Rhinoplasty and Septorhinoplasty
Introduction
Rhinoplasty and septorhinoplasty are among the most important facial plastic surgery topics for MBBS, ENT PG, INI-CET, FMGE, and NEET PG examinations. These procedures improve both the appearance and function of the nose by correcting nasal deformities, restoring airway patency, and preserving structural support. This chapter covers indications, anatomy, surgical principles, operative steps, grafts, complications, revision surgery, viva questions, MCQs, and high-yield revision points in a simple, exam-oriented format.
Definition
Rhinoplasty is a surgical procedure that reshapes the external nose to improve its appearance, function, or both while preserving structural stability and nasal airway patency. Modern rhinoplasty focuses on preservation and structural reconstruction rather than excessive tissue removal. The aim is to create a natural-looking nose with good airway function and long-term stability. Sushruta first described nasal reconstruction in ancient India, and modern aesthetic rhinoplasty was pioneered by John Orlando Roe in 1887.
Septorhinoplasty is a surgical procedure in which septoplasty and rhinoplasty are performed together in a single operation. It is done in patients who have both nasal obstruction due to septal deviation and external nasal deformity. Correcting only the external shape of the nose does not improve nasal breathing if the septum remains deviated. Similarly, septoplasty alone does not correct external nasal deformity. Therefore, performing both procedures together provides the best functional and cosmetic results. Septoplasty also creates a stable central framework for nasal reconstruction and provides septal cartilage for grafting when required. In patients undergoing purely cosmetic rhinoplasty, septoplasty is performed only if it is needed to correct septal deviation, improve nasal breathing, or obtain cartilage for grafting.
Objectives of Rhinoplasty
The objectives of rhinoplasty are to:
- Improve facial harmony while preserving the patient’s natural appearance.
- Maintain or improve nasal airway function.
- Correct congenital or acquired nasal deformities.
- Restore and preserve the structural support of the nose.
- Achieve stable long-term cosmetic and functional results.
- Meet realistic patient expectations through careful preoperative planning.
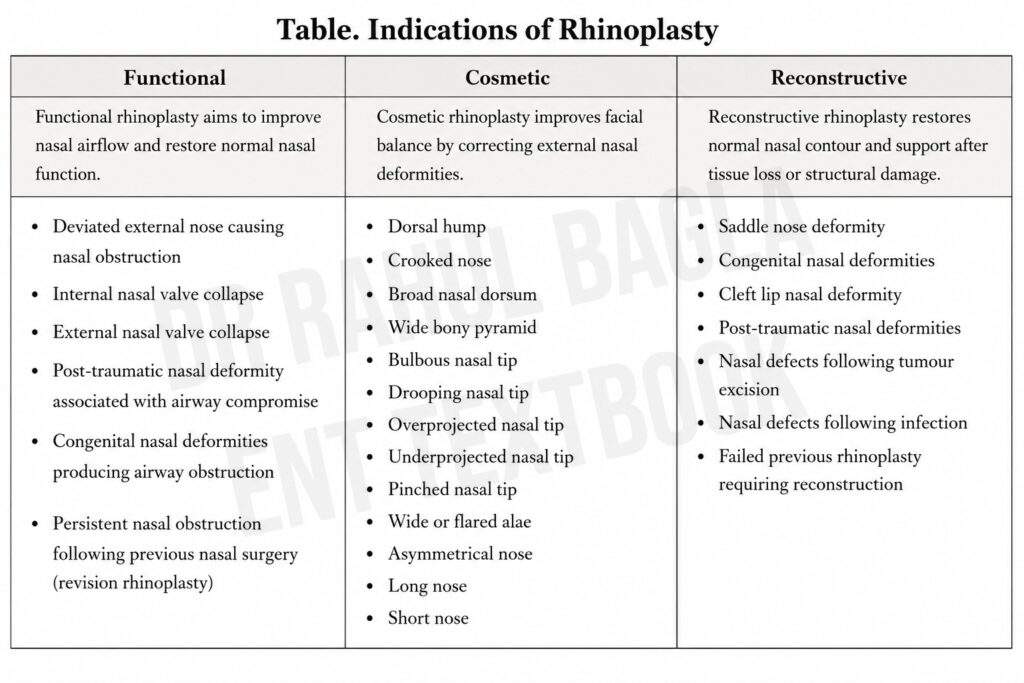
Indications of Rhinoplasty
Rhinoplasty may be performed for functional, cosmetic, reconstructive, or combined indications.
Contraindications of Rhinoplasty
Rhinoplasty should be postponed or avoided in the following situations:
- Unrealistic patient expectations
- Suspected or confirmed body dysmorphic disorder (BDD), as these patients often remain dissatisfied despite excellent surgical results.
- Untreated psychiatric illness
- Active nasal or sinonasal infection
- Poor general medical condition
- Uncontrolled systemic disease
- Incomplete facial growth (except in selected patients with severe functional impairment or post-traumatic deformity)
- Patients who are not willing to comply with postoperative instructions or follow-up
Timing of Rhinoplasty
Rhinoplasty is usually performed after completion of facial growth, generally after 16 years in females and 17-18 years in males. Earlier surgery may be indicated in selected patients with severe congenital deformity, significant post-traumatic deformity, or marked functional airway obstruction.
Applied Surgical Anatomy of Rhinoplasty
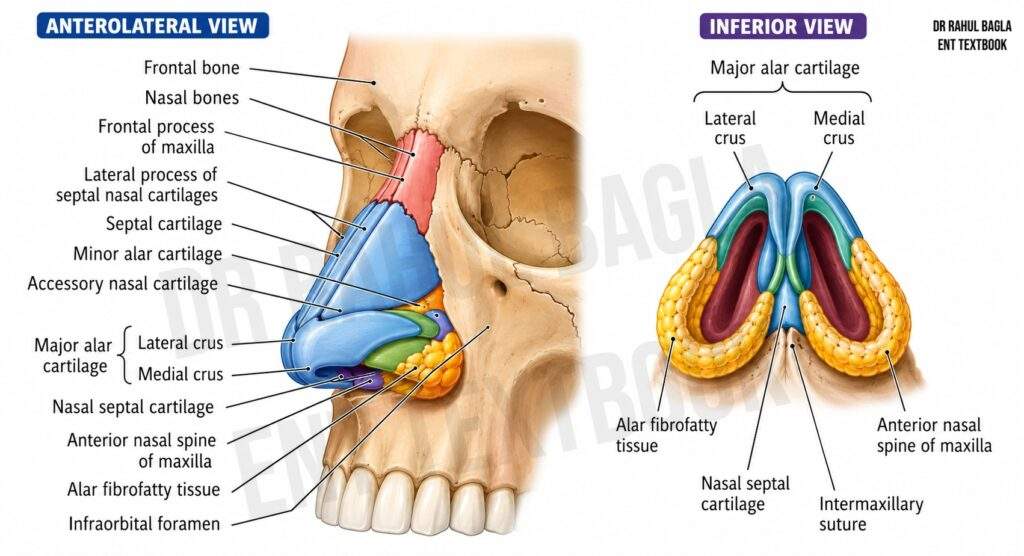
Knowledge of nasal anatomy is essential for safe and successful rhinoplasty. The external nose is divided into three parts:
Upper third (Bony vault)
- Formed by the nasal bones and the frontal process of the maxilla.
