|
The following CBME core competencies are covered in this chapter.
|
Physiology of the Nose and Paranasal Sinuses
The nose is an essential organ that performs a variety of physiological functions crucial for respiration, protection, and sensory perception. Its role extends beyond a mere passage for air to the lungs, encompassing air conditioning, protection of lower airways, vocal resonance, reflex actions, and olfaction. These functions work harmoniously to ensure optimal respiratory and sensory performance.
Functions of the Nose and Paranasal Sinuses
The primary functions of the nose are classified as follows:
- Respiration
- Air-conditioning of Inspired Air
- Protection of the Lower Airway
- Vocal Resonance
- Nasal Reflex Functions
- Somatic Sensation
- Olfaction
Respiration.
The nose serves as the natural pathway for breathing, an instinctive function critical for life. Mouth breathing is an acquired act that can compromise respiratory efficiency. For instance, a newborn with choanal atresia – a blockage of the nasal airway – can experience life-threatening asphyxiation if not treated promptly. The nose also facilitates simultaneous breathing and eating. A healthy adult normally breathes about 12–24 times a minute and inhales around 10,000 litres of air in a day at different temperatures, humidity, with dust and microorganisms.
1. Mechanism of Respiration
- Inspiration: During quiet breathing, air flows through the middle part of the nose, passing between the turbinates and the nasal septum. Minimal air passes through the inferior meatus or olfactory region, requiring substances with weak odours to be actively sniffed to reach the olfactory area.
- Expiration: Air exits through the same pathway, but forms eddies due to resistance at the limen nasi. This eddy formation ventilates the paranasal sinuses through their openings, ensuring proper aeration. The anterior end of the inferior turbinate undergoes swelling and shrinkage, thus regulating the inflow of air.

2. Nasal Cycle: The nasal mucosa undergoes rhythmic congestion and decongestion, known as the nasal cycle, which alternates airflow between the two nasal chambers. This cycle typically spans 2.5–4 hours and ensures efficient respiratory function even if one nasal passage is partially blocked.
Air-Conditioning of Inspired Air.
The nasal mucosa undergoes rhythmic congestion and decongestion, known as the nasal cycle, which alternates airflow between the two nasal chambers. This cycle typically spans 2.5–4 hours and ensures efficient respiratory function even if one nasal passage is partially blocked.
1. Filtration and Purification
- Nasal Vibrissae: The small hairs at the entrance of the nose trap large particles up to 3 μm, such as cotton fibres.
- Mucus Layer: A mucus blanket on the nasal mucosa traps finer particles like dust, pollen, and bacteria. This filtering system is highly efficient, trapping particles as small as 0.5 microns in diameter. Particles smaller than 0.5 μm pass easily through the nose into the lower airways.
2. Temperature Regulation: The nasal mucosa, especially near the middle and inferior turbinates and adjacent parts of the septum, is highly vascular with cavernous venous spaces or sinusoids. It controls the blood flow, and this increases or decreases the size of the turbinates. Blood flow in the venous sinusoids of the mucosa acts as a radiator system, warming cold air to near body temperature within milliseconds. This makes an efficient radiator system, warming cold air to near body temperature within milliseconds, from 20°C or 0°C or even at subzero temperatures to near body temperature (37°C). Similarly, hot air is cooled before reaching the lungs.
3. Humidification: Inspired air is humidified by water that evaporates from the nasal mucosa and raises the relative humidity of the inspired air to 75% or more. This ensures the air reaches the lungs at optimal moisture levels, preserving ciliary function and preventing respiratory infections. Moisture is crucial for keeping the ciliary epithelium healthy and functional. If the relative humidity drops to 50%, the ciliary function can stop within 8 to 10 minutes. This means that breathing dry air can increase the likelihood of respiratory tract infections. Each day, about 1 litre of water evaporates from the nasal mucosa to maintain these humidity levels.
Protection of the Lower Airway.
The nasal cavity employs several mechanisms to safeguard the lower respiratory tract from harmful dust particles, bacteria and viruses.
1. Mucociliary Mechanism and Clearance: The mucociliary mechanism in the nasal mucosa plays a vital role in trapping and clearing pathogens and particles from the air we breathe. The mucosa contains goblet cells and secretory glands that produce a mucous blanket, consisting of a superficial mucus layer and a deeper serous layer. This mucous blanket moves like a conveyor belt towards the nasopharynx. Cilia beat continuously, moving this blanket toward the nasopharynx at a speed of 5–10 mm per minute, clearing it every 10–20 minutes and removes 80% of the particles before the air reaches the pharynx. This process traps bacteria, viruses, and dust particles, preventing respiratory infections. The presence of turbinates increases the surface area for trapping particles. In mammals, cilia beat 10–20 times per second, with an effective stroke that pushes mucus forward and a recovery stroke that returns them to their original position. Conditions like immotile cilia syndrome (Kartagener Syndrome) can impair this function, leading to mucus buildup and chronic issues such as rhinosinusitis and bronchiectasis. Factors like drying, drugs, and pollutants can also affect ciliary movement.
2. Enzymes and immunoglobulins: Nasal secretions contain immunoglobulins (IgA, IgG, IgM and IgE) that provide immunity against infections. It also contains enzymes like lysozymes and lactoferrin, protective proteins such as complement, antigen-presenting cells and T and B lymphocytes in the mucosa.
3. Protective Reflexes: Sneezing expels foreign particles that irritate the nasal mucosa. This reflex, combined with a large flow of nasal secretions efficiently washes them out. The pH of these nasal secretions remains nearly constant at 7, which is optimal for the action of cilia and lysozyme. Changes in nasal pH, caused by infections or nasal drops, can significantly impair the functions of cilia and lysozyme. The nose performs its functions so efficiently that it filters, humidifies, and warms about 500 cubic feet of air every 24 hours. This process clears the air of dust, bacteria, and viruses before it reaches the lungs.
Vocal Resonance.
The nasal cavity serves as a resonating chamber for certain consonants during speech, such as “M,” “N,” and “NG.” When the nasal passage is blocked, these sounds become denasalized, i.e. M/N/NG are uttered as B/D/G, respectively. Conversely, velopharyngeal insufficiency may lead to hypernasal speech.
Nasal Reflexes.
The nasal mucosa initiates various reflex actions:
- Sneezing: Sneezing expels foreign particles that irritate the nasal mucosa.
- Salivation and Gastric Secretion: Smelling palatable food stimulates the secretion of saliva and gastric juices.
- Pulmonary Reflexes: Long-standing nasal obstruction (i.e., tonsil and adenoid hypertrophy) can increase pulmonary resistance leading to pulmonary hypertension or cor pulmonale. Surgical correction of nasal blockage often improves pulmonary function.
Somatic Sensation
While the olfactory region handles the sense of smell, the rest of the nasal cavity is responsible for a different set of sensations. This area is richly supplied by the ethmoidal branch of the trigeminal nerve (cranial nerve V), and it detects what we call somatic sensations—feelings like touch, temperature, and pain.
- The ethmoidal branch of the trigeminal nerve innervates the entire nasal cavity except the olfactory area, providing somatic sensations like pain and irritation.
- Strong substances such as ammonia and chilli powder stimulate this nerve, not the olfactory nerve, creating a sharp, protective response.
- This stimulation triggers protective reflexes: sneezing, lacrimation (tearing), and rhinorrhoea (runny nose) to expel or dilute the irritant.
- Clinically, this explains why ammonia should never be used to test smell—it tests trigeminal sensation, not olfaction.

Olfaction: The Sense of Smell
The human nose is an extraordinary sensory organ, capable of distinguishing more than 10,000 different odours. While our sense of smell is not as powerful as in many animals, it remains vital for detecting dangers like smoke or gas and is essential for the full enjoyment of food. This process begins in a specialised area of the nasal cavity known as the olfactory region.
The Olfactory Region:
Imagine looking into the nose; the olfactory region is located high up, occupying the roof of the nasal cavity, the upper part of the septum and the lateral wall. This area is distinct because a patch of yellowish-brown tissue lines it called the olfactory mucosa. This mucosa is relatively small, covering an area of only 2–4 cm², yet it houses approximately 10 million specialised olfactory receptor cells.
The olfactory mucosa has a unique structure designed to detect airborne chemicals. Its surface is covered by a thin layer of mucus, which is secreted by specialised Bowman’s glands. This mucus is crucial because it dissolves odorant molecules, allowing them to reach the receptor cells below.
The Olfactory Receptor Cells: The olfactory epithelium is composed of three main cell types:
- Receptor Cells: These are the primary sensory neurons for smell. They are bipolar, meaning they have two distinct processes. A dendrite (peripheral process) that extends to the surface of the epithelium. Its tip swells into a small knob from which several immotile cilia project into the mucus layer. These cilia are covered with receptor proteins that detect odorants. And another is an axon (central process) that travels in the opposite direction.
- Sustentacular Cells: These are supporting cells that provide structural and metabolic support to the receptor cells.
- Basal Cells: These are stem cells that can regenerate and replace damaged receptor cells.
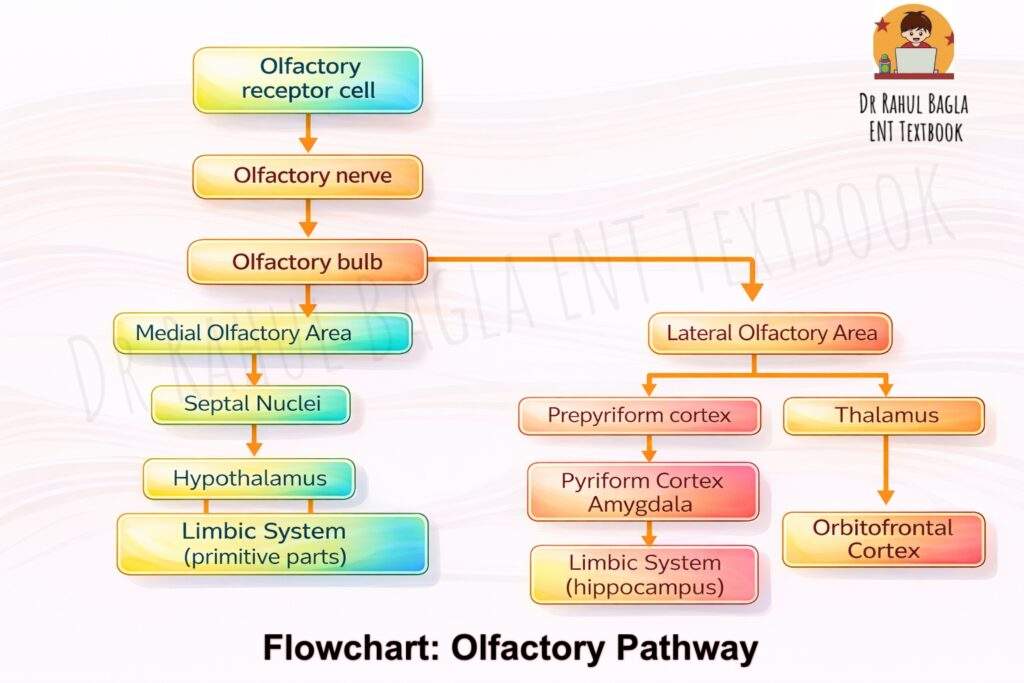
The Olfactory Pathway:
- Activation: Odorant molecules in the air dissolve in the mucus and bind to specific receptor proteins on the cilia of the receptor cells. This binding triggers a chemical reaction inside the cell, generating an electrical signal.
- The First Relay: The Olfactory Bulb: The axons of millions of receptor cells gather into small bundles that pass through tiny holes in the cribriform plate of the ethmoid bone. These bundles collectively form the olfactory nerves (Cranial Nerve I). They travel a short distance to the olfactory bulb, which sits just above the cribriform plate.
- Synapse and Convergence: Inside the olfactory bulb, the axons form connections, or synapses, with other neurons. They converge in spherical structures called glomeruli. It’s a highly organised system: about 25,000 receptor axons synapse with just 25 mitral cells in each glomerulus. This convergence ratio of 1000:1 helps amplify the signal.
- The Pathway to Consciousness: From the olfactory bulb, the axons of the mitral cells form the olfactory tract. This tract carries the smell information directly to higher brain centres, primarily the olfactory cortex. Unlike other senses, smell signals do not first pass through the thalamus. The key areas for conscious smell perception are the prepyriform cortex and the amygdaloid nucleus.
The Physiology of Smell: The intensity of a smell is directly related to the number of odorant molecules that bind to the receptor cells. The process is quite sophisticated:
- Molecular Binding: Odorant molecules first bind to special proteins in the mucus. This complex then binds to specific G protein-coupled receptors on the cilia.
- Signal Generation: This binding triggers a cascade of events that depolarises the receptor cell, generating an action potential if the stimulus is strong enough.
Important Note on Testing Smell: Ammonia vapours are not used to test the sense of smell. This is because ammonia also strongly stimulates the trigeminal nerve, causing a sensation of pain or irritation rather than a true smell.
Adaptation and Fatigue. Our sense of smell is designed to be sensitive to new stimuli, not to dwell on constant ones. This leads to:
- Adaptation: When exposed to the same odour continuously, we become less aware of it (e.g., not noticing your own perfume after a while). This is due to reduced sensitivity of the receptor cells.
- Cross-adaptation: This occurs when exposure to one odour reduces the ability to detect a different, but often related, odour.
Disorders of Smell.
For proper smell perception, the odorous substances must be volatile and reach the olfactory area without obstruction. Healthy olfactory mucosa and intact neural pathways are also necessary. To test the sense of smell, a patient can sniff common odours like lemon or peppermint with their eyes closed, one nostril at a time. More precise measurements require special equipment. Olfactory disorders encompass a range of conditions that affect the sense of smell. The following terms are commonly used to describe various olfactory dysfunctions:
- Anosmia is a total absence of smell function, and Hyposmia (or Microsmia) is a decreased sensitivity to odours, resulting in a diminished ability to perceive smell. These can occur due to nasal obstructions like polyps or swelling from conditions such as colds or allergies. Anosmia can also result from atrophic rhinitis, nerve injuries from head trauma, pressure from tumours or infections affecting the olfactory tract.
- Partial Anosmia: The patient can perceive some odours while being unable to detect others.
- Hyperosmia: The patient has an increased sensitivity to common odours, leading to an enhanced olfactory perception.
- Dysosmia (cacosmia or parosmia) is a distortion of smell where patients misinterpret odours, often finding them unpleasant. This can occur during recovery from anosmia and may indicate nerve fibre issues. Intracranial tumours should be ruled out in cases of parosmia.
- Phantosmia: This phenomenon involves the perception of a dysosmic sensation in the absence of an actual odour stimulus, commonly known as an olfactory hallucination.
- Olfactory Agnosia: Olfactory agnosia is characterised by an inability to recognise odour sensations despite intact olfactory processing, language capabilities, and general intellectual functions. This condition may be observed in certain stroke patients.
Additionally, several less commonly used terms describe specific olfactory phenomena:
- Heterosmia: A condition in which all odours are perceived as having the same scent.
- Presbyosmia: This term refers to a decline in the sense of smell associated with ageing. It is important to note that presbyosmia is less specific than other terms, as it does not differentiate between anosmia and hyposmia. Furthermore, it implies that age itself is the primary factor contributing to the age-related olfactory deficit.
- Osmophobia: Osmophobia denotes a dislike or fear of certain smells, which can significantly impact an individual’s quality of life.
——– End of the chapter ——–
High-Yield Points for Revision (NEET PG & University Exams)
- Nasal Cycle: Alternating congestion/decongestion, 2.5-4 hr duration, ensures efficient airflow.
- Choanal Atresia: Life-threatening in newborns due to obligate nasal breathing.
- Air-Conditioning: Nose warms (0°C to 37°C), humidifies (to >75% RH), and filters (>0.5μm particles).
- Ciliary Function: Stops if RH <50% for 8-10 mins, leading to increased infection risk.
- Mucociliary Clearance: Moves mucus 5-10 mm/min, clears blanket every 10-20 mins. Impaired in Kartagener Syndrome.
- Nasal Secretions: Contain lysozyme (antibacterial/antiviral) and IgA/IgE (immunity). Optimal pH 7.
- Vocal Resonance: Denasalization (M/N/NG to B/D/G) in nasal obstruction. Hypernasality in velopharyngeal insufficiency.
- Pulmonary Reflexes: Chronic nasal obstruction can lead to pulmonary hypertension/cor pulmonale.
- Olfactory Pathway: Olfactory receptor cells (bipolar neurons) -> Cribriform plate -> Olfactory bulb (glomerulus, mitral/tuft cells) -> Olfactory tract -> Prepyriform cortex/Amygdaloid nucleus.
- Ammonia Test: Stimulates the trigeminal nerve, not the olfactory receptors; avoid for smell testing.
- Anosmia: Total loss of smell.
- Dysosmia/Parosmia: