Submandibular Gland Surgery
It is a surgical procedure that involves the surgical removal of the submandibular salivary gland.
Click here to: Read Anatomy of the Submandibular Glands

Indications
- Recurrent or chronic sialadenitis not responding to conservative therapy.
- Sialolithiasis (stones) causing obstruction, pain, swelling, and repeated infection.
- Benign tumours (most common: pleomorphic adenoma)
- Malignant tumours (e.g., mucoepidermoid carcinoma, adenoid cystic carcinoma).
- As part of a selective, modified, radical neck dissection to remove lymph nodes in level I of the neck
Contraindications
- Known high-grade malignancy
- Bleeding disorder
- Acute infection of the gland
- Stones confined to the distal portion of Wharton’s duct
Anatomy Relevant to Submandibular Gland Surgery
| Structure | Relations | Key Points for Surgery |
|---|---|---|
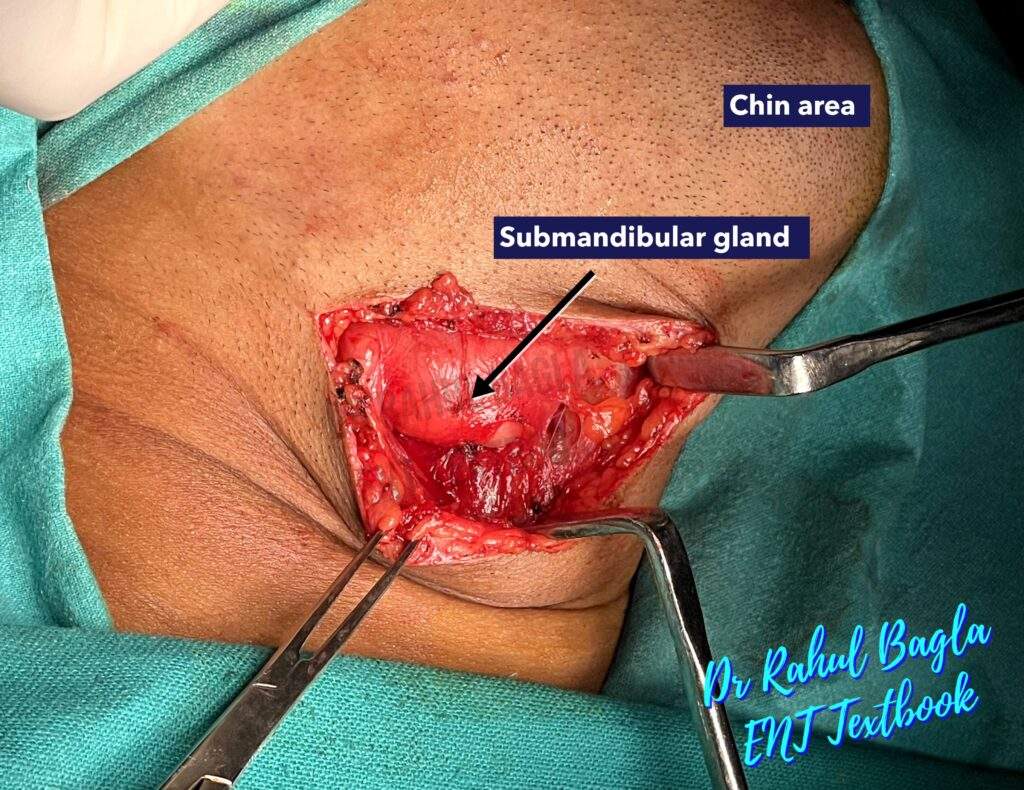
| Submandibular gland | Lies in the submandibular triangle, superficial to mylohyoid muscle, deep to platysma | Divided into superficial & deep lobes separated by mylohyoid muscle; the duct (Wharton’s) runs forward beneath the tongue. |
| Marginal mandibular branch of facial nerve (MMB FN) | Runs below lower border of mandible anterior to angle, loops over facial artery/vein, supplies muscles of lower lip | Risk of injury during skin incision / flap elevation. |
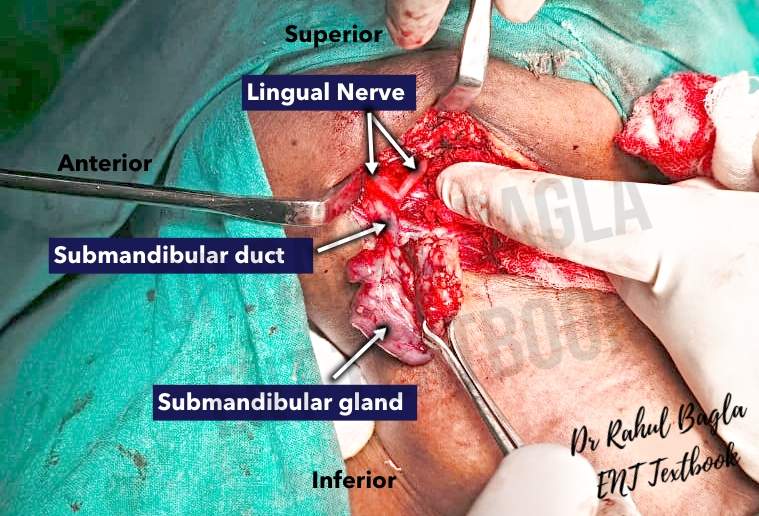
