Vestibular Schwannoma (Acoustic Neuroma, neurilemmoma or eighth nerve tumour)
Introduction
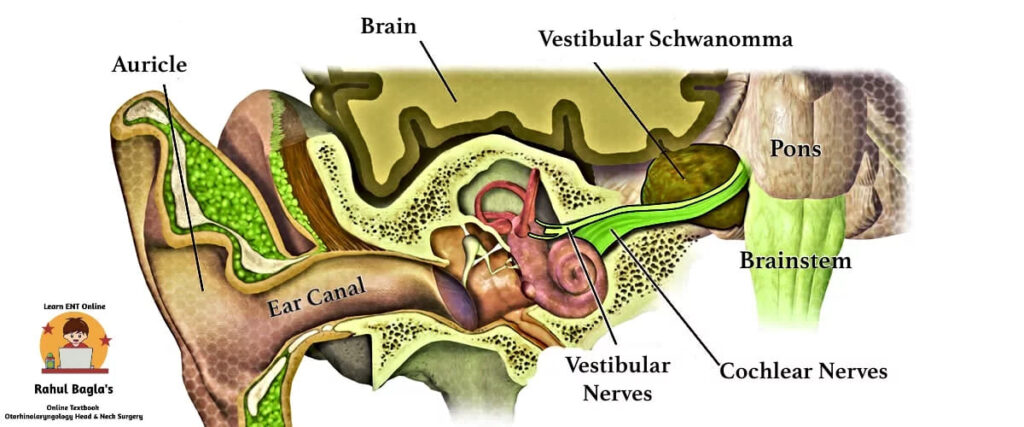
Vestibular schwannoma (acoustic neuroma) is a benign, slow-growing tumour arising from the Schwann cells of the vestibular division of the vestibulocochlear nerve (CN VIII). Although it is commonly called an acoustic neuroma, this name is technically incorrect because the tumour arises from the vestibular nerve, not the cochlear (acoustic) nerve.
The tumour usually grows slowly over several years and compresses nearby nerves and the brainstem as it enlarges. However, malignant transformation is extremely rare. Vestibular schwannoma accounts for 80–90% of all cerebellopontine angle (CPA) tumours, while the remaining tumours include meningiomas, epidermoid cysts, and other rare lesions. Overall, CPA tumours constitute about 10% of all intracranial tumours. Patients usually present with unilateral sensorineural hearing loss, tinnitus, and imbalance. MRI with gadolinium is the gold standard investigation.
This chapter covers anatomy, pathology, clinical features, MRI findings, diagnosis, treatment, surgery, viva questions, MCQs, and high-yield revision notes for MBBS, ENT PG, INI-CET, FMGE, and NEET PG.
Relevant Surgical Anatomy
Pathology (Earliest nerve involved in acoustic neuroma)
Vestibular schwannoma usually arises from the Schwann cells of the inferior vestibular nerve, although it may also originate from the superior vestibular nerve. Earlier studies considered the superior vestibular nerve to be the common site of origin; however, current evidence shows that the inferior vestibular nerve is affected more often.
The tumour usually begins at the Obersteiner-Redlich zone, where central myelin changes to peripheral myelin near the internal auditory canal (IAC). As it enlarges, the tumour compresses the nerve instead of invading it.
| Bill’s bar is named after William House (nickname Dr Bill). Bill’s bar is a vertical bony ridge located at the fundus of the internal auditory canal. It separates the facial nerve from the superior vestibular nerve. Surgeons use Bill’s bar as an important landmark because it helps them identify the facial nerve early during vestibular schwannoma surgery. Since most tumours arise from the vestibular nerve, the facial nerve usually remains uninvolved initially but becomes compressed as the tumour enlarges. |

Anatomy of Internal canal:
The internal auditory canal (IAC) is a critical structure in the pathogenesis and progression of vestibular schwannomas. It is divided into four quadrants by two anatomical landmarks: the crista falciformis (a horizontal bony ridge) and Bill’s bar (a vertical bony crest). The contents of these quadrants are as follows:
- Anterior Superior Quadrant: Contains the motor root of the facial nerve and the nervus intermedius.
- Posterior Superior Quadrant: Contains the superior vestibular nerve.
- Anterior Inferior Quadrant: Contains the cochlear nerve.
- Posterior Inferior Quadrant: Contains the inferior vestibular nerve.
There is a close anatomical relationship between the motor root of the facial nerve, nervus intermedius and the vestibulocochlear nerve. This explains the disturbances in lacrimation, taste, salivary flow, hearing, balance or facial motor control that may result from lesions in either the cerebellopontine angle or internal acoustic meatus.
