Diseases of the Nasal Septum
The nasal septum forms the central partition of the nasal cavity and divides it into right and left nasal passages. Structurally, it consists of septal cartilage anteriorly, the perpendicular plate of the ethmoid superiorly, and the vomer inferiorly and posteriorly. Functionally, it maintains laminar airflow, supports the nasal dorsum, and contributes to humidification and filtration of inspired air. Therefore, even minor septal pathology can significantly affect nasal breathing, sinus ventilation, and facial contour. Read more on: 🔗Anatomy of Nasal Septum

Diseases of the nasal septum are commonly present in outpatient ENT practice and frequently appear in university theory examinations, practical examinations, viva voce, and NEET PG multiple-choice questions. Among these, Deviated Nasal Septum (DNS), septal hematoma, and septal perforation represent the most clinically important and exam-relevant conditions.
Deviated Nasal Septum (DNS)
Definition. A deviated nasal septum refers to the displacement of the septum from the midline, resulting in asymmetry between the two nasal cavities. Consequently, it causes major nasal obstruction. Although minor deviations occur in a large proportion of the population, only symptomatic deviation requires clinical attention. Therefore, the presence of deviation alone does not justify surgery; symptoms guide management.
Causes
1.Developmental / Racial Causes
- During growth, disproportionate development between the septum and surrounding facial bones may cause bending or buckling.
- Genetic predisposition. A family history of DNS can sometimes be elicited.
2. Trauma
- Childhood injury. In many adults, the deviation originates from childhood trauma, although patients often fail to recall such injury. Thus, when you evaluate a patient with DNS, always enquire about childhood injury, even if the patient initially denies trauma.
- Accidental trauma. Such as falls, sports injuries, road traffic accidents, or physical assault, also contribute significantly.
- Birth trauma. During prolonged labour, the nasal cartilage may be compressed and lead to later deviation.
Types of Septal Deviation (Morphological Classification)

Septal deviation presents in characteristic patterns.
- C-shaped deviation is the most common type. In this condition, the septum bends to one side forming a single curve. The nasal cavity on the concave side becomes wider. As a result, the turbinate on that side may enlarge to compensate, which is called compensatory hypertrophy.
- S-shaped deviation shows double curvature. The septum bends in two opposite directions. This deformity may occur in the vertical plane or in the anteroposterior plane. Since both nasal cavities become narrow at different levels, the patient may develop bilateral nasal obstruction.
- Septal spur is a sharp projection usually seen at the junction of cartilage and bone. The spur may press against the lateral nasal wall. Because of this pressure, the patient may complain of nasal obstruction, recurrent epistaxis, or even headache.
- Septal thickening refers to localized enlargement of the septum. This thickening may occur due to an organized hematoma or overlapping of fractured septal fragments after trauma.
- Caudal dislocation means forward displacement of the lower end of the septum into one nasal cavity. This type is commonly visible on anterior rhinoscopy and may cause visible nasal deformity.
In practical examinations, examiners commonly ask you to identify the type of deviation on anterior rhinoscopy. Therefore, always describe the direction, location, and extent of deviation clearly.
Clinical Features
- Nasal Obstruction. This is the most common symptom. It may be unilateral or bilateral, depending on the severity and type of deviation. High septal deviations cause more obstruction than low ones because airflow mainly passes through the upper nasal cavity. Importantly, constant obstruction usually indicates structural blockage, such as DNS. In contrast, intermittent obstruction suggests mucosal causes such as turbinate hypertrophy or allergic rhinitis. When obstruction changes sides periodically, the nasal cycle likely explains the symptom. Decongestant Test. A simple bedside method helps differentiate structural from mucosal causes. After applying a topical nasal decongestant, if obstruction improves significantly, mucosal elements contribute to the blockage. However, if no improvement occurs, anatomical deviation likely predominates. This clinical reasoning often appears in NEET PG MCQs.
- Epistaxis. Patients, especially those with a septal spur, may develop recurrent nosebleeds. The spur stretches and thins the mucosa, leading to crust formation. When the crust is removed, bleeding occurs.
- Headache. A deviated septum may touch the turbinate and stimulate the anterior ethmoidal nerve. This contact produces headache, sometimes referred to as Sluder’s neuralgia.
- Recurrent Sinusitis. DNS may block sinus openings and interfere with normal drainage and ventilation. As a result, patients may experience recurrent sinus infections.
