Cerebrospinal Fluid (CSF) Rhinorrhoea
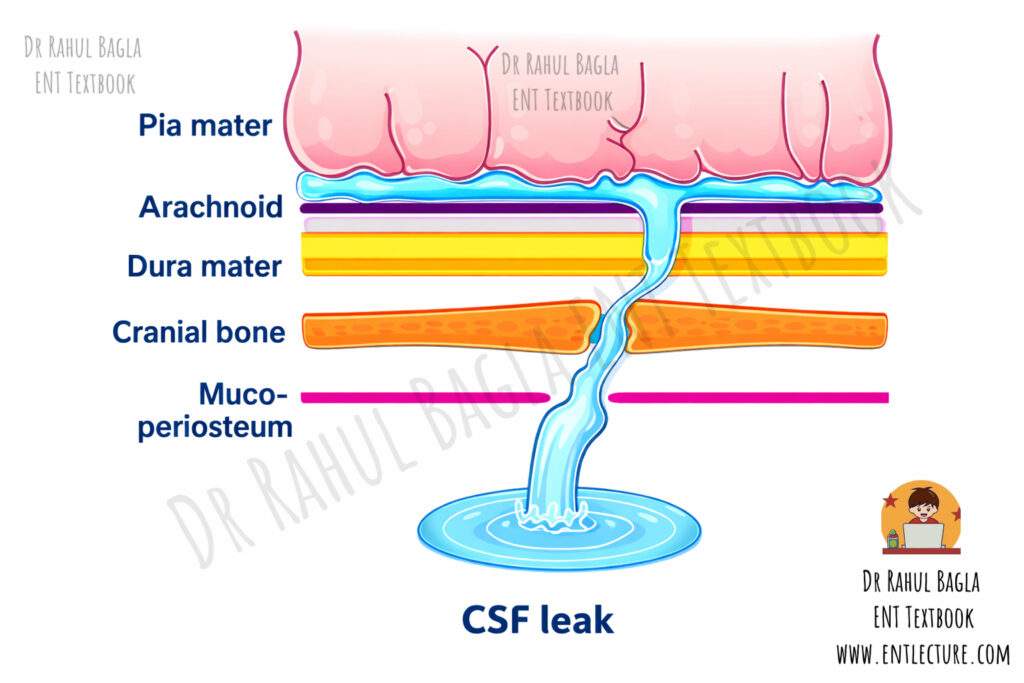
Cerebrospinal fluid (CSF) rhinorrhoea is a condition characterised by the leakage of CSF from the nose. This is not a disease in itself but rather a symptom of an underlying problem. Fundamentally, it results from an abnormal communication, or fistula, between the subarachnoid space and the nasal cavity or paranasal sinuses.
CSF rhinorrhoea occurs only when two defects are present. A bony defect develops in the skull base, and a tear occurs in the overlying dura mater. These defects create a communication between the intracranial cavity and the nasal cavity. As a result, clear, watery CSF leaks through the nose.
This condition is clinically serious because it forms a direct pathway for bacteria from the nasal cavity to enter the normally sterile central nervous system. This can lead to life-threatening complications, most commonly meningitis, and rarely pneumocephalus (air within the cranial cavity). In fact, some patients present with recurrent episodes of meningitis, and only after thorough investigation are they ultimately diagnosed with an occult CSF leak.
Physiology of Cerebrospinal Fluid (CSF)
CSF is a clear, plasma-like fluid that surrounds the brain and spinal cord and forms a protective fluid cushion. It acts as a shock absorber and protects the central nervous system from sudden jerks and mechanical injury. CSF is produced by the choroid plexus in the lateral, third, and fourth ventricles. The fluid then circulates through the ventricular system and reaches the subarachnoid space. The arachnoid villi absorb CSF into the dural venous sinuses. These villi act as one-way valves. They allow CSF to move from the subarachnoid space into the venous blood, but they prevent reverse flow from blood to CSF.
The total volume of CSF in adults ranges from 90 to 150 mL. The body produces CSF at a rate of about 20 mL per hour (350–500 mL per day). Therefore, the entire CSF volume replaces itself three to five times every day. The normal CSF pressure during lumbar puncture ranges from 50–150 mm H₂O. CSF pressure increases during coughing, sneezing, nose blowing, straining during defecation, or lifting heavy objects. Patients with CSF leaks or those who have had CSF repair surgery should avoid these activities because they increase intracranial pressure and worsen the leak.