Boundaries of Cerebellopontine angle:
The cerebellopontine angle (CPA) is a triangular space located in the posterior cranial fossa. It is bordered by the following structures:
- Posteriorly: The cerebellum
- Anteromedially: The pons
- Laterally: The petrous part of the temporal bone
This space is a common site for the development of vestibular schwannomas and other CPA tumours, which can compress the adjacent cranial nerves and brainstem, leading to a variety of neurological deficits.
Aetiology
Vestibular schwannomas can occur due to several etiological factors, including:
- Idiopathic: Most cases of vestibular schwannoma occur sporadically without a known cause. The incidence is highest in individuals aged 40-60 years, with no significant difference in prevalence between males and females.
- Genetic: Bilateral vestibular schwannomas are the characteristic feature of Neurofibromatosis Type 2 (NF2), an autosomal dominant disorder caused by mutation of the NF2 gene located on chromosome 22q12. The NF2 gene encodes the tumour suppressor protein Merlin (Schwannomin), which regulates Schwann cell proliferation. Loss of Merlin function results in uncontrolled Schwann cell growth and tumour formation. Patients with NF2 usually present at a younger age than those with sporadic vestibular schwannomas and frequently develop multiple intracranial and spinal tumours, including meningiomas, ependymomas, and schwannomas involving other cranial and peripheral nerves.
- Environmental: Exposure to high-dose ionising radiation has been identified as a risk factor for the development of vestibular schwannomas, though this is relatively uncommon.
Natural History of Tumour