- Anosmia or Hyposmia. Severe deviation may prevent inspired air from reaching the olfactory area, leading to partial or complete loss of smell.
- External nasal deformity. Significant septal deformity may be associated with deviation of the nasal dorsum, tip, or columella, producing visible cosmetic deformity.
- Predisposition to Middle ear infection. Chronic nasal obstruction may affect Eustachian tube function and increase the risk of otitis media, especially in children.
Examination and Diagnosis
- Anterior Rhinoscopy. It allows direct visualisation of deviation (identify type, site, and direction of deviation), spur, thickening, or caudal dislocation. However, posterior deviations and associated conditions require diagnostic nasal endoscopy. Always perform this before and after decongestion to assess the mucosal component.
- Diagnostic Nasal Endoscopy (DNE). Endoscopy also helps detect polyps, turbinate hypertrophy, sinus disease, or adenoid enlargement. When examining a patient with nasal obstruction, always identify the exact site of obstruction. It may occur at the vestibule, nasal valve, attic region (upper septum), turbinate region, or choana. Posterior causes, such as a choanal polyp, may be missed without endoscopy.
- CT Scan (PNS). Not routine but used for complex cases, sinusitis, or pre-op planning. Shows the relationship of the deviation to the sinuses. Ordered by the surgeon; not a first-line diagnostic test.
- Cottle’s test evaluates the internal nasal valve. When you gently pull the cheek laterally and upwards, the nasal valve area widens. If airflow improves, the test is positive and indicates obstruction at the level of the internal nasal valve. This area offers maximum resistance to airflow and therefore plays a crucial role in nasal physiology.

Grading and Clinical Significance
Clinical grading. Septal deviation can be clinically categorised into simple, obstructed, and impacted types.
- Simple deviation produces no symptoms.
- Obstructed deviation causes symptoms but improves with decongestants, suggesting a mucosal component.
- Impacted deviation impinges on the lateral nasal wall and does not improve with decongestants, indicating a purely structural problem.
Mladina’s Classification. Mladina classified septal deformities into seven types based on rhinoscopic or radiological findings. These include mild vertical deviation (Type I), anterior vertical deviation (Type II), posterior vertical deviation (Type III), S-shaped deformity (Type IV), horizontal crest (Type V), maxillary crest deformity (Type VI), and combination deformities (Type VII).
Management
Management depends entirely on symptoms. Asymptomatic deviation requires no treatment. However, symptomatic cases require surgical correction. 🔗Septoplasty remains the preferred procedure because it preserves the septal framework while correcting deviation. In contrast, 🔗Submucosal resection (SMR) removes larger portions of cartilage and bone and therefore carries a greater risk of complications such as septal perforation or saddle nose deformity. Modern practice strongly favours septoplasty over SMR.
Table: Differences between Septoplasty and Submucosal Resection
|
Feature |
Septoplasty (The Modern Choice) |
Submucosal Resection (SMR) (Historical) |
|
Principal |
Preserve and Reconstruct. Only the deviated parts are removed, reshaped, or repositioned. |
Resect and Remove. Most of the quadrangular cartilage and bone are removed. |
|
Cartilage Removal |
Minimal. The L-strut (dorsal and caudal strip) is always preserved for support. |
Extensive. The central part of the cartilage is removed, leaving only a dorsal and caudal rim. |
|
Indications |
Almost all cases of DNS in adults and children. |
Obsolete for routine cases. Occasionally used for very severe deformities or access. |
|
Complications |
Low risk of perforation or saddle nose. |
High risk of septal perforation and saddle nose deformity due to loss of support. |
High-Yield Surgical Tip: In septoplasty, preserving an L-strut of cartilage (a 1-1.5cm strip along the dorsal and caudal border) is vital to maintain nasal dorsum and tip support.
Septal Hematoma and Abscess
Definition:
Septal hematoma refers to a collection of blood between the septal cartilage and its overlying mucoperichondrium. This condition constitutes an ENT emergency because delayed treatment may result in cartilage necrosis, septal abscess, and permanent nasal deformity (saddle nose).
Pathophysiology
The septal cartilage derives its nutrition entirely from the overlying perichondrium. During trauma, submucosal vessels rupture and blood accumulates between cartilage and mucoperichondrium. As separation persists, cartilage loses blood supply and undergoes ischemic necrosis within 24-72 hours. Moreover, stagnant blood provides an excellent medium for bacterial growth, which may lead to a septal abscess. Therefore, early recognition and drainage are essential to prevent complications.
Etiology
- Trauma (Most common). Sports injuries, roadside accidents, falls, and assault.
- Iatrogenic. After septoplasty, Submucous resection (SMR), Functional endoscopic sinus surgery (FESS)
- Atraumatic (Less common). Bleeding disorders, Anticoagulant therapy, Spontaneous vascular rupture.
Clinical Presentation.
Patients usually present soon after nasal trauma.
Symptoms
- Bilateral nasal obstruction (most common symptom)
- Nasal pain
- Frontal headache
- Pressure over the nasal bridge
- Rhinorrhoea
- Fever (if infection develops)
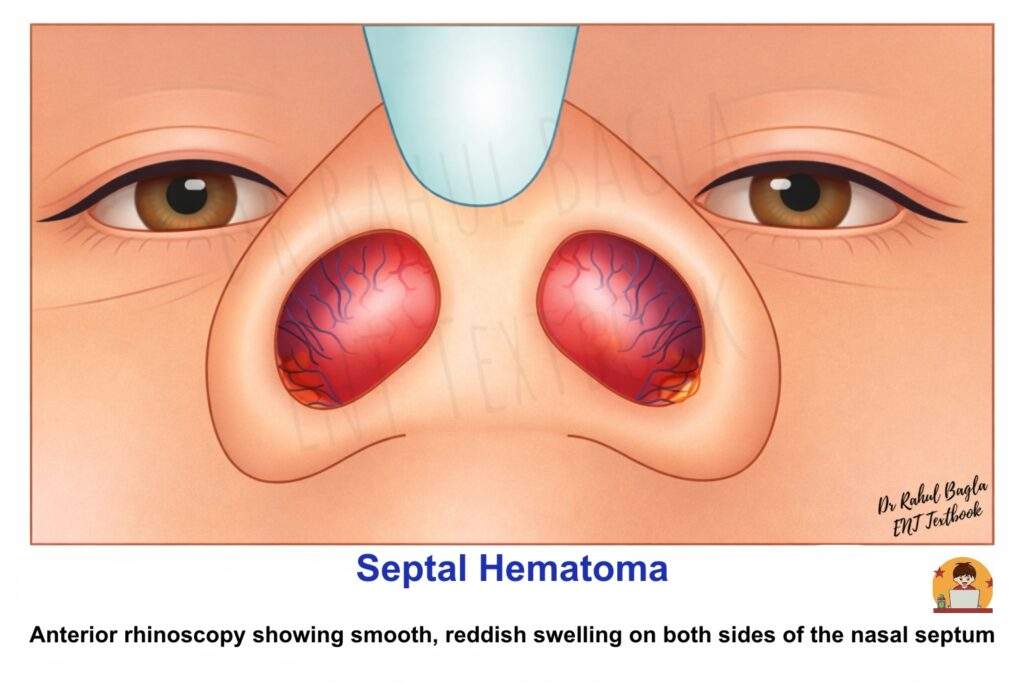
Signs (Anterior Rhinoscopy). Typical findings include:
- Smooth, reddish swelling on both sides of the nasal septum
- Fluctuant swelling
- Swelling obliterates the nasal cavity
Key examination point: Septal hematoma usually presents as bilateral swelling, which helps differentiate it from a deviated nasal septum (DNS). Viva tip: “Septal hematoma appears as a bilateral soft fluctuant swelling of the septum and requires urgent drainage.”
Management.
Septal hematoma requires urgent treatment to prevent cartilage necrosis.
- Aspiration: Small hematomas can be managed by aspiration using a wide-bore sterile needle
- Incision and Drainage (Preferred): Larger haematomas are incised and drained by a small anteroposterior incision parallel to the nasal floor. Excision of a small piece of mucosa from the edge of the incision gives better drainage.
- Prevention of Recollection: After drainage, bilateral nasal packing is done, or Quilting sutures (through-and-through absorbable sutures that hold the flaps together) are applied to approximate the mucoperichondrium to cartilage.
- Antibiotics: Broad-spectrum systemic antibiotics are given to prevent infection and septal abscess.
Complications of Untreated Hematoma
If not treated early, several serious complications may occur.