| Lingual nerve | Deep to submandibular duct, passes over hyoglossus, under mucosa of tongue | Must be identified / protected when dissecting duct or submandibular ganglion. |
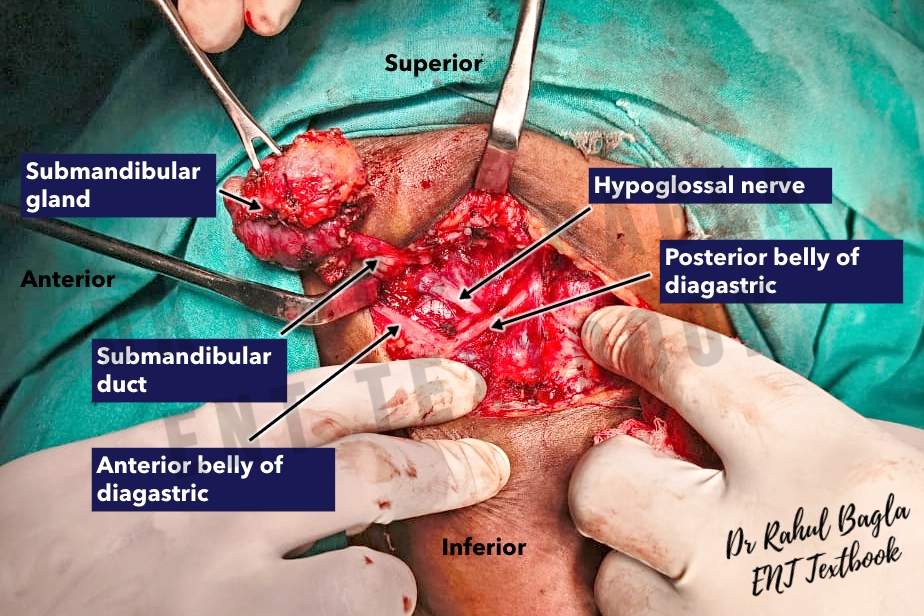
| Hypoglossal nerve (CN XII) | Deep to posterior belly of digastric, over hyoglossus, supplies tongue muscles | Risk during deep dissection, especially inferior & posterior aspects. |
| Submandibular (Chorda tympani / ganglion) | Parasympathetic to gland via ganglion; runs with lingual nerve | Needs careful separation during gland removal. |
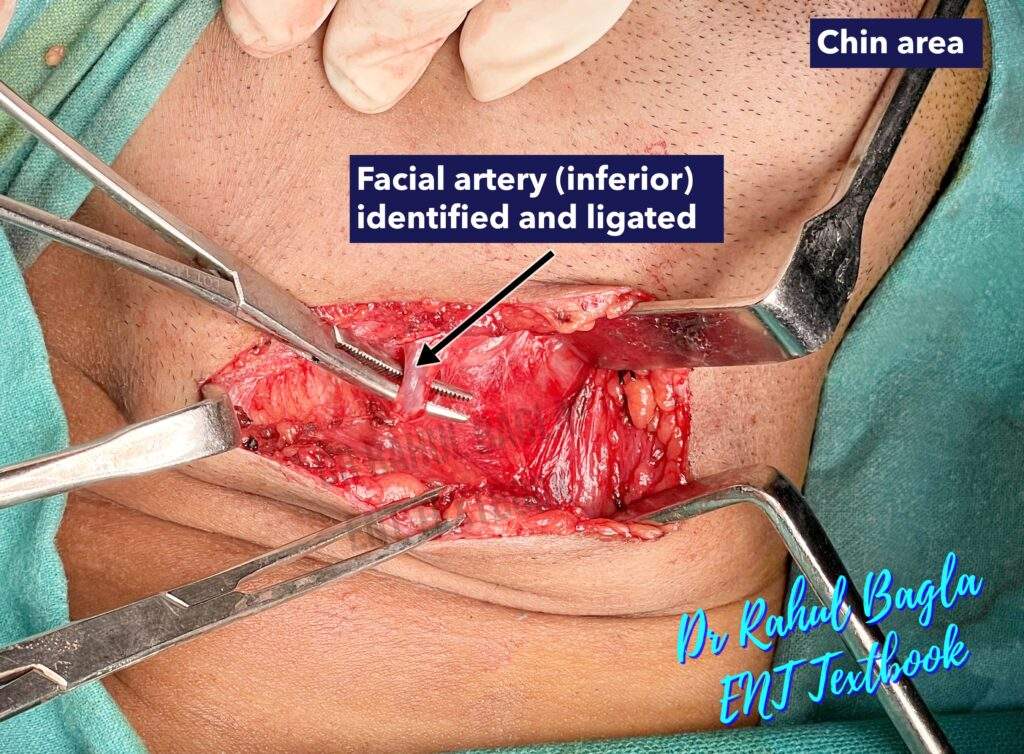
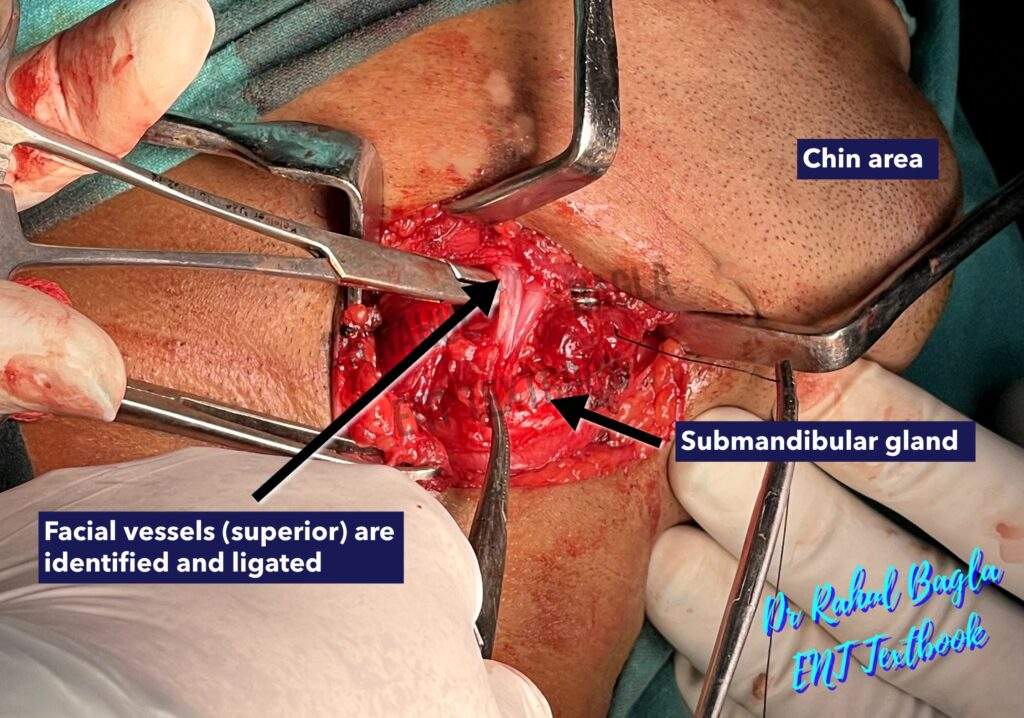
| Facial artery & vein | Facial artery crosses inferior border of mandible just anterior to masseter, enters gland; facial vein is posterior or lateral | Must ligate facial vessels; useful landmarks for MMB FN. |
Steps of submandibular gland surgery
- Patient position & Anaesthesia. The patient lies supine with the face turned away from the operative side, neck slightly extended (shoulder roll). General anaesthesia with oral endotracheal tube.
- Informed consent must specifically mention the risks of marginal mandibular, lingual, and hypoglossal nerve injuries, along with bleeding, infection, and scar formation.
- Skin Incision. A horizontal incision is made at least 2 cm below the inferior border of the mandible, ideally in a natural skin crease. The length of the incision should be 3-4 cm.

