|
The following CBME core competencies are covered in this chapter.
|
Benign and Intermediate Tumours of Nose and Paranasal Sinuses
Introduction
Sinonasal tumours present one of the most challenging topics in otorhinolaryngology because their early symptoms mimic chronic rhinosinusitis so closely. Consequently, we often diagnose these neoplasms late, typically with a delay of six to eight months after symptom onset. Therefore, every otorhinolaryngologist must maintain a high index of suspicion for these tumours, especially when a patient presents with unilateral persistent nasal symptoms.
Epidemiology and Clinical Significance
Sinonasal tumours account for less than 3% of all aerodigestive tract tumours. Despite their rarity, they carry significant morbidity and mortality because patients present late, and the anatomical location makes complete surgical resection challenging. The annual incidence of sinonasal malignancies ranges from 0.5 to 1 case per 100,000 population worldwide. In India, these cancers constitute approximately 0.44% of all body cancers, with a slightly higher incidence in males (0.57%) compared to females (0.44%).
The maxillary sinus represents the most common site of origin for sinonasal malignancies, accounting for nearly 70% of cases. The ethmoid sinuses follow with 20% involvement, while the sphenoid and frontal sinuses contribute only 3% and 1%, respectively. This distribution pattern has significant clinical implications because maxillary sinus tumours produce distinct symptom complexes depending on their direction of spread.
Classification of Sinonasal Tumours
We broadly classify tumours of the nose and PNS as benign, intermediate (locally aggressive with malignant potential), and malignant. The table below summarises the most important entities.
| Category | Tumours / Examples |
| Benign | Epithelial tumours: Inverted papilloma, Pleomorphic adenoma Mesenchymal tumours: Osteoma, Haemangioma, Fibroma, Chondroma, Juvenile nasal angiofibroma, Ossifying fibroma Neural-related tumours: Schwannoma Other tumour-like lesions: Giant cell granuloma, Mucocele / Pyocele |
| Intermediate | Esthesioneuroblastoma Inverted papilloma Hemangiopericytoma Meningioma Oncocytoma Cylindroma |
| Malignant | Squamous cell carcinoma Tumours of minor salivary glands Sarcomas: Chondrosarcoma, Rhabdomyosarcoma Malignant melanoma Esthesioneuroblastoma (ENB) Lymphoreticular neoplasms Adenocarcinoma Undifferentiated carcinoma Basal cell carcinoma |
Note: Inverted papilloma appears in both benign and intermediate categories because it is histologically benign but behaves locally aggressively and carries a 5–15% risk of malignant transformation.
Benign Tumours of Nose and Paranasal Sinuses
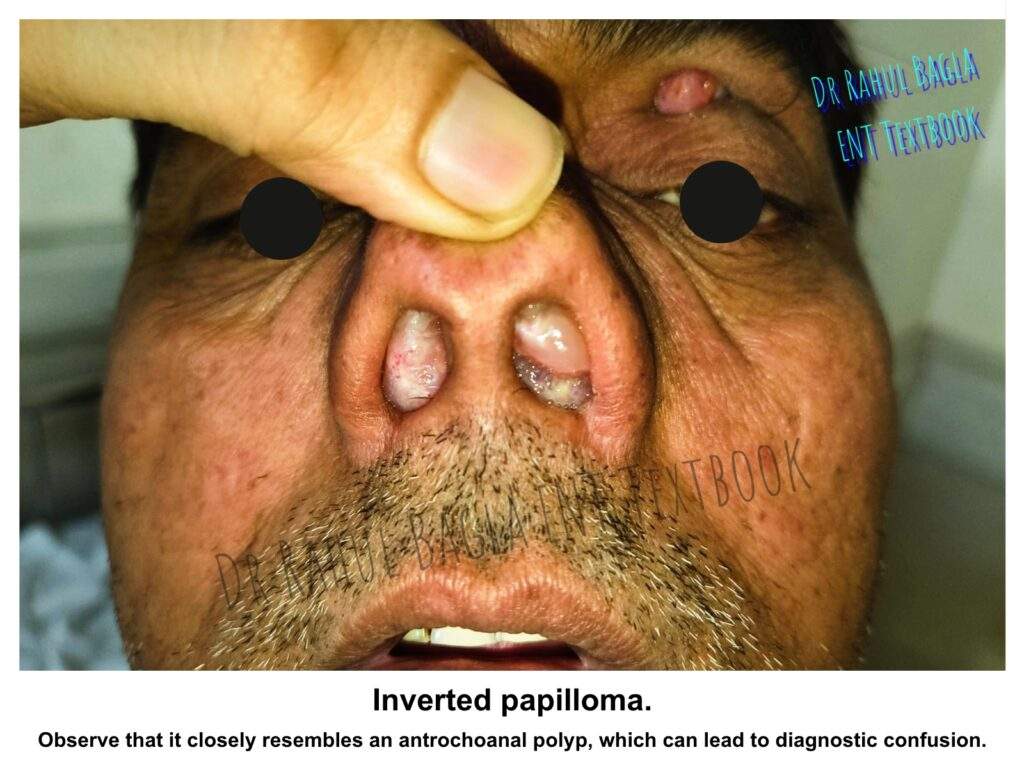
1. Inverted Papilloma
Inverted papilloma represents the most clinically significant benign epithelial tumour of the sinonasal tract because it behaves locally aggressively and carries a definite risk of malignant transformation. Other names for this tumour include Ringertz tumour, Schneiderian papilloma, transitional cell papilloma, Ewing’s papilloma, villiform cancer, and papillary sinusitis. However, the term “inverted papilloma” remains most widely used because it accurately describes the characteristic histological finding of epithelial invagination into the underlying stroma.
- Epidemiology and Aetiology. Inverted papilloma accounts for approximately 5% of all primary nasal tumours. The tumour shows a striking male predominance, with men affected four to five times more commonly than women. The peak incidence occurs between the fifth and seventh decades of life, making this distinctly a middle-aged to elderly patient’s disease.
- Human papillomavirus (HPV), particularly subtypes 6 and 11, appears to play a significant aetiological role. Additionally, some studies have implicated HPV subtypes 16 and 18 in those cases showing malignant transformation. Despite this viral association, inverted papilloma does not behave like a typical viral wart and requires complete surgical excision.
- Clinical Presentation. The most common site of origin for inverted papilloma is the lateral nasal wall, specifically in the region of the middle meatus. From this location, the tumour can extend into the maxillary sinus, ethmoid sinus, frontal sinus, and sphenoid sinus. Less commonly, the tumour arises from the nasal septum.
- Patients typically present with unilateral nasal obstruction as the dominant symptom. This obstruction progressively worsens over time because the tumour grows steadily. Unilateral rhinorrhoea, often blood-stained, represents the second most common complaint. Epistaxis occurs frequently because the tumour is vascular and friable. Facial pain and headache develop when the tumour obstructs sinus ostia, producing secondary sinusitis or mucocele formation. Epiphora may occur if the tumour extends into the nasolacrimal duct region.
- Examination. On anterior rhinoscopy or nasal endoscopy, you will see a fleshy, pinkish-grey mass with a smooth to lobulated surface. The appearance strikingly resembles a simple nasal polyp, and herein lies the diagnostic trap. Therefore, any unilateral nasal polyp in a middle-aged or elderly patient must raise suspicion for inverted papilloma until proven otherwise by histopathological examination.
- Histopathological Features. Grossly, inverted papillomas appear grey to pink and show a friable, polypoidal consistency. The diagnostic histological feature is the inverted growth pattern, where the surface epithelium grows downward into the underlying connective tissue stroma rather than outward in an exophytic manner. The epithelium is typically thickened, squamous or transitional type, and you may see mucous cysts or microabscesses within the epithelium. Approximately five to 15% of cases show foci of squamous cell carcinoma within the tumour, which is why we consider this an intermediate-grade neoplasm despite its benign histological appearance.
Imaging and Biopsy
- CT scan: Shows a homogeneous soft tissue mass with bony remodelling (not destruction) and possible sclerosis of the adjacent bone. It helps to plan surgery.
- MRI: Better delineates the tumour from retained secretions and detects intracranial or orbital extension. On T2-weighted images, the tumour shows a characteristic “convoluted cerebriform” pattern.
- Biopsy: Perform a preoperative biopsy to confirm the diagnosis. However, be cautious because the tumour is vascular, and bleeding can be brisk.
Treatment – Surgical Excision is the Gold Standard
Complete surgical excision represents the only curative treatment for inverted papilloma. The fundamental principle guiding surgery is the complete removal of the tumour along with its mucosal attachment site because leaving any residual disease guarantees recurrence. The recurrence rate approaches 50% with incomplete excision but drops to less than 15% when we achieve complete removal.