Vestibular schwannoma usually grows slowly. However, its growth pattern varies among patients. Some tumours continue to enlarge, whereas others remain unchanged for many years. Rarely, the tumour may even shrink spontaneously. Therefore, we cannot accurately predict the behaviour of an individual tumour at diagnosis.
Long-term observational studies have shown that approximately 70% of extrameatal vestibular schwannomas remain unchanged, 29% demonstrate measurable growth, and about 1% decrease in size during follow-up. Among intrameatal tumours, nearly 83% remain confined to the internal auditory canal, whereas 17% eventually develop extrameatal extension. Importantly, the majority of tumour growth occurs within the first five years after diagnosis. These observations have provided the scientific basis for the modern “wait-and-scan” (active surveillance) strategy in carefully selected patients with small, asymptomatic vestibular schwannomas.
Growth Pattern of Tumour
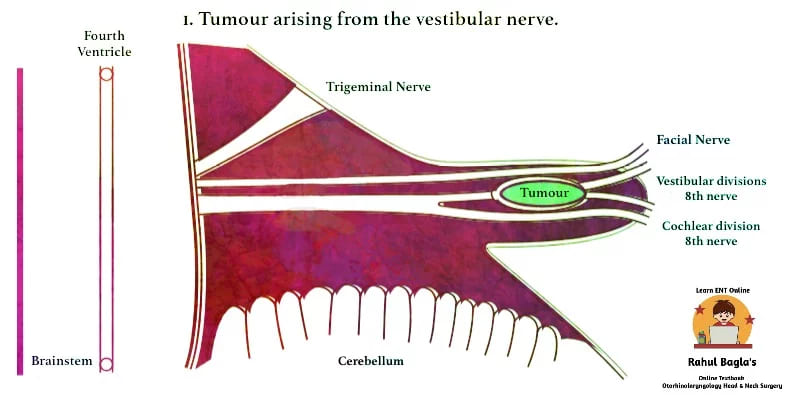
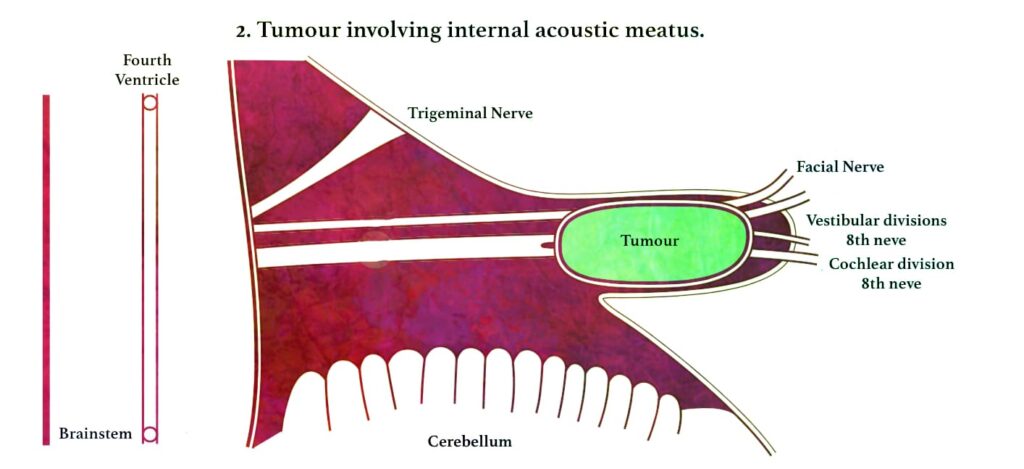
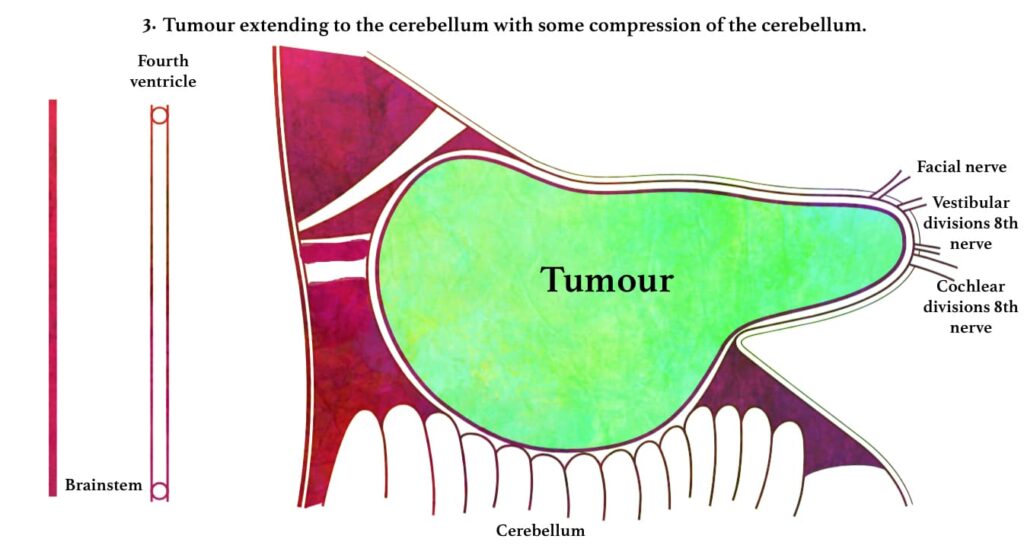
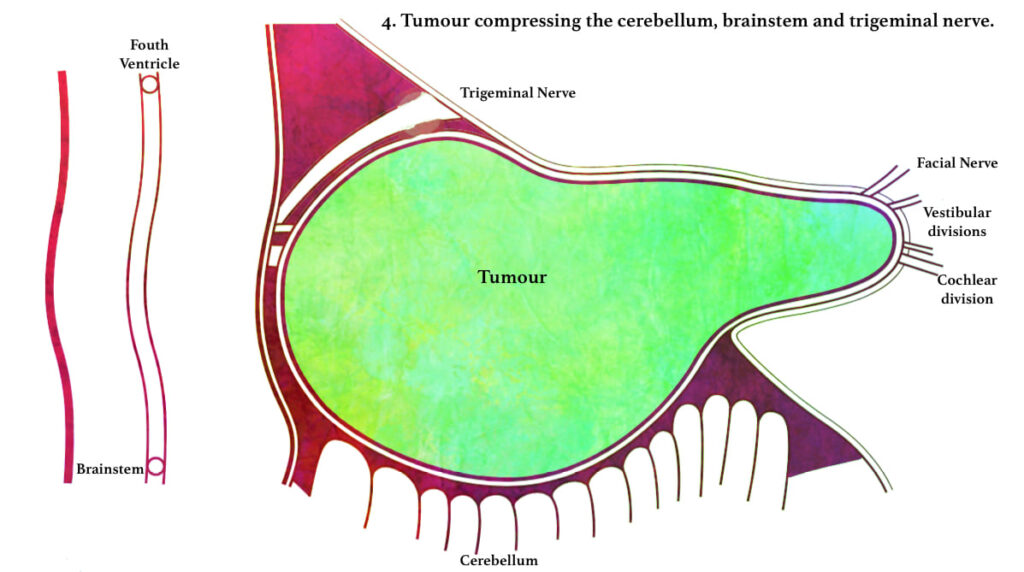
Vestibular schwannomas arise within the internal auditory canal and enlarge in a characteristic sequence. Initially, the tumour develops from the vestibular nerve and gradually fills the internal auditory canal. Continued enlargement causes widening of the bony canal due to slow bone resorption before the tumour extends through the porus acousticus into the cerebellopontine angle (CPA). As the tumour enlarges further, it progressively compresses the facial nerve (VII) and vestibulocochlear nerve (VIII), followed by the trigeminal nerve (V). Very large tumours may subsequently compress the lower cranial nerves (IX, X and XI), cerebellum and brainstem, and obstruct the fourth ventricle, resulting in obstructive hydrocephalus. If left untreated, progressive brainstem compression may become life-threatening.
