Introduction
Head and neck space infections present a significant clinical challenge due to the complexity of the anatomical structures involved and the potential for rapid progression to life-threatening conditions. These infections can arise from various sources and may involve multiple fascial spaces in the head and neck region. A comprehensive understanding of these spaces, the pathways of infection, and the associated clinical presentations is essential for timely diagnosis and effective management. The primary spaces of interest in head and neck infections include:
- Parotid Space
- Submandibular Space (Submaxillary and Sublingual Spaces)
- Peritonsillar Space
- Retropharyngeal Space
- Danger Space
- Parapharyngeal Space (Lateral Pharyngeal Space or Pharyngomaxillary Space)
- Prevertebral Space
- Masticator Space
 Each of these anatomical spaces has distinct features, pathways of infection, and implications for clinical management, making them unique in their presentation and treatment. This chapter provides a detailed exploration of these spaces, including the aetiology, bacteriology, clinical features, complications, and treatment strategies for infections that affect them.
Each of these anatomical spaces has distinct features, pathways of infection, and implications for clinical management, making them unique in their presentation and treatment. This chapter provides a detailed exploration of these spaces, including the aetiology, bacteriology, clinical features, complications, and treatment strategies for infections that affect them.
1. Parotid Space and Parotid Abscess.
 The parotid space is enclosed within the deep cervical fascia, which bifurcates into superficial and deep layers to encapsulate the parotid gland and its associated neurovascular structures. The key contents of the parotid space include the parotid gland, parotid lymph nodes, the facial nerve, the external carotid artery, and the retromandibular vein. The deep cervical fascia layer is very thick on the superficial side but very thin on the deep side of the parotid gland. This structural difference is significant because an abscess formed in the parotid gland can burst through the thin deep fascia, leading to the formation of a parapharyngeal abscess. From there, the infection can potentially spread further into the mediastinum, a serious and life-threatening complication.
The parotid space is enclosed within the deep cervical fascia, which bifurcates into superficial and deep layers to encapsulate the parotid gland and its associated neurovascular structures. The key contents of the parotid space include the parotid gland, parotid lymph nodes, the facial nerve, the external carotid artery, and the retromandibular vein. The deep cervical fascia layer is very thick on the superficial side but very thin on the deep side of the parotid gland. This structural difference is significant because an abscess formed in the parotid gland can burst through the thin deep fascia, leading to the formation of a parapharyngeal abscess. From there, the infection can potentially spread further into the mediastinum, a serious and life-threatening complication.
Aetiology of parotid abscess: Parotid abscesses typically occur in conditions of dehydration, particularly in postoperative or debilitated patients where there is stagnation of salivary flow. The infection usually originates from oral cavity pathogens that ascend via the parotid gland duct (Stenson’s duct) into the parotid gland, leading to multiple small abscesses within the gland that may then coalesce to form a single large abscess.
Bacteriology of parotid abscess: The predominant causative organism is Staphylococcus aureus, though infections may also involve streptococci, anaerobes, and occasionally Gram-negative organisms.
Clinical Features of Parotid Abscess: Symptoms generally develop 5-7 days postoperatively and include swelling, redness, and tenderness in the parotid region and at the angle of the mandible. The abscess is typically unilateral, though bilateral involvement can occur. Due to the thickness of the gland’s capsule, fluctuation may be difficult to detect. Stenson’s duct may exhibit congestion, and pus may be expressed under pressure. Patients often present with systemic signs such as high fever and dehydration.
Diagnosis of parotid abscess: Diagnosis is confirmed through imaging modalities such as ultrasound or CT scanning, which can delineate the extent of the abscess. Aspiration of pus for culture and sensitivity testing is recommended.
Treatment of parotid abscess involves rehydration, improving oral hygiene, sialogogues for promoting salivary flow, and administering intravenous antibiotics. Surgical drainage, typically performed via a preauricular incision, is required to evacuate the abscess, with careful dissection to avoid injury to the facial nerve. A drain is placed in the skin incision and allowed to heal by secondary intention. Monitoring for potential spread to the parapharyngeal space and mediastinum is crucial.
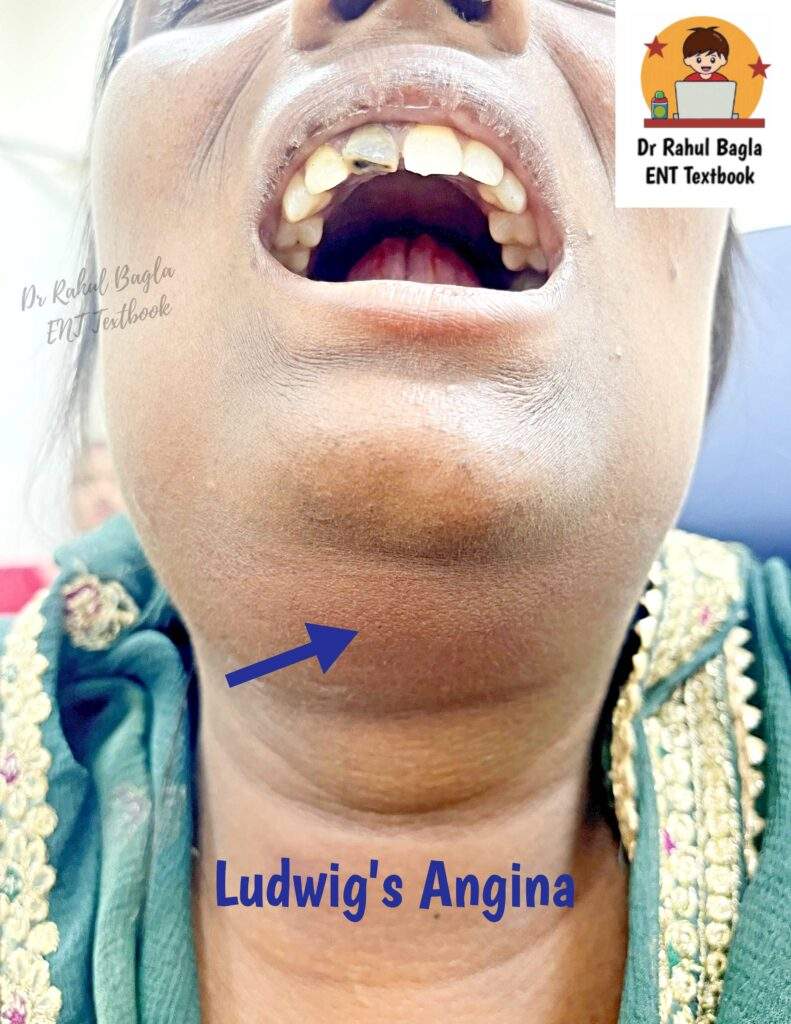
2. Submandibular Space Infections (Ludwig’s Angina)
The submandibular triangle and its underlying submandibular space possess significant anatomical and clinical relevance. The submandibular triangle, also known as the digastric triangle, is a key anatomical area in the anterior neck. It is bounded superiorly by the lower border of the mandible extending to the mastoid process, anteriorly by the anterior belly of the digastric muscle and posteriorly by the posterior belly of the digastric muscle and stylohyoid muscle. Its floor consists of two muscles: the mylohyoid anteriorly and the hyoglossus posteriorly.
Within this triangle, several vital structures reside. These include the marginal mandibular branch of the facial nerve, submandibular gland, level Ib lymph nodes, the facial vein (superficial to the gland), and the facial artery (deep to the gland). Additionally, the inferior portion of the parotid gland lies in the posterior segment of this triangle.

Anatomical Division of the Submandibular Space. Ludwig’s angina is an infection of the submandibular space. The submandibular space is anatomically located between two critical boundaries. On one side, it is bordered by the mucous membrane of the floor of the mouth and the tongue, while on the opposite side, it is enclosed by the superficial layer of the deep cervical fascia, which stretches between the hyoid bone and the mandible.
The mylohyoid muscle divides this space into two distinct compartments:
- Sublingual (Supramylohyoid) Compartment: Positioned above the mylohyoid, it houses the sublingual gland, Wharton’s duct, and hypoglossal nerve (CN XII).
- Submaxillary (Inframylohyoid) Compartment: Located below the mylohyoid, it contains the submandibular gland, lingual nerve, and facial artery.
These compartments communicate around the posterior border of the mylohyoid, facilitating the spread of infections, particularly in pathologies such as Ludwig’s angina.
Aetiology. Infections of the submandibular space are primarily odontogenic, with dental infections, especially from molar and premolar teeth, accounting for nearly 80% of Ludwig’s angina cases. Premolar roots typically lie above the mylohyoid line, allowing infections to involve the sublingual space, whereas molar roots extend below, thereby affecting the submaxillary space. Other etiological factors include:
- Submandibular sialadenitis
- Oral mucosal trauma
- Mandibular fractures
Microbial Spectrum. The bacteriology of Ludwig’s angina is typically polymicrobial, involving both aerobic and anaerobic flora. Common pathogens include:
- Alpha-hemolytic streptococci
- Staphylococcus aureus
- Bacteroides species
- Occasionally, Haemophilus influenzae, E. coli, and Pseudomonas species
Clinical Presentation. Patients with submandibular space infections often present with a triad of symptoms:
- Odynophagia (painful swallowing)
- Trismus (restricted mouth opening)
- Submandibular and submental swelling
When infection localizes in the sublingual space, the tongue is displaced upward and backward, posing a severe airway obstruction risk. Involvement of the submaxillary space results in tender and firm, “woody” swelling of the neck, indicating cellulitis more than a frank abscess. As the infection progresses, the tongue is pushed upwards and backwards, creating a significant risk of airway obstruction. Laryngeal oedema may develop, further endangering the airway and necessitating urgent intervention.
Management and Surgical Approach. Effective treatment of submandibular space abscesses combines broad-spectrum intravenous antibiotics with surgical drainage. The approach to drainage depends on the infection’s location:
- Sublingual space abscesses: Drain intraorally.
- Submaxillary space abscesses: External drainage is required via a transverse incision below the mandible.
In critical cases, particularly when airway compromise is suspected, a tracheostomy is often warranted. A transverse cervical incision, extending from one mandibular angle to the other, allows for comprehensive drainage. Blunt dissection through the midline tongue musculature facilitates decompression. Interestingly, the aspirated material may often be serous, reflecting cellulitis rather than liquefied pus. Nonetheless, pressure release through drainage significantly alleviates symptoms and prevents progression.
Complications and Prognosis. Complications of Ludwig’s angina are potentially life-threatening. These include:
- Airway obstruction due to tongue base displacement or laryngeal oedema
- Mediastinal extension of infection
- Septicemia
- Aspiration pneumonia
- Spread to the parapharyngeal or retropharyngeal spaces
The submandibular space lies between the mucous membrane of the floor of the mouth and the tongue on one side and the superficial layer of the deep cervical fascia extending between the hyoid bone and mandible on the other side.

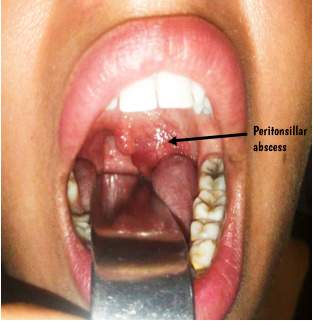
3. Peritonsillar Space and Abscess (Quinsy)
A peritonsillar abscess is a collection of pus in the peritonsillar space, located between the capsule of the tonsil and the superior constrictor muscle. It often follows acute tonsillitis but may also arise independently.
Aetiology of Peritonsillar Space: The abscess typically begins with an infection in one of the tonsillar crypts, most often the crypta magna, leading to an intratonsillar abscess. This abscess eventually breaches the tonsillar capsule, resulting in peritonsillitis and the formation of a peritonsillar abscess.
Bacteriology of Peritonsillar Space: Bacteriological cultures of pus from the abscess commonly reveal a mixed growth of aerobic and anaerobic organisms, including Streptococcus pyogenes, Staphylococcus aureus, and various anaerobes.
Clinical Features of Peritonsillar Space: Peritonsillar abscess primarily affects adults, although acute tonsillitis is more common in children. The abscess is usually unilateral, though bilateral cases have been recorded.
Symptoms:
- Fever (up to 104°F), chills, rigors
- General malaise, body aches, headache
- Nausea and constipation
- Severe Throat Pain: Typically unilateral.
- Odynophagia: Painful swallowing, often so severe that the patient is unable to swallow saliva, leading to drooling.
- Muffled Speech: Often described as a “hot potato voice.”
- Foul Breath: Due to sepsis in the oral cavity and poor oral hygiene.
- Ipsilateral Earache: Referred pain via the glossopharyngeal nerve (CN IX).
- Trismus: Difficulty opening the mouth due to spasm of the pterygoid muscles.
Examination of Peritonsillar Space:
- Tonsillar Area: Congested and swollen tonsil, pillars, and soft palate on the affected side.
- Uvula: Swollen, oedematous, and displaced to the opposite side.
- Soft Palate and Anterior Pillar: Bulging above the tonsil.
- Mucopus: May be present over the tonsillar region.
- Cervical Lymphadenopathy: Commonly involving jugulodigastric lymph nodes.
- Torticollis: The patient often tilts the neck toward the side of the abscess.
Treatment of Peritonsillar Space:
- Hospitalization: Necessary for monitoring and intensive care.
- Intravenous Fluids: To manage dehydration.
- Antibiotics: Administered intravenously in large doses to cover both aerobic and anaerobic organisms.
- Analgesics: Paracetamol for pain relief and fever reduction. In severe cases, stronger analgesics like pethidine may be required. Aspirin is avoided due to the risk of bleeding.
- Oral Hygiene: Maintained with hydrogen peroxide or saline mouthwashes.
- Surgical Intervention: If a frank abscess has formed, incision and drainage are required.
- Incision and Drainage: The abscess is typically opened at the point of maximum bulge above the upper pole of the tonsil, or lateral to the junction of the anterior pillar with a line drawn through the base of the uvula. A guarded knife is used to make a small stab incision, followed by insertion of sinus forceps to open the abscess.
- Interval Tonsillectomy: Performed 4–6 weeks after an attack of quinsy to prevent recurrence.
- Abscess or Hot Tonsillectomy: Some practitioners prefer to remove the tonsils during the acute stage (“hot” tonsillectomy), though this carries risks such as rupture of the abscess during anesthesia and excessive bleeding.
Complications of Peritonsillar Space: Complications are rare with modern treatment but can include:
- Parapharyngeal Abscess: A peritonsillar abscess can potentially progress to a parapharyngeal abscess.
- Laryngeal Oedema: May require tracheostomy to secure the airway.
- Septicaemia: Other possible complications include endocarditis, nephritis, and brain abscess.
- Pneumonitis or Lung Abscess: Due to aspiration of pus if the abscess ruptures spontaneously.
- Jugular Vein Thrombosis.
- Spontaneous Haemorrhage: From the carotid artery or jugular vein.

