|
The following CBME core competencies are covered in this chapter.
|
Disorders of Tympanic Membrane
Introduction
The tympanic membrane (TM) is a thin, semi-transparent membrane that separates the external auditory canal from the middle ear cleft. It plays a major role in sound conduction, middle ear protection, and pressure regulation. However, the TM is not just a hearing structure. It is also a mirror of middle ear disease, because many middle ear pathologies first present as TM changes. Common symptoms include otalgia, ear discharge, hearing loss, tinnitus, and ear fullness.
Normal Tympanic Membrane:
- Pearly grey
- Semi-transparent
- Cone of light present
- Handle of malleus visible
- Pars tensa and pars flaccida identifiable
Clinical rule: If the TM looks abnormal, always think of middle ear pathology, unless proven otherwise.
Table: Classification of Tympanic Membrane Disorders
| Category | Disorders Included |
| 1. Inflammatory disorders | Acute bullous myringitis Granular chronic myringitis |
| 2. Structural and degenerative disorders | Retraction and retraction pockets Atelectasis Atrophic tympanic membrane Tympanosclerosis |
| 3. Perforations of tympanic membrane | Central perforation Marginal perforation Attic perforation |
| 4. Traumatic disorders | Traumatic perforation (blunt, penetrating, barotrauma) |
Inflammatory Disorders of Tympanic Membrane
Myringitis
Definition: Inflammation of the tympanic membrane.
Types:
- Acute bullous myringitis
- Granular chronic myringitis
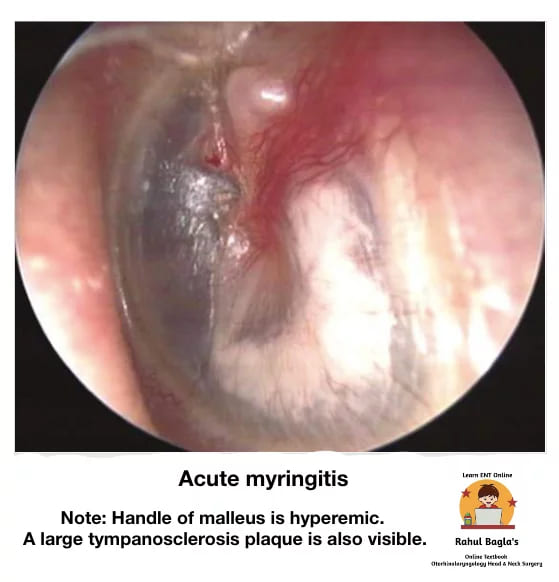
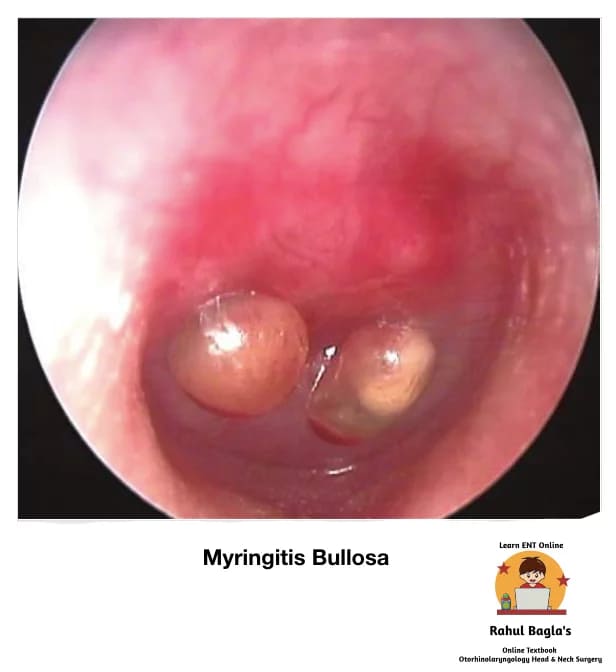
Acute Bullous Myringitis
Definition: It is an acute, painful inflammatory condition characterised by single or multiple bullae or vesicles on the tympanic membrane and adjacent bony meatus. The bullae develop between the middle fibrous and outer squamous layers of the TM. Causative organisms are similar to those seen in acute otitis media.