The average growth rate is variable and may be categorised as:
- Slow growth: approximately 0.02 cm/year
- Medium growth: approximately 0.20 cm/year
- Fast growth: approximately 1.00 cm/year

.
.
.
Classification according to the size of the tumour
To standardise reporting, the Consensus Meeting on Reporting Systems for Vestibular Schwannoma (2003) recommended classifying vestibular schwannomas according to the largest extrameatal diameter.
 Intrameatal – The tumour is within the meatus and does not extend beyond the porus (medial end of IAC). Extrameatal size of such a tumour is zero.
Intrameatal – The tumour is within the meatus and does not extend beyond the porus (medial end of IAC). Extrameatal size of such a tumour is zero.
Alternatively, another commonly used classification includes:
- Intracanalicular: Tumour limited to the internal auditory canal.
- Small size: Tumour up to 1.5 cm.
- Medium size: Tumour between 1.5–4 cm.
- Large size: Tumour over 4 cm.
Tumour size is one of the most important determinants of treatment selection, hearing preservation, and prognosis.
Gross and Microscopic Appearance
Gross Appearance
Grossly, vestibular schwannomas are well-circumscribed, benign, encapsulated tumours.
- Small tumours are pink-yellow and rubbery.
- Larger tumours appear yellow, mottled, and may show haemorrhage, fibrosis, and cystic degeneration.
Microscopic Appearance
Microscopically, vestibular schwannomas are composed of two distinct histological patterns:
- Antoni A fibres: These are cellular, compact fibres with spindle-shaped cells and nuclei arranged in whorling or palisading patterns (Verocay bodies).
- Antoni B fibres: These are less cellular, loosely packed, and have a spongy appearance.
Most tumours display a predominance of Antoni A fibres with interspersed Antoni B areas.
Cystic Vestibular Schwannoma
Cystic vestibular schwannoma is an uncommon variant, accounting for approximately 5–6% of surgically treated vestibular schwannomas. Histologically, these tumours contain increased amounts of Antoni B tissue, with cyst formation occurring within the tumour.
Compared with solid vestibular schwannomas, cystic tumours often enlarge more rapidly and produce earlier compression of the brainstem and fourth ventricle. Surgical excision is technically more challenging because facial nerve preservation is more difficult, resulting in comparatively poorer postoperative facial nerve outcomes. Large cystic vestibular schwannomas are generally considered less suitable for prolonged observation or stereotactic radiosurgery, and microsurgical excision is usually the preferred treatment.
Clinical Features
The clinical presentation of vestibular schwannoma is largely dependent on the size and location of the tumour. Early symptoms are often subtle and may be attributed to other conditions, leading to delays in diagnosis.
1. Vestibulocochlear Symptoms (Most common):
- Hearing Loss: The most common initial symptom of vestibular schwannoma is unilateral sensorineural hearing loss, which is typically slow and progressive. In some cases, however, hearing loss may occur suddenly. The hearing loss is often associated with a disproportionate decrease in speech discrimination ability compared to the degree of pure-tone hearing loss. In rare instances, patients may present with normal hearing despite the presence of a tumour. More than 90% of patients present with slowly progressive unilateral hearing loss with or without tinnitus. Sudden sensorineural hearing loss occurs in approximately 5–10% of patients.
- Tinnitus: Patients frequently experience high-pitched, continuous tinnitus in the affected ear. This symptom may be particularly bothersome in individuals with concurrent hearing loss.
- Vertigo and Imbalance: Patients may experience episodic vertigo or a sense of imbalance, particularly with head movements. However, because the contralateral vestibular system often compensates for the slow loss of vestibular function, symptoms may be mild or absent.
2. Cranial Nerve Involvement:
- Eighth Cranial Nerve: Tinnitus, hearing loss, and vestibular symptoms are indicative of eighth nerve involvement. Audiological testing typically reveals sensorineural hearing loss.
- Seventh Cranial Nerve (Facial Nerve): Sensory fibres of the facial nerve may be affected before the motor fibres, leading to hypesthesia (reduced sensation) or pain in the external auditory canal (Hitzelberger’s sign), loss of taste on the anterior two-thirds of the tongue, delayed blink reflex, and reduced lacrimation.
- Fifth Cranial Nerve (Trigeminal Nerve): Involvement of the trigeminal nerve is common in larger tumours, particularly those greater than 2.5 cm in diameter. Symptoms may include diminished corneal reflex, facial paraesthesia, and numbness. Muscle involvement is rare but possible in advanced cases.
- Other Cranial Nerves: Although less common, large vestibular schwannomas may affect additional cranial nerves, including the glossopharyngeal (IX), vagus (X), accessory (XI), and hypoglossal (XII) nerves, leading to dysphagia, nasal regurgitation, vocal changes, and other deficits. In rare cases, the oculomotor (III), trochlear (IV), and abducens (VI) nerves may also be involved.
3. Brainstem and Cerebellar Dysfunction:
- Large vestibular schwannomas may compress the brainstem, leading to symptoms such as ataxic gait, weakness, and sensory disturbances in the extremities, and exaggerated tendon reflexes.
- Cerebellar dysfunction may manifest as dysmetria (inability to control the distance, speed, and power of a movement), dysdiadochokinesia (inability to perform rapidly alternating movements), and ataxic gait. Patients may also have difficulty walking in a straight line and may tend to fall towards the side of the lesion.
4. Raised Intracranial Pressure:
- In advanced cases, the tumour may obstruct cerebrospinal fluid pathways, leading to hydrocephalus and raised intracranial pressure. Symptoms of increased intracranial pressure include headache, nausea, vomiting, diplopia (double vision), and papilledema (swelling of the optic disc).
Diagnosis and Investigations
Early diagnosis of vestibular schwannoma is crucial for optimal management and preservation of neurological function. A thorough evaluation of patients presenting with unilateral sensorineural hearing loss, tinnitus, or imbalance is necessary to detect the tumour at an early stage.
1. Audiological Tests:
- Pure Tone Audiometry (PTA): Asymmetrical sensorineural hearing loss, particularly in the high frequencies, with poor speech discrimination, is suggestive of vestibular schwannoma.
- Speech Audiometry: Disproportionate speech discrimination loss relative to pure-tone thresholds and the presence of a rollover phenomenon (decrease in discrimination score with increasing loudness) are indicative of retrocochlear pathology.
- Short Increment Sensitivity Index (SISI) test shows a retrocochlear type of lesion (score of 0–20%). Threshold tone decay test shows a retrocochlear type of lesion. Stapedial reflex delay present. It is not done routinely as more sensitive and specific tests are available. Recruitment phenomenon is absent as it is in cochlear lesions.
- Brainstem Auditory Evoked Response (BAER) or Auditory Brainstem Response (ABR): This test assesses the conduction of electrical impulses along the auditory nerve pathways. In vestibular schwannoma, there may be a prolonged latency in waves III and V, and an increased interpeak latency between waves I and V. However, this test is less sensitive for small tumours and is largely supplanted by MRI.
2. Imaging Studies:
- Magnetic Resonance Imaging (MRI): Magnetic resonance imaging (MRI) with gadolinium contrast is the gold standard investigation for vestibular schwannoma. MRI accurately demonstrates the size of the tumour, its intracanalicular and cerebellopontine angle components, and its relationship to adjacent neurovascular structures.
Typical MRI features include:
- Well-defined enhancing mass arising from the internal auditory canal
- Extension into the cerebellopontine angle in larger tumours
- Widening of the internal auditory canal
- Homogeneous enhancement in small tumours
- Heterogeneous enhancement with cystic degeneration in larger tumours
MRI with gadolinium contrast has nearly 100% sensitivity for detecting vestibular schwannomas larger than 2–3 mm and is the investigation of choice in all patients with unexplained unilateral audiovestibular symptoms.
- Computed Tomography (CT) Scan: CT scanning may be useful in certain situations, such as when MRI is contraindicated. CT can detect bone erosion or widening of the internal auditory canal, but it is less sensitive than MRI for detecting soft tissue tumors.
- Plain X-rays (transorbital, Stenver’s, Towne’s and submentovertical views). It can detect about 80% of tumours except for intracanalicular tumours.
- Vertebral angiography.
3. Vestibular Function Tests:
- Romberg Test: The patient may demonstrate a tendency to fall towards the side of the lesion when standing with feet together and eyes closed.
- Unterberger Step Test: The patient may rotate towards the side of the lesion when marching in place with eyes closed.