4. Retropharyngeal Space and Abscess
- Retropharyngeal Space: This anatomical space is situated posterior to the pharynx, between the buccopharyngeal fascia (which covers the pharyngeal constrictor muscles) and the prevertebral fascia. It extends from the base of the skull down to the bifurcation of the trachea. The retropharyngeal space is divided into two lateral compartments, known as the spaces of Gillette, by a fibrous raphe. Each of these lateral spaces contains retropharyngeal lymph nodes, which typically regress by the age of 3–4 years. The retropharyngeal space also communicates with the parapharyngeal space, allowing infections to potentially spread from the retropharyngeal space to the mediastinum via the area posterior to the esophagus.
- Prevertebral Space: Located between the vertebral bodies (posteriorly) and the prevertebral fascia (anteriorly), the prevertebral space extends from the base of the skull to the coccyx. Infections within this space often originate from spinal caries. A distinguishing feature is that an abscess in the prevertebral space usually causes a midline bulge, in contrast to a retropharyngeal abscess, which typically results in a unilateral bulge.
Acute Retropharyngeal Abscess
- Aetiology: This condition is most commonly observed in children under the age of 3. It typically arises from the suppuration of retropharyngeal lymph nodes secondary to infections in the adenoids, nasopharynx, posterior nasal sinuses, or nasal cavity. In adults, it may result from a penetrating injury to the posterior pharyngeal wall or cervical esophagus. Rarely, pus from acute mastoiditis may track along the undersurface of the petrous bone and present as a retropharyngeal abscess.
- Clinical Features:
- Dysphagia and Breathing Difficulty: These symptoms are prominent due to the obstruction of the air and food passages by the abscess.
- Stridor and Croupy Cough: These may be present due to airway obstruction.
- Torticollis: The neck becomes stiff, and the head is held in an extended position.
- Bulge in the Posterior Pharyngeal Wall: This is typically seen on one side of the midline.
- Treatment:
- Incision and Drainage: The abscess is typically drained without anesthesia due to the risk of rupture during intubation. The patient is placed in a supine position with the head lowered. After the mouth is opened with a gag, a vertical incision is made in the most fluctuant area of the abscess. Suction is essential to prevent aspiration of pus.
- Systemic Antibiotics: Appropriate antibiotics are administered to treat the infection.
- Tracheostomy: In cases where a large abscess causes mechanical obstruction of the airway or leads to laryngeal edema, a tracheostomy may be required.
Chronic Retropharyngeal Abscess
Aetiology: Chronic retropharyngeal abscesses are typically tubercular in nature. They may result from caries of the cervical spine or tuberculous infection of the retropharyngeal lymph nodes, secondary to tuberculosis of deep cervical nodes. Abscesses resulting from spinal caries tend to present centrally behind the prevertebral fascia, while those originating from tuberculous lymph nodes are usually located on one side of the midline, similar to true retropharyngeal abscesses.
- Clinical Features:
- Patients may experience discomfort in the throat, though dysphagia is typically mild.
- The posterior pharyngeal wall may show a fluctuant swelling, either centrally or on one side of the midline.
- Tuberculous lymph nodes may be palpable in the neck.
- Diagnostic imaging, particularly X-rays, is crucial in cases involving spinal caries.
- Treatment:
- Incision and Drainage: The abscess can be drained through a vertical incision along the anterior border of the sternocleidomastoid muscle for low abscesses or along its posterior border for high abscesses.
- Antitubercular Therapy: A full course of antitubercular medication is necessary to treat the underlying infection.
5. Danger Space
The danger space, named for its potential severity, is a fascial space extending from the base of the skull to the diaphragm, lying between the prevertebral fascia and the alar fascia. Its name derives from its direct communication with the mediastinum. It contains loose areolar tissue allowing infections to spread rapidly from the neck to the chest.
Aetiology: Infections typically arise from the rupture of a retropharyngeal abscess, allowing the infection to descend into the mediastinum.
Treatment: Given the critical nature of infections in this space, aggressive treatment with intravenous antibiotics and prompt surgical drainage are essential to prevent mediastinitis and other serious complications.
6. Parapharyngeal Space and Abscess
The parapharyngeal space, also known as the pharyngomaxillary or lateral pharyngeal space, has a pyramidal shape, with its base located at the skull base and its apex at the hyoid bone.
Relations:
- Medial: The buccopharyngeal fascia, which covers the constrictor muscles of the pharynx.
- Posterior: The prevertebral fascia, covering the prevertebral muscles and the transverse processes of the cervical vertebrae.
- Lateral: The medial pterygoid muscle, the mandible, and the deep surface of the parotid gland.
The styloid process and the muscles attached to it divide the parapharyngeal space into anterior and posterior compartments.
- Anterior Compartment (Prestyloid): This compartment is related medially to the tonsillar fossa and laterally to the medial pterygoid muscle. It contains internal maxillary artery; fat; inferior alveolar, lingual, and auriculotemporal nerves.
- Posterior Compartment (Poststyloid): This compartment is related medially to the posterior part of the lateral pharyngeal wall and laterally to the parotid gland. It also contains the carotid artery, jugular vein, cranial nerves IX, X, XI, and XII, the sympathetic trunk, and the upper deep cervical nodes.
The parapharyngeal space communicates with several other spaces, including the retropharyngeal, submandibular, parotid, carotid, and visceral spaces.
Aetiology. Infection of the parapharyngeal space can originate from various sources:
- Pharyngeal Infections: Acute and chronic infections of the tonsils and adenoids, as well as the rupture of a peritonsillar abscess, can lead to parapharyngeal space infection.
- Dental Infections: Infections typically originate from the lower last molar tooth.
- Ear Infections: Conditions such as Bezold’s abscess and petrositis can extend into this space.
- Infections from Adjacent Spaces: These include infections of the parotid, retropharyngeal, and submaxillary spaces.
- External Trauma: Penetrating injuries to the neck and complications from local anesthetic injections for tonsillectomy or mandibular nerve block can introduce infection into the parapharyngeal space.
Clinical Features. The clinical presentation varies depending on whether the anterior or posterior compartment is involved.
- Anterior Compartment:
- Prolapse of the Tonsil and Tonsillar Fossa.
- Trismus: Due to spasm of the medial pterygoid muscle.
- External Swelling: Noted behind the angle of the jaw.
- Odynophagia: Significant pain on swallowing.
- Posterior Compartment:
- Bulging of the Pharynx: Behind the posterior pillar.
- Cranial Nerve Paralysis: Involvement of cranial nerves IX, X, XI, XII, and the sympathetic chain.
- Swelling of the Parotid Region.
- Minimal Trismus or Tonsillar Prolapse.
Fever, sore throat, odynophagia, torticollis (due to spasm of the prevertebral muscles), and signs of systemic toxaemia are common in infections of both compartments.
Complications. Parapharyngeal abscesses can lead to several serious complications:
- Acute Laryngeal Edema: This can cause respiratory obstruction.
- Thrombophlebitis of the Jugular Vein: This can lead to septicaemia.
- Spread of Infection to the Retropharyngeal Space.
- Spread of Infection to the Mediastinum: Via the carotid space.
- Mycotic Aneurysm of the Carotid Artery: Caused by weakening of the arterial wall by purulent material, which may involve the common or internal carotid artery.
- Carotid Blowout: Resulting in massive hemorrhage.
- Cranial nerve palsies.
Treatment
- Systemic Antibiotics: Aggressive intravenous antibiotics are often necessary to effectively combat the infection.
- Drainage of Abscess: This procedure is usually performed under general anaesthesia. If trismus is severe, a preoperative tracheostomy may be required. The abscess is drained through a horizontal incision made 2–3 cm below the angle of the mandible. Blunt dissection is then carried out along the inner surface of the medial pterygoid muscle toward the styloid process, and the abscess is evacuated. A drain is inserted. Transoral drainage is contraindicated due to the risk of injury to major vessels passing through this space.
- Airway management.
7. Prevertebral Space
The prevertebral space extends from the base of the skull to the coccyx, lying between the vertebral bodies and the prevertebral fascia. Infections in this space are usually secondary to tuberculosis of the spine (Pott’s abscess) or result from penetrating trauma.
- Clinical Features and Treatment: Patients with prevertebral space infections typically present with neck pain, stiffness, and a midline bulge. Management involves treating the underlying infection, such as tuberculosis, with appropriate medications, and surgical drainage of the abscess if necessary.
8. Masticator Space Infections
The masticator space extends from the base of the skull to the lower border of the mandible and is bounded by the superficial layer of the deep cervical fascia and the muscles of mastication. The masticator space contains the muscles of mastication, the internal maxillary artery, and the mandibular nerve. Infections in this space are commonly related to dental infections, particularly of the third molar.
Compartments:
- Masseteric Space: Located between the masseter muscle and the ramus of the mandible.
- Pterygoid Space: Situated between the pterygoid muscles and the ramus of the mandible.
- Superficial Temporal Space: Found between the superficial temporal fascia and the temporalis muscle.
- Deep Temporal Space: Lies between the temporal fascia and the temporal bone.
- Signs and Symptoms: Patients may present with edema over the posterior ramus of the mandible and trismus.
- Complications: Potential complications include osteomyelitis of the mandible and the extension of infection into adjacent neck spaces.
- Treatment: Management involves addressing the underlying dental infection, which may necessitate surgical intervention to drain any abscesses. Systemic antibiotics are also a crucial part of the treatment regimen.
|
Table: Important spaces of the head and neck and their source of infection |
|||
|
Space |
Extent |
Location |
Source of Infection |
|---|---|---|---|
|
Parotid space |
Between the two layers of superficial layer of deep cervical fascia |
Parotid area |
Infection of oral cavity via Stenson’s duct |
|
Submandibular space |
• Sublingual space. • Submandibular space. |
Below the tongue Submental and submandibular triangles |
Sublingual sialadenitis, Submandibular gland sialadenitis or Molar tooth infection |
|
Peritonsillar space |
Between superior constrictor and capsule of tonsil |
Lateral to tonsil |
Infection of tonsillar crypt |
|
Retropharyngeal space |
Base of skull to tracheal bifurcation (T4) |
Between alar fascia and the buccopharyngeal fascia covering constrictor muscles |
Extension of infection from parapharyngeal space, parotid or masticator space, Oesophageal perforation, Suppuration of retropharyngeal nodes |
|
Danger space |
Base of skull to diaphragm |
Between prevertebral fascia and alar fascia |
Infected by rupture of retropharyngeal abscess |
|
Prevertebral space |
Base of skull to coccyx |
Between vertebrae on one side and prevertebral muscles and the prevertebral fascia on the other |
Tuberculosis of spine Penetrating trauma |
|
Parapharyngeal space |
Base of skull to hyoid bone and submandibular gland |
Buccopharyngeal fascia covering lateral aspect of pharynx medially, and fascia covering pterygoid muscles, mandible and parotid gland laterally |
Peritonsillar abscess, Parotid abscess, Submandibular gland infection, Masticator space abscess |
|
Masticator space |
Base of skull to lower border of mandible |
Between superficial layer of deep cervical fascia and the muscles of mastication— masseter, medial and lateral pterygoids insertion of temporalis muscle and the mandible |
Infection of third molar |
1. Pterygopalatine Fossa (Pterygomaxillary Space)
The pterygopalatine fossa is a pyramidal-shaped space located below the apex of the orbit. This space houses important neurovascular structures, including the maxillary division of the trigeminal nerve, the vidian nerve, the sphenopalatine nerve, the lesser and greater palatine nerves, the sphenopalatine ganglion, and the internal maxillary artery. Infections in this area typically originate from the maxillary teeth or from osteomyelitis.
- Signs and Symptoms: Gingival edema, facial cellulitis, trismus, and ocular symptoms. Infections may also extend into the infratemporal fossa.
- Treatment: Drainage via the Caldwell-Luc approach through the oral buccal sulcus, alongside an appropriate antibiotics.
2. Buccal Space
The buccal space is bounded by the buccinator muscle, the cheek, the pterygomandibular raphe, the zygomatic arch, and the inferior mandible. The most common source of infection is odontogenic in origin.
- Signs and Symptoms: Infections can cause buccal swelling that may extend to the eyelid (preseptal) and involve the orbicularis oris.
- Complications: Serious complications include cavernous sinus thrombosis, intracranial infections, and extension of the infection into other spaces and the orbit.
- Treatment: Prompt drainage, often via an external approach, and an aggressive antibiotic regimen are critical in management.
3. Carotid Sheath Space
The carotid sheath space extends from the base of the skull to the thoracic inlet. It contains the carotid artery, internal jugular vein, and vagus nerve. Infections may extend into this space from adjacent fascial planes.
- Signs and Symptoms: Clinical signs may include torticollis, typically with the head tilted toward the uninvolved side.
- Complications: Potential complications are severe and include shock, carotid blow-out, endocarditis, and cavernous sinus thrombosis.
- Treatment: Surgical drainage and aggressive antibiotic therapy are essential in managing infections in this space.
4. Visceral Space
The visceral space lies between the pharyngeal constrictor muscles and the alar fascia and extends from the skull base to the mediastinum. This space contains critical structures, including the pharynx, oesophagus, larynx, trachea, and thyroid gland.
- Source of Infections: Infections typically arise from perforations of the anterior oesophagal wall due to instrumentation or trauma.
- Signs and Symptoms: Patients may present with dysphagia, hoarseness, emphysema, respiratory compromise, and subcutaneous emphysema.
- Complications: Serious complications include mediastinitis, sepsis, pneumonia, and laryngeal oedema.
- Treatment: Management involves withholding oral intake (nothing by mouth), external drainage, aggressive antibiotic therapy, and possibly a tracheotomy.
———— End of the chapter ————
Download the full PDF Link:
Head and neck space infections Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Juvenile Angiofibroma. https://www.entlecture.com/juvenile-angiofibroma/
- Please read. Tumours of Hypopharynx . https://www.entlecture.com/tumours-of-the-hypopharynx/
- Please read. Anatomy of Oesophagus. https://www.entlecture.com/anatomy-of-oesophagus/
Keywords: Parotid Space, Submandibular Space, Peritonsillar Space, Retropharyngeal Space, Danger Space, Prevertebral Space, Parapharyngeal Space, Masticator Space, Head and Neck Space Infections: Causes, Signs, and Symptoms; Management of Deep Neck Space Infections; Types of Head and Neck Space Infections; Complications of Untreated Neck Space Infections; Diagnosis of Deep Neck Abscess; Surgical Treatment for Neck Space Infections; Risk Factors for Head and Neck Infections; Antibiotics for Deep Neck Infections; Prevention of Head and Neck Space Infections. Head and Neck Space Infections: Causes, Symptoms, and Treatments. Deep Neck Space Infections: Diagnosis and Management Explained. Signs and Symptoms of Head and Neck Space Infections You Shouldn’t Ignore. Complications of Untreated Head and Neck Space Infections: What to Watch For. Comprehensive Guide to Surgical and Antibiotic Treatments for Neck Infections. Understanding the Risk Factors and Prevention Strategies for Neck Space Infections. Types of Head and Neck Space Infections and How They Are Treated. Deep Neck Abscess: Causes, Diagnosis, and Effective Management. Prevention and Early Detection of Head and Neck Infections. How to Identify and Treat Severe Head and Neck Infections Safely.
Thank you sir
Nice presentation
And we need from you add
Empirical treatment for each space according
Sure.
Thanks for the appreciation.
Me encantó la presentación, muchas gracias.
Thanks