- Local Complications: Septal abscess, Septal perforation, Saddle nose deformity, Nasal valve collapse, Sinusitis, Nasal vestibulitis, Facial cellulitis
- Systemic Complication: Sepsis
- Orbital Complications: Subperiosteal abscess, Orbital cellulitis, Orbital abscess
- Intracranial Complication: Cavernous sinus thrombosis
Septal Perforation
Definition
A septal perforation is a defect or hole in the nasal septum that allows communication between the two nasal cavities. The perforation usually occurs due to trauma, infection, inflammatory diseases, or iatrogenic causes. Small perforations may remain asymptomatic, whereas larger perforations often produce crusting, epistaxis, and a whistling sound during breathing.
Aetiology (Causes) of Septal Perforation
- Traumatic Causes. Nasal surgery (septoplasty, SMR), Habitual nose picking (digital trauma), Septal hematoma or septal abscess, Bilateral septal cauterisation, Cryosurgery, Nasal packing for epistaxis, Nasogastric or endotracheal intubation, Nasal foreign bodies (especially button batteries)
- Chemical Irritants. Cocaine snuff, Heroin inhalation, Overuse of decongestant nasal sprays, Intranasal corticosteroids, Occupational exposure: copper, chromic acid, sulphuric acid, arsenic, mercury, cement, glass dust, salt or lime dust
- Infectious Causes. Tuberculosis, Leprosy, Syphilis, Rhinoscleroma, Mucormycosis, Rhinosporidiosis, Aspergillosis, Histoplasmosis, Leishmaniasis, Cryptococcosis, Nasal myiasis
- Neoplasms. Adenocarcinoma, Melanoma, Lymphoma
- Chronic Granulomatous Diseases. Relapsing polychondritis, Granulomatosis with polyangiitis (Wegener’s granulomatosis), Systemic lupus erythematosus, Sarcoidosis, Rheumatoid arthritis, Atrophic rhinitis
Clinical Features
The symptoms of septal perforation vary depending on the size, location, and underlying cause of the perforation. Small perforations often produce more noticeable airflow disturbances, while large perforations mainly cause dryness and crusting.
Symptoms
- Crusting inside the nose (most common). Drying of nasal secretions leads to crust formation around the edges of the perforation.
- Epistaxis. Recurrent nasal bleeding occurs due to fragile mucosa and trauma during the removal of crusts.
- Whistling sound during breathing. Characteristically seen in small perforations, where air passing through the narrow defect produces a whistling noise.
- Nasal obstruction. Usually caused by crusts accumulating around the margins of the perforation.
- Recurrent bleeding after crust removal. Patients often remove crusts manually, leading to repeated trauma and bleeding.
- Dryness and nasal irritation. More common in large perforations due to excessive airflow and mucosal drying.
Clinical Examination
A detailed history and physical examination are essential to identify the cause, size, and extent of the perforation.
History. Important points include:
- History of nasal surgery (septoplasty or SMR)
- Habitual nose picking
- Use of intranasal drugs or decongestant sprays
- Occupational chemical exposure
- History of systemic diseases or infections affecting the nose
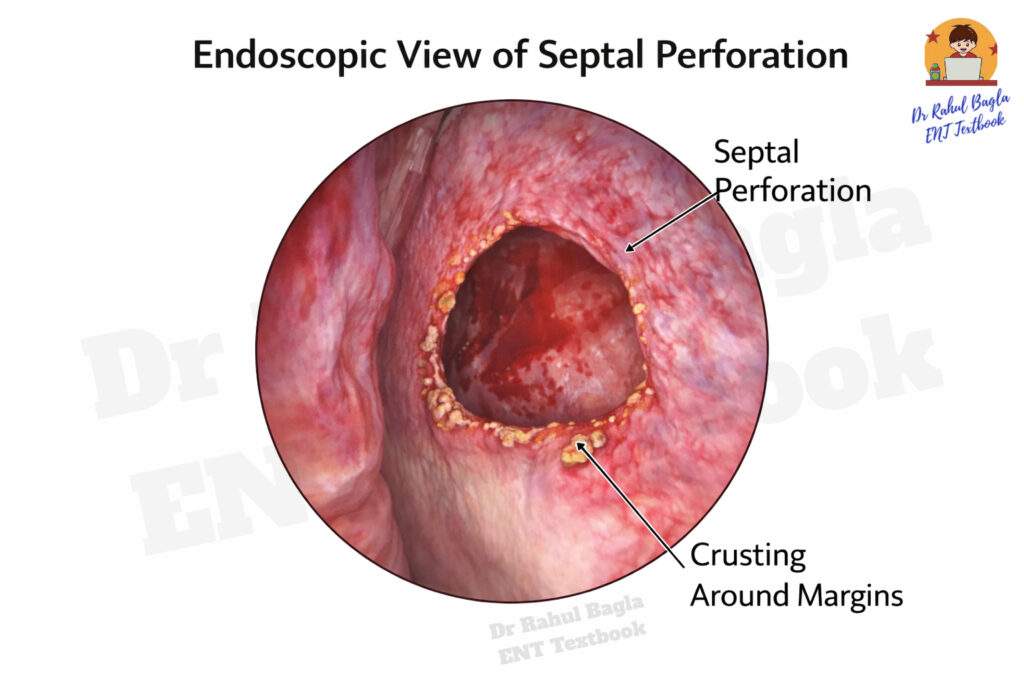
Anterior Rhinoscopy. The perforation appears as a round or oval defect in the nasal septum with surrounding crusting.
Nasal Endoscopy. Nasal endoscopy provides a better assessment of the lesion, especially when the perforation is located posteriorly. It helps to:
- Visualize posterior septal perforations
- Determine the exact size and shape
- Assess margins of the perforation
- Identify crusting, infection, or granulation tissue
Classification Based on Size. Septal perforations are commonly classified according to their diameter, which helps guide management.
- Small – Less than 0.5 cm
- Medium – 0.5 – 2 cm
- Large – Greater than 2 cm
Management
The treatment of septal perforation depends on the presence or absence of symptoms, the size of the perforation, the underlying cause, & general condition of the patient
1. Prevention. Prevention is the most important aspect of management, especially after nasal surgery. Preventive measures include:
- Using careful surgical technique during septoplasty or SMR
- Avoiding bilateral mucosal injury
- Early detection and treatment of septal hematoma or septal abscess
2. No Treatment (Observation). Small, asymptomatic perforations may not require active treatment. These cases can be managed with observation and periodic follow-up.
3. Conservative (Nonsurgical) Treatment. Conservative treatment is aimed at relieving symptoms, particularly crusting and bleeding.
- Saline nasal sprays. Keep the nasal mucosa moist and reduce dryness.
- Alkaline nasal douches. Help soften and remove crusts.
- Lubricating nasal ointments. Prevent mucosal dryness and irritation.
4. Septal Button. A septal button is a prosthetic device usually made of silicone material that mechanically closes the perforation.
Advantages
- Prevents the drying effect of airflow
- Reduces whistling sound
- Decreases epistaxis
- Promotes epithelialization of the margins
It is particularly useful in patients unsuitable for surgery.
- Surgical Treatment. Surgery is indicated in symptomatic perforations, especially when conservative treatment fails.
- Enlargement of the Perforation. In some very small perforations, surgical enlargement may eliminate the whistling sound, reduce turbulent airflow, & Improve crusting
- Surgical Repair. The aim of surgery is closure of the perforation and restoration of normal nasal physiology. Two main approaches are used:
- Closed technique. Performed through the nasal cavity, often with endoscopic assistance.
- Open technique. Performed using an external rhinoplasty approach, allowing better exposure for large perforations.
Repair is achieved using local nasal mucosal flaps, mucoperichondrial or mucoperiosteal flaps, and autografts such as temporalis fascia
——– End of the chapter——–
High-Yield Points for NEET PG & University Exams
- Most common cause of septal perforation: Iatrogenic (previous septal surgery).
- Complication of untreated septal hematoma: Saddle nose deformity.
- Decongestant test: Differentiates anatomical (DNS) from mucosal (turbinate hypertrophy) obstruction.
- Cartilage preservation is key: This is the main difference between septoplasty (preserves L-strut) and SMR (resects widely).
- Whistling: Characteristic of a small, anterior septal perforation.
- Saddle Nose Deformity: Caused by loss of septal support (from trauma, abscess, or over-resection in SMR).
- Bilateral nasal obstruction + history of trauma: Think of septal hematoma.
Clinical Case Scenarios for Practical/Viva
Scenario 1: The Trauma Patient
A 25-year-old male presents to the casualty department 2 days after a fistfight. He complains of severe bilateral nasal obstruction and pain. On examination, his nose is tender, and anterior rhinoscopy reveals a smooth, reddish-blue, fluctuant swelling on both sides of the septum, completely occluding both nasal cavities.
- Q1: What is the most likely diagnosis? A: Septal hematoma.
- Q2: Why is this an emergency? A: The septal cartilage is avascular and depends on the perichondrium for nutrition. The hematoma strips the perichondrium, leading to avascular necrosis of the cartilage within 72 hours. If infected, it can lead to a septal abscess and intracranial complications.
- Q3: How will you manage this patient? A: Immediate incision and drainage under local or general anaesthesia, followed by quilting sutures or bilateral nasal packing to prevent re-accumulation, and broad-spectrum antibiotics.
Scenario 2: The Crooked Nose
A 30-year-old female presents with difficulty breathing through her nose, especially on the right side, a problem she’s had for years. She also gets frequent headaches and occasional nosebleeds from the right side. On examination, you see a sharp, shelf-like projection from the septum pressing against the right inferior turbinate. The left nasal cavity is roomy.
- Q1: What is the likely finding on anterior rhinoscopy? A: A right-sided septal spur.
- Q2: What test will you do to confirm the cause of obstruction? A: A decongestant test. If the obstruction persists after spraying a decongestant, it confirms the obstruction is primarily anatomical (the spur).
- Q3: What is the definitive management? A: Septoplasty with spur excision.
Scenario 3: The Whistling Nose
A 45-year-old man with a history of nasal surgery 10 years ago complains of a persistent whistling sound when he breathes. He also reports nasal dryness and occasional bleeding when he picks his nose.
- Q1: What is the most likely diagnosis? A: A small, anterior septal perforation.
- Q2: What is the most common cause in this patient? A: Iatrogenic from his previous nasal surgery (likely SMR).
- Q3: What is the first line of management for his symptoms? A: Conservative treatment with saline nasal sprays and lubricating ointments to reduce crusting. A silicone septal button could also be offered.
NEET PG-Style MCQs
1. A 10-year-old boy presents with bilateral nasal obstruction and low-grade fever, 5 days after being hit on the nose by a cricket ball. Anterior rhinoscopy reveals a bilateral, smooth, reddish swelling of the nasal septum. Which of the following is the most appropriate next step in management?
a) Prescribe a course of oral antibiotics and review in 1 week.
b) Apply a nasal decongestant spray and review in 2 days.
c) Perform an immediate incision and drainage.
d) Order a CT scan of the paranasal sinuses.
2. Which of the following is a characteristic symptom of a small, anterior septal perforation?
a) Saddle nose deformity
b) Bilateral nasal obstruction
c) Whistling sound during breathing
d) Anosmia
3. The single most important step in the surgical management of a Deviated Nasal Septum (Septoplasty) is to preserve the:
a) Vomer bone
b) Perpendicular plate of ethmoid
c) Entire quadrangular cartilage
d) L-strut of cartilage
4. A patient presents with recurrent epistaxis and a deviated nasal septum with a sharp projection. The most likely type of deviation is:
a) C-shaped deviation
b) S-shaped deviation
c) Septal spur
d) Caudal dislocation
5. An untreated septal hematoma is most likely to lead to which of the following deformities?
a) Tension pneumocephalus
b) Saddle nose deformity
c) Adenoid facies
d) Polyps
6. Cottle’s test is used to assess the patency of the:
a) Osteomeatal complex
b) Sphenoethmoidal recess
c) Internal nasal valve
d) Choana
7. A 50-year-old male with a history of chronic cocaine use presents with nasal crusting and a foul smell. On examination, he has a large septal perforation. What is the most important investigation to order next?
a) Fungal culture
b) Biopsy from the edge of the perforation
c) Serum ACE levels
d) Sweat chloride test
8. The primary advantage of septoplasty over submucous resection (SMR) is:
a) It is a faster procedure
b) It preserves the septal cartilage to prevent nasal deformity
c) It can be done under local anesthesia
d) It has a lower chance of post-operative bleeding
9. Which of the following is NOT a typical causative organism in a septal abscess?
a) Staphylococcus aureus
b) Streptococcus pneumoniae
c) Pseudomonas aeruginosa
d) Haemophilus influenzae
10. A patient’s nasal obstruction due to a deviated septum does NOT improve after applying a topical decongestant. This suggests that the obstruction is primarily due to:
a) Allergic rhinitis
b) Compensatory turbinate hypertrophy
c) The nasal cycle
d) A fixed anatomical deviation
Answers and Explanations
- (c) Perform an immediate incision and drainage. The presentation is classic for a post-traumatic septal hematoma, which is an emergency requiring immediate drainage.
- (c) Whistling sound during breathing. Small anterior perforations cause turbulent airflow, resulting in a whistle. Large perforations cause crusting.
- (d) L-strut of cartilage. Preserving the dorsal and caudal L-strut is essential to maintain nasal dorsum height and tip support, preventing a saddle nose deformity.
- (c) Septal spur. A sharp, thorn-like projection is the definition of a septal spur, which is prone to causing epistaxis by stretching the overlying mucosa.
- (b) Saddle nose deformity. Ischemic necrosis of the septal cartilage from an untreated hematoma leads to loss of dorsal support, resulting in a saddle nose deformity.
- (c) Internal nasal valve. Cottle’s test involves laterally retracting the cheek to open the internal nasal valve area and assess its contribution to nasal obstruction.
- (b) Biopsy from the edge of the perforation. While cocaine use is a known cause, it is crucial to rule out malignancy (e.g., squamous cell carcinoma) and vasculitis (e.g., GPA) with a biopsy.
- (b) It preserves the septal cartilage to prevent nasal deformity. Septoplasty is a cartilage-preserving procedure, while SMR removes cartilage, leading to a higher risk of complications like perforation and saddle nose.
- (c) Pseudomonas aeruginosa. The most common pathogens in a septal abscess are S. aureus, S. pneumoniae, H. influenzae, and anaerobes. Pseudomonas is less common in this specific context.
- (d) A fixed anatomical deviation. The decongestant test helps differentiate mucosal (reversible) from structural (fixed) causes of obstruction. No improvement points to a fixed anatomical problem like DNS.
Frequently Asked Questions in Viva
- What is the main difference between septoplasty and SMR?
Septoplasty is a cartilage-preserving surgery that only removes the deviated parts while maintaining an L-strut for support. SMR is an older, more radical procedure that removes most of the septal cartilage, leading to a higher risk of complications like septal perforation and saddle nose deformity. - Why is a septal hematoma considered an emergency?
The nasal septum cartilage is avascular and receives its nutrition solely from the overlying perichondrium. A hematoma separates the perichondrium from the cartilage, causing ischemic necrosis of the cartilage within days. This can lead to permanent deformity (saddle nose) and life-threatening intracranial infections if it forms an abscess. - What causes a whistling sound from the nose?
A whistling sound is typically caused by a small, anterior septal perforation. As air rushes through this narrow, abnormal opening, it creates turbulent airflow that produces an audible whistle. - How do you differentiate a deviated nasal septum from turbinate hypertrophy?
A simple bedside test called the decongestant test is used. After applying a topical decongestant spray, if the nasal obstruction significantly improves, the cause is mainly mucosal swelling (turbinate hypertrophy). If there is little to no improvement, the obstruction is likely due to a fixed anatomical deviation like DNS. - Can a deviated nasal septum cause headaches?
Yes, this is known as a rhinogenic headache. When the deviated part of the septum (like a spur) presses against the lateral nasal wall (turbinates), it can stimulate the sensory nerves, leading to a reflex headache. Septal surgery often resolves this type of headache.
——– End——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Deviated nasal septum notes for MBBS students, DNS causes symptoms and management summary, Septal hematoma emergency treatment ENT guide, Septal perforation causes and surgical repair notes, ENT nasal septum diseases CBME curriculum chapter, NEET PG MCQs on deviated nasal septum with answers and explanations, Cottle test clinical significance in nasal obstruction, Septoplasty versus SMR difference for exams, Saddle nose deformity causes and management ENT notes, Nasal obstruction differential diagnosis ENT exam revision guide, Deviated Nasal Septum notes, DNS etiology MBBS, Septal hematoma management, Septal perforation causes NEET PG, Nasal septum diseases CBME, DNS clinical features revision, Septal spur symptoms, Cottle test explanation, Septoplasty indications exam guide, Mladina classification DNS, NASAL mnemonic DNS symptoms, Septal abscess complications, ENT nasal septum MCQs, High yield points nasal septum, Septal perforation treatment summary, DNS grading for viva, CBME ENT nasal septum competencies, NEET PG DNS questions, Septal diseases practical exam tips, Nasal septum flowchart diagnosis.
very nice, loved it fullly