Medial maxillectomy constitutes the standard surgical procedure for inverted papilloma arising from the lateral nasal wall. This operation removes the entire medial wall of the maxillary sinus along with the tumour attachment site. We can perform medial maxillectomy through three main approaches.
- Endoscopic endonasal approach – The endoscopic endonasal approach has become the preferred method for most cases because it avoids external incisions, reduces postoperative morbidity, and provides excellent visualisation when performed with modern instrumentation. This approach works well for tumours limited to the nasal cavity, maxillary sinus medial wall, and ethmoid sinuses.
- Lateral rhinotomy – The lateral rhinotomy approach provides wide external exposure for larger tumours or those extending into the frontal sinus, orbit, or anterior cranial fossa. This incision extends from the medial canthus along the nasofacial groove and can be extended as needed.
- Midfacial degloving – The midfacial degloving approach combines excellent exposure with no external scar. The surgeon raises the facial soft tissues through bilateral sublabial incisions, exposing the entire midface skeleton. This approach works particularly well for bilateral disease or when we need access to both nasal cavities and maxillary sinuses simultaneously.
Important clinical point: Radiotherapy has no role in treating inverted papilloma because it does not eradicate the tumour and may actually induce malignant transformation. Therefore, we reserve radiation only for cases with associated malignancy that cannot be surgically resected.
Prognosis and Follow-up
Even after complete excision, inverted papilloma shows a recurrence rate of 10-15%. Recurrences typically appear within two to three years after surgery, but can occur even after ten years. Therefore, patients require long-term endoscopic surveillance, typically every six to twelve months, for at least five years. Malignant transformation occurs in 5-15% of cases, either at presentation or during recurrence. When malignancy coexists, the prognosis depends entirely on the stage and grade of the carcinomatous component.
2. Osteoma
Osteoma represents the most common benign tumour of the paranasal sinuses, with a particular predilection for the frontal sinus. These slow-growing bony tumours arise from the membranous elements of the skull and typically remain asymptomatic for many years.
- Site Distribution. Frontoethmoidal osteomas account for 95% of all sinus osteomas. The frontal sinus alone is involved in approximately 70% of cases, while the ethmoid sinuses are involved in 20-30%. Maxillary sinus osteomas occur in less than 5% of cases, and sphenoid sinus involvement is exceedingly rare.
- Clinical Presentation. Small osteomas are mostly asymptomatic and found incidentally on X-ray. When symptomatic, frontal headache (due to obstruction of the frontal sinus drainage) is the most common complaint. Large osteomas can cause facial pain, proptosis, diplopia, or even a visible forehead bossellation. Proptosis occurs from direct mass effect, while diplopia results from extraocular muscle impingement. Epiphora may develop from nasolacrimal duct obstruction. Cosmetic bosselation or visible forehead swelling can occur with large frontal sinus osteomas that expand the anterior table. The peak incidence occurs between the third and fourth decades of life
- Radiology. CT scan shows a well-defined, dense, homogenous mass with smooth borders. It is the investigation of choice to assess the size and relation to the skull base and orbit.
Treatment
- Asymptomatic small osteomas – No treatment; only follow-up with periodic serial imaging.
- Symptomatic or enlarging osteomas – Surgical removal. Indications include: tumour extending beyond the frontal sinus, causing chronic sinusitis, orbital/intracranial involvement, or persistent headache. Surgical approaches include endoscopic removal (for ethmoid, frontal recess or small frontal osteomas) and external approach osteoplastic frontal sinusotomy, which raises the anterior table of the frontal sinus as a bony flap, providing excellent exposure of the entire sinus cavity (for large frontal sinus osteomas). Combined endoscopic and external approaches may be necessary for very large or complex osteomas that extend beyond the sinus confines.
3. Nasal Hemangioma
Haemangioma represents a benign vascular tumour consisting of blood vessels embedded in connective tissue stroma.
Radiology. Contrast-enhanced CT shows a strongly enhancing mass without bony erosion (differentiates it from malignancy).
Types and Treatment
- Capillary haemangioma (bleeding polyp of the septum): Arises from the anterior part of the nasal septum (Little’s area). The tumour appears as a soft, dark red, pedunculated or sessile mass that bleeds profusely with minimal trauma. Do not biopsy a suspected haemangioma in the clinic because it can cause severe haemorrhage. Treatment consists of complete local excision with a cuff of surrounding mucoperichondrium to prevent recurrence. We can achieve this endoscopically for most cases. Preoperative embolisation is rarely necessary for such small lesions. However, we must control bleeding during surgery using cautery or laser ablation.
