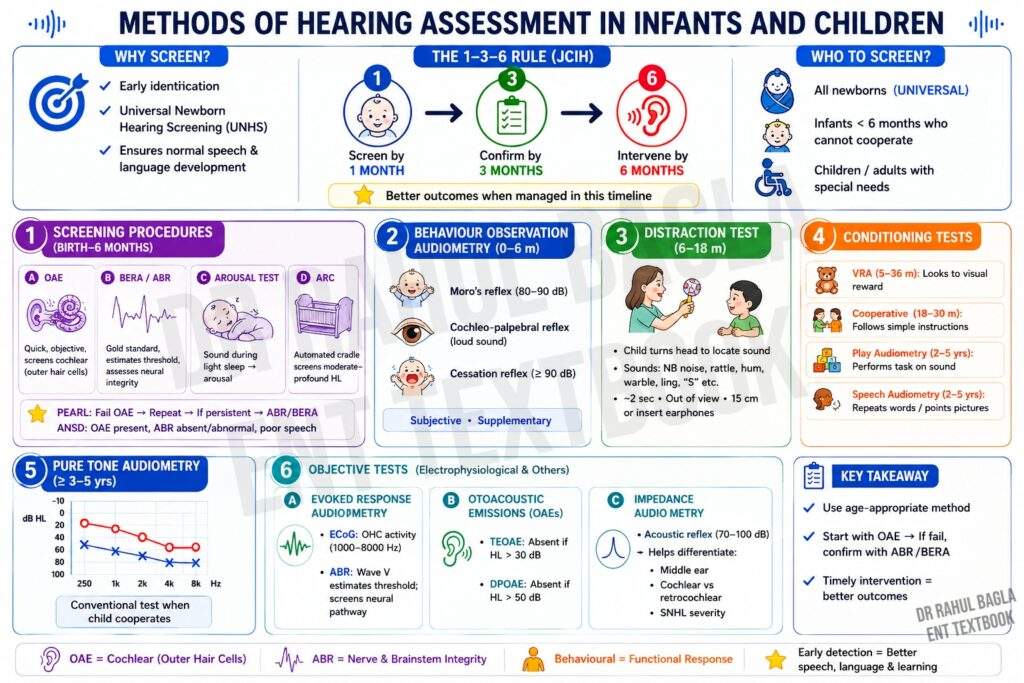
Accurate assessment of hearing in infants and children depends primarily on the child’s developmental age rather than chronological age. As the child grows, behavioural responses become more reliable and progressively replace objective electrophysiological tests. No single hearing test is suitable for all age groups. Therefore, a combination of behavioural and objective tests is often required for accurate diagnosis.
1. Screening Procedures
Key developmental age: Birth–6 months (and older children or adults who cannot cooperate)
Screening tests are used for early identification of hearing loss, particularly in newborns and high-risk infants. Universal Newborn Hearing Screening (UNHS) is recommended for all newborns.
Universal Newborn Hearing Screening (UNHS): The goal of UNHS is early identification and intervention to ensure normal speech and language development.
The 1–3–6 Rule: The 1–3–6 rule is recommended by the Joint Committee on Infant Hearing (JCIH).
- Hearing screening by 1 month
- Confirmation of hearing loss by 3 months
- Appropriate intervention by 6 months
Children managed within this timeline achieve significantly better speech and language outcomes.
OAE and BERA are key electrophysiological objective tests for early identification of hearing loss in infants under 6 months, who cannot cooperate. These tests are also useful for children or adults with special needs who are unable to cooperate. OAE is quick and cost-effective, while BERA provides more accurate results but is more time-consuming. Other methods, like the arousal test and ARC, offer additional screening options.
A. Otoacoustic Emissions (OAE)
OAE is the preferred initial screening test because it is rapid, objective, non-invasive and inexpensive. OAEs are low-intensity sound signals produced by the outer hair cells of the cochlea, which are recorded through a microphone in the external ear canal.
The signals travel in reverse direction from outer hair cells→ basilar membrane → perilymph → oval window → ossicles → tympanic membrane → external ear canal. OAEs detect outer hair cell dysfunction earlier than a pure tone audiogram.
- OAEs are present when: i. Outer hair cells are functioning normally ii. Hearing threshold is generally better than 30 dB HL iii. Auditory neuropathy spectrum disorder (ANSD), where cochlear outer hair cell function is preserved
- OAEs are absent when: i. Outer hair cells are damaged ii. Sensorineural hearing loss exceeds 30 dB HL iii. Middle ear effusion is present iv. External auditory canal is blocked by wax or debris v. Congenital cochlear malformations affecting outer hair cells are present
- Advantages of OAEs: i. Quick (2–5 minutes) ii. No sedation required iii. Ideal for newborn hearing screening iv. Detects cochlear (outer hair cell) dysfunction
- Limitations of OAEs: i. Does not assess the auditory nerve or brainstem ii. Cannot accurately estimate the degree of hearing loss iii. May be absent because of middle ear disease despite normal cochlear function
Clinical Pearl: A child who fails OAE screening should undergo repeat testing and, if persistent, diagnostic ABR/BERA.
To read more about Otoacoustic emissions, click on the link: https://www.entlecture.com/otoacoustic-emissions/
Auditory Neuropathy Spectrum Disorder (ANSD): In auditory neuropathy spectrum disorder, outer hair cell function remains normal, but neural transmission through the auditory nerve is impaired.
Characteristic findings:
- OAE present
- ABR absent or grossly abnormal
- Speech discrimination disproportionately poor
- Hearing thresholds may fluctuate
ANSD is an important cause of hearing impairment in infants admitted to the NICU.
B. Brainstem Evoked Response Audiometry (BERA)
BERA is the gold standard objective test for estimating hearing thresholds in infants who cannot cooperate. It assesses the integrity and function of the central auditory pathway, including the VIIIth nerve, pons, and midbrain. It records electrical potentials generated by the auditory system in response to sound stimuli (clicks or tone bursts), measured via surface electrodes on the scalp. It may require sedation in children. To measure the hearing threshold in an infant, ABR tracing is obtained first at the higher sound stimulus and then gradually lowered till wave V is just identifiable but repeatable. If an infant fails the BERA twice, further assessment is recommended.
- Indications: i. Failed OAE screening on two occasions ii. Infants admitted to NICU iii. Suspected sensorineural hearing loss iv. Auditory neuropathy spectrum disorder (ANSD) v. Suspected retrocochlear pathology vi. Children unable to cooperate for behavioural audiometry
- Interpretation: i. Wave V is the most reliable wave for estimating hearing threshold ii. Hearing threshold is determined by reducing stimulus intensity until Wave V is just identifiable and reproducible iii. Responses around 30–35 dB nHL generally indicate normal hearing iv. Severe or profound hearing loss produces absent or poorly formed waveforms
- Advantages: i. Objective test ii. Estimates hearing threshold iii. Detects retrocochlear pathology iv. Can be performed soon after birth
- Limitations: i. More time-consuming than OAE ii. May require sedation iii. Costlier than OAE
To read more about BERA, click on the link: https://www.entlecture.com/bera/
C. Arousal test
The arousal test is a simple behavioural screening method used in young infants.
Method: The infant is examined during light sleep. A narrow-band high-frequency sound is presented three times, each lasting approximately 2 seconds.
Interpretation: A normally hearing infant becomes aroused at least two out of three presentations.
D. Auditory response cradle (ARC)
ARC is a fully automated screening device for newborns. ARC has largely been replaced by automated OAE and automated ABR in modern newborn hearing screening programmes.
Method: In this test, the infant is placed in a cradle and his behavioural responses (head jerk or turn, body movements, and respiration) in response to sound stimulus (high-pass noise). The responses are monitored by transducers. The transducer is a polyethylene band placed around the infant’s abdomen. ARC is a useful test for screening moderate, severe or profound hearing loss in babies.