Aetiology of Cerebrospinal fluid (CSF) rhinorrhoea
CSF rhinorrhoea develops due to trauma, spontaneous causes, or congenital defects. Trauma remains the most common cause, while spontaneous leaks are strongly associated with raised intracranial pressure. Congenital causes mainly affect children and involve persistent anatomical pathways.
A. Traumatic
- Accidental Trauma: This is the most common cause, accounting for approximately 80% of cases. It usually follows fractures of the anterior skull base, especially involving the cribriform plate, frontal sinus, or sphenoid sinus. These fractures create a defect in the bone and dura mater, allowing CSF to leak into the nasal cavity.
- Iatrogenic (Surgical) Trauma: Surgical trauma causes about 20% of CSF rhinorrhoea cases, and its incidence is increasing due to the widespread use of endoscopic sinus surgery (ESS). Common procedures that may cause CSF leaks include Endoscopic sinus surgery (ESS), Trans-sphenoidal hypophysectomy, Nasal polypectomy, Skull base surgery and Neurosurgical procedures. During ESS, the junction of the lateral lamella of the cribriform plate and the fovea ethmoidalis is the most vulnerable site because this area is extremely thin. Even minor surgical injury at this site can cause a bony defect and dural tear, leading to CSF leak.
B. Spontaneous (Non-Traumatic). Spontaneous CSF leaks occur without any history of trauma. They commonly develop due to chronically raised intracranial pressure (ICP).
- Idiopathic Intracranial Hypertension (IIH): This is the most important cause. Long-standing raised ICP leads to progressive remodelling, thinning, and erosion of the skull base bones. At the cribriform plate, for instance, the raised pressure causes dilatation of the dural sheaths surrounding the olfactory nerve filaments, creating a pathway for leakage. These leaks may be multiple.
- Tumours: Tumours of the skull base can also cause CSF rhinorrhoea. Tumours such as pituitary adenomas and olfactory groove meningiomas directly erode bone and dura, leading to leakage.
- Congenital Anomalies: These are more common in children and involve persistent embryonic pathways.
- Other conditions, such as hydrocephalus and dural sinus thrombosis, increase intracranial pressure and predispose patients to CSF leakage.
C. Congenital Leaks. In children, CSF rhinorrhoea can result from persistent fetal communications.
- Inner Ear Dysplasias: Anomalies like Mondini malformation (incomplete partition of the cochlea) or a patent cochlear aqueduct can allow CSF to leak into the middle ear. From there, it drains via the Eustachian tube into the nasopharynx and nose, presenting as CSF otorhinorrhoea.
- Skull Base Pathways: A persistent craniopharyngeal canal or Sternberg’s canal (lateral craniopharyngeal canal) can lead to a leak from the lateral recess of the sphenoid sinus.
Table: Summary of Classification of CSF Rhinorrhoea
| Type | Subtype | Key Features & Examples |
| Traumatic | Accidental | Most common cause (80%). Due to fracture of the anterior skull base, such as those involving the cribriform plate, frontal sinus, or sphenoid sinus. |
| Iatrogenic | Seen in 20% of cases, and its incidence is increasing. Common during endoscopic sinus surgery at the cribriform plate-fovea ethmoidalis junction. | |
| Spontaneous | High-Pressure Leaks | Associated with Idiopathic Intracranial Hypertension (IIH), typically in middle-aged, obese females. Can present with empty sella syndrome. |
| Normal-Pressure Leaks | Due to tumours, skull base erosions from infection or inflammation. | |
| Congenital | Inner Ear Anomalies | E.g., Mondini dysplasia. Leak reaches the nose via the Eustachian tube (CSF otorhinorrhoea). |
| Skull Base Defects | e.g., Persistent craniopharyngeal canal (Sternberg’s canal). |
Clinical Features and Presentation of Cerebrospinal fluid (CSF) rhinorrhoea
The presentation can be classic or subtle, and a high index of suspicion is required.