- Provides the rigid bony framework.
- Modified during osteotomies and dorsal hump reduction.
Middle third (Middle vault)
- Formed by the upper lateral cartilages and cartilaginous septum.
- Contains the internal nasal valve, the narrowest part of the nasal airway.
- Loss of support may cause internal nasal valve collapse after surgery.
Lower third (Tip complex)
- Formed by the lower lateral (alar) cartilages, which consist of the medial, intermediate, and lateral crura.
- Determines tip projection, rotation, and definition.
- Most tip surgeries involve reshaping or supporting these cartilages.
Septum
- Forms the central support of the nose.
- Deviation of the septum is corrected during septoplasty to improve nasal airflow.
- Provides the preferred source of cartilage grafts for rhinoplasty.
Soft Tissue Envelope
- The skin and superficial soft tissue cover the nasal framework.
- Thin skin shows minor contour irregularities, whereas thick skin masks tip refinement and prolongs postoperative oedema.
Clinical Pearl: The upper third is bone, the middle third is the upper lateral cartilage–septum complex, and the lower third is the lower lateral cartilage (tip complex). Preservation of these structures maintains both nasal shape and airway function.
Aesthetic Subunits of the Nose
The external nose is divided into nine aesthetic subunits, which are important during rhinoplasty and nasal reconstruction because scars placed along subunit borders are less noticeable. The nine subunits are the dorsum, tip, columella, paired sidewalls, paired alae, and paired soft triangles.
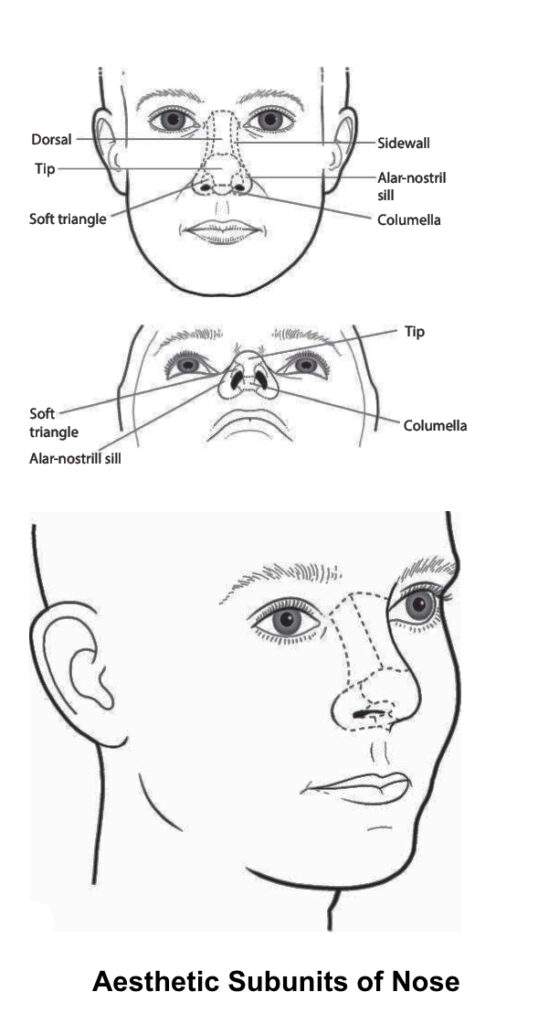
Clinical Importance
- Incisions should, whenever possible, lie along the borders of these subunits to camouflage scars.
- If more than 50% of an aesthetic subunit is lost, reconstructing the entire subunit often provides a better cosmetic result than repairing only the missing portion (Burget and Menick principle).
- Knowledge of aesthetic subunits also helps during the planning of local flaps and reconstruction after tumour excision or trauma.
Clinical Pearl:
Think in aesthetic subunits, not just defects. Replacing an entire subunit often produces a more natural appearance than patch repair.
Preoperative Assessment for Septorhinoplasty
Successful septorhinoplasty depends on careful patient selection, realistic expectations, and meticulous preoperative planning as much as on surgical skill. A detailed preoperative assessment helps the surgeon identify functional and cosmetic problems, choose the appropriate surgical technique, reduce complications, and improve long-term patient satisfaction.