2. Behaviour Observation Audiometry (BOA)
(Key developmental age: 0–6 months)
The idea is to check behavioural responses to sound stimuli delivered to an infant. BOA is subjective and has poor test-retest reliability; therefore, it is used mainly as a supplementary behavioural assessment rather than a definitive hearing test. The responses can be alterations in sucking response, alerting, cessation of activity, widening of eyes or facial grimacing. Although BOA is not preferred over electrophysiological tests. But it may be of particular value in infants having auditory neuropathy spectrum disorder when ABR is a poor indicator of functional hearing levels.
- Moro’s reflex is a reflex reaction of infants in response to a sound of 80–90 dB. It is characterised by the sudden extension of arms and legs away from the body and then drawing back. Extension of the head is also present.
- Cochleo-palpebral reflex: There is contraction of the orbicularis muscle, causing blinking of the eye in response to a loud sound.
- Cessation reflex: In response to a sound of 90 dB, an infant stops activity or starts crying.
3. Distraction Test
(Key developmental age: 06-18 months).
The test incorporates the principle that young children at this age turn their head to locate the source of an auditory stimulus.
Method: In this test, the child sits on the parent’s lap or on an infant seat. The child is lightly distracted by an assistant sitting directly in front who holds their attention. While the examiner produces a sound for <2 seconds. Sounds used are calibrated narrow-band noise (500–4000 Hz), high-frequency rattle (8 kHz), low-frequency hum, warble tones or ling sounds, whispered sounds such as “S, S, S”, and xylophone. The sound is delivered from a distance of 15 cm and should be out of the peripheral vision of the child. or delivered via insert earphones. Both the distractor and examiner can observe the response.
4. Conditioning tests
These tests condition the child to perform a learned response whenever a sound is heard.
- Visual reinforcement audiometry (VRA). Key developmental age: 6-36 months. It is a conditioning technique in which a child is trained to look for a visual stimulus in response to a sound stimulus by turning his head. This behaviour is reinforced by a flashing light or an animated toy. It is a commonly used test battery for hearing assessment in preschool children. This test uses standard audiometric methods to determine the hearing threshold. Headphones or earphones deliver the sound.
- The cooperative test. Key developmental age: 18–30 months. It is a valuable alternative test where equipment and facilities are limited. The child is asked to discriminate three different simple instructions, for instance, having been handed a small toy, asked to ‘give it to Mummy’ or ‘give it to Daddy’ or ‘give it to baby’. Starting at a supra-threshold level, the voice is then dropped. A child with normal hearing may discriminate the instruction at 35–40dB(A).
- Play audiometry. Key developmental age: 2–5 years. The test follows the principle that the child is conditioned to wait for a sound signal and then to respond by performing a specific task. Simple tasks which involve a simple repetitive activity, such as placing a toy in a box, putting a ring on a stick or putting balls in a bucket, each time when the child hears a sound signal. Hearing thresholds can be determined by the 10dB down, 5dB-up/ descending-ascending technique as described for pure tone audiometry. Each correct response is reinforced with vocal praise, clapping or a reward.
- Speech audiometry. Key developmental age: 2–5 years. In a quiet room, using live voice, the child is asked to repeat the names of toys or point to pictures placed on a table. The live voice level is gradually lowered. In this way, hearing thresholds and speech discrimination thresholds or scores are recorded. A child with normal hearing is expected to repeat 80% of the names of toys or point to pictures at ≤40dB(A). The ability of a child to discriminate speech signals is an important measure of functional hearing with normal to moderate degrees of hearing loss.
5. Pure tone audiometry
(Key developmental age: ≥3–5 years)
Once the child can cooperate reliably, hearing thresholds can be measured using conventional pure tone audiometry. Young children often undergo PTA using play audiometry techniques before progressing to standard adult testing procedures.
6. Objective tests
A. Evoked Response Audiometry.
- Electrocochleography (ECoG). Electrocochleography (ECoG) is an invasive electrophysiological test that records three distinct potentials from the cochlea and auditory nerve: the cochlear microphonic (generated by outer hair cells), the summating potential (generated by inner hair cells), and the compound action potential (generated by the auditory nerve). It is primarily used in the diagnosis of Meniere’s disease, where an elevated SP/AP ratio (>0.35) is considered diagnostic. Due to its invasiveness (requiring a transtympanic needle electrode), it is not used for routine hearing threshold estimation in infants or children—that role belongs to Auditory Brainstem Response (ABR/BERA). Furthermore, ECoG assesses cochlear (peripheral) function and cannot evaluate retrocochlear pathology; retrocochlear assessment requires ABR or MRI.”
- Auditory Brainstem Response (ABR). ABR evaluates auditory thresholds by analysing identifiable waveforms, especially wave V, which correlates closely with behavioural pure-tone thresholds. In screening, a response to click stimuli at ≤40 dB nHL indicates normal hearing. For diagnostic purposes, thresholds are determined by reducing sound intensity until wave V is just identifiable.
B. Otoacoustic Emissions (OAEs). OAEs measure cochlear function and are commonly used in newborn hearing screenings. Transient Evoked OAEs (TEOAEs): Absent when hearing loss exceeds 30 dB. Distortion Product OAEs (DPOAEs): Absent when hearing loss exceeds 50 dB.
C. Impedance audiometry. It is based on the fact that a loud sound 70–100 dB above the hearing threshold of one ear causes bilateral contraction of the stapedius muscle (which pulls the stapes slightly outward and upward) & and the tensor tympani muscle (pulls the tympanic membrane slightly inward). The effect is more pronounced on the stapedius muscle than on the tensor tympani. The absence of the acoustic reflex indicates middle ear disorder, retrocochlear hearing loss or severe to profound SNHL. It differentiates cochlear and retro-cochlear pathology. In cochlear lesions, the stapedial reflex is present at lower intensities, e.g. 40–60 dB, than the usual 70 dB(recruitment phenomenon). Absence of acoustic reflex but an abnormal tympanogram generally indicates conductive loss. The absence of an acoustic reflex, but a normal tympanometry, with parental concern for hearing loss, suggests the possibility of SNHL of a severe to profound degree. Since ABR and OAEs provide more information, the use of acoustic reflexes in the assessment of paediatric testing is not commonly done.
Summary
Summary
- Early diagnosis is critical: Early identification and intervention prevent speech, language and cognitive delay.
- 1–3–6 rule (JCIH): Hearing screening by 1 month, definitive diagnosis by 3 months, and intervention by 6 months.
- Universal Newborn Hearing Screening (UNHS): Essential because nearly 50% of infants with congenital hearing loss have no identifiable risk factors.
- Otoacoustic Emissions (OAE): First-line, rapid screening test assessing outer hair cell function; typically absent when hearing loss exceeds 30 dB.
- Auditory Brainstem Response (ABR/BERA): Gold-standard objective test for estimating hearing threshold; Wave V is the most reliable waveform.
- Auditory Neuropathy Spectrum Disorder (ANSD): Characterised by present OAE, absent/abnormal ABR, and poor speech discrimination; commonly seen in NICU infants.
- NICU screening: Infants admitted to the NICU should undergo Automated ABR (AABR) rather than OAE alone.