Symptoms
- Clear Watery Discharge: This is the hallmark symptom. The discharge is typically unilateral, though it can be bilateral. Patients often report a constant runny nose. A key differentiator from allergic rhinitis is that the patient cannot sniff the discharge back; it flows forward persistently.
- Positional Variation (Reservoir Sign): The discharge increases dramatically when the patient bends forward, strains, or rises from a recumbent position. This happens because CSF accumulates in the sinuses (the “reservoir”) and then pours out when the head position changes.
- Postural Headache: A headache that is worse when upright and better when lying down suggests low CSF pressure (intracranial hypotension) due to the leak.
- Salty or Metallic Taste: Patients may notice a salty or metallic taste in the back of their throat as the CSF drips down.
- Recurrent Meningitis: A history of one or more episodes of pneumococcal meningitis is a red flag for an undiagnosed CSF leak.
Signs
- Halo Sign (or Double-Ring Sign): This is a simple bedside test for a bloody discharge. When a drop lands on a filter paper or bedsheet, it separates into two rings: a central, inner ring of blood and a larger, outer, lighter ring of CSF, which diffuses further. However, this sign is not specific to CSF and can be seen with any serosanguinous fluid (e.g., from allergic rhinitis), so it is only a screening tool.
- Target Sign: Similar to the halo sign, observed on a gauze piece.
The Typical Spontaneous Leak Patient
A classic clinical picture is a middle-aged, obese female presenting with a unilateral watery nasal discharge. She may have a history of headaches (suggesting IIH) and is often misdiagnosed and treated for allergic rhinitis for months before the correct diagnosis is made.
Anatomy: Sites of Leak of Cerebrospinal Fluid (CSF) rhinorrhoea
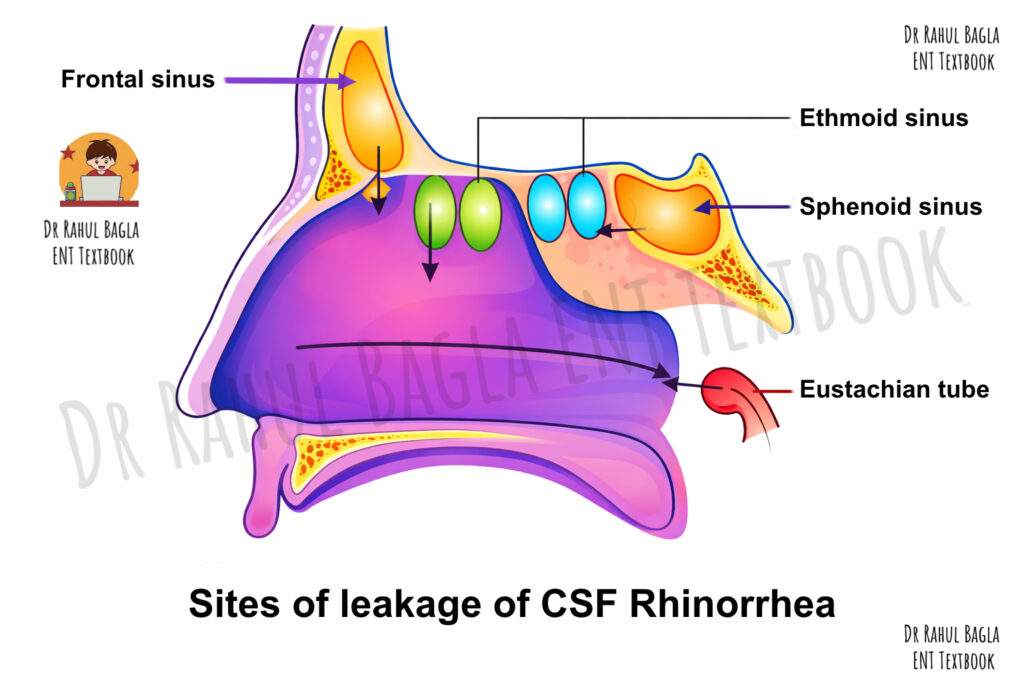
The site of CSF leakage depends on the location of the skull base defect. CSF from different cranial fossae follows specific pathways to reach the nose.