- Flap elevation & Protection of the Marginal mandibular branch of the facial nerve. The marginal mandibular branch of the facial nerve enters the neck 1cm in front of the angle of the mandible, loops over the facial artery and vein 2cm below the lower border of the body of the mandible, before sweeping superiorly to the angle of the mouth.
Generally, the submandibular gland is removed without the identification of the marginal mandibular nerve to avoid its injury. For this, a superior subplatysmal flap is not raised as the marginal mandibular branch of the facial nerve runs in the same tissue plane. Elevation of the subplatysmal flap superiorly may cause inadvertent injury to the nerve and cause paresis in the postoperative period. - Identification and Ligation of facial vessels. Dissection is initially directed to the inferior surface of the gland and proceeds cautiously along the capsule from inferior to superior until the facial vessels are ligated and reflected superiorly (subcapsular flap is elevated). The marginal mandibular nerve lies lateral to the facial vessels and can then be lifted out of the operative field by traction.
- Dissection of deep structures. Identify the digastric muscle (posterior belly) as a landmark. Retract posterior belly of digastric; maintain plane over mylohyoid muscle.
- Identification of the hypoglossal nerve. During inferior dissection, keep the dissection along the capsule over the digastric muscles to prevent injury to the hypoglossal nerve, which runs deep to the digastric muscles. The submandibular gland is pulled superiorly to expose the course of the hypoglossal nerve. The nerve runs on the surface of the hyoglossus muscle.

- Identification of the lingual nerve and submandibular ganglion. The posterior border of the mylohyoid muscle is retracted anteriorly, and the submandibular gland is pulled inferiorly, which draws the lingual nerve inferiorly into the field of dissection. The lingual nerve appears as a ribbon-like V-shaped band loosely attached to the body of the gland. The submandibular ganglion is surgically identified as the attachment point of the gland to the lingual nerve. The lingual nerve is then separated from the gland by sharp dissection through the fibres (the parasympathetic secretomotor supply) attached from the submandibular ganglion to the submandibular gland (submandibular duct mainly). This causes the lingual nerve to move upwards automatically and out of the surgical field.

- Identification of the submandibular (Wharton’s) duct for ligation. The posterior border of the mylohyoid muscle is retracted anteriorly, and the submandibular gland is pulled posteriorly to identify the submandibular duct on tension. The submandibular gland duct is covered by the sublingual gland and should be separated before tying it. It is important to palpate the submandibular gland duct to ensure there are no stones in the duct. The duct is then divided and tied off. Then the gland is removed.