- Caloric Testing: There may be a diminished or absent response on caloric testing, indicating a loss of vestibular function on the affected side.
4. Neurological Examination: A detailed neurological examination should assess cranial nerve function, vestibular function, cerebellar function, and signs of brainstem involvement. Fundus is examined to see blurring of disc margins or papilloedema caused by raised intracranial pressure and optic nerve compression.
Treatment
The management of vestibular schwannoma depends on various factors, including tumour size, location, patient age, and overall health. Treatment options include observation, surgical resection, and radiation therapy.
1. Observation: Active Surveillance (Wait-and-Scan Policy): Active surveillance is an accepted management strategy for selected patients with vestibular schwannoma, particularly those with small tumours, minimal symptoms, advanced age, significant medical comorbidities, or preserved hearing.
Based on long-term natural history studies, a commonly recommended follow-up schedule consists of:
- Annual MRI for the first 5 years
- MRI every 2 years for the next 4 years
- One additional MRI after 5 years
Patients demonstrating significant tumour growth, progressive neurological symptoms, brainstem compression, or hydrocephalus should be considered for active treatment by microsurgery or stereotactic radiosurgery.
2. Stereotactic Radiosurgery (SRS): For small to medium-sized tumours, radiosurgery using Gamma Knife or CyberKnife can be effective in controlling tumour growth while minimising damage to surrounding tissues. SRS is particularly useful in patients who are not candidates for surgery. Cyberknife is more accurate. It uses real-time image guidance technology through computer-controlled robotics.
3. Surgical Resection: Surgical removal of the tumour is indicated in symptomatic patients or when the tumour shows significant growth on serial imaging. The surgical approach depends on the size of the tumour. The various surgical approaches to the cerebellopontine angle are:
- Translabyrinthine Approach: Most favoured approach. Early identification of the facial nerve and avoidance of cerebellar retraction or resection are its advantages. It involves the destruction of the inner ear and so is not an option for hearing preservation surgery. It has a higher incidence of cerebrospinal fluid (CSF) fistula than other approaches. Usually done in CPA tumours < 3 cm in size.
- Retrosigmoid (suboccipital) Approach: Preferred for the removal of all posterior fossa tumours, but particularly for large ones. But it gives a limited view of the internal auditory canal, and the chances of residual tumour are greater. Usually done in large CPA tumours> 3 cm in size.
- Middle Fossa Approach: The middle fossa approach is preferred in hearing preservation surgery and small intracanalicular tumours. However, the approach is somewhat cramped. Usually done in intracanalicular tumours < 1 cm in size.
- Combined translabyrinthine-suboccipital approach.
Although surgery has a role for those with large tumours (>3 cm maximal intracranial diameter), the role of stereotactic radiotherapy is considered minimal. For smaller tumours, a conservative approach is commonly advised.
4. Radiation Therapy: Fractionated stereotactic radiotherapy (FSRT) may be used for larger tumours or those in sensitive locations where surgery is risky. It involves delivering multiple small doses of radiation over several weeks. It can also be done in patients who are not willing to undergo surgery, have contraindications to surgery, or have a residual tumour. Radiotherapy arrests the growth (and hence avoids surgery) of the tumour and preserves auditory function.
Complications of surgery:
- 7th, 5th, 6th, 4th Cranial nerve palsy
- CSF fluid leakage (Otorrhea, Rhinorrhoea)
- Intracranial infection (Meningitis)
- Intraoperative bleeding
- Brain oedema
- Venous air embolism
- Cardiac arrhythmia
- Brain herniation
- Death, stroke, haemorrhage, brain injury
Differential Diagnosis
Acoustic neuroma should be differentiated from the other three most common cerebellopontine angle tumours, e.g. meningioma, primary cholesteatoma and arachnoidal cyst. One should also rule out Meniere’s disease.
Tumours of Cerebellopontine Angle:
- Acoustic neuroma
- Meningioma
- Epidermoid (cholesteatoma)
- Arachnoid cyst
- Schwannoma of other cranial nerves (e.g. CN V >VII > IX, X, XI)
- Aneurysm
- Glomus tumour
- Metastasis
———— End of the chapter ————
High-Yield Points for NEET PG & University Exams
- Vestibular schwannoma arises from Schwann cells of the inferior vestibular nerve (not cochlear nerve)
- Origin point: Obersteiner-Redlich zone (transition zone between central and peripheral myelin)
- Most common CPA tumour: Vestibular schwannoma (80-90% of all CPA tumours)
- Gold standard investigation: MRI with gadolinium contrast
- Most common symptom: Unilateral sensorineural hearing loss (>90%)
- NF2:Autosomal dominant, chromosome 22q12, bilateral vestibular schwannomas
- Bill’s bar: Vertical ridge separating facial nerve from superior vestibular nerve
- Hitzelberger’s sign: Hypesthesia or pain in external auditory canal (facial nerve sensory involvement)
- Rollover phenomenon: Decreased speech discrimination with increasing loudness (retrocochlear)
- Antoni A: Cellular, compact fibres with Verocay bodies
- Antoni B: Less cellular, loosely packed, spongy appearance
- Cystic vestibular schwannoma: 5-6% of cases, more rapid growth, poorer facial nerve outcomes
- Translabyrinthine approach: Most favoured, destroys hearing, early facial nerve identification
- Middle fossa approach: Best for hearing preservation, intracanalicular tumours (<1 cm)
- Retrosigmoid approach: Large tumours (>3 cm), hearing preservation possible
- Active surveillance: Annual MRI for 5 years, then every 2 years for 4 years
- Gamma Knife/CyberKnife: Effective for small to medium tumours (<3 cm)
- Growth rates: Slow 0.02 cm/year, Medium 0.20 cm/year, Fast 1.00 cm/year
- 70% of extrameatal tumours remain unchanged on follow-up
- Most common complication of surgery: Facial nerve palsy
Clinical Pearls for Viva
How to present a case of vestibular schwannoma:
“This patient presents with right-sided progressive hearing loss, tinnitus, and imbalance. On examination, there is evidence of unilateral sensorineural hearing loss. MRI with gadolinium shows a well-defined enhancing mass arising from the right internal auditory canal with extension into the cerebellopontine angle. The differential diagnoses include meningioma and epidermoid cyst. The management options are active surveillance, stereotactic radiosurgery, or surgical resection depending on tumour size and patient factors.”
Common viva questions:
- What is the most common CPA tumour? (Vestibular schwannoma)
- Which nerve does vestibular schwannoma arise from? (Inferior vestibular nerve)
- What is the role of MRI in diagnosis? (Gold standard, shows enhancing mass)
- What are the surgical approaches and their indications? (Translabyrinthine <3 cm, Retrosigmoid >3 cm, Middle fossa <1 cm for hearing preservation)
- What is the difference between neurofibromatosis type 1 and type 2? (NF2 has bilateral vestibular schwannomas, NF1 has neurofibromas)
- What is the rollover phenomenon? (Decreased speech discrimination with increasing loudness)
- What are the prognostic factors? (Tumour size, patient age, hearing status)
NEET PG-Style MCQs
1: The most common tumour of the cerebellopontine angle is: A. Meningioma B. Epidermoid cyst C. Vestibular schwannoma D. Arachnoid cyst.
2: Vestibular schwannoma most commonly arises from: A. Cochlear nerve B. Superior vestibular nerve C. Inferior vestibular nerve D. Facial nerve.
3: The gold standard investigation for diagnosing vestibular schwannoma is: A. CT scan B. MRI with gadolinium C. BAER D. Caloric testing.
4: The most common initial symptom of vestibular schwannoma is: A. Tinnitus B. Vertigo C. Unilateral sensorineural hearing loss D. Facial numbness.
5: The transition zone where vestibular schwannoma commonly originates is called: A. Bill’s bar B. Crista falciformis C. Obersteiner-Redlich zone D. Porus acousticus.
6: The vertical bony ridge separating the facial nerve from the superior vestibular nerve is: A. Crista falciformis B. Bill’s bar C. Trautmann’s triangle D. MacEwen’s triangle.
7: The following is NOT a feature of Neurofibromatosis Type 2: A. Bilateral vestibular schwannomas B. Meningiomas C. Neurofibromas D. Ependymomas.
8: The rollover phenomenon on speech audiometry indicates: A. Cochlear pathology B. Retrocochlear pathology C. Conductive hearing loss D. Normal hearing.
9: The surgical approach that best preserves hearing is: A. Translabyrinthine B. Retrosigmoid C. Middle fossa D. Combined approach.
10: The translabyrinthine approach is contraindicated when: A. Tumour is >3 cm B. Hearing preservation is desired C. Facial nerve preservation is desired D. CSF leak is a concern.
MCQs Answers: 1: C. 2: C. 3: B. 4: C. 5: C. 6: B. 7: C. 8: B. 9: C. 10: B.
Clinical Case Scenarios for Practical Exams & Viva
- Case 1.A 55-year-old female presents with progressive right-sided hearing loss and tinnitus for the past 2 years. She also complains of occasional imbalance but denies vertigo. Pure tone audiometry shows asymmetrical sensorineural hearing loss in the right ear with poor speech discrimination. Most likely diagnosis: Vestibular schwannoma. Best investigation: MRI with gadolinium contrast. Best management depends on tumour size: observation for small asymptomatic tumours, radiosurgery for 1.5-3 cm tumours, and surgical resection for large tumours (>3 cm).
- Case 2.A 35-year-old male with known Neurofibromatosis Type 2 presents with bilateral hearing loss, headache, and ataxia. MRI shows bilateral enhancing masses in both internal auditory canals with extension into the cerebellopontine angles. Most likely diagnosis: Bilateral vestibular schwannomas in NF2. Best management: Multidisciplinary approach with genetic counselling; consider hearing preservation surgery on the better hearing side and radiosurgery on the contralateral side; tumour growth rate monitoring is essential.
- Case 3.A 60-year-old diabetic patient with a 2 cm vestibular schwannoma and good hearing in the affected ear is being counselled for management. The patient is keen to preserve hearing and avoid major surgery. Most likely diagnosis: Small vestibular schwannoma with serviceable hearing. Best management: Stereotactic radiosurgery (Gamma Knife) offers tumour control with hearing preservation; alternatively, active surveillance if the patient prefers no intervention. Surgical resection would risk hearing loss.
- Case 4.A 45-year-old woman presents with right-sided hearing loss, facial numbness, and difficulty walking. MRI reveals a 4 cm enhancing mass in the right cerebellopontine angle causing brainstem compression. Most likely diagnosis: Large vestibular schwannoma with brainstem compression. Best management: Urgent surgical resection via retrosigmoid approach; monitor for hydrocephalus and raised intracranial pressure; postoperative facial nerve function may be compromised due to the large tumour size.
Frequently Asked Questions in Viva
- Q: What is the difference between acoustic neuroma and vestibular schwannoma?
A: Acoustic neuroma is a misnomer because the tumour arises from the vestibular nerve, not the acoustic (cochlear) nerve. Vestibular schwannoma is the correct and preferred term. - Q: What is Neurofibromatosis Type 2 and how does it relate to vestibular schwannoma?
A:NF2 is an autosomal dominant disorder caused by mutation of the NF2 gene on chromosome 22q12. It is characterised by bilateral vestibular schwannomas, which are the hallmark feature, along with other intracranial and spinal tumours like meningiomas and ependymomas. - Q: What is the role of MRI in diagnosing vestibular schwannoma?
A: MRI with gadolinium contrast is the gold standard investigation. It shows a well-defined enhancing mass arising from the IAC, with homogeneous enhancement in small tumours and heterogeneous enhancement in larger ones. It has nearly 100% sensitivity for tumours >2-3 mm. - Q: What is the treatment algorithm for vestibular schwannoma?
A: Treatment depends on tumour size, patient age, hearing status, and symptoms. Observation is preferred for small asymptomatic tumours; radiosurgery is suitable for 1.5-3 cm tumours with preserved hearing; surgical resection is indicated for large tumours (>3 cm) or those with brainstem compression. - Q: What is the best surgical approach for hearing preservation?
A: The middle fossa approach provides the best hearing preservation rates because it allows access to the internal auditory canal without destroying inner ear structures. It is ideal for small intracanalicular tumours. - Q: What are the common complications of vestibular schwannoma surgery?
A: Facial nerve palsy is the most common complication. Other complications include CSF leakage, meningitis, hearing loss, brain oedema, and rarely death. The risk of complications increases with larger tumour size. - Q: What is the role of stereotactic radiosurgery in vestibular schwannoma?
A:Gamma Knife or CyberKnife radiosurgery is effective for controlling tumour growth in small to medium-sized tumours (<3 cm). It is particularly useful in patients who are not candidates for surgery or who wish to avoid surgery, with hearing preservation rates being reasonable.
———— End ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords:Earliest nerve involved in acoustic neuroma, Surgery to remove the tumor, Large tumors, Tumor grows, Hearing loss in one ear, Symptoms of the eighth cranial nerve, Brain tumor, Ear to the brain, Vestibular schwannoma, Acoustic neuroma surgery, Acoustic neuroma MRI, Acoustic neuroma Treatment, Brain tumour symptoms, Obersteiner-Redlich zone, Neurofibromatosis Type 2, Gamma Knife or CyberKnife, Acoustic neuroma, Vestibular schwannoma, Hitzelberger’s sign, Antoni A & B fibers
Hai
The pdf download option is not available
Please enable it to download