|
The following CBME core competencies are covered in this chapter.
|
Chronic Otitis Media (COM)
Definition
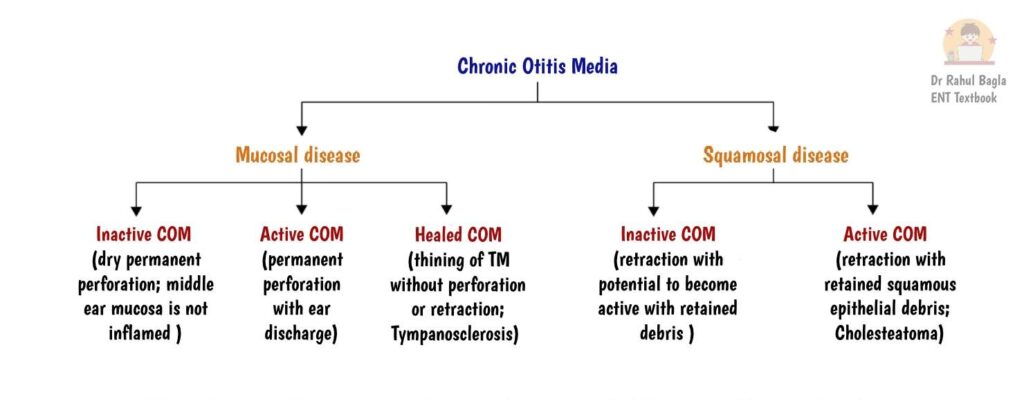
Chronic otitis media (COM) is a chronic inflammatory disease of the middle ear cleft that produces a permanent structural abnormality of the tympanic membrane. This abnormality can be either a permanent perforation or a permanent retraction pocket involving the pars tensa or pars flaccida. The condition may remain active with infection or become inactive without discharge.
A perforation becomes permanent when the outer squamous epithelial layer merges with the inner mucosal layer at the perforation margins. This fusion prevents spontaneous healing because the middle fibrous layer cannot regenerate across the defect. A tympanic membrane perforation persisting for more than 12 weeks is generally considered permanent.
Other common features of COM include hearing loss, recurrent or persistent ear discharge, retraction pockets, granulation tissue, cholesteatoma and cholesterol granuloma.
Historical Terminology
You will often encounter the term chronic suppurative otitis media (CSOM) in older textbooks and examinations. However, modern practice prefers the broader term chronic otitis media (COM) because many patients have chronic middle ear disease without active suppuration or discharge. Therefore, CSOM now specifically refers to the active, discharging form of mucosal COM rather than all chronic ear diseases.
Similarly, the traditional classification into tubotympanic (safe) and atticoantral (unsafe) disease is no longer recommended. These terms are misleading because even so-called safe diseases can occasionally develop complications, while some unsafe ears may remain stable for many years. Nevertheless, you should recognise these terms because they still appear in examinations and older literature.

Epidemiology
According to the WHO, CSOM affects 65–330 million people worldwide, with nearly 50% suffering from hearing impairment. It remains a major cause of preventable hearing loss and is associated with approximately 28,000 deaths annually due to its complications.
COM is more common in developing countries and is associated with:
- Low socioeconomic status
- Overcrowding
- Poor hygiene
- Recurrent upper respiratory tract infections
- Inadequate treatment of acute otitis media
- Limited access to healthcare
In India, the prevalence is higher in rural than in urban populations.
Aetiology and Predisposing Factors
Major predisposing factors include:
- Recurrent acute otitis media (AOM), otitis media with effusion (OME), and Eustachian tube dysfunction
- Recurrent upper respiratory tract infections (URTIs)
- Adenoid hypertrophy causing Eustachian tube obstruction
- Allergic rhinitis and chronic rhinosinusitis
- Low socioeconomic status, overcrowding, poor hygiene, day-care attendance, passive smoking, and air pollution
- Craniofacial abnormalities, especially cleft palate
- Ciliary dysfunction (e.g., primary ciliary dyskinesia/Kartagener syndrome)
- Immunodeficiency states (e.g., HIV infection)
- Genetic predisposition
- Gastro-oesophageal reflux disease (GORD) (possible association)
Factors Influencing Disease Activity
The activity of chronic otitis media depends on several factors that determine whether the ear remains dry or develops recurrent discharge.
- Infection: Bacterial infection is the most important factor responsible for active disease. Common organisms include Pseudomonas aeruginosa, Staphylococcus aureus, Proteus spp., Klebsiella spp., and Escherichia coli. Mixed aerobic and anaerobic infections are common.
- Biofilms: Bacteria may form biofilms, which protect them from antibiotics and host immune responses. Biofilms contribute to persistent infection, recurrent ear discharge, and treatment failure. They are more common in cholesteatoma than in mucosal COM.
- Upper Respiratory Tract Infections (URTIs): URTIs can precipitate disease activity by causing Eustachian tube dysfunction and secondary middle ear infection.
- Water Contamination: Entry of contaminated water into the middle ear through a tympanic membrane perforation during bathing or swimming may trigger recurrent infection and ear discharge.
- Host Factors: Poor immunity, malnutrition, uncontrolled diabetes mellitus, smoking, and poor compliance with treatment may prolong or reactivate the disease.
Pathogenesis of Chronic Otitis Media
Repeated episodes of middle ear inflammation damage the fibrous layer (lamina propria) of the tympanic membrane. Depending on the predominant pathological mechanism, the membrane either perforates or progressively retracts under the influence of chronic Eustachian tube dysfunction and persistent negative middle ear pressure. The weakened tympanic membrane then follows one of two distinct pathways depending on the dominant pathophysiological mechanism.