- A small vacuum drain is inserted and brought out through the skin posteriorly. The wound is closed in two layers (deep fascia, platysma/skin).
Complications
- Marginal mandibular nerve injury. Occurs temporarily in 10–15% of cases and permanently in 1–3% (PMC). Caused by injury during flap elevation, use of electrocautery, or nerve traction. Leads to lower lip asymmetry, drooling, and cosmetic dissatisfaction.
- Lingual nerve injury. Seen in 1–4% of surgeries (PMC). Occurs during duct dissection or separation of the submandibular ganglion. May result in altered tongue sensation or taste disturbance.
- Hypoglossal nerve injury. Very rare, with less than 2% incidence (PMC). Results from deep dissection near the posterior belly of the digastric or excessive traction. Long-term effects include tongue deviation, speech difficulty, and swallowing issues.
- Retained stone in the distal portion of Wharton’s duct. Seen in 15–20% of sialolithiasis surgeries (PMC). Caused by failure to detect or remove distal duct stones. Leads to recurrent pain, swelling, or infection.
- Bleeding and hematoma
- Infections are rare; antibiotics are only used preoperatively if history of sialadenitis
——– End of the chapter ——–
High-Yield Points for NEET PG and University Exams
- The marginal mandibular nerve lies 1 cm anterior to the angle of the mandible and loops over the facial vessels 2 cm below the mandible.
- Do not raise a superior subplatysmal flap because this injures the marginal mandibular nerve.
- The facial vessels are ligated and reflected superiorly to protect the marginal mandibular nerve.
- The posterior belly of the digastric is the most important landmark for deep dissection.
- The hypoglossal nerve runs on the hyoglossus deep to the digastric; injury causes ipsilateral tongue deviation.
- The lingual nerve appears as a V-shaped ribbon-like band attached to the gland via the submandibular ganglion.
- Divide the ganglion fibres to free the gland while preserving the lingual nerve.
- Wharton’s duct runs forward beneath the tongue and is covered by the sublingual gland.
- Temporary marginal mandibular nerve paresis occurs in 10-15% of cases.
- Retained distal duct stones occur in 15-20% of sialolithiasis surgeries.
NEET PG Style MCQs
- 1: Which nerve is most vulnerable during skin incision and flap elevation in submandibular gland surgery? A. Lingual nerve B. Hypoglossal nerve C. Marginal mandibular nerve D. Facial nerve.
- 2: A patient develops ipsilateral tongue deviation toward the affected side after submandibular sialadenectomy. Which nerve is injured? A. Lingual nerve B. Hypoglossal nerve C. Glossopharyngeal nerve D. Marginal mandibular nerve.
- 3: The posterior belly of which muscle serves as the key surgical landmark during deep dissection? A. Mylohyoid B. Geniohyoid C. Digastric D. Stylohyoid.
- 4: What is the incidence of permanent marginal mandibular nerve injury following submandibular gland surgery? A. 1-3% B. 5-7% C. 10-15% D. 20-25%.
- 5: The submandibular ganglion connects the gland to which nerve? A. Hypoglossal nerve B. Facial nerve C. Glossopharyngeal nerve D. Lingual nerve.
- 6: A 40-year-old woman undergoes submandibular sialadenectomy for chronic sialadenitis. Post-operatively, she complains of altered taste and ipsilateral tongue numbness. Most likely diagnosis: A. Hypoglossal nerve injury B. Lingual nerve injury C. Marginal mandibular nerve injury D. Chorda tympani injury.
- 7: Which structure lies immediately deep to the posterior belly of digastric muscle? A. Lingual nerve B. Facial artery C. Hypoglossal nerve D. Submandibular duct.
- 8: What is the recommended management for a stone located within 1 cm of the Wharton’s duct papilla? A. Submandibular sialadenectomy B. Transoral ductal dilatation and stone removal C. Extracorporeal shockwave lithotripsy D. Observation only.
- 9: Which vessel crosses the inferior border of the mandible just anterior to the masseter and serves as a landmark for the marginal mandibular nerve? A. Facial vein B. External carotid artery C. Facial artery D. Retromandibular vein.
- 10: A patient develops lower lip asymmetry and drooling while drinking water one day after submandibular gland excision. The most appropriate next step is: A. Immediate surgical exploration B. Botulinum toxin injection C. Supportive care and observation D. Corticosteroid therapy.
Answers to MCQs
1: C. 2: B. 3: C. 4: A. 5: D. 6: B. 7: C. 8: B. 9: C. 10: C.
Clinical Case Scenarios for Viva and Practical Exams
Case 1. A 35-year-old woman presents with recurrent painful swelling in the right submandibular region occurring immediately after meals for the past 8 months. On examination, you palpate a hard, mobile swelling in the right submandibular triangle. Bimanual palpation of the floor of the mouth reveals a firm nodule in the anterior part of Wharton’s duct. Most likely diagnosis: Sialolithiasis of the submandibular gland. Best next investigation: Ultrasound of the submandibular region. Best management: If the stone is in the distal duct within 1 cm of the papilla, perform transoral ductal dilatation and stone removal. If the stone is proximal or intra-glandular, proceed with submandibular sialadenectomy.
Case 2. A 55-year-old male smoker presents with a painless, progressively enlarging swelling in the left submandibular region for 2 years. The swelling is firm, mobile, and non-tender. No cervical lymphadenopathy is present. Most likely diagnosis: Pleomorphic adenoma of the submandibular gland. Best next investigation: Contrast-enhanced CT or MRI neck. Best management: Complete submandibular sialadenectomy with capsule preservation and negative margins. What is the risk of recurrence if the capsule is ruptured? Recurrence rate increases from 2-5% to 20-45%.
Case 3. A 60-year-old diabetic patient undergoes elective submandibular sialadenectomy for chronic sialadenitis. On post-operative day 2, she develops progressive neck swelling, difficulty breathing, and a drop in haemoglobin from 12 to 8 g/dL. Most likely diagnosis: Post-operative hematoma with airway compromise. Best immediate management: Emergency bedside evacuation of hematoma followed by return to the operating room for hemostasis. Which vessel is most likely bleeding? The facial artery stump or its branches.
Case 4. A 45-year-old woman complains of persistent right submandibular swelling and pain even after undergoing submandibular sialadenectomy 6 months ago. She reports that the symptoms are identical to her pre-operative symptoms. Most likely diagnosis: Retained stone in the distal Wharton’s duct. Best next investigation: Ultrasound or CT sialography. Best management: Sialendoscopy with stone retrieval or transoral ductal exploration.
Frequently Asked Questions in Viva
- What is the most common complication of submandibular gland surgery? Temporary marginal mandibular nerve paresis occurs in 10-15% of cases, presenting as lower lip asymmetry and drooling during drinking.
- How do you protect the marginal mandibular nerve during surgery? Avoid raising a superior subplatysmal flap, ligate and reflect facial vessels superiorly, and keep the incision at least 2 cm below the mandible.
- What happens if the lingual nerve is injured during submandibular sialadenectomy? The patient experiences ipsilateral tongue numbness, altered taste sensation, and possible difficulty in speech articulation.
- Why does the tongue deviate to the same side after hypoglossal nerve injury? The genioglossus muscle protrudes the tongue forward and toward the opposite side; therefore, loss of ipsilateral genioglossus function causes unopposed action of the contralateral muscle, deviating the tongue toward the injured side.
- Can you remove a submandibular gland without identifying the marginal mandibular nerve? Yes, most surgeons avoid direct identification of the marginal mandibular nerve to prevent injury, relying instead on proper incision placement and avoiding superior flap elevation.