Clinical Features:
- Sudden-onset severe unilateral otalgia, often along with upper respiratory tract infection.
- Scanty serosanguinous ear discharge following rupture of the bulla
- Hearing loss is transient and recovers fully. Conductive hearing loss is very common. Mixed or sensorineural hearing loss is also well documented.
- Fullness in the ears
Otoscopic Findings
- Congested TM
- Bullae/vesicles on the TM surface
- Possible blood-stained discharge if bullae rupture
Treatment:
- Usually, a self-limiting disease
- Management is similar to acute otitis media
- Symptomatic: analgesia, warm compresses
- Incision of bullae may be done for pain relief
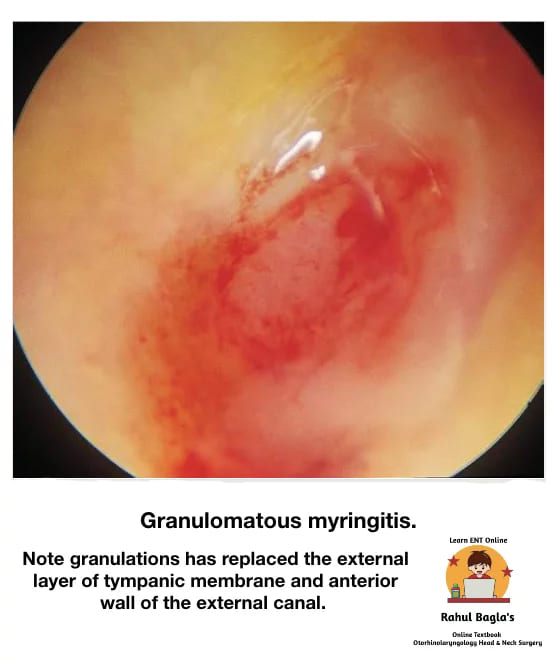
 Granular Chronic Myringitis
Granular Chronic Myringitis
Definition: It is a chronic inflammatory disorder characterised by the presence of nonspecific granulations following de-epithelialization of the outer (epithelial) layer of the tympanic membrane (TM), and there is no middle ear disease.
Aetiology: Unknown. Possible causes: injury to the outer layer of TM impairing epithelialization and promoting granulation tissue formation; Eustachian tube blockage; external ear infection.
Clinical features:
- Persistent or recurrent painless ear discharge, which can be foul-smelling.
- Itching or fullness of the ears.
- Mild conductive hearing loss.
- Some patients may not have symptoms at all.
Otoscopic Findings:
- Granulation tissue/ polyp is present, replacing normal squamous epithelium. It may be localised or diffused.
- Most commonly seen in the posterosuperior region.
- May involve the adjacent bony meatus
- Thickened TM
Management:
- Aural toilet and suction clearance
- Topical antibiotic + steroid drops
- Topical antifungals if fungal infection is suspected
- Topical antiseptics (e.g., acetic acid)
- Dilute vinegar solution (simple and effective)
- Silver nitrate cauterisation of granulation tissue (recurrent cases)
Structural and Degenerative Disorders of Tympanic Membrane
1. Retraction of Tympanic Membrane
Definition: Retraction of the tympanic membrane is invagination of the TM due to negative middle ear pressure, most commonly caused by Eustachian tube dysfunction.
Pathogenesis:
- Eustachian tube blockage → negative middle ear pressure
- TM becomes pulled medially
- TM appears dull and lustreless
Clinical Significance:
- Mild retractions may remain stable
- Deep retractions can trap keratin debris and progress to cholesteatoma
Detailed discussion of retractions is presented in the 🔗 retraction pockets chapter.
 2. Retraction Pocket and Atelectasis
2. Retraction Pocket and Atelectasis
Retraction Pocket
A retraction pocket is a localised invagination of the TM into the middle ear cleft, commonly seen in:
- Pars flaccida (attic region)
- Posterosuperior pars tensa
A deep pocket may accumulate squamous debris and lead to cholesteatoma.
Atelectasis of the Tympanic Membrane
Atelectasis refers to severe retraction where the TM becomes thin and plastered onto middle ear structures, such as the promontory or ossicles.
3. Atrophic Tympanic Membrane
Definition: It is the thinning of the pars tensa of TM due to the absence of the middle fibrous layer, making it weak and prone to retraction and reperforation. It may also remain stable for many years. It is usually circular in outline and sometimes called a replacement membrane.
Occurs in:
- Long-standing serous otitis media. Enzymes present in the middle ear effusion cause loss of the middle fibrous and elastic layers of TM.
- It is also the end result of natural healing of tympanic membrane perforation as it heals only by epithelial and mucosal layers without the middle fibrous layer.
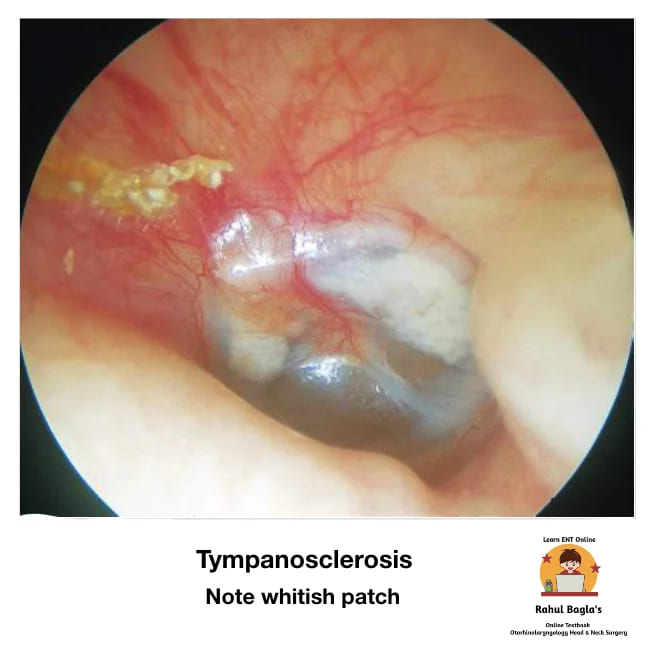
4. Tympanosclerosis (Myringosclerosis)
Definition: It develops in the middle fibrous layer of the tympanic membrane between the outer epidermis and inner mucosal epithelium of the tympanic membrane. It is characterised by hyaline degeneration and, later on, calcification of the tympanic membrane and the middle ear mucosa. The hyaline deposits consist of acellular material seen as chalky white plaques and white nodular deposits.
Note: Mostly affects only TM (myringosclerosis) and rarely causes significant hearing loss. Middle ear tympanosclerosis may involve ligaments, joints of ossicles, and the middle ear cleft, causing ossicular fixation and more severe conductive hearing loss.
5. Perforations of Tympanic Membrane
Detailed discussion of perforations (central, attic, marginal) and their association with chronic otitis media is presented in the 🔗 chronic otitis media chapter. This chapter only notes the classification.
Trauma of Tympanic Membrane
Definition: Traumatic perforation from blunt or penetrating injuries or rapid barometric pressure changes.
Common Causes:
- Penetrating injury (hairpin, matchstick, unskilled instrumentation for wax or foreign body)
- Rapid barometric pressure changes (slap or kiss on ear, forceful Valsalva, sudden implosive blast/pressure wave)
- Pressure by fluid column (diving, aquatic sports, forceful syringing)
- Foreign bodies (button batteries, caustic substances, insects)
- Temporal bone fracture
- Thermal injuries (welders, lightning strike)
 Signs on Examination:
Signs on Examination:
- Perforation and congestion of TM with inverted margins
- Blood clots may be seen
Symptoms:
- Decreased hearing (mainly conductive)
- Pain in the ear
- Tinnitus
- Headache
- Occasionally vertigo
Investigations: Pure tone audiometry (PTA) to assess the degree and type of hearing loss
Management
- Reassurance and observation in uncomplicated cases
- Keep the ear dry
- Avoid instrumentation and water entry
- Avoid ear drops unless infection is suspected
- Antibiotics, nasal decongestants, and symptomatic treatment if needed
- Button batteries require urgent removal
- Prophylactic antibiotics may be given to prevent secondary infection
Healing: Spontaneous healing takes 1-3 months. Therefore, formal repair is advisable only after 3 months.