Pathway 1: Perforation Pathway
Middle ear inflammation
↓
Fibrous layer damage
↓
Permanent perforation of pars tensa
↓
Mucosal COM
Pathway 2: Retraction Pathway
Eustachian tube dysfunction
↓
Persistent negative middle ear pressure
↓
Retraction pocket formation
↓
Accumulation of squamous debris
↓
Cholesteatoma formation
↓
Squamous COM
This concept forms the basis of the modern classification of COM.
Current Classification of Chronic Otitis Media
Mucosal COM
- Active mucosal COM
- Inactive mucosal COM
- Healed COM
Squamous COM
Inactive Squamous COM
- Retraction pockets
- Atelectasis
- Epidermization
Active Squamous COM
- Acquired cholesteatoma
Mucosal COM
Definition
Mucosal COM is characterised by a permanent perforation of the pars tensa without invasion of the middle ear by keratinising squamous epithelium. The middle ear mucosa remains intact but may become inflamed during active episodes. Bone erosion does not occur in uncomplicated mucosal COM. Chronic mucosal otitis media usually develops following recurrent or inadequately treated acute otitis media (AOM), in which the tympanic membrane perforation fails to heal. Less commonly, it may occur after ventilation tube insertion due to persistent perforation, particularly with long-term tubes.
Types of Mucosal COM
- Inactive Mucosal COM (Dry Perforation): This condition is characterised by a permanent central perforation of the pars tensa. The middle ear mucosa is not inflamed, and there is no ear discharge. On otoscopy, the middle ear mucosa appears normal and pale pink. The ear may remain dry for months or years, become active, or occasionally heal spontaneously.
- Active Mucosal COM (Wet Perforation): This condition is characterised by a permanent central perforation of the pars tensa. The middle ear mucosa is inflamed and oedematous, with mucopurulent ear discharge. The disease may remain active, become inactive with treatment, or occasionally lead to complications.
- Healed COM: This condition is characterised by complete healing of the tympanic membrane perforation, either spontaneously or following treatment. The healed tympanic membrane may be thin (atrophic) and/or show localised or generalised opacification of the pars tensa due to loss of the fibrous layer. Residual changes include circular atrophy, tympanosclerosis, retraction pockets, and atelectasis. The atrophic membrane is prone to retraction with persistent negative middle ear pressure and to reperforation following acute otitis media or barotrauma. Most healed ears remain stable; however, persistent Eustachian tube dysfunction may lead to progressive retraction or adhesive otitis media. Tympanosclerosis appears as white hyaline plaques on the tympanic membrane or within the middle ear, where it may involve the promontory, ossicles, oval window, and the tendons of the stapedius and tensor tympani muscles. Involvement of the ossicular chain or oval window may cause conductive hearing loss and reduce the success of tympanoplasty. Most patients remain asymptomatic, although periodic follow-up is advisable because atrophic tympanic membranes and retraction pockets may predispose to recurrent disease or cholesteatoma.





Pathology
- Central Perforation of Pars Tensa: The perforation is always central and may be located anterior, posterior, or inferior to the handle of the malleus. The central perforation is defined as a perforation in the pars tensa that is surrounded by a normal remnant of the tympanic membrane. The size of the perforation can vary, being small, medium, large, or extending up to the annulus, known as subtotal.
According to current recommendations:
-
- Small involves <25% of the tympanic membrane.
- Medium involves 25 to 50%
- Large involves 50 to 75%
- Subtotal involves >75%, leaving only the annulus.
Preferably, perforation size should be documented as a percentage loss of tympanic membrane tissue. However, you should know both systems.
- Middle Ear Mucosa: In inactive mucosal COM, the middle ear mucosa appears normal, pale pink, and moist. During active disease, it becomes red, oedematous, and velvety due to chronic inflammation. Histologically, the middle ear and mastoid mucosa show oedema, submucosal fibrosis, hypervascularity, and inflammatory cell infiltration. There is also an increase in the number of goblet cells and basal cell hyperplasia in the middle ear epithelium. Importantly, there is usually no erosion of the bony walls of the middle ear in mucosal COM.
- Polyps and Granulations: A mucosal polyp may protrude through the perforation. This polyp is a smooth, swollen mass of inflamed mucous membrane. Despite its polypoid appearance, it is actually a large granulation mass that bleeds when touched or removed. You should never avulse an aural polyp blindly because it may arise from the stapes, facial nerve, or horizontal semicircular canal.
- Ossicular Changes: The ossicles are generally preserved in mucosal COM, but they may occasionally undergo necrosis. The lenticular process of the incus is most commonly affected because of its precarious blood supply, followed by the stapes crura, body of incus and manubrium of malleus. Ossicular erosion results from hyperaemic decalcification from increased vascularity and pressure necrosis caused by granulation tissue.
- Tympanosclerosis: Tympanosclerosis is another common finding. It represents hyalinization and calcification of the subepithelial connective tissue from long-standing inflammation. It presents as white, chalky deposits on the tympanic membrane, ossicles, joints, tendons, promontory, and around the oval and round windows. These deposits impair mobility and cause conductive hearing loss.
- Fibrosis and Adhesions: Fibrosis and adhesions may develop during the healing process, further restricting ossicular chain mobility and Eustachian tube function.
Causative Organisms
COM commonly involves multiple aerobic and anaerobic organisms during active infection:
- Aerobic: Pseudomonas aeruginosa, Proteus species, Escherichia coli, Staphylococcus aureus.
- Anaerobic: Bacteroides fragilis, anaerobic Streptococci.
Clinical Features
- Ear Discharge: This is the most common symptom. The discharge is typically profuse, intermittent, and non-foul-smelling. It may be mucoid, mucopurulent, or purulent depending on the bacterial infection. Episodes are often triggered by upper respiratory infections or water entering the perforated ear. The discharge usually responds well to antibiotic ear drops, after which the ear becomes dry.
- Hearing Loss: The hearing loss is primarily conductive, usually not exceeding 50 dB. However, you should understand a fascinating phenomenon called the round window shielding effect. When the ear is actively discharging, the discharge covers the round window and prevents sound waves from striking it. Only the oval window receives sound stimulation, so the phase differential is preserved, and hearing may actually improve compared to the dry state. When the ear is dry, sound waves strike both the oval and round windows simultaneously, causing phase cancellation and worsening hearing loss. Prolonged disease can also cause mixed hearing loss because toxins absorbed through the round window damage the cochlea. Ossicular necrosis, especially of the long process of the incus, further increases the conductive loss.
Investigations
- Otoscopy/ Microscopy/ Endoscopy: Identifies a central perforation of the pars tensa. Note the following:
- Size: The perforation can be small, medium, large, or subtotal.
- Position: It can be located anterior, posterior, or inferior to the handle of the malleus.
- Middle Ear Mucosa: When the perforation is large, the middle ear mucosa can be observed. Normally, it appears pale pink and moist. When inflamed, it looks red, oedematous, and swollen.
- Examination under microscope (EUM): EUM is the ‘gold standard’ for the diagnosis of COM, and it is essential for all patients with chronic middle ear disease. This allows you to clean the discharge thoroughly, confirm the diagnosis, assess the ossicular chain status, identify granulations, rule out hidden cholesteatoma, detect tympanosclerosis and adhesions, and collect pus for culture and sensitivity testing. An otoendoscope with a video camera provides excellent visualisation, documentation, and patient education.
- Pure Tone Audiometry and Tuning Fork Tests: Determine the degree and type of hearing loss (conductive, sensorineural, or mixed).
- Culture and Sensitivity: Identifies causative microorganisms and guides appropriate antibiotic therapy to avoid resistance.
- Mastoid X-ray: Mastoid X-rays have little role in mucosal COM today. They may show a sclerotic or pneumatized mastoid with clouded air cells, but they cannot differentiate soft tissue from bone erosion.
- HRCT Temporal Bone: It is recommended when the ear fails to dry with medical treatment or when you suspect squamous disease, cholesteatoma, complications, or ossicular erosion. It evaluates mastoid pneumatization, bony erosion, ossicular status, and the extent of disease.
Treatment of Mucosal COM
The goals of treatment are to eradicate infection, achieve a dry ear, close the tympanic membrane perforation, improve hearing, and prevent complications.
Medical management
Medical management focuses on controlling active infection, achieving a dry ear, and preparing the ear for surgery when indicated.
- Aural Toilet: Essential for removing discharge and debris. It is achieved through dry mopping, suction cleaning under a microscope, or irrigation with sterile saline, followed by thorough drying.
- Ear Drops: Antibiotic-steroid ear drops are the mainstay of treatment for active mucosal COM. Commonly used antibiotics include ciprofloxacin, gentamicin, chloramphenicol, and polymyxin. Topical therapy achieves much higher middle ear drug concentrations than systemic antibiotics. Fluoroquinolone drops (e.g., ciprofloxacin or ofloxacin) are preferred because they are effective and non-ototoxic, whereas aminoglycosides (e.g., gentamicin) should be used cautiously in the presence of a tympanic membrane perforation. Proper instillation involves lying with the affected ear upward, instilling the drops, and pumping the tragus to facilitate entry into the middle ear.
- Systemic Antibiotics: Systemic antibiotics are useful during acute-on-chronic exacerbations but have limited efficacy in chronic cases.
- Treatment of Contributory Causes: Treat associated conditions such as adenoid hypertrophy, chronic rhinosinusitis, tonsillitis, allergic rhinitis, and Eustachian tube dysfunction to reduce recurrence.
- Precautions: Patients should avoid water entry into the ear during bathing or swimming by using protective earplugs. They should also refrain from hard-nose blowing and self-cleaning.
- Acidic solutions: Diluted acetic acid (1.5–2%) may help control Pseudomonas infection but should be used cautiously because prolonged use may cause canal irritation, fungal overgrowth, or rarely ototoxicity.
Surgical management
Surgery is indicated in patients with persistent tympanic membrane perforation causing recurrent ear discharge, significant hearing loss, difficulty with water exposure, or when complications are suspected.
- Aural polyps or granulations: Remove aural polyps or granulations before local antibiotic treatment to enhance efficacy. Polyps should be excised sharply under direct vision. An aural polyp should never be avulsed, as it may arise from structures such as the stapes, facial nerve, or horizontal canal, which can lead to complications such as facial paralysis or labyrinthitis.
- Reconstructive Surgery: Reconstructive surgery aims to restore hearing and prevent reinfection. Myringoplasty closes the tympanic membrane perforation alone. Tympanoplasty combines myringoplasty with ossicular reconstruction.
-
For small perforations, chemical cauterisation using 50% trichloroacetic acid or 25% silver nitrate can be done. Repeat the procedure after two weeks if the perforation has not healed completely. Another option is the fat plug myringoplasty (pop-in technique), which uses lobular fat as an inlay graft.
-
For large perforations, perform myringoplasty using temporalis fascia as the most common graft material. If the ossicular chain is disrupted, add ossicular reconstruction and call the procedure tympanoplasty.
-
- Cortical mastoidectomy: Cortical mastoidectomy with myringoplasty may be performed in selected cases of active mucosal COM. Although surgery is preferably done in a dry ear, an active ear is not an absolute contraindication.
Inactive Squamous Chronic Otitis Media (Retraction, Atelectasis and Epidermization)
Definition
This condition is characterised by chronic negative middle ear pressure, which causes retraction (atelectasis) of the tympanic membrane, resulting in a retraction pocket. A retraction pocket is a localised area of invagination of the tympanic membrane into the middle ear or attic. Retraction pockets may be free (mobile) or fixed (adherent to middle ear structures). Along with chronic Eustachian tube dysfunction, inflammatory mediators, including collagenase and elastase, released during recurrent middle ear inflammation, contribute to the degradation of the middle fibrous layer (lamina propria), making the tympanic membrane atrophic and more susceptible to retraction. While inactive squamous COM has no discharge, the retraction pockets may harbour squamous debris that can later become infected and develop into cholesteatoma. Some pockets are shallow and self-cleansing, but others are deep with narrow necks that trap keratin.
See Chapter: Retraction Pockets
Classification of Pars Tensa Retractions (Sade)
- Grade 1: The pars tensa is slightly retracted, not touching the ossicles
- Grade 2: The pars tensa is retracted and adherent to the ossicles.
- Grade 3: The pars tensa is draping the promontory, without adhering to it.
- Grade 4: The pars tensa is draped and adherent to the promontory.
Classification of Pars Flaccida Retractions (Tos)
- Grade 1: There is a dimple in the pars flaccida, but not adherent to the malleus.
- Grade 2: Pars flaccida is adherent to the neck of the malleus with no erosion of scutum.
- Grade 3: Partial erosion of the bony outer attic wall (scutum).
- Grade 4: Gross outer attic wall erosion.
Atelectasis and Epidermization
Atelectasis refers to the diffuse collapse of the tympanic membrane onto middle ear structures from prolonged negative pressure. Adhesive otitis media is an advanced stage of atelectasis in which the entire tympanic membrane becomes firmly adherent to the promontory and ossicles because of prolonged Eustachian tube dysfunction and loss of the fibrous layer. It represents the end stage of tympanic membrane retraction.
Epidermization is a more advanced stage where the middle ear mucosa is replaced by keratinising squamous epithelium without retention of keratin debris.
Management
- Observe stable, self-cleansing retractions with regular follow-up.
- Provide medical treatment for underlying allergy and sinonasal disease.
- Surgical options include excision of the retraction pocket, cartilage tympanoplasty, or marsupialisation, where indicated. Mastoid surgery is not routinely indicated in the absence of cholesteatoma.
- Hearing aids should always be considered in patients whose primary complaint is hearing impairment, particularly when surgery is unlikely to provide significant hearing improvement.
Active Squamous COM (Cholesteatoma)
Definition of Cholesteatoma
Cholesteatoma is a benign cystic lesion lined by keratinising stratified squamous epithelium, and it is the hallmark of active squamous COM. It contains desquamated keratin debris and is a locally destructive, bone-eroding lesion. It is associated with reduced middle ear volume, poor Eustachian tube function, osteitis, granulation tissue formation, and progressive bone erosion. Cholesteatoma may involve the ossicular chain, mastoid air cell system, facial nerve canal, labyrinth, and surrounding temporal bone, predisposing to both intratemporal and intracranial complications. Despite its name, it contains no cholesterol and is not a tumour. The term is a misnomer that persists for historical reasons.
Aetiology of Cholesteatoma
It most commonly develops from a retraction pocket, typically in the pars flaccida or posterosuperior part of the pars tensa due to chronic eustachian tube dysfunction and negative middle ear pressure. These regions are particularly vulnerable to inflammatory damage during acute otitis media and otitis media with effusion, resulting in weakening of the fibrous layer of the tympanic membrane. The weakened areas of the tympanic membrane are sucked inward, forming a pocket. If the pocket neck becomes narrow, desquamated keratin cannot escape and accumulates. As the keratin mass enlarges, it releases collagenase and other proteolytic enzymes that erode bone. Less commonly, cholesteatoma develops by epithelial migration through a pre-existing marginal perforation (secondary acquired cholesteatoma). Congenital cholesteatoma presents behind an intact tympanic membrane in a child with no previous history of otorrhoea, tympanic membrane perforation, or ear surgery.
Pathology
Active squamous COM is associated with the following pathological processes:
- Cholesteatoma. Cholesteatomas invade surrounding structures, initially following the path of least resistance and later through enzymatic bone destruction. They can extend backwards into the aditus, antrum, and mastoid, and downwards into the mesotympanum, surrounding ossicles like the incus and malleus. Bone destruction is mediated by inflammatory cytokines and proteolytic enzymes released by inflammatory cells and cholesteatoma matrix, which stimulate osteoclastic bone resorption, rather than pressure necrosis.
- Osteitis and Granulation Tissue. Chronic inflammation surrounding the cholesteatoma produces osteitis and exuberant granulation tissue. Granulation tissue may fill the attic, antrum, and mastoid and may present as a fleshy red polyp. Osteitis reflects the underlying inflammatory process and contributes to progressive bone destruction through cytokine-mediated osteoclastic activity and facilitates the spread of infection.
- Ossicular Necrosis. Ossicular necrosis, particularly of the long process of the incus (but can extend to the superstructure of the stapes, the handle of the malleus, or the entire ossicular chain), is common in active squamous COM, resulting in severe hearing loss. However, in some cases, cholesteatoma bridges the gap left by necrosed ossicles, preserving hearing (“cholesteatoma hearer”).
- Cholesterol granuloma: It is a pathological entity characterised by a mass of granulation tissue containing foreign body giant cells that encircle cholesterol crystals. This condition arises as a reaction to the prolonged retention of secretions or haemorrhage and may or may not coexist with cholesteatoma. When a cholesterol granuloma is present in the mesotympanum, behind an intact tympanic membrane, the latter may appear blue.
See Chapter: Cholesteatoma
Symptoms
- Ear Discharge: The discharge is typically scanty but foul-smelling due to osteitis, bone erosion by cholesteatoma, putrefaction of desquamated epithelial cells in the cholesteatoma sac and anaerobic bacterial infection. The discharge usually persists despite topical or systemic antibiotics because the underlying disease is cholesteatoma rather than infection alone. Antibiotics temporarily control secondary infection but cannot eradicate the underlying cholesteatoma. Blood-tinged discharge can be seen after cleaning the ear due to the presence of granulations. Sudden cessation of discharge, especially after prolonged activity, is a serious sign that suggests obstruction by crusted discharge, inflammatory mucosa, or a polyp. This obstruction can lead to pus accumulation and cause complications.
- Hearing Loss: Hearing loss may not be apparent if the ossicular chain is intact or if cholesteatoma bridges gaps left by necrosed ossicles (“cholesteatoma hearer”). While hearing loss is predominantly conductive, there may also be a sensorineural component. Eroding cholesteatoma causes ossicular necrosis, leading to conductive deafness, and inner ear involvement, resulting in sensorineural deafness.
- Bleeding: Bleeding may occur from granulations or polyps.
- Perforation and retraction pockets: There may be an attic perforation or a retraction pocket in the posterior–superior quadrant. The deep retraction pocket with a narrow neck may collect debris and have cholesteatoma flakes.
- Complications: In case of active squamous COM, there is a higher chance of complications; therefore, it is important to take relevant history and examinations to rule out these.
 Clinical Examination
Clinical Examination
- Attic perforation
- Retraction pocket
- Keratin debris/ Cholesteatoma flakes
- Attic crust hiding an underlying cholesteatoma
- Granulations
- Aural polyp
- Hidden discharge
- Evidence of bone erosion (e.g. scutum erosion or widened attic)
- Ossicular status
- Self-cleansing/non-self-cleansing pocket assessment
Features Suggesting Complications in COM
- Pain: Pain is uncommon in uncomplicated chronic suppurative otitis media (CSOM). Its presence is considered serious as it may indicate extradural, perisinus, or brain abscess. Sometimes, it is due to otitis externa associated with a discharging ear.
- Vertigo: Vertigo indicates erosion of the lateral semicircular canal, which may progress to labyrinthitis or meningitis. A fistula test should be performed in all cases.
- Persistent Headache: A persistent headache is suggestive of an intracranial complication.
- Facial Weakness: Facial weakness indicates erosion of the facial canal.
- Listless Child: A listless child refusing to take feeds and easily falling asleep may indicate an extradural abscess.
- Fever, Nausea, and Vomiting: These symptoms are indicative of an intracranial infection.
- Irritability and Neck Rigidity: These symptoms are suggestive of meningitis.
- Diplopia: Diplopia may indicate Gradenigo syndrome or petrositis.
- Ataxia: Ataxia may indicate labyrinthitis or cerebellar abscess.
- Abscess Around the Ear: This indicates mastoiditis.
Investigations
- Microscopic Examination under microscope (EUM). It allows thorough cleaning of the discharge and confirmation of the diagnosis. Assesses ossicular chain status, identifies granulations, epithelial ingrowth, hidden discharge or cholesteatoma, tympanosclerosis, and adhesions. Facilitates pus collection for Culture and Sensitivity testing. All patients with chronic middle ear disease should be examined under the microscope.
- Classify the retraction according to Tos.
- Assessment of Retraction Pocket: Visibility of fundus, Presence of keratin debris, Evidence of cholesteatoma, Self-cleansing or non-self-cleansing nature. A small, clean retraction pocket in the pars flaccida or pars tensa is likely to be self-cleansing, but such judgements can only be confirmed over time by clinical review.
- Examination of cholesteatoma, its site and extent, evidence of bone destruction, granuloma, condition of ossicles and pockets of discharge.
- Otoendoscopy: Useful for outpatient assessment, especially in patients with narrow ear canals.
- Audiometry and Tuning Fork Tests: Determine the degree and type of hearing loss (conductive, sensorineural, or mixed).
- Culture and Sensitivity: Identifies causative microorganisms and guides appropriate antibiotic therapy, avoiding resistance.
- X-ray mastoids. They indicate the extent of bone destruction and the degree of mastoid pneumatization. Although largely replaced by HRCT temporal bone scanning, mastoid radiographs may occasionally be useful for assessing mastoid pneumatization, sclerosis, a low-lying dura, an anteriorly placed sigmoid sinus, and destruction of the attic and antrum (key area).
- HRCT Temporal Bone Scan: It is preferred over mastoid X-rays. It provides detailed anatomical landmarks, shows the extent of bone destruction, identifies scutum erosion, ossicular erosion, facial canal dehiscence, and labyrinthine fistula.
- DW-MRI: Differentiates cholesteatoma from inflammatory tissue. It is very useful for detecting residual cholesteatoma after surgery. A negative DW-MRI performed 9–12 months after surgery can often avoid routine second-look surgery and has become the preferred method for detecting residual cholesteatoma in many centres.
Treatment
Principles of Management. The primary management of active squamous COM is surgical, which involves mastoid exploration (mastoidectomy) to remove disease from the mastoid and middle ear. Discharge in active squamous COM is primarily due to bony erosion, so medical management with local or systemic antibiotics is reserved for superimposed acute infections or complications like intracranial infections caused by cholesteatoma.
Medical treatment has only a limited role and is aimed at controlling secondary infection and preparing the ear for surgery. Cholesteatoma itself cannot be eradicated medically; therefore, definitive treatment is surgical.
AIM of mastoid surgery:
The aims of mastoid surgery, listed in order of priority, are:
- Eradication of disease from the ear (especially cholesteatoma): The surgeon removes all diseased tissue using appropriate mastoidectomy procedures. These procedures aim to expose, excise, and exteriorise (EEE) the diseased areas, thereby creating a safe ear and preventing recurrence or complications.
- Creation of a dry, well-epithelialized ear: Following disease clearance, the surgeon aims to achieve a dry and self-cleaning ear. The mastoid cavity gradually epithelializes over approximately 6–10 weeks, depending on its size and extent.
- Preservation or improvement of hearing: Once disease eradication has been achieved, the surgeon attempts to preserve or restore hearing whenever feasible. Hearing reconstruction may be performed using autografts of the incus or malleus, or with prosthetic devices such as a partial ossicular replacement prosthesis (PORP) or total ossicular replacement prosthesis (TORP), commonly made of titanium or Teflon. Ossiculoplasty may be performed during the primary surgery or as a second-stage procedure after 9–12 months.
Postoperative mastoid cavities affect the acoustics of the external auditory canal, thereby producing additional hearing loss and difficulty in fitting the hearing aids, if so required.
Two Main Surgical Approaches:
- Canal Wall Down Mastoidectomy: The posterior wall of the middle ear is removed entirely to provide better access and visualisation of the disease. Canal wall down procedures have a lower recurrence rate of cholesteatoma (approximately 5–15%), and recurrent disease is usually detected during routine follow-up without the need for planned second-look surgery.
- Intact Canal Wall Mastoidectomy: A small opening is made in the posterior wall of the middle ear (common wall between the middle ear and mastoid) while preserving the canal wall. The recurrence or residual disease rate is higher (approximately 20–40%) than with canal wall down surgery.
The initial steps of mastoid exploration (mastoidectomy) for both mastoidectomies are identical until reaching the mastoid antrum. The steps are:
- A post-auricular incision (Wilde’s incision) is made, and Macewen’s triangle is exposed.
- Mastoid exploration begins at Macewen’s triangle using cutting burrs to remove mastoid air cells.
- Adequate irrigation is maintained during drilling to wash away bone dust, improve visualisation, and reduce heat-related injury risks.
- Near critical structures like the facial nerve, diamond burrs are used for precision.
- Haemostasis is achieved using bipolar cautery, bone wax, or diamond burrs, which produce bone dust to seal bleeding vessels.
- Canal Wall Down Procedures (Open Cavity): These procedures leave the mastoid cavity open into the external auditory canal, fully exteriorising the diseased area. Commonly performed operations include:
- Atticotomy: Limited to the attic region; the defect in the attic wall is closed with tragal or conchal cartilage.
- Atticoantrostomy: An anterior-to-posterior approach where cholesteatoma is identified in the epitympanum or posterior mesotympanum and followed backwards.
- Modified Radical Mastoidectomy: A posterior-to-anterior approach where the mastoid is opened behind the external auditory canal, the cholesteatoma is identified, and the posterior bony wall of the canal is removed.
- Radical Mastoidectomy: Extensive removal of diseased tissue.
Common causes of ear discharge following canal wall down procedures include:
- a high facial ridge
- a sump in the cavity below the floor of the external auditory canal
- perforation in the tympanic membrane
- small external auditory meatus.
- Canal Wall-Up Procedures (Closed Cavity or Combined Approach Tympanoplasty):
In this, the disease is removed both per-meatally and through a cortical mastoidectomy & posterior tympanotomy approach, creating a window between the mastoid and middle ear through the facial recess to reach the sinus tympani, retaining an intact external auditory canal without creating a mastoid cavity. Hearing reconstruction, if required, is done through the EAC side. This approach is technically more challenging and time-consuming, but it results in a dry ear and facilitates the reconstruction of the hearing mechanism.

Steps of surgery:
- Post-Auricular Incision: A Wilde’s incision exposes Macewen’s triangle, the surgical landmark for mastoid exploration.
- Mastoid Exenteration: Mastoid air cells are meticulously drilled to access the mastoid antrum (~1.5 cm deep to Macewen’s triangle).
- Antral Disease Removal: Cholesteatoma or granulations within the antrum are excised.
- Posterior Tympanotomy: A small opening is made in the facial recess (lateral to the vertical fallopian canal) to access the middle ear.
- Sinus Tympani Clearance: The sinus tympani, medial to the fallopian canal and a common site for residual disease, is visualised and cleared through the tympanotomy window.
Advantages:
- Preserves natural ear anatomy, reducing postoperative cavity maintenance.
- Facilitates hearing reconstruction (ossiculoplasty) via the EAC.
- Achieves a dry, functional ear with minimal cosmetic impact.
Challenges:
- Residual Disease Risk: There is a risk of leaving residual cholesteatoma behind, leading to a high incidence (20-50%) of recurrent disease.
- Second-Look Surgery: Often required after 12–18 months to detect residual disease. A second look can often be avoided with the use of diffusion-weighted MRI (DW-MRI).
Conservative Treatment: Conservative treatment has a limited role in managing cholesteatoma but can be attempted in selected cases where the cholesteatoma is small and easily accessible to suction clearance under an operating microscope. Repeated suction clearance and periodic check-ups are essential. Conservative treatment is also considered for elderly patients above 65, those unfit for general anaesthesia, or those refusing surgery. Polyps and granulations can be surgically removed by cup forceps or cauterised with chemical agents like silver nitrate or trichloroacetic acid. Additional measures such as aural toilet and dry ear precautions are also necessary. Hearing aids should always be considered in cases of hearing disability.


Clinical Approach to a Patient with Chronic Ear Discharge
History
↓
Otoscopy
↓
Microscopy/Otoendoscopy
↓
Audiological assessment
↓
Imaging when indicated
↓
Classification of disease
↓
Treatment planning
Table: Comparison of Mucosal and Squamous COM
| Feature | Mucosal COM | Squamous COM |
| Pathology | Perforation | Retraction/Cholesteatoma |
| Tympanic membrane finding | Central perforation | Attic perforation/ Posterosuperior retraction pocket |
| Discharge | Profuse, non-foul | Scanty, foul |
| Hearing loss | Usually mild to moderate conductive | Often more severe; may be mixed |
| Bone erosion | Uncommon (may occur due to osteitis) | Common |
| Cholesteatoma | Absent | Present |
| Complications | Uncommon | Common |
| Treatment | Medical + Tympanoplasty | Mastoid surgery |
———— End of the chapter ————
High-Yield Points for NEET PG and University Exams
- Chronic otitis media requires a permanent TM abnormality persisting beyond 12 weeks. Central perforation has a normal TM remnant all around, while marginal perforation reaches the annulus or involves the attic.
- The round window shielding effect explains why hearing may improve during active discharge in the mucosal COM.
- Never use aminoglycoside ear drops (gentamicin, neomycin) through a perforated TM because they can cause sensorineural hearing loss. Fluoroquinolones are safe.
- Cholesteatoma erodes bone through enzymatic action (collagenase, proteases), not pressure necrosis.
- The most common ossicle to necrose in the COM is the long process of the incus due to its poor blood supply.
- Pars flaccida and posterosuperior pars tensa are the weakest areas of the TM because they have less fibrous tissue.
- Tos classification is for pars flaccida retractions (Grade 1 to 4). Sade classification is for pars tensa retractions (Grade 1 to 4).
- A positive fistula test (nystagmus with pressure changes) indicates erosion of the lateral semicircular canal.
- Sudden cessation of foul-smelling discharge with increasing pain suggests complications due to obstruction of drainage.
- DW-MRI has high sensitivity (90 to 94%) for detecting residual cholesteatoma >2mm and can avoid second-look surgery if negative at 9 to 12 months.
- The EEE principle of cholesteatoma surgery stands for Expose, Excise, Exteriorise.
- Canal wall down procedures require lifelong cavity care. Canal wall up procedures have higher residual disease rates but no cavity.
- A cholesteatoma hearer has good hearing despite ossicular necrosis because the cholesteatoma sac itself conducts sound.
NEET PG-Style MCQs with Answers
- A 35-year-old patient has had a central perforation of the pars tensa with intermittent, non-foul discharge for 2 years. The ear becomes dry with ciprofloxacin drops. What is the most appropriate diagnosis? A. Active squamous COM B. Active mucosal COM C. Inactive squamous COM D. Healed COM
- Which of the following is the most common organism isolated in active mucosal COM? A. Streptococcus pneumoniae B. Pseudomonas aeruginosa C. Haemophilus influenzae D. Moraxella catarrhalis
- A patient with a dry central perforation reports that his hearing worsens when the ear is dry but improves when it discharges. What explains this phenomenon? A. Cochlear ototoxicity B. Ossicular fixation C. Round window shielding effect D. Eustachian tube opening
- Which ossicle is most commonly necrosed in chronic otitis media? A. Malleus head B. Stapes footplate C. Long process of incus D. Malleus handle
- A patient has a retraction pocket in the pars flaccida with partial erosion of the scutum seen on HRCT. According to Tos classification, this is: A. Grade 1 B. Grade 2 C. Grade 3 D. Grade 4
- Which of the following is a contraindication for using gentamicin ear drops in a patient with ear discharge? A. Age less than 10 years B. Presence of a tympanic membrane perforation C. Pregnancy D. Associated diabetes mellitus
- A patient with chronic ear discharge suddenly develops severe headache, fever, and neck rigidity. What is the most likely complication? A. Labyrinthitis B. Mastoiditis C. Meningitis D. Facial paralysis
- Diffusion-weighted MRI is most useful in cholesteatoma for: A. Preoperative diagnosis B. Detecting residual disease post-surgery C. Assessing hearing loss severity D. Planning ossiculoplasty
- The EEE principle of cholesteatoma surgery stands for: A. Explore, Excise, Examine B. Expose, Examine, Evaluate C. Expose, Excise, Exteriorize D. Explore, Evaluate, Exteriorise
- A patient with cholesteatoma has surprisingly good hearing despite extensive ossicular necrosis on HRCT. What is the term for this phenomenon? A. Cholesteatoma paradox B. Cholesteatoma hearer C. Ossicular bypass D. Round window shielding
Answers: 1:B, 2:B, 3:C, 4:C, 5:C, 6:B, 7:C, 8:B, 9:C, 10:B
Clinical Case Scenarios
Case 1. A 25-year-old woman presents with intermittent, non-foul discharge from the left ear for 3 years. She has had multiple episodes triggered by swimming. Otoscopy shows a large central perforation of the pars tensa with a moist, pale middle ear mucosa. Her pure tone audiometry shows 40 dB conductive hearing loss. What is the most likely diagnosis? What is the first step in management? What surgical procedure would you plan after the ear becomes dry?
Answer: Active mucosal COM. First step is aural toilet and topical ciprofloxacin drops. After the ear becomes dry, plan myringoplasty with a temporalis fascia graft.
Case 2. A 45-year-old man presents with scanty, foul-smelling discharge from the right ear for 6 months. He has no pain but reports occasional dizziness when he blows his nose. Otoscopy shows a retraction pocket in the pars flaccida with keratin debris. Pure tone audiometry shows 50 dB mixed hearing loss. What is the most likely diagnosis? What investigation would you order next? What is the surgical approach of choice?
Answer: Active squamous COM with cholesteatoma. Order an HRCT temporal bone to assess bone erosion and rule out a lateral canal fistula. Surgical approach depends on findings; canal wall down mastoidectomy is preferred if there is a fistula or extensive disease.
Case 3. A 60-year-old diabetic patient with known COM for 10 years presents with sudden-onset severe left ear pain, fever, and postauricular swelling. He had a foul discharge that stopped suddenly 2 days ago. What is the most likely diagnosis? What is emergency management?
Answer: Acute mastoiditis with possible intracranial complication. The sudden cessation of discharge suggests obstruction. Emergency management includes admission, IV antibiotics (ceftriaxone + metronidazole), contrast-enhanced CT scan, and emergency mastoidectomy.
Case 4. A 30-year-old patient undergoes a canal wall-up mastoidectomy for cholesteatoma. The surgeon plans a second-look surgery at 12 months. However, at 9 months, a DW-MRI shows no restricted diffusion. What is the appropriate next step?
Answer: Second-look surgery can be avoided because a negative DW-MRI at 9 to 12 months has a high negative predictive value (92 to 95%) for residual cholesteatoma >2mm. Continue clinical follow-up.
Frequently Asked Questions in Viva
- What is the difference between CSOM and COM? CSOM (chronic suppurative otitis media) specifically refers to active, discharging COM, while COM includes both active and inactive disease, with or without discharge. The term COM is now preferred because many patients have chronic middle ear disease without active suppuration.
- How long does a perforation need to persist to be called permanent? A tympanic membrane perforation persisting for more than 12 weeks is generally considered permanent because spontaneous healing becomes unlikely after this period.
- Why should I never use gentamicin ear drops in a patient with a perforated eardrum? Aminoglycosides like gentamicin are ototoxic and can be absorbed through the round window membrane, causing sensorineural hearing loss. Fluoroquinolones (ciprofloxacin, ofloxacin) are safe alternatives.
- What is a cholesteatoma, and why is it dangerous? Cholesteatoma is a sac of keratinising squamous epithelium that accumulates keratin debris and erodes bone through enzyme release (collagenase, proteases). It is dangerous because it can erode the ossicles, facial nerve canal, lateral semicircular canal, and the bony covering of the brain (tegmen), leading to hearing loss, facial paralysis, vertigo, meningitis, and brain abscess.
- What is the difference between a canal wall up and a canal wall down mastoidectomy? Canal wall up preserves the posterior bony ear canal, avoids a cavity, and requires no lifelong care, but has a higher residual disease risk (20-50%) and needs a second-look surgery. Canal wall down removes the canal wall, creates an open cavity that needs lifelong cleaning, but provides excellent disease clearance and is preferred for extensive disease or complications.
- When can I avoid second-look surgery after canal wall up mastoidectomy? If a diffusion-weighted MRI (DW-MRI) at 9 to 12 months post-surgery shows no restricted diffusion, you can avoid second-look surgery because the negative predictive value is 92 to 95% for residual cholesteatoma larger than 2mm.
- What are the red flag signs that suggest complications in COM? Pain, vertigo (especially with a positive fistula test), persistent headache, facial weakness, fever with neck rigidity, listlessness in a child, ataxia, and diplopia are all red flags that require immediate investigation and intervention.
———— End ————
Download the full PDF Link:
Chronic Suppurative Otitis Media Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Chronic suppurative otitis media PPT, Chronic suppurative otitis media in adults, CSOM treatment guidelines, Natural remedies for chronic ear discharge, Causes of chronic ear infections, Complications of chronic suppurative otitis media, Chronic ear infection surgical options, Chronic ear discharge in children, Hearing loss due to chronic ear infections, Chronic middle ear infection symptoms, Chronic otitis media home management, Understanding Chronic Suppurative Otitis Media in Adults: Causes and Treatment Options, CSOM Treatment Guidelines: Medical and Surgical Management Explained, How Chronic Suppurative Otitis Media Affects Hearing: What You Need to Know, Complications of CSOM: Preventing Serious Middle Ear Infections, Natural Remedies for Chronic Suppurative Otitis Media: Do They Work?, Chronic Ear Discharge in Children: Causes, Symptoms, and Management, Surgical Solutions for Chronic Ear Infections: What Are Your Options?, Preventing Hearing Loss Due to Chronic Suppurative Otitis Media, Recognizing the Symptoms of Chronic Middle Ear Infections, Home Care Tips for Managing Chronic Suppurative Otitis Media”Tubotympanic, Atticoantral, Tympanosclerosis, Cholesteatoma, Osteitis and Granulation Tissue, Cholesterol Granuloma, Mucosal disease, Squamosal disease
Very nicely explained
Very nice read for scholars. MBBS easy notes.