- What is the success rate of submandibular sialadenectomy for chronic sialadenitis? Success rates exceed 90% when surgery is performed for appropriate indications after failed medical therapy.
- How long does temporary marginal mandibular nerve paresis last? Most temporary paresis resolves completely within 3-6 months with supportive care and facial physiotherapy.
——– End——–
Download the full PDF Link:
Submandibular Gland Surgery Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Steps of submandibular gland surgery, Marginal mandibular nerve injury, Lingual nerve injury, Hypoglossal nerve injury, Retained stone in the Wharton’s duct. This chapter provides a clear, exam-friendly guide to submandibular gland surgery: indications, anatomy, operative steps, complications, NEET PG-style MCQs with explanations, clinical scenarios, high yield points, mnemonics, and FAQs. A must-know ENT topic for MBBS, ENT PG theory, viva, and practical exams. What you will learn & why it is important: By the end of this chapter, you will be able to explain when to operate on the submandibular gland, know relevant anatomy, perform or describe the operative steps, anticipate complications, answer NEET PG MCQs, and handle viva and clinical/practical exam questions. This is a complete, standalone resource for submandibular gland surgery. ENT topics for NEET PG MBBS ENT notes submandibular gland surgery, ENT viva questions submandibular gland, NEET PG MCQs salivary gland surgery, CBME ENT curriculum submandibular excision, Submandibular sialadenectomy indications, Complications of submandibular gland surgery Transcervical vs transoral removal, Wharton’s duct, Marginal mandibular nerve injury prevention, Drainless submandibular gland excision safety, Submandibular gland surgery notes, Submandibular sialadenectomy steps, Marginal mandibular nerve injury prevention, Submandibular gland anatomy for NEET PG, Wharton’s duct stone management, Lingual nerve protection during surgery, Hypoglossal nerve injury complications, Submandibular gland surgery indications CBME, Chronic sialadenitis surgical treatment, Submandibular triangle surgical anatomy, Submandibular gland surgery complications pdf, How to remove submandibular gland, Submandibular sialadenectomy viva questions, Submandibular gland surgery MCQs NEET PG, Submandibular gland surgery revision for ENT PG, Submandibular gland surgery clinical cases, Submandibular gland surgery contraindications, Facial artery ligation submandibular gland, Posterior belly digastric landmark surgery, Submandibular ganglion division technique, Retained Wharton’s duct stone management, Submandibular sialadenectomy recovery time, Submandibular gland surgery step by step guide, Submandibular gland surgery learning resources for MBBS, Submandibular gland surgery high yield points..
Good.
Nice
Hello Dr. Hakeem Yousef! 🙏
Thank you so much — it truly means a lot! I’m very happy to hear that you found the chapter helpful. It’s always a pleasure to know that the work is reaching and supporting fellow medical professionals. Please don’t hesitate to reach out if you ever have questions. Wishing you continued success!
Warm regards,
Dr. Rahul Bagla
Dear Dr.
Nicely explained the surgical excision of submandibular gland. One thing I want to say, if I go through intracapsular dissection (in benign disease), it is possible to save the facial vessels. Otherwise, it’s fine. In some videos, I have seen somebody is raising the upper flap upto the margin of mandible, identifying the marginal mandibular nerve & then doing all the dissensions.
Thanks & regards.
Hello Mohammed Sirazul Islam
Yes, some surgeons prefer to elevate the subplatysmal flap up to the inferior margin of the mandible to identify the marginal mandibular nerve before proceeding with dissection. The nerve can typically be located just above and anterior to the posterolateral edge of the mandible (gonion point). Visual identification of the marginal mandibular nerve prior to dissection is advisable, as it helps reduce the risk of injury.
Both approaches are acceptable; however, actively searching for the nerve carries a higher chance of inadvertent trauma. Additionally, excessive or high elevation of the subplatysmal flap can risk injuring the nerve and lead to postoperative paresis. Ultimately, the choice of technique depends on the surgeon’s preference and experience.
Regards
Dr Rahul Bagla