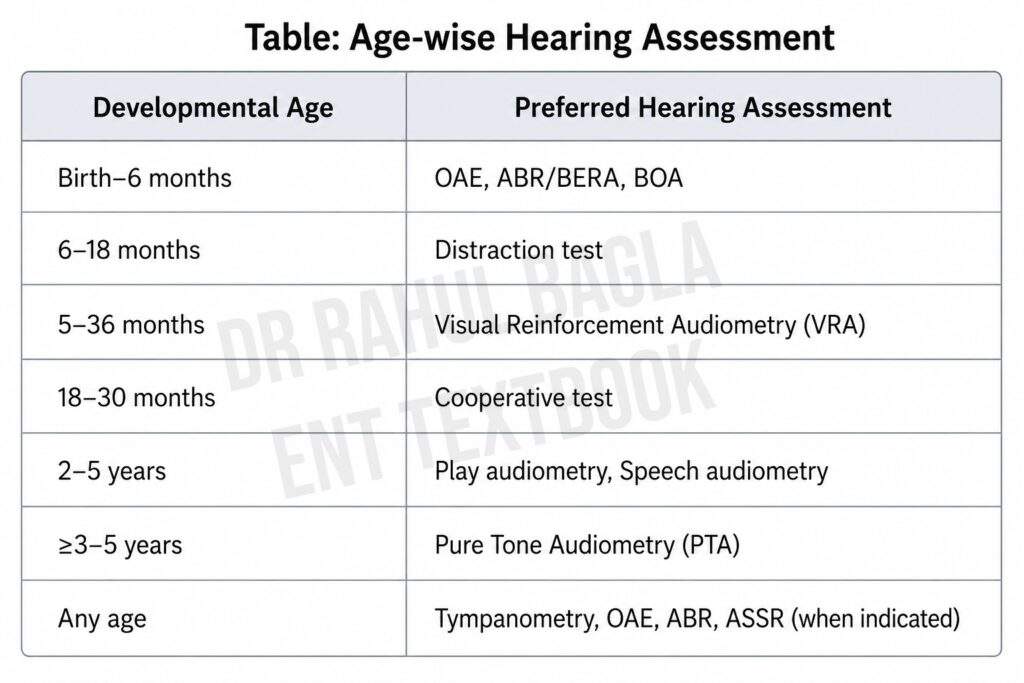
- Age-appropriate hearing assessment:
- 0–6 months: Behavioural Observation Audiometry (BOA)
- 6–18 months: Distraction test / Visual Reinforcement Audiometry (VRA)
- 6 months–2.5 years: VRA / Cooperative audiometry
- 2–5 years: Play audiometry and Speech audiometry
- ≥3–5 years: Pure Tone Audiometry (PTA), depending on the child’s cooperation
- Imaging:
- CT temporal bone: Best for evaluating the bony labyrinth and ossicular abnormalities.
- MRI: Essential before cochlear implantation to assess the cochlear nerve and membranous labyrinth.
- Inner ear malformations:
- Mondini malformation: Most common bony and membranous inner ear anomaly.
- Scheibe (cochleosaccular) dysplasia: Most common membranous inner ear malformation.
——–End of the Chapter———–
High-Yield Revision
- Universal newborn hearing screening is recommended for all newborns.
- Follow the 1–3–6 rule: screen by 1 month, diagnose by 3 months, intervene by 6 months.
- OAE evaluates cochlear outer hair cell function.
- BERA evaluates the auditory nerve and brainstem.
- OAE may be normal in auditory neuropathy spectrum disorder.
- Wave V is used to estimate hearing threshold on ABR.
- MRI is mandatory before cochlear implantation.
- Connexin-26 mutation is the commonest genetic cause of congenital non-syndromic hearing loss.
- Mondini dysplasia is the commonest bony labyrinth malformation.
- Scheibe dysplasia is the commonest membranous labyrinth anomaly.
NEET PG High-Yield MCQs
- Universal Newborn Hearing Screening should ideally be completed by: A. Birth B. 1 month C. 3 months D. 6 months.
- Otoacoustic emissions (OAE) primarily assess the function of: A. Inner hair cells B. Outer hair cells C. Cochlear nerve D. Brainstem.