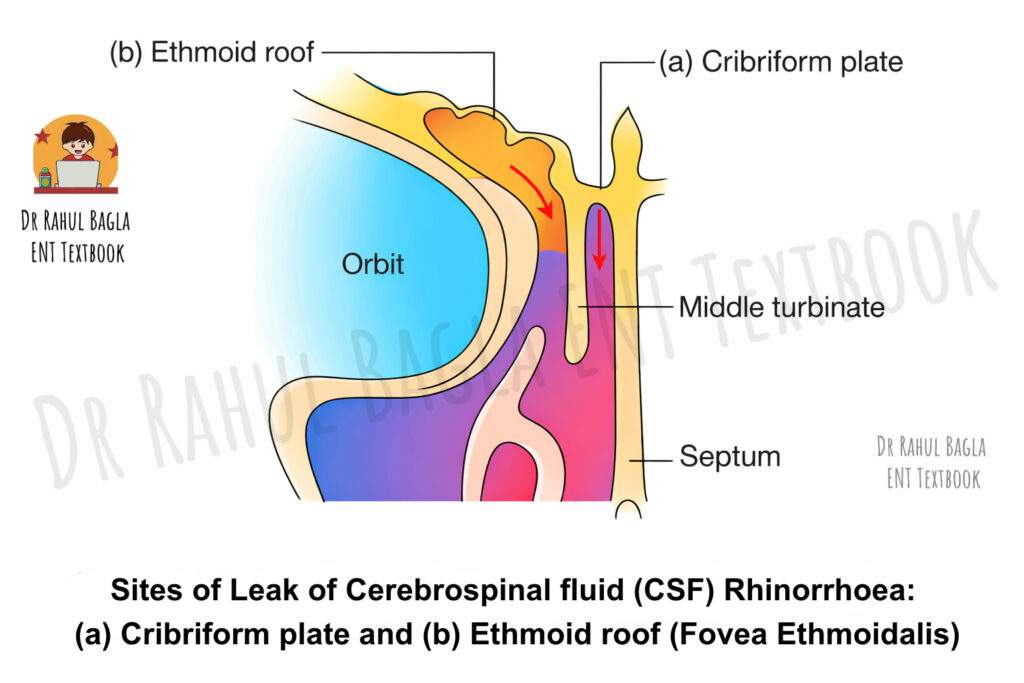
- CSF from the anterior cranial fossa most commonly leaks into the nasal cavity. It passes through the cribriform plate, which is thin and perforated by olfactory nerve filaments, making it the most frequent site of leakage. CSF may also leak through the roof of the ethmoid air cells (fovea ethmoidalis) or through defects in the frontal sinus. The junction of the lateral lamella of the cribriform plate and the fovea ethmoidalis is the most vulnerable site because this area is extremely thin.
- CSF from the middle cranial fossa usually leaks through the sphenoid sinus. Injury or erosion in this region allows CSF to pass into the sphenoid sinus and then into the nasal cavity.
- In temporal bone fractures, CSF follows a different route. It first enters the middle ear cavity, then passes through the Eustachian tube into the nasopharynx, and finally appears as nasal discharge. This condition is known as CSF otorhinorrhoea.
Investigations: A Stepwise Approach
The investigation aims to confirm that the fluid is CSF and to localise the site of the leak.
Fluid Analysis
- Beta-2 Transferrin (Tau Protein): This is the non-invasive gold standard for confirming a fluid as CSF. Beta-2 transferrin is a protein found almost exclusively in CSF (and perilymph). It is highly sensitive and specific.
- Beta-Trace Protein (Prostaglandin D Synthase): Another highly sensitive marker, often used as a rapid test.
- Glucose and Protein: CSF typically has a glucose concentration of >30 mg/dL (or >50-60% of blood glucose) and a lower protein concentration than nasal mucus. However, these tests are less reliable as nasal secretions can contaminate the sample, leading to false results. A simple urinary dipstick for glucose is not a reliable test.
Radiology. Imaging helps to identify the site of the bony defect.
- High-Resolution Computed Tomography (HRCT): It is the initial investigation of choice and provides excellent bone detail. It uses thin sections (0.5–1 mm) in coronal and sagittal planes to clearly show the skull base defect. It is quick, non-invasive, and excellent for surgical planning.
- Magnetic Resonance Imaging (MRI): It complements HRCT and provides soft tissue details.