- Cavernous haemangioma: Cavernous haemangioma arises from the turbinates on the lateral nasal wall rather than from the septum. This tumour consists of large, dilated, thin-walled vascular spaces and appears as a bluish, compressible mass. Patients present with nasal obstruction and epistaxis, but the bleeding is typically less dramatic than with capillary haemangioma. Treatment requires surgical excision, but we often employ preliminary cryotherapy or laser photocoagulation to reduce vascularity before excision. Extensive lesions may require preoperative embolisation followed by surgical removal. Radiotherapy has a limited role for cavernous haemangiomas that cannot be completely excised.
- Mixed type: Contains both capillary and cavernous elements.
4. Pleomorphic Adenoma
Pleomorphic adenoma, the most common tumour of the major salivary glands, rarely occurs in the nasal cavity. When it does occur, the nasal septum represents the most common site of origin from the minor salivary glands present in the submucosa. Clinically, pleomorphic adenoma presents as a firm, painless, slow-growing mass causing unilateral nasal obstruction. The tumour typically appears smooth and rounded on examination. Because these tumours have a pseudocapsule and can recur if incompletely excised, wide surgical excision with clear margins represents the treatment of choice. Endoscopic excision works well for smaller tumours, while larger lesions may require lateral rhinotomy.
5. Chondroma
Pure chondromas arising from the nasal cavity, ethmoid sinuses, or nasal septum are rare tumours. They appear smooth, firm, and lobulated. More commonly, we see mixed tumours such as fibrochondroma, osteochondroma, or angiochondroma. The clinical significance of chondroma lies in its tendency for malignant transformation to chondrosarcoma after repeated surgical intervention. Therefore, we perform wide excision for recurrent or large tumours rather than repeated limited excisions. Complete surgical removal with clear margins offers the best prognosis.
6. Schwannoma
Schwannoma, also called neurilemmoma, arises from Schwann cells of the nerve sheath and represents an uncommon benign neoplasm in the sinonasal tract. The tumour can involve the ethmoid, maxillary, or sphenoid sinuses, as well as the nasal cavity proper. Clinically, a schwannoma presents as a rounded, firm mass that may show a yellowish colour with visible blood vessels coursing over its surface. Despite being benign, the tumour can cause pressure necrosis of the surrounding bone as it expands. CT and MRI help define the tumour’s extent, but histopathological examination of a biopsy specimen provides the definitive diagnosis.
Complete surgical excision offers a cure, and we can remove most schwannomas endoscopically. However, large tumours involving critical structures may require external approaches.
7. Juvenile nasopharyngeal angiofibroma
8. Meningioma
Primary extranasal meningioma can occur in the nose; treat by lateral rhinotomy.
Intermediate Tumours of Nose and Paranasal Sinuses
Understanding the Intermediate Category
The intermediate category includes tumours that are histologically benign but demonstrate locally aggressive behaviour, have a definite risk of malignant transformation, or both.
1. Esthesioneuroblastoma (Olfactory Neuroblastoma)
Esthesioneuroblastoma arises from the olfactory epithelium in the upper third of the nasal cavity and cribriform plate region. This tumour shows a bimodal age distribution, with peaks occurring at ten to twenty years and again at fifty to sixty years.
- Clinical Presentation. Patients typically present with unilateral nasal obstruction and epistaxis. Orbital invasion produces proptosis, diplopia, and blurred vision. Intracranial extension through the cribriform plate causes headache and may eventually produce neurological deficits. Cervical lymph node metastases occur in 10-15% of patients at presentation.
- Examination. On endoscopic examination, you will see a friable, cherry-red or greyish, polypoidal mass occupying the superior nasal cavity. Because the tumour is highly vascular, a biopsy without prior imaging carries a significant risk of severe bleeding. Therefore, always obtain a CT scan or MRI before attempting a biopsy.
- Radiological Features. High-resolution CT scan shows the tumour’s extent and may demonstrate destruction or erosion of the cribriform plate, fovea ethmoidalis, or orbital walls. Calcifications within the tumour may be visible. MRI with gadolinium enhancement better defines intracranial extension and dural involvement. The tumour typically shows an intermediate signal on T1-weighted images and enhances intensely with contrast.