- In auditory neuropathy spectrum disorder (ANSD), the typical finding is: A. OAE absent, ABR normal B. OAE present, ABR absent C. OAE absent, ABR present D. Both OAE and ABR absent.
- The most reliable wave for estimating hearing threshold in ABR/BERA is: A. Wave I B. Wave III C. Wave V D. Wave VII.
- The commonest congenital malformation involving both the bony and membranous labyrinth is: A. Michel aplasia B. Mondini dysplasia C. Scheibe dysplasia D. Common cavity deformity.
- The commonest membranous labyrinth anomaly in congenital deafness is: A. Alexander dysplasia B. Bing-Siebenmann dysplasia C. Scheibe dysplasia D. Michel aplasia.
- Before cochlear implantation, the most important investigation to confirm the presence of the cochlear nerve is: A. X-ray mastoid B. CT temporal bone C. MRI internal auditory canal D. Tympanometry.
- Which infant is at the highest risk for permanent congenital hearing loss? A. Healthy full-term infant B. Infant admitted to NICU for >48 hours C. Infant with physiological jaundice D. Infant born by elective caesarean section.
- The most appropriate hearing assessment for a cooperative 3-year-old child is: A. BOA B. Play audiometry C. Distraction test D. OAE.
- According to the 1–3–6 rule, intervention for congenital hearing loss should ideally begin by: A. 1 month B. 3 months C. 6 months D. 12 months.
Answers: 1: B. 2: B. 3: B. 4: C. 5: B. 6: C. 7: C. 8: B. 9: B. 10: C.
Clinical Case Scenarios
- Case 1. A 2-day-old newborn fails OAE screening in both ears. Best next step: Repeat OAE, and if persistent, perform diagnostic BERA/ABR.
- Case 2. A 9-month-old infant admitted to NICU after birth has poor response to sound despite normal otoscopy. Most likely diagnosis: Sensorineural hearing loss. Best investigation: BERA/ABR.
- Case 3. A 4-year-old child has delayed speech, repeatedly increases television volume and has bilateral middle ear effusion on otoscopy. Most likely diagnosis: Secretory otitis media causing conductive hearing loss. Best hearing test: Pure tone/play audiometry with tympanometry.
- Case 4. A 3-month-old infant has present OAE but absent ABR with poor speech perception later in infancy. Most likely diagnosis: Auditory Neuropathy Spectrum Disorder (ANSD).
- Case 5. A 1-year-old child with bilateral profound sensorineural hearing loss shows little benefit despite appropriately fitted hearing aids. Best next step: MRI to confirm cochlear nerve followed by cochlear implant evaluation.
Frequently Asked Questions
- What is the best screening test for newborn hearing loss? OAE is the preferred initial screening test because it is rapid, objective and inexpensive.
- What is congenital hearing loss? Congenital hearing loss is hearing impairment present at birth due to genetic abnormalities, intrauterine infections, perinatal complications or developmental anomalies of the auditory system.
- What is Universal Newborn Hearing Screening? Universal Newborn Hearing Screening (UNHS) is a programme in which every newborn undergoes hearing screening using OAE and/or automated ABR before one month of age.
- What is the gold standard hearing test in infants? BERA/ABR is the gold standard objective test for estimating hearing thresholds in infants.
- What is the 1–3–6 rule? Screen by 1 month, diagnose by 3 months and intervene by 6 months.
- Which hearing test evaluates outer hair cells? Otoacoustic emissions.
- Which hearing test evaluates the auditory nerve? BERA
- Which imaging is preferred before cochlear implantation? MRI
- Which congenital anomaly is most severe? Michel aplasia.
- Which anomaly is most common? Scheibe dysplasia.
- Which syndrome is associated with prolonged QT? Jervell and Lange-Nielsen syndrome.
- Why is early diagnosis important? Speech and language development occurs mainly during the first five years of life.
——–End———–
Download full PDF Link:
Evaluation of deaf child Dr Rahul Bagla ENT Textbook
———— End of the chapter ————
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/