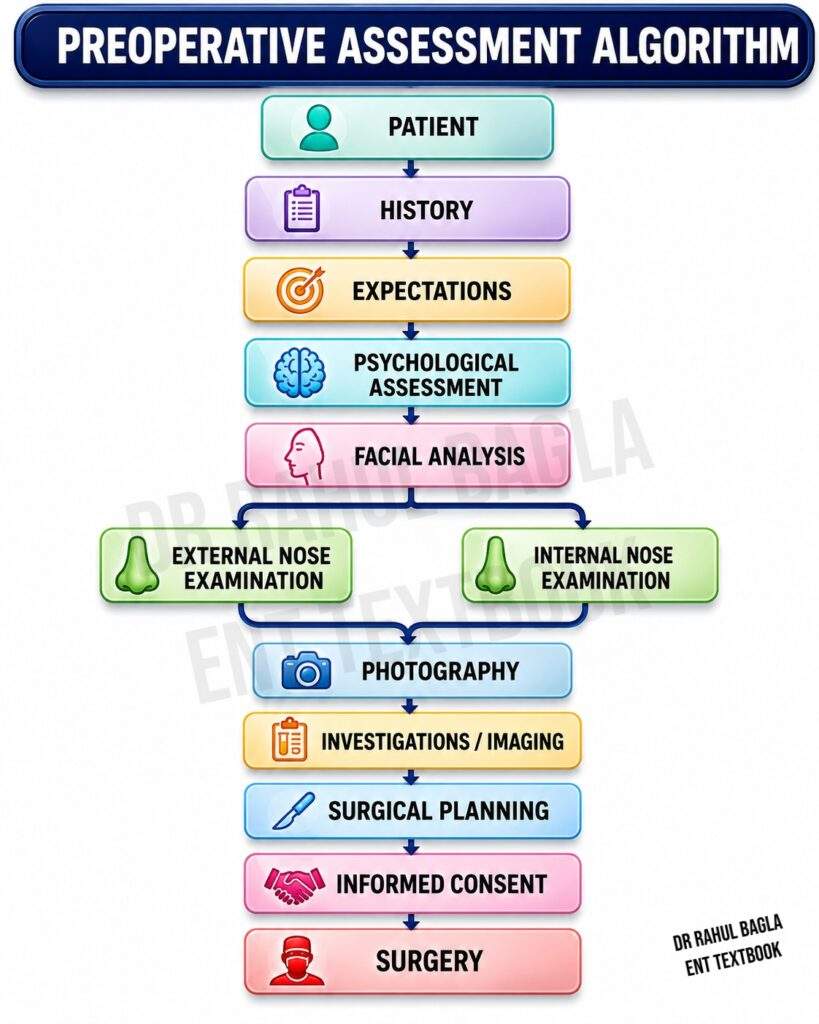
- History: A detailed history should assess both functional and cosmetic concerns. The surgeon should ask about nasal obstruction, mouth breathing, snoring, recurrent sinusitis, epistaxis, and allergic rhinitis. Previous nasal trauma, surgery, infections, or congenital deformities should be documented. The patient’s cosmetic concerns, motivation for surgery, and desired outcome must be explored in depth. Medical conditions such as diabetes, hypertension, bleeding disorders, autoimmune diseases, smoking, cocaine abuse, and the use of anticoagulants or antiplatelet drugs should be reviewed, as these factors may affect healing and surgical planning.
- Assessment of Patient Expectations: Assessing the patient’s expectations carefully is absolutely critical. Rhinoplasty should improve facial harmony and nasal function, not create a “perfect” nose. The surgeon must explain that complete facial symmetry is impossible, postoperative swelling may last several months, and the final cosmetic result usually becomes apparent after 6 to 12 months. Patients should also understand that revision surgery may occasionally be required.
- Psychological Assessment: Psychological assessment is an essential component of preoperative evaluation. Patients with unrealistic expectations or underlying psychiatric conditions are at high risk for dissatisfaction. Body dysmorphic disorder (BDD) is particularly important to identify because these patients often remain dissatisfied despite excellent surgical results.
- Analysis of Face: Evaluate the nose in relation to the entire face. Assess facial symmetry, facial proportions, chin projection, lip position, forehead profile, and skin thickness. The rule of thirds and rule of fifths may be used as guides to assess facial proportions during surgical planning. However, these measurements are only guidelines and should be individualised according to the patient’s facial features, gender, ethnicity, and expectations.
- Physical Examination: Physical examination should be systematic and thorough. The external nose should be examined from multiple views: frontal, right lateral, left lateral, right oblique, left oblique, basal, and superior (bird’s-eye) views. Skin thickness is an important consideration because thin skin reveals minor contour irregularities, whereas thick skin masks tip definition and prolongs postoperative oedema. Nasal length and width, dorsal hump, saddle deformity, deviation, tip projection and rotation, alar symmetry, and nasolabial angle should all be evaluated.
Internal nasal examination should identify septal deviation, turbinate hypertrophy, nasal valve collapse, septal perforation, polyps, chronic rhinosinusitis, and mucosal disease. Nasal endoscopy helps evaluate suspected septal or sinonasal pathology. Functional airway assessment is mandatory because surgery should preserve or improve nasal breathing. Simple bedside tests, such as the Cottle test and modified Cottle test, help identify nasal valve dysfunction. The Cottle manoeuvre is performed by placing a fingertip on the patient’s cheek and applying gentle lateral traction adjacent to the nasal sidewall; improvement in airflow suggests internal nasal valve collapse.
-
Standardised Preoperative Photography: Standardised photographs are an essential part of preoperative assessment. They help to analyse the deformity, plan surgery, counsel the patient, compare preoperative and postoperative results, and provide medicolegal documentation. Standard views include frontal, right lateral, left lateral, right oblique, left oblique, basal, and superior (bird’s-eye) views. Careful review of preoperative photographs may reveal subtle asymmetry or deformities that are overlooked during clinical examination and also provide an objective record of pre-existing abnormalities.
- Preoperative Investigations: Routine investigations depend on the patient’s age, medical condition, and the planned procedure. Common investigations include complete blood count, blood glucose, coagulation profile (when indicated), and viral markers according to institutional protocol.
- Imaging: CT scan of the nose and paranasal sinuses is not routinely required but is useful in patients with facial trauma, chronic rhinosinusitis, revision rhinoplasty, complex deformities, or associated sinonasal disease. Preoperative CT can help detect anatomical variations and pathologies that may impact surgical outcome.
- Surgical Planning: Modern rhinoplasty is individualised. Therefore, every patient requires a written surgical plan based on anatomical findings, functional abnormalities, and cosmetic goals.
- Informed Consent: Informed consent should be obtained after discussing the expected cosmetic and functional outcomes, possible complications, residual asymmetry, prolonged swelling, temporary numbness, need for cartilage grafts, and the possibility of revision surgery.
Types of Rhinoplasty
Rhinoplasty can be classified according to the surgical approach or the surgical objective.
A. According to Surgical Approach
Rhinoplasty can be performed using either an open (external) or closed (endonasal) approach. Both techniques aim to improve nasal appearance and function, but they differ mainly in the method of surgical exposure.
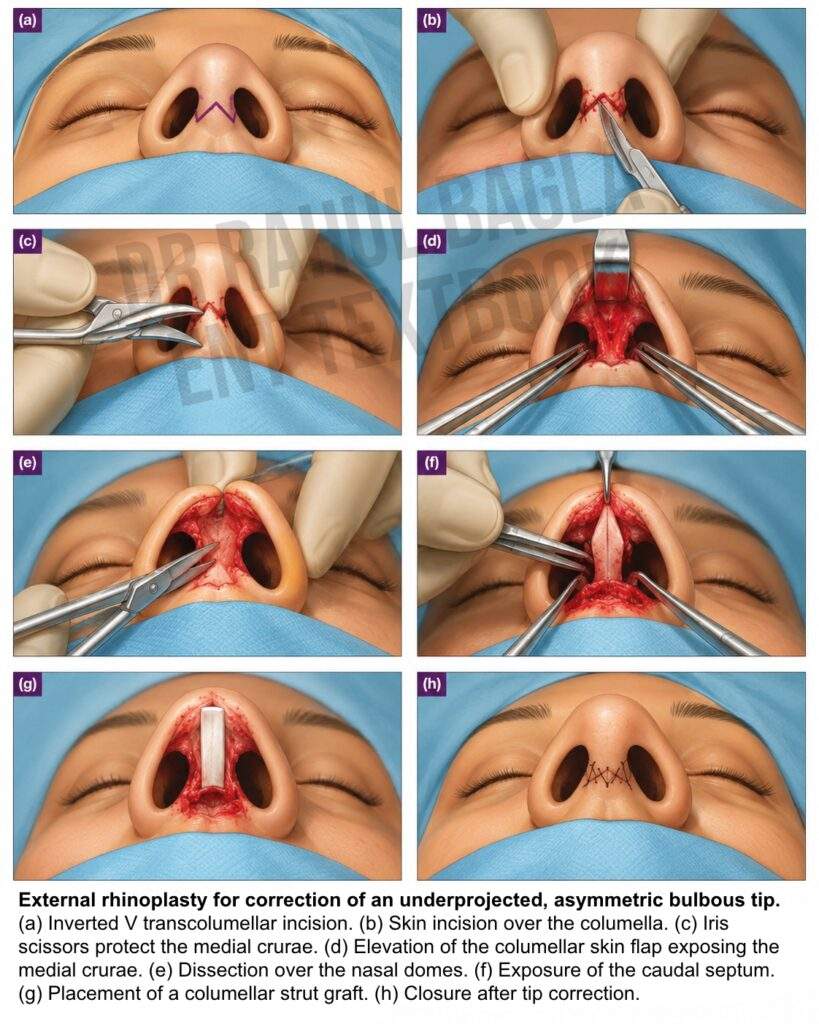
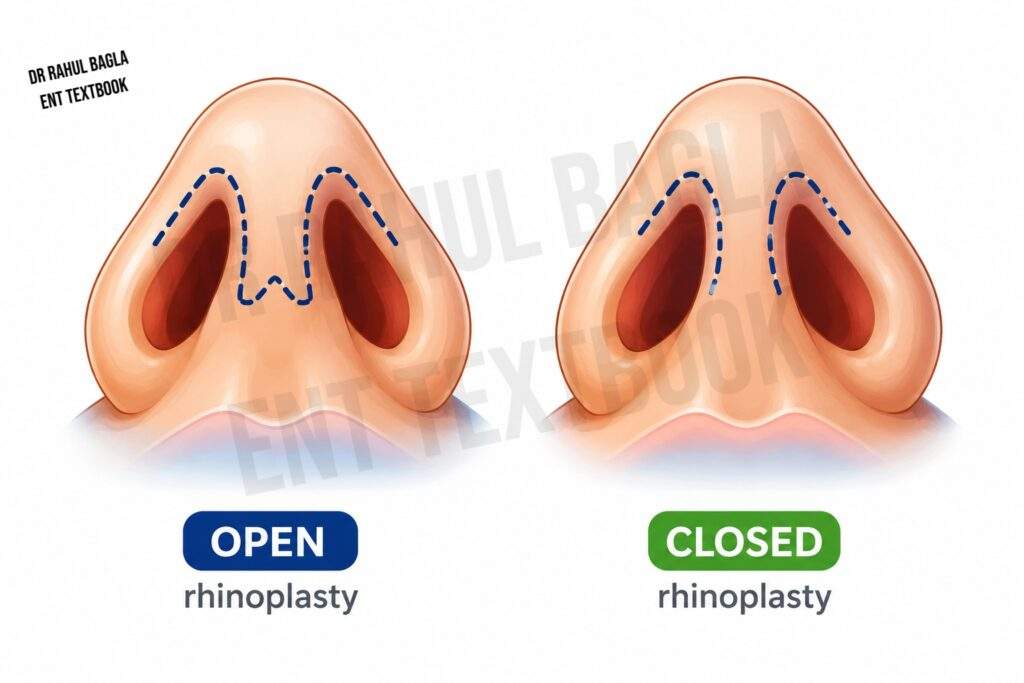
Open (External) Rhinoplasty
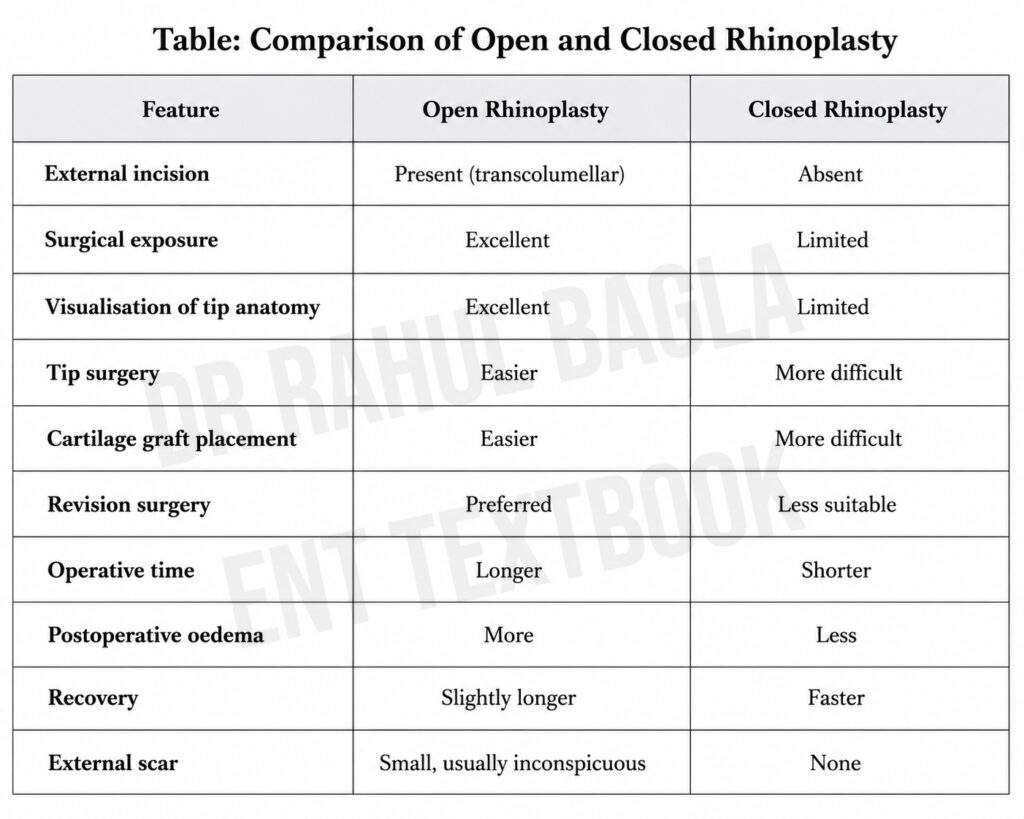
Open rhinoplasty provides direct visualisation of the osteocartilaginous framework through a small external incision. Open rhinoplasty is performed through an inverted V-shaped transcolumellar incision connected to bilateral marginal incisions. Elevation of the skin envelope exposes the lower lateral cartilages, upper lateral cartilages, septum, and nasal bones. This approach provides excellent visualisation of the nasal framework, making cartilage reshaping, graft placement, and tip surgery easier. Therefore, it is preferred for severe deformities, crooked nose, major tip abnormalities, cleft lip nose, congenital deformities, extensive grafting, and revision rhinoplasty. However, it requires a longer operation, causes more postoperative swelling, and leaves a small but usually inconspicuous columellar scar.
Closed (Endonasal) Rhinoplasty
Closed rhinoplasty is performed entirely through intranasal incisions, leaving no visible external scar. It causes less soft tissue dissection, reduced postoperative oedema, shorter operative time, and faster recovery. However, surgical exposure is limited, making cartilage grafting and correction of complex deformities more difficult. It is therefore best suited for simple primary rhinoplasty, minor dorsal hump reduction, mild cosmetic deformities, and selected tip corrections.
Common incisions used in closed rhinoplasty include:
- Intercartilaginous incision: placed between the upper and lower lateral cartilages
- Transcartilaginous incision: placed through the lower lateral cartilage
- Marginal incision: placed along the caudal border of the lower lateral cartilage
- Hemitransfixion incision: placed along the caudal septum
- Complete transfixion incision: placed through the entire caudal septum
Clinical Pearl: The choice of approach does not determine success. Careful planning, preservation of structural support, and meticulous surgical technique are far more important than the incision used.
B. According to Surgical Objective
- Cosmetic rhinoplasty: performed primarily to improve appearance
- Functional rhinoplasty: performed primarily to improve breathing
- Septorhinoplasty: combined functional and cosmetic procedure
- Reduction rhinoplasty: reduces the size of the nose
- Augmentation rhinoplasty: increases the size or projection of the nose
- Reconstructive rhinoplasty: reconstructs the nose after trauma or tumour resection
- Revision rhinoplasty: corrects unsatisfactory results from previous surgery
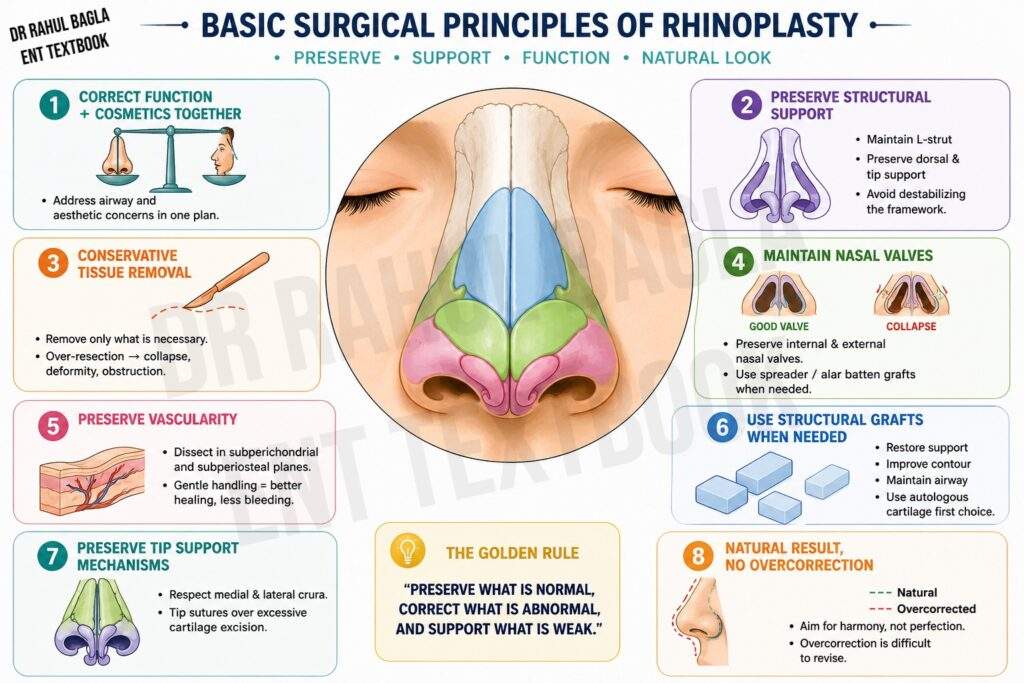
Basic Surgical Principles
Modern rhinoplasty aims to improve both nasal function and facial appearance while preserving normal anatomy. The surgeon should correct functional and cosmetic deformities together, preserve adequate structural support, perform conservative bone and cartilage removal, and maintain the internal and external nasal valves. Preservation of the internal nasal valve is one of the most important principles of modern rhinoplasty. Excessive dorsal reduction or over-resection of the upper lateral cartilages can narrow the valve and produce postoperative nasal obstruction. When required, spreader grafts are inserted between the septum and upper lateral cartilages to restore the valve angle and maintain adequate airflow.
Surgical dissection is usually performed in the subperichondrial and subperiosteal planes to preserve vascularity and reduce bleeding. When necessary, cartilage grafts restore dorsal and tip support while preserving the major tip support mechanisms. The goal is to create a natural-looking nose that complements the patient’s face without compromising breathing. Overcorrection should always be avoided because it is difficult to revise.
Surgical Steps of Septorhinoplasty
Septorhinoplasty follows a planned sequence to improve both nasal function and appearance. Although surgeons may use either an open or closed approach, the basic principles remain the same. Modern surgery emphasises preservation and structural reconstruction instead of excessive tissue removal. The aim is to create a strong, natural-looking nose with a well-functioning airway.
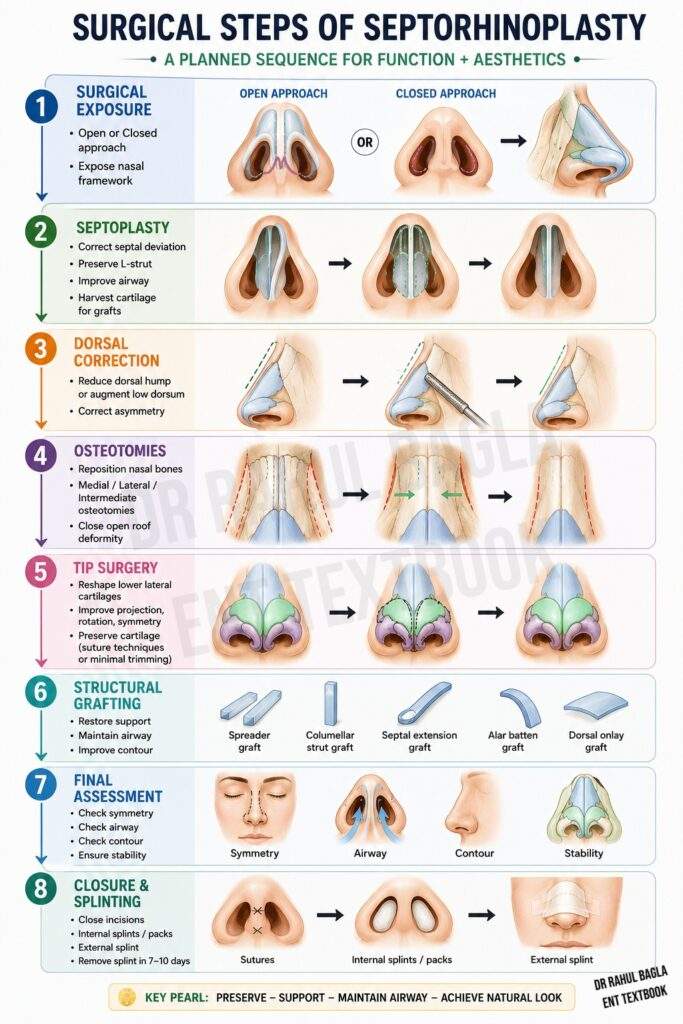
Step 1. Surgical Exposure: The surgeon first exposes the nasal framework through an open or closed approach. The choice depends on the complexity of the deformity, need for grafting, tip reconstruction, revision surgery, and the surgeon’s experience.
Step 2. Septoplasty: Septoplasty is usually the first operative step because it restores the central support of the nose, corrects septal deviation, preserves the L-shaped strut, improves nasal breathing, and provides septal cartilage for grafting when required.
Step 3. Dorsal Correction: The surgeon reshapes the nasal dorsum by reducing a dorsal hump, augmenting a low dorsum, or correcting dorsal asymmetry. After hump removal, an open roof deformity may occur and usually requires osteotomies.
Step 4. Osteotomies: Controlled osteotomies reposition the nasal bones when needed. They are commonly performed for a broad bony nose, crooked nose, post-traumatic deformity, or open roof deformity. Depending on the case, medial, lateral, or intermediate osteotomies may be used.
Step 5. Tip Surgery: The nasal tip is refined by reshaping the lower lateral cartilages. The surgeon corrects tip projection, rotation, and symmetry using cartilage-preserving sutures, limited cartilage trimming, or cartilage grafts. The nasal tip is supported by the two lateral crura and the united medial crura of the lower lateral cartilages (tripod theory). Altering their length or position changes tip projection and rotation. Modern rhinoplasty prefers preservation over aggressive excision.
Step 6. Structural Grafting: Cartilage grafts strengthen the nose, improve contour, and maintain airway patency. They are commonly used for weak tip support, saddle nose, nasal valve collapse, crooked nose, and revision rhinoplasty. Septal cartilage is the preferred graft material, followed by conchal and costal cartilage.
Step 7. Final Assessment: Before closure, the surgeon reassesses nasal symmetry, dorsal contour, tip position, airway patency, and structural stability. Any minor correction is completed at this stage.
Step 8. Closure and Splinting: The incisions are closed with fine sutures. Internal splints or nasal packs may be placed after septoplasty, and an external nasal splint is applied to stabilize the nasal bones. The external splint is usually removed after 7–10 days.
Structural Grafting in Rhinoplasty
Structural grafts restore nasal support, maintain airway patency, improve contour, and reduce the risk of postoperative collapse.
Common Cartilage Grafts
- Spreader graft: placed between the septum and upper lateral cartilage to prevent internal nasal valve collapse.
- Columellar strut graft: placed between the medial crura to support the nasal tip.
- Septal extension graft: extends the septum to control tip projection and rotation
- Tip graft: placed over the tip to improve definition
- Shield graft: placed over the tip to create a more defined appearance
- Alar batten graft: placed in the alar sidewall to prevent external nasal valve collapse
- Dorsal onlay graft: placed over the dorsum to augment height
- Composite graft: A composite graft contains both skin and cartilage, usually harvested from the auricle. It is mainly used for small defects of the alar rim, soft triangle, or columella and provides both structural support and skin cover in a single graft.
Common Sources of Cartilage
- Septal cartilage (preferred): straight, strong, readily available, and harvested through the same operative field
- Conchal cartilage: useful for contour grafts but less rigid
- Costal cartilage: provides abundant material for structural support, especially in revision cases
Synthetic implants such as silicone, expanded polytetrafluoroethylene (ePTFE/Gore-Tex), and porous polyethylene (Medpor) may be used for dorsal augmentation in selected patients. However, they carry a higher risk of infection, extrusion, and foreign body reaction than autologous cartilage grafts.
Correction of Common Nasal Deformities
- Dorsal Hump: A dorsal hump is reduced with a rasp or osteotome. After hump removal, an open roof deformity may occur and usually requires osteotomies to close the gap.
- Pseudohump: An apparent dorsal hump may result from an underprojected nasal tip or low radix rather than true dorsal excess. Treatment focuses on correcting the underlying deformity rather than simply removing the dorsal profile.
- Crooked Nose: A crooked nose requires septoplasty, osteotomies, and realignment of the bony and cartilaginous framework. The septum must be straightened and stabilised in the midline.
- Wide Bony Nose: A wide bony nose is narrowed by controlled medial and lateral osteotomies. These osteotomies allow the nasal bones to be mobilised and repositioned medially.
- Bulbous Tip: A bulbous tip is corrected mainly with cartilage-preserving suture techniques and structural grafts rather than aggressive cartilage excision. Interdomal sutures can narrow the tip, while lateral crural sutures can refine the contour.