- T2-Weighted Sequences: CSF is hyperintense (bright). MRI can show a fluid column traversing the defect and can identify associated meningoceles or encephaloceles (herniation of meninges or brain tissue through the defect).
- Brain Findings: MRI is excellent for picking up signs of raised ICP, such as an empty sella syndrome (where the pituitary gland is flattened by CSF pressure) or dilated optic nerve sheaths.
- CT Cisternography: This is an invasive test where contrast is injected into the thecal sac via lumbar puncture. After manoeuvring the patient to encourage leakage, a CT scan is performed. It is considered the gold standard for localising an active leak when the site is not clear on HRCT or MRI. However, it is less useful for intermittent or inactive leaks.
Table: Comparison of Key Investigations
| Investigation | Purpose | Advantages | Disadvantages |
| Beta-2 Transferrin | Confirm fluid is CSF | Non-invasive, highly sensitive & specific | Expensive, not universally available |
| HRCT | Locate a bony defect | Excellent bone detail, Quick, Non-invasive | Cannot differentiate CSF from other fluids. No info on brain/meninges |
| MRI | Assess for encephalocele, signs of raised ICP | Excellent soft tissue detail, Non-invasive | Poor bone detail, Longer scan time |
| CT Cisternography | Gold standard for active leak localisation | Dynamic test, Pinpoints the exact leak site | Invasive (LP), Radiation, Only useful for active leaks |
Table: Differences between CSF and Nasal secretions
|
Feature |
CSF Rhinorrhoea |
Nasal Secretion |
|
History |
Head injury, Nasal/sinus surgery, Intracranial tumour |
Sneezing, Nasal blockage, Itching, Watering from eyes |
|
Flow of discharge |
Increases on bending forward / straining, Cannot sniff back |
Continuous, No change with posture, Can sniff back |
|
Nature (Character) |
Thin, watery, clear |
Thick (mucus) or watery (tears) |
|
Taste |
Sweet |
Salty |
|
Sugar level |
> 30 mg/dL |
< 10 mg/dL |
|
β₂-transferrin |
Present (specific for CSF) |
Absent |
Management of Cerebrospinal fluid (CSF) rhinorrhoea
The goal of management is to stop the leak and prevent ascending meningitis.
Conservative Management. This is the first-line approach for most post-traumatic leaks. It is indicated in a recent onset (<7 days) of traumatic leak.
- Bed Rest: The patient is nursed in a 15-30 degree head-up position to reduce ICP.
- Avoid Straining: Stool softeners are given to prevent the Valsalva manoeuvre.
- Avoid Nose Blowing: The patient is strictly instructed not to blow their nose for at least 2-3 weeks.
- Observation: Most traumatic leaks (approximately 80%) will close spontaneously within 7-10 days with these measures.
Medical Management
- Acetazolamide: A carbonic anhydrase inhibitor that reduces CSF production by the choroid plexus. It is used to lower ICP, especially in patients with spontaneous leaks and IIH.
- Topiramate: An antiepileptic that also has carbonic anhydrase inhibitor properties. It is considered more potent than acetazolamide in lowering ICP.
- Antibiotics: The role of prophylactic antibiotics in traumatic leaks is debated. They are often given for 5-7 days, but their benefit in preventing meningitis is not conclusively proven and may select for resistant organisms.
Surgical Management. Surgery is indicated for:
- Leaks persisting for >10-14 days despite conservative measures.
- Large skull base defects.
- Leaks associated with encephaloceles or meningoceles.
- Spontaneous and congenital leaks.