Options after 3 months:
- Cauterisation of perforation margins with trichloroacetic acid or silver nitrate
- Edges of the perforation repositioned and splinted under the operating microscope
- Paper patches or gel foam is also used to splint the perforation surgically.
- Myringoplasty
Urgent Exploration Indications:
- Facial paralysis
- Subluxation of stapes (vertigo and nystagmus)
- Sensorineural hearing loss
———— End of the Chapter ————
High-Yield Points
- Bullous myringitis causes severe pain but little discharge; incision of bullae relieves pain dramatically.
- Granular myringitis is painless, has granulations on TM, and normal middle ear – differentiate from cholesteatoma.
- Retraction pockets in posterosuperior quadrant are dangerous because they can erode the incus.
- Atelectasis means TM plastered onto promontory – treat with ventilation tube.
- Tympanosclerosis white plaques on TM – if only TM (myringosclerosis), no significant hearing loss.
- Traumatic perforation has inverted margins; chronic perforation has everted margins.
- Wait 3 months before doing myringoplasty for traumatic perforation.
- Vertigo + traumatic perforation = suspect stapes subluxation or perilymph fistula – urgent exploration.
- Button battery in ear is an emergency – causes liquefaction necrosis and perforation.
- Atrophic TM results from loss of middle fibrous layer – prone to retraction and reperforation.
NEET PG-Style MCQs
- A 30-year-old presents with sudden severe ear pain, a few vesicles on the tympanic membrane, and no discharge. The most likely diagnosis is: A. Acute suppurative otitis media B. Bullous myringitis C. Herpes zoster oticus D. Granular myringitis.
- Which of the following is true about granular chronic myringitis? A. Always associated with cholesteatoma B. Granulation tissue on TM with normal middle ear C. Caused by Streptococcus pyogenes D. Requires systemic antibiotics as first line.
- A patient has a central perforation of the tympanic membrane with inverted margins. This indicates: A. Chronic otitis media B. Traumatic perforation C. Cholesteatoma D. Tympanosclerosis.
- Chalky white plaques on the tympanic membrane without hearing loss are called: A. Myringosclerosis B. Tympanosclerosis C. Atrophic TM D. Retraction pocket.
- The most dangerous site for a retraction pocket is: A. Anterior quadrant B. Posterosuperior quadrant C. Pars flaccida D. Inferior quadrant.
- In traumatic perforation of TM, spontaneous healing occurs in most cases within: A. 1 week B. 1–3 months C. 6 months D. 1 year.
- A patient with traumatic perforation develops vertigo and nystagmus. The next best step is: A. Observe for 3 months B. Start oral steroids C. Urgent surgical exploration D. Perform myringoplasty.
- Which layer is lost in an atrophic tympanic membrane? A. Outer epithelial layer B. Middle fibrous layer C. Inner mucosal layer D. All three layers.
- First-line topical treatment for granular myringitis is: A. Systemic antibiotics B. Antifungal powder C. Antibiotic + steroid drops with aural toilet D. Silver nitrate cautery.
- A 25-year-old diver develops sudden hearing loss and bloody otorrhea after surfacing. Otoscopy shows an irregular perforation with inverted edges. The most appropriate initial management is: A. Immediate myringoplasty B. Keep ear dry and observe C. Irrigate with warm water D. Pack ear with antibiotic gauze.
Answers:
1: B. 2: B. 3: B. 4: A. 5: B. 6: B. 7: C. 8: B. 9: C. 10: B.
Clinical Case Scenarios
1. Case 1. A 20-year-old male develops sudden severe ear pain after URTI. Otoscopy shows multiple fluid-filled vesicles on TM with congestion. Most likely diagnosis: Acute bullous myringitis. Best management: Analgesics + treat like acute otitis media, consider incision of bullae for pain relief.
2. Case 2. A 35-year-old woman has recurrent painless foul-smelling discharge with itching. Otoscopy shows granulation tissue on posterosuperior TM without middle ear disease. Most likely diagnosis: Granular chronic myringitis. Best management: Aural toilet + topical antibiotic-steroid drops, acetic acid/vinegar solution, cautery if recurrent.
3. Case 3. A 14-year-old child complains of ear blockage and mild hearing loss. Otoscopy shows a deep posterosuperior retraction pocket with keratin debris. Most likely diagnosis: Retraction pocket with early cholesteatoma. Best next step: Microscopic ear examination + imaging if needed, surgical evaluation.
4. Case 4. A 28-year-old male presents after slap injury with pain, tinnitus, and hearing loss. Otoscopy shows TM perforation with blood clots. PTA shows conductive hearing loss. Best management: Keep ear dry + observation, follow-up for healing over 1–3 months, surgery only if persistent after 3 months.
FAQ in Viva
- Q: What is the most dangerous type of tympanic membrane perforation? A: Attic and marginal perforations are dangerous because they can lead to cholesteatoma.
- Q: How long does traumatic tympanic membrane perforation take to heal? A: Most heal spontaneously within 1–3 months if infection is prevented.
- Q: What is the difference between granular myringitis and CSOM? A: Granular myringitis affects only the TM surface without middle ear disease, while CSOM involves middle ear mucosa.
- Q: Why is a retraction pocket clinically important? A: It traps keratin debris and can progress to acquired cholesteatoma.
- Q: What is myringosclerosis? A: It is chalky white calcified plaques on the TM due to tympanosclerosis limited to the membrane.
- Q: What is atrophic tympanic membrane? A: It is a thin TM lacking fibrous layer, often after OME or healed perforation, and is prone to retraction.
- Q: When should surgery be considered for traumatic TM perforation? A: If it does not heal after 3 months or if complications like SNHL/facial palsy occur.
———— End ————
Download the full PDF Link:
Download PPT:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Otitis media tympanic membrane changes notes, Tympanic membrane disorders mbbs notes, Bullous myringitis symptoms and treatment, Granular myringitis vs csom difference, Retraction pocket tympanic membrane cholesteatoma risk, Atelectasis tympanic membrane adhesive otitis media, Atrophic tympanic membrane replacement membrane, Tympanosclerosis myringosclerosis otoscopy appearance, Central vs marginal vs attic perforation differences, Traumatic tympanic membrane perforation management guidelines, Tympanic membrane perforation healing time, Tympanic membrane perforation neet pg mcqs, Tympanic membrane disorders viva questions, Tympanic membrane examination steps otoscopy, Tympanic membrane retraction due to eustachian tube dysfunction, Cholesteatoma early signs retraction pocket, Tympanic membrane disorders cbme ent, Tympanic membrane perforation classification table, Tympanosclerosis causes and clinical significance, Ear trauma slap injury tympanic membrane rupture, Tympanic membrane perforation paper patch technique, Myringoplasty indications after traumatic perforation, Tympanic membrane disorders summary and revision notes, Tympanic membrane disorders mnemonics and diagrams, Tympanic membrane disorders exam guide india, Tympanic membrane disorders important questions for mbbs, Tympanic membrane disorders pg entrance preparation, Tympanic membrane disorders short notes for viva, Tympanic membrane disorders mcq bank ent, Tympanic membrane pathology otoscopy images description, Tympanic membrane disorders clinical case scenarios, Disorders of tympanic membrane notes for MBBS, Tympanic membrane disorders NEET PG questions, Myringitis causes and treatment, Tympanosclerosis vs myringosclerosis, Traumatic perforation management guidelines, Retraction pocket vs atelectasis, Chronic granular myringitis viva, TM perforation healing time, CBME ENT chapter tympanic membrane, MCQ on bullous myringitis, How to diagnose retraction pocket, Difference between central and marginal perforation, Tympanic membrane anatomy and disorders pdf, ENT practical exam case scenarios, High yield topics tympanic membrane.