- Drooping Tip: A drooping tip requires repositioning of the lower lateral cartilages. Septal extension grafts or columellar strut grafts can increase tip projection and rotation.
- Saddle Nose Deformity: Saddle nose deformity requires augmentation using cartilage grafts, preferably septal cartilage, followed by conchal or costal cartilage if needed. Dorsal onlay grafts restore the dorsal contour.
- Columellar Deformities: Columellar deformities are corrected with a columellar strut or septal extension graft. These grafts provide support and improve the columellar-labial angle.
- Alar Deformities: Alar deformities are managed with alar batten grafts, composite grafts, or alar base reduction, depending on the defect. Alar batten grafts prevent external nasal valve collapse.
- Wide Alar Base: A wide alar base may require alar base reduction (Weir excision) to improve nasal width. Patients should be counselled regarding the presence of small permanent scars hidden within the alar-facial crease.
- Other Tip Deformities: Rhinoplasty may also correct bifid tip, pinched tip, overprojected tip, underprojected tip, and asymmetric tip using cartilage-preserving sutures, grafts, or cartilage repositioning techniques.
Postoperative Care
Proper postoperative care is essential for achieving optimal functional and cosmetic outcomes. Patients should be advised to:
- Keep the head elevated for the first few days.
- Apply cold compresses around the eyes during the first 24-48 hours to reduce swelling.
- The external nasal splint is usually removed after 7–10 days, whereas internal splints or nasal packs, if used, are generally removed within 1–7 days, depending on the procedure and surgeon’s preference.
- Avoid nose blowing for approximately 2 weeks.
- Sneeze with the mouth open whenever possible.
- Avoid strenuous exercise, heavy lifting, and contact sports for 4-6 weeks.
- Protect the nose from accidental trauma.
- Avoid wearing heavy spectacles directly on the nasal bridge until adequate healing has occurred.
- Attend regular follow-up visits for assessment and splint removal.
Patients should also be informed that:
- Swelling and bruising are common during the first 1-2 weeks.
- Tip oedema may persist for several months.
- Temporary numbness of the nasal tip or upper incisors may occur.
- The final cosmetic result usually becomes apparent 6-12 months after surgery.
Complications
Complications may be early or late.
Early Complications
- Bleeding (epistaxis): usually self-limiting but may require packing
- Septal haematoma: requires immediate drainage to prevent necrosis
- Infection (including wound infection): rare but requires appropriate antibiotic therapy.
- Skin flap oedema: common and resolves spontaneously
- Periorbital ecchymosis: common and resolves within 1-2 weeks
- Subdermal haematoma: May develop beneath the external dressing or splint and should be evacuated promptly to minimise cosmetic deformity.
- Airway obstruction: due to oedema or nasal packing
- Septal perforation: rare but can occur with opposing septal tears
Late Functional Complications
- Persistent nasal obstruction: may indicate inadequate correction or scarring
- Internal nasal valve collapse: requires spreader grafts
- External nasal valve collapse: requires alar batten grafts
- Septal perforation: may require surgical repair
- Persistent septal deviation: may require revision septoplasty
Late Cosmetic Complications
- Residual dorsal hump: may require revision reduction
- Saddle nose deformity: requires augmentation grafting
- Polly-beak deformity: supratip fullness caused by inadequate dorsal reduction, loss of tip support, excessive scar tissue, or thick skin. Management depends on the underlying cause and may require revision surgery with cartilage grafting or scar reduction.
- Inverted V deformity: collapse of the upper lateral cartilages
- Crooked nose: persistent deviation
- Tip asymmetry: requires revision tip surgery
- Pinched tip: over-resection of the lower lateral cartilages
- Bossae formation: cartilage irregularities
- Over-rotation or under-rotation of the tip: requires revision
- Excessive or inadequate dorsal reduction: requires revision
- Visible graft irregularities: may require camouflage or removal
- Columellar scar (after open rhinoplasty): usually inconspicuous
A 2024 systematic review reported that severely crushed cartilage has substantially higher complication rates—resorption (3.4%) and revision (17.9%)—compared to non-severely crushed cartilage (0.9% and 3.5%, respectively).
Revision Rhinoplasty
Revision rhinoplasty is performed to correct persistent cosmetic deformity, functional nasal obstruction, or both after previous rhinoplasty. It should generally be planned only after complete healing, usually at least 12 months after the primary surgery, unless early revision is required for major complications. Revision surgery is required in approximately 5–15% of patients after primary rhinoplasty, depending on case complexity, patient expectations, and surgical technique.
Common indications include:
- Persistent nasal deformity
- Pollybeak deformity
- Drooping or over-rotated nasal tip
- Saddle nose deformity
- Residual dorsal hump
- Nasal asymmetry
- Pinched nasal tip
- Internal nasal valve collapse causing nasal obstruction
Revision rhinoplasty is technically more difficult than primary rhinoplasty because of:
- Scar tissue
- Distorted anatomy
- Loss of normal tissue planes
- Deficiency of septal cartilage, often requiring auricular or costal cartilage grafts
Successful revision surgery depends on careful analysis of the underlying deformity, restoration of structural support, and realistic patient expectations.
———End of the Chapter———–
High-Yield Points for Quick Revision
- Septorhinoplasty combines septoplasty and rhinoplasty in a single operation to correct both functional and cosmetic deformities.
- Open rhinoplasty uses a transcolumellar incision and provides excellent exposure; closed rhinoplasty uses intranasal incisions only and leaves no external scar.
- Septal cartilage is the preferred graft material because it is straight, strong, and readily available.
- The L-shaped strut must be preserved during septoplasty to maintain tip support.
- The internal nasal valve is formed by the angle between the septum and the upper lateral cartilage; the external nasal valve is formed by the alar rim.
- The Cottle test helps diagnose internal nasal valve collapse.
- Spreader grafts prevent internal nasal valve collapse; alar batten grafts prevent external nasal valve collapse.
- Polly-beak deformity results from inadequate tip support or excessive supratip fullness.
- Inverted V deformity results from collapse of the upper lateral cartilages after hump reduction.
- Revision rhinoplasty should be delayed for at least 12 months to allow scar maturation.
- Septoplasty is usually the first step in septorhinoplasty because it restores central support and provides graft material.
- Body dysmorphic disorder (BDD) is a contraindication to rhinoplasty.
- Preoperative photographs are mandatory for surgical planning and medicolegal documentation.
- The final cosmetic result becomes apparent 6 to 12 months after surgery.
- Costal cartilage is preferred for structural support when septal cartilage is unavailable.