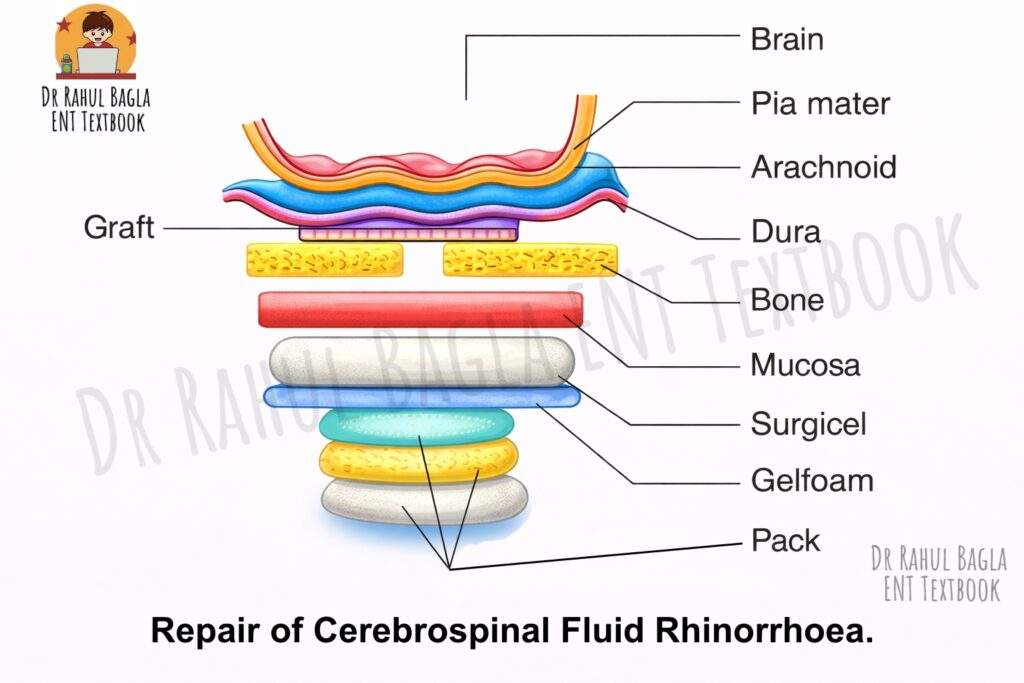
The Endoscopic Endonasal Approach. This is the modern standard of care, having largely replaced open craniotomy due to its superior visualisation, lower morbidity, and high success rate (>90%). Its principle. The repair is a multilayered closure that recreates the barrier between the intracranial and nasal cavities. Steps are:
- Identification: The precise site of the leak is identified endoscopically. If not visible, intrathecal fluorescein can be used.
- Preparation: A margin of mucosa (at least 5 mm) is carefully stripped from around the bony defect. Any loose bone spicules are removed.
- Graft Placement:
- Underlay (Intracranial) Graft: A piece of cartilage (e.g., from the nasal septum), bone, or fascia is placed between the dura and the skull base, plugging the defect from above.
- Overlay (Extracranial) Graft: A free mucosal graft or a vascularised flap is placed over the bony defect on the nasal side.
- Support: The grafts are held in place with absorbable packing, fibrin glue, and Gelfoam.
Intrathecal Fluorescein: This is a valuable adjunct. A small amount of CSF is removed via lumbar puncture, mixed with 10% fluorescein (0.1 ml), and then reinjected slowly. During endoscopy with a blue light filter, the fluorescein glows bright green, pinpointing the exact leak site. A separate consent is mandatory as this is an off-label use with a risk of neurotoxicity if doses are exceeded.
Vascularised Flaps. For large defects, especially after tumour resection, vascularised flaps provide a robust, well-healing closure. Hadad-Bassagasteguy Flap (Nasoseptal Flap): This is the workhorse. It is a mucoperiosteal and mucoperichondrial flap based on the septal branch of the sphenopalatine artery. It is harvested from the nasal septum and rotated to cover the defect.
Management of Meningoencephaloceles
If a meningocele or encephalocele is present, it is carefully reduced or amputated, and its contents are cauterised with bipolar diathermy. The resulting dural and bony defect is then repaired as described above.
Post-Operative Care
- Position: Bed rest with head elevated (15-30 degrees).
- Precautions: Strict instructions to avoid nose blowing, sneezing with an open mouth, straining, and heavy lifting for 2-4 weeks.
- Medications: Broad-spectrum antibiotics, stool softeners, and antiemetics are prescribed.
- Lumbar Drain: In select high-risk patients (e.g., those with IIH, large leaks), a lumbar drain may be placed for 3-5 days post-operatively to divert CSF and reduce pressure on the repair site. Its routine use is not recommended.
——– End of the Chapter——–
High-Yield Points for Exams
- Most common cause: Accidental trauma (80%).
- Most common site: Cribriform plate.
- Most common site for iatrogenic leak: Junction of the lateral lamella of the cribriform plate and fovea ethmoidalis.
- Gold standard confirmatory test: Beta-2 transferrin assay.
- Gold standard imaging for localising an active leak: CT Cisternography.
- Initial imaging of choice: High-Resolution CT (HRCT) skull base.
- Most common presentation of spontaneous leak: Middle-aged, obese female with unilateral watery rhinorrhoea.
- Classic MRI finding in spontaneous leak: Empty Sella Syndrome.
- First-line management for recent traumatic leak: Conservative (bed rest, head-up position, no straining).
- Standard of care for surgical repair: Endoscopic endonasal repair.
- Most common vascularised flap: Hadad-Bassagasteguy flap (Nasoseptal flap).
- Drugs to reduce ICP: Acetazolamide and Topiramate (Topiramate is more potent).
- Triad for CSF otorhinorrhoea: Congenital inner ear anomaly (e.g., Mondini dysplasia) -> CSF leak into middle ear -> Eustachian tube -> Nose.
NEET PG Style Multiple Choice Questions (MCQs)
- A 45-year-old obese female presents with unilateral clear watery discharge from the right nostril for 6 months. She has been treated for allergic rhinitis without relief. The discharge increases when she bends down to tie her shoes. What is the most likely diagnosis? a) Allergic rhinitis b) Vasomotor rhinitis c) CSF rhinorrhoea d) Sinonasal polyp
- Which of the following is the most common cause of CSF rhinorrhoea overall? a) Spontaneous b) Iatrogenic c) Congenital d) Accidental trauma
- A patient presents with bloody nasal discharge following a head injury. A drop of the discharge on a filter paper shows a central blood stain with a surrounding clear halo. This sign is: a) Diagnostic of CSF leak, b) Highly specific for CSF, c) A non-specific sign for serous fluid, d) Pathognomonic of skull base fracture
- The investigation of choice to non-invasively confirm that a nasal fluid is CSF is: a) High-resolution CT scan, b) Glucose estimation c) Beta-2 transferrin assay, d) CT cisternography
- Which of the following is the most common site for an iatrogenic CSF leak during endoscopic sinus surgery? a) Frontal recess b) Maxillary sinus ostium c) Junction of lateral lamella of cribriform plate and fovea ethmoidalis d) Sphenoid sinus ostium
- A 10-year-old child presents with recurrent meningitis and a history of unilateral watery nasal discharge. On examination, the nasal discharge increases on bending forward. HRCT temporal bone shows Mondini dysplasia. What is the most likely pathway of the CSF leak? a) Through the cribriform plate b) Through a persistent craniopharyngeal canal c) From the internal auditory canal to the middle ear and then via the Eustachian tube d) Through a defect in the fovea ethmoidalis
- What is the first-line management for a 30-year-old patient who developed CSF rhinorrhoea 2 days after a road traffic accident? a) Immediate endoscopic repair b) Intrathecal fluorescein injection c) Conservative management with bed rest and head elevation d) Placement of a lumbar drain
- The Hadad-Bassagasteguy flap, used in endoscopic skull base reconstruction, is based on which artery? a) Anterior ethmoidal artery b) Posterior ethmoidal artery c) Greater palatine artery d) Nasoseptal branch of the sphenopalatine artery
- Which medication is most effective for reducing intracranial pressure in a patient with a spontaneous CSF leak? a) Furosemide b) Mannitol c) Acetazolamide d) Topiramate
- An MRI finding of “empty sella” in a patient with CSF rhinorrhoea suggests: a) A pituitary tumour, b) A congenital anomaly, c) Chronically raised intracranial pressure, d) A leak from the frontal sinus
Answers
- (c)
- (d)
- (c)
- (c)
- (c)
- (c)
- (c)
- (d)
- (d)
- (c)
Clinical Case Scenarios for Viva/Practical Exams
Scenario 1: A 50-year-old male, a known case of acromegaly, underwent endoscopic transsphenoidal resection of a pituitary macroadenoma 5 days ago. On post-op day 5, he complains of a “salty taste” in his mouth and notices a clear fluid dripping from his left nostril when he leans forward.
- Question 1: What is your diagnosis?
- Question 2: How would you confirm the nature of the fluid?
- Question 3: What is the initial step in management?
- Question 4: If the leak persists, what surgical approach would you consider?
Scenario 2: A 35-year-old woman presents to the ENT OPD with a 1-year history of a persistent runny nose on the right side. She has tried multiple nasal sprays from her local doctor with no improvement. She is otherwise healthy but has a BMI of 34. On examination, anterior rhinoscopy is normal. You ask her to bend forward, and a gush of clear fluid comes out of her right nostril.
- Question 1: What is your differential diagnosis?
- Question 2: What is the most likely underlying condition in this patient profile?
- Question 3: What is the single best radiological investigation to order first?
- Question 4: If this investigation shows a defect in the cribriform plate, what is the definitive management?
Frequently Asked Questions in Viva
- What is the reservoir sign in CSF rhinorrhoea? The reservoir sign refers to the increase in nasal discharge when the patient bends forward or moves from a lying to a standing position, as CSF that has pooled in the sinuses (the reservoir) drains out.
- Is the halo sign reliable for diagnosing CSF? No, the halo sign is not reliable. It is a simple bedside screening test, but is non-specific, as any fluid mixed with blood can produce a similar ring pattern on filter paper.
- What is the difference between CT and CT cisternography? HRCT is a static scan that shows the bony anatomy and can suggest a defect. CT cisternography is a dynamic test where contrast is injected into the CSF via lumbar puncture, and then a CT is performed to see the contrast actively leaking out, which precisely localises the fistula site during an active leak.
- Why is separate consent required for the use of intrathecal fluorescein? Intrathecal use of fluorescein is an “off-label” use, meaning it is not a formally approved indication by drug regulatory authorities. Therefore, explicit informed consent from the patient is mandatory, explaining the potential (though rare) risks of neurotoxicity, including seizures, lower limb weakness, and paraesthesia.
- When is a lumbar drain used in the management of CSF rhinorrhoea? Lumbar drains are used selectively, not routinely. They are most helpful in high-risk patients, such as those with very high ICP (e.g., IIH), large or complex skull base defects, or as a temporary measure to divert CSF and protect a fresh surgical repair in the immediate post-operative period.
- Can CSF rhinorrhoea be mistaken for something else? Yes, it is commonly misdiagnosed as allergic rhinitis or vasomotor rhinitis because it presents with a clear, watery discharge. The key differentiators are the unilateral nature, positional variation (reservoir sign), and lack of response to standard anti-allergy treatment.
——– End——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: CSF rhinorrhoea notes, CSF leak causes and management, CSF rhinorrhoea classification, Beta-2 transferrin test, Empty sella syndrome ENT, CSF leak CT scan, Skull base defect repair, Endoscopic CSF leak repair, Hadad flap, CSF rhinorrhoea vs allergic rhinitis, CSF rhinorrhoea NEET PG questions, CSF leak treatment guidelines, Anterior skull base fractures, Meningitis and CSF leak, CSF otorhinorrhoea, Intrathecal fluorescein use, Idiopathic intracranial hypertension ENT, CSF rhinorrhoea surgery, Post-traumatic CSF leak management, Spontaneous CSF leak, CBME ENT notes, CSF rhinorrhoea revision, ENT PG entrance exam guide, CSF Rhinorrhoea Notes For MBBS Students, CSF Rhinorrhoea ENT Exam Guide, CSF Rhinorrhoea Summary For NEET PG, CSF Leak From Nose Causes Diagnosis Treatment, CSF Rhinorrhoea Mnemonics For Medical Students, CSF Rhinorrhoea Viva Questions ENT, CSF Rhinorrhoea Flowchart Diagnosis Management, Reservoir Sign In CSF Rhinorrhoea Explained, Halo Sign CSF Leak ENT MCQ Guide, Beta 2 Transferrin Test CSF Rhinorrhoea Diagnosis, CT Cisternography Gold Standard CSF Leak Investigation, Endoscopic Repair Of CSF Leak ENT Surgery Notes, CSF Otorhinorrhoea Causes Mondini Malformation, Empty Sella Syndrome CSF Leak ENT Concept, CSF Rhinorrhoea Clinical Case Scenarios ENT PG Revision, CSF Rhinorrhoea CBME Curriculum ENT Notes, CSF Leak Nose Symptoms Diagnosis Treatment Medical Students, CSF Rhinorrhoea Quick Revision High Yield Points NEET PG