|
The following CBME core competencies are covered in this chapter.
|
Otalgia
Otalgia, or ear pain, is a common symptom that can arise from pathologies within the ear (primary otalgia) or as referred pain from distant structures (referred otalgia). Understanding the sensory innervation of the ear and the potential sources of referred pain is crucial for accurate diagnosis and management.
Primary Otalgia
Primary otalgia results from direct stimulation of sensory nerves supplying the ear. The ear receives sensory innervation from:
- Greater auricular nerve (C2, C3).
- Lesser occipital nerve (C2, C3).
- Auriculotemporal nerve (V3).
- Facial nerve (VII).
- Jacobson’s nerve (branch of glossopharyngeal nerve, IX).
- Arnold’s nerve (auricular branch of the vagus nerve, X).

Causes of Primary Otalgia
- Pinna: Trauma, cellulitis, herpes zoster oticus, malignancy, chronic relapsing perichondritis, chondrodermatitis nodularis helicis.
- External Auditory Canal (EAC): Otitis externa (acute, chronic, malignant), furuncle, keratosis obturans, herpes zoster oticus, malignancy, bullous myringitis.
- Middle Ear: Otitis media, malignancy.
- Inner Ear: Noise-induced injury.

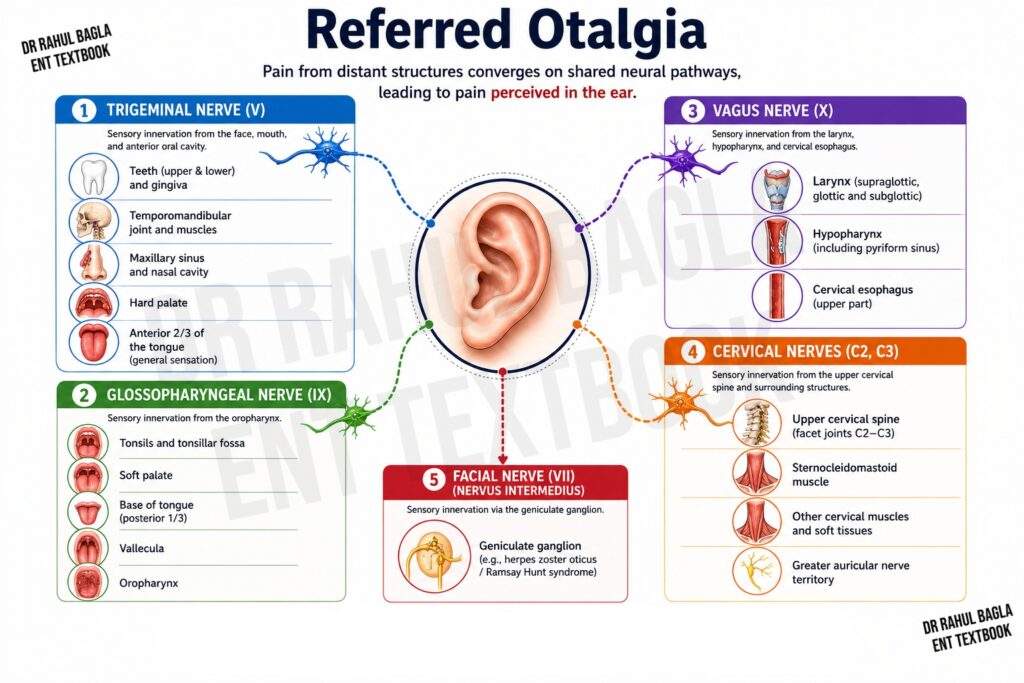
Referred Otalgia
Referred otalgia occurs when pain from distant structures is perceived in the ear due to shared neural pathways. The nerves involved include:
1. Trigeminal Nerve (V)
Supplies the anterior two-thirds of the tongue, floor of the mouth, palate, lower teeth, salivary glands, temporomandibular joint (TMJ), and mandible.
- Site of Perception: Pinna, tragus, anterior wall of EAC.
- Causes: Dental caries, impacted molars, tongue malignancy, TMJ osteoarthritis, ill-fitting dentures, parotid infections.
2. Glossopharyngeal Nerve (IX)
Supplies the posterior third of the tongue, tonsils, nasopharynx, hypopharynx, and parapharyngeal space.
- Site of Perception: Deep ear pain, middle ear, Eustachian tube.
- Causes: Acute tonsillitis, peritonsillar abscess, base of tongue or tonsillar malignancy, Eagle syndrome, parapharyngeal abscess.
3. Vagus Nerve (X)
Supplies the valleculae, supraglottis, thyroid gland, tracheobronchial tree, and esophagus.
- Site of Perception: Inferior and posterior EAC.
- Causes: Malignancy of supplied structures, thyroiditis.
4. Upper Cervical Nerves (C2, C3)
Supply the cervical spine muscles and facet joints.
- Site of Perception: Posterior pinna, skin over mastoid.
- Causes: Cervical spondylitis, spinal stenosis, osteoarthritis.
Temporomandibular Joint (TMJ) Dysfunction Syndrome
- Characteristics: Diffuse pain around the TMJ, crepitus, trismus.
- Predisposition: More common in females; bruxism is a key etiological factor (present in 50% of cases).
- Clinical Findings: Tenderness of the lateral pterygoid muscles (present in approximately 85% of patients) is the most reliable clinical finding and can be confirmed by intraoral palpation. Tenderness of the medial pterygoid muscle may also be present.
- Signs of Bruxism: Flattened occlusal surfaces of the molars, worn incisors, linear scarring of the buccal mucosa, and linear scarring along the lateral border of the tongue.
- Treatment: Soft diet, hot fomentation, muscle relaxants.
Costen Syndrome (TMJ Neuralgia)
Pathophysiology: Hypertonia of the muscles of mastication causes referred pain to the ear and adjacent head and neck regions.
Symptoms: Ear pain, tinnitus, dizziness, and aural congestion.
Treatment:
- Rest, soft diet, and non-steroidal anti-inflammatory drugs (e.g., ibuprofen or diclofenac).
- Muscle relaxants may be useful for reducing muscle spasm.
- Benzodiazepines or low-dose tricyclic antidepressants may be considered in refractory cases.
- Occlusal splints are useful in selected patients. Surgical treatment (condylotomy) is reserved only for patients who fail conservative treatment.
Glossopharyngeal Neuralgia
Characteristics: Severe, transient pain in the ear, base of the tongue, tonsillar fossa, or below the jaw.
Types:
- Tympanic type: Ear pain.
- Oropharyngeal type: Oropharyngeal pain
Triggers: Swallowing, coughing, yawning, talking.
Cause: In most patients, no structural lesion is identified. The commonest cause is vascular compression of the glossopharyngeal nerve by the posterior inferior cerebellar artery (PICA).
Treatment:
- First-line: Carbamazepine.
- Surgical: Microvascular decompression or nerve section (posterior fossa, neck, or transtonsillar approach).
Eagle’s Syndrome (Styalgia)
Cause: The normal styloid process measures approximately 2.5 cm and is considered elongated when it exceeds 4 cm. Elongation usually results from ossification or calcification of the stylohyoid ligament. Symptoms are thought to result from irritation of the glossopharyngeal nerve, impingement of the carotid vessels, or inflammation at the insertion of the stylohyoid ligament.
Symptoms: Dull throat pain radiating to the ear, odynophagia, foreign body sensation.
Diagnosis: The elongated styloid process may be palpable in the tonsillar fossa. Temporary relief of pain following local anaesthetic infiltration into the tonsillar fossa supports the diagnosis. Confirmation is by X-ray skull, orthopantomogram (OPG), or CT scan.
Management:
- Conservative: Analgesics or NSAIDs, local anaesthetic injection, and neuropathic pain medications (e.g., carbamazepine) in selected patients.
- Surgical: Transoral or transcervical styloidectomy is the definitive treatment for persistent symptoms.
Clinical Pearl
Persistent unilateral otalgia with a normal otoscopic examination should always raise suspicion of an occult head and neck malignancy until proven otherwise. A complete examination of the oral cavity, oropharynx, hypopharynx, larynx, temporomandibular joint, cranial nerves, and neck should be performed, with flexible nasopharyngolaryngoscopy when indicated.
Red Flags in Otalgia
Consider occult head and neck malignancy in patients with:
- Persistent unilateral otalgia
- Normal ear examination despite severe pain
- Associated dysphagia or odynophagia
- Hoarseness
- Neck swelling
- Weight loss
- History of smoking or alcohol use
Psychogenic Causes
When no organic cause is identified, otalgia may be psychogenic. Patients should be monitored and periodically re-evaluated to rule out underlying pathology.
———— End of the chapter ————
Download the full PDF Link:
Otalgia Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords:Otalgia, Costen syndrome, Glossopharyngeal Neuralgia, Temporomandibular Joint (TMJ) Dysfunction Syndrome, Ear pain causes, Ear pain treatment, Ear pain diagnosis, Referred ear pain, Primary otalgia, Referred otalgia, Ear pain and TMJ, Ear pain and dental issues, Ear pain and sinus infection, Why does my ear hurt? Ear pain without infection, Ear pain and jaw pain, Ear pain and throat pain, Ear pain and headache, Sharp ear pain Dull ear pain, Ear pain when swallowing, Ear pain and tinnitus, Ear pain and dizziness, Otalgia and glossopharyngeal neuralgia, Otalgia and Eagle’s syndrome, Otalgia and temporomandibular joint disorder, Otalgia and ear infection, Otalgia and sinusitis, Ear pain in adults, Ear pain in children, Ear pain during pregnancy, Ear pain after flying, Ear pain after swimming