NEET PG-Style MCQs
- A 28-year-old woman undergoes septorhinoplasty. Fracture of the septal L-strut will most likely result in which of the following complications? A. Bossa formation B. Tip ptosis C. Septal perforation D. Dorsal hump recurrence.
- Which cartilage is the preferred graft material in rhinoplasty? A. Conchal cartilage B. Septal cartilage C. Costal cartilage D. Auricular cartilage.
- The Cottle manoeuvre is used to assess which of the following? A. Septal deviation B. Turbinate hypertrophy C. Internal nasal valve collapse D. External nasal valve collapse.
- Which of the following is a contraindication to rhinoplasty? A. Mild dorsal hump B. Body dysmorphic disorder C. Nasal airway obstruction D. Post-traumatic deformity.
- The internal nasal valve is formed by the angle between which structures? A. Upper and lower lateral cartilages B. Septum and upper lateral cartilage C. Septum and lower lateral cartilage D. Nasal bones and upper lateral cartilage.
- Which graft is used to prevent internal nasal valve collapse? A. Alar batten graft B. Spreader graft C. Columellar strut graft D. Shield graft.
- When should revision rhinoplasty generally be performed? A. 3 months after primary surgery B. 6 months after primary surgery C. 12 months after primary surgery D. Immediately if the patient is dissatisfied.
- Which of the following is a late functional complication of rhinoplasty? A. Septal haematoma B. Epistaxis C. Internal nasal valve collapse D. Wound infection.
- The open rhinoplasty approach uses which incision? A. Intercartilaginous incision B. Transcartilaginous incision C. Transcolumellar incision D. Marginal incision.
- Which cartilage is preferred for contour grafts when septal cartilage is unavailable? A. Conchal cartilage B. Costal cartilage C. Fresh frozen cadaveric cartilage D. Auricular cartilage.
MCQ Answers Key: 1. B 2. B 3. C 4. B 5. B 6. B 7. C 8. C 9. C 10. A
Clinical Case Scenarios
Case 1: A 32-year-old woman presents with a dorsal hump and nasal obstruction. On examination, she has a deviated nasal septum and bilateral inferior turbinate hypertrophy. What is the most appropriate surgical procedure? Answer: Septorhinoplasty with turbinate reduction. This combined approach addresses both the cosmetic deformity (dorsal hump) and the functional problems (septal deviation and turbinate hypertrophy) in a single operation.
Case 2: A 45-year-old man presents with nasal obstruction that worsens on deep inspiration. On examination, the nasal valve angle appears narrowed. The Cottle test improves his airflow. What is the most likely diagnosis and what is the best surgical intervention? Answer: Internal nasal valve collapse. The best surgical intervention is placement of spreader grafts between the septum and upper lateral cartilage to widen the nasal valve angle.
Case 3: A 25-year-old woman who underwent rhinoplasty 18 months ago presents with a persistent dorsal hump and an inverted V deformity. What is the most likely cause and what is the recommended management? Answer: The inverted V deformity results from collapse of the upper lateral cartilages after hump reduction. The recommended management is revision rhinoplasty with spreader grafts to reconstruct the middle vault. Revision surgery should be delayed until at least 12 months after the primary procedure.
Case 4: A 55-year-old man with a history of nasal trauma presents with a saddle nose deformity and nasal obstruction. Examination reveals a septal perforation. What is the most appropriate surgical approach? Answer: Open septorhinoplasty with cartilage grafting. The open approach provides excellent exposure for septal perforation repair and dorsal augmentation using cartilage grafts. Septal cartilage is preferred if available; otherwise, costal or conchal cartilage may be used.
Frequently Asked Questions (FAQ)
- What is the difference between rhinoplasty and septorhinoplasty? Rhinoplasty reshapes the external nose, while septorhinoplasty combines septoplasty (correction of septal deviation) with rhinoplasty to address both functional and cosmetic issues in a single operation.
- What is the recovery time after rhinoplasty? Most patients return to normal activities within 2 weeks, but swelling may persist for several months, and the final cosmetic result typically becomes apparent 6 to 12 months after surgery.
- What are the common complications of rhinoplasty? Early complications include bleeding, septal haematoma, and infection. Late complications include persistent nasal obstruction, nasal valve collapse, and cosmetic deformities such as polly-beak or inverted V deformity.
- When is revision rhinoplasty indicated? Revision rhinoplasty is indicated for persistent functional problems (nasal obstruction, valve collapse) or unsatisfactory cosmetic results (residual deformity, overcorrection, undercorrection). It should be delayed for at least 12 months.
- What grafts are used in rhinoplasty? Common grafts include spreader grafts (for internal nasal valve), columellar strut grafts (for tip support), alar batten grafts (for external nasal valve), and dorsal onlay grafts (for augmentation). Septal cartilage is the preferred source.
- What is the Cottle test? The Cottle test is a bedside manoeuvre where lateral traction is applied to the cheek; improvement in airflow suggests internal nasal valve collapse.
- Is rhinoplasty safe in children? Rhinoplasty is generally avoided until facial growth is complete, except in selected patients with severe functional impairment or post-traumatic deformity.
———End———–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Rhinoplasty notes, Septorhinoplasty notes, Rhinoplasty surgery notes, Rhinoplasty MBBS, Rhinoplasty ENT PG, Rhinoplasty NEET PG, Rhinoplasty INI CET, Rhinoplasty FMGE, Rhinoplasty viva questions, Rhinoplasty MCQs, Rhinoplasty exam guide, Rhinoplasty revision notes, Septorhinoplasty procedure, Septoplasty and rhinoplasty difference, Open rhinoplasty vs closed rhinoplasty, Structural rhinoplasty notes, Rhinoplasty indications, Rhinoplasty contraindications, Rhinoplasty complications, Rhinoplasty grafts, Septal cartilage graft, Saddle nose deformity, Dorsal hump correction, Nasal tip surgery, Rhinoplasty operative steps, Rhinoplasty postoperative care, Revision rhinoplasty, Functional rhinoplasty, Cosmetic rhinoplasty, Reconstructive rhinoplasty, Rhinoplasty CBME notes, ENT surgery notes, Nose surgery notes, Rhinoplasty flowchart, Rhinoplasty mnemonics, Rhinoplasty summary, Rhinoplasty viva guide, Rhinoplasty practical exam, Rhinoplasty OSCE, Rhinoplasty long question, Rhinoplasty short notes, Rhinoplasty exam revision, Septorhinoplasty high yield, Rhinoplasty anatomy for surgery, Rhinoplasty classification.