- Histopathology. Low-grade tumours show formation of pseudorosettes (Flexner-Wintersteiner rosettes) and Homer-Wright rosettes. High-grade tumours demonstrate nuclear pleomorphism, mitotic figures, and necrosis without rosette formation. Immunohistochemistry helps differentiate this tumour from lymphoma, melanoma, rhabdomyosarcoma, and undifferentiated carcinoma. Esthesioneuroblastoma stains positively for neuron-specific enolase, synaptophysin, and chromogranin.
- Treatment. Craniofacial resection followed by adjuvant radiation represents the standard approach for most patients. For advanced lesions extending into the orbit, cribriform plate, or intracranially, preoperative chemotherapy and radiation followed by craniofacial resection may improve outcomes. Cervical lymph node metastases, when present, require neck dissection and postoperative radiation to the neck. The prognosis depends on tumour grade, extent at presentation, and completeness of surgical resection.
2. Other Intermediate Tumours of Nose and Paranasal Sinuses
- Inverted papilloma (discussed above – 5–15% malignant transformation).
- Haemangiopericytoma – Arises from pericytes (capillary surrounding cells). Patients present with epistaxis. Histology cannot predict behaviour; treat by wide local excision.
- Oncocytoma – Rare, from oncocytes of seromucinous glands.
- Cylindroma (adenoid cystic carcinoma-like but less aggressive) – Actually, most authorities now classify adenoid cystic carcinoma as malignant; this is a historical term.
—-End of the Chapter—-
High-Yield Points
- Inverted papilloma is benign but locally aggressive and shows 5–15% malignant transformation.
- Unilateral nasal polyp in an older patient strongly suggests inverted papilloma.
- MRI inverted papilloma shows a convoluted cerebriform pattern.
- Medial maxillectomy (endoscopic preferred) is standard surgery for inverted papilloma.
- Osteoma is the most common benign tumour of the PNS, and the frontal sinus is the most common site.
- JNA occurs in adolescent males, causes profuse recurrent epistaxis, and arises near the sphenopalatine foramen.
- Holman-Miller sign is the anterior bowing of the posterior maxillary wall due to JNA extension.
- Never biopsy JNA because catastrophic bleeding can occur.
- Esthesioneuroblastoma arises from the olfactory epithelium and causes obstruction + epistaxis + anosmia.
- Sinonasal tumour red flag: unilateral symptoms + bleeding + non-response to treatment.
NEET PG Style MCQs
- The most common site of origin of inverted papilloma is: A. Nasal septum B. Lateral nasal wall near middle meatus C. Inferior turbinate D. Nasopharynx
- MRI finding most characteristic of inverted papilloma is: A. Sunburst pattern B. Onion peel appearance C. Convoluted cerebriform pattern D. Ground-glass appearance
- Malignant transformation rate of inverted papilloma is approximately: A. 1–2% B. 5–15% C. 25–30% D. 40–50%
- Juvenile nasopharyngeal angiofibroma typically occurs in: A. Elderly females B. Adolescent males C. Children of both sexes D. Middle-aged smokers
- Holman-Miller sign is classically associated with: A. Osteoma B. Nasal haemangioma C. JNA D. ENB
- The most common sinus involved in osteoma is: A. Maxillary sinus B. Ethmoid sinus C. Frontal sinus D. Sphenoid sinus
- The correct management of suspected JNA is: A. OPD biopsy followed by surgery B. Steroid trial followed by biopsy C. CT/MRI + angiography + embolisation + surgery D. Radiotherapy as first line
- Esthesioneuroblastoma arises from: A. Maxillary sinus mucosa B. Olfactory epithelium C. Nasopharyngeal tonsil D. Inferior turbinate mucosa
- The most common presenting symptom of inverted papilloma is: A. Facial swelling B. Anosmia C. Unilateral nasal obstruction D. Neck node enlargement
- Which tumour is most strongly associated with severe epistaxis on minimal touch? A. Osteoma B. Pleomorphic adenoma C. Capillary haemangioma D. Schwannoma
Answers
A1. B – Most inverted papillomas arise from the lateral nasal wall near the middle meatus.
A2. C – Cerebriform pattern on MRI is highly suggestive of inverted papilloma.
A3. B – Malignant transformation occurs in about 5–15%.
A4. B – JNA occurs almost exclusively in adolescent males.
A5. C – Holman-Miller sign is due to JNA expansion into the pterygopalatine fossa.
A6. C – Frontal sinus is the commonest site of osteoma.
A7. C – Imaging and embolisation are mandatory before surgery due to vascularity.
A8. B – ENB originates from the olfactory neuroepithelium in the superior nasal cavity.
A9. C – Unilateral progressive obstruction is the commonest symptom.
A10. C – Capillary haemangioma (bleeding polyp) bleeds profusely even with minor trauma.
Frequently Asked Questions in Viva
- Q: What is the most common benign tumour of paranasal sinuses? A: Osteoma, especially of the frontal sinus.
- Q: Why is an inverted papilloma clinically important? A: It recurs frequently and has 5–15% risk of malignant transformation.
- Q: What is the hallmark MRI feature of inverted papilloma? A: Convoluted cerebriform pattern on T2-weighted MRI.
- Q: Why should JNA not be biopsied? A: It is highly vascular, and a biopsy can cause life-threatening bleeding.
- Q: What is the Holman-Miller sign? A: Anterior bowing of the posterior wall of the maxillary sinus due to JNA spread into the pterygopalatine fossa.
- Q: What is the common origin site of JNA? A: Posterolateral wall of the nasopharynx near the sphenopalatine foramen.
- Q: What is the typical symptom triad of JNA? A: Nasal obstruction, recurrent epistaxis, and nasopharyngeal mass.
Clinical Case-Based Questions (Practical + Viva)
- Case 1. A 16-year-old boy presents with recurrent profuse epistaxis and unilateral nasal obstruction. Endoscopy shows a reddish lobulated mass in the nasopharynx. Q: Most likely diagnosis and next step? Answer: Juvenile nasopharyngeal angiofibroma. The next step is CT/MRI and angiography, followed by embolisation and surgical excision.
- Case 2. A 58-year-old man had unilateral nasal obstruction and blood-stained discharge for 8 months. Endoscopy shows a polypoidal mass in the middle meatus. Q: Most likely diagnosis and management? Answer: Inverted papilloma. Confirm by biopsy and treat with complete endoscopic excision/medial maxillectomy.
- Case 3. A 35-year-old patient has a chronic frontal headache. CT scan shows a dense bony mass in the frontal sinus. Q: Diagnosis and treatment plan?m Answer: Osteoma. Observe if small and asymptomatic. Remove surgically if symptomatic/enlarging.
- Case 4. A 55-year-old patient has unilateral nasal obstruction with anosmia and epistaxis. MRI shows a superior nasal cavity mass with cribriform plate erosion. Q: Diagnosis and treatment? Answer: Esthesioneuroblastoma. Treat with craniofacial resection and radiotherapy ± chemotherapy.
—-End—-
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Benign and intermediate tumours of the nose and paranasal sinuses (PNS) are uncommon but clinically important because they often mimic chronic rhinosinusitis and nasal polyposis. Therefore, many patients present late, and clinicians may initially miss the diagnosis. However, early suspicion and correct evaluation can prevent complications such as orbital spread, intracranial extension, recurrent disease, and malignant transformation.Sinonasal tumours remain challenging because the sinonasal region has complex anatomy, narrow drainage pathways, and close proximity to the orbit, skull base, and cranial nerves. Consequently, even histologically benign tumours can behave aggressively and cause significant morbidity. Benign sinonasal tumours notes, Intermediate sinonasal tumours summary, Inverted papilloma MBBS notes, Inverted papilloma NEET PG MCQs, Juvenile nasopharyngeal angiofibroma JNA notes, JNA staging and management, Holman Miller sign explanation, Osteoma frontal sinus notes, Osteoma paranasal sinus CT findings, Sinonasal haemangioma diagnosis and treatment, Bleeding polyp of nasal septum capillary haemangioma, Cavernous haemangioma turbinate management, Pleomorphic adenoma nasal septum ENT, Schwannoma of nose and paranasal sinuses, Chondroma nasal cavity and malignant transformation, Esthesioneuroblastoma olfactory neuroblastoma notes, Esthesioneuroblastoma CT MRI findings, Sinonasal tumour differential diagnosis unilateral nasal mass, Unilateral nasal obstruction causes ENT, CBME ENT sinonasal tumours, Sinonasal tumour viva questions, Sinonasal tumour exam guide MBBS, Sinonasal tumours high yield revision, Sinonasal tumours flowchart and mnemonics, Endoscopic medial maxillectomy inverted papilloma, Endoscopic surgery for sinonasal tumours notes, Sinonasal tumour imaging CT vs MRI, How to approach unilateral nasal mass, Nose and PNS tumours NEET PG questions, ENT rhinology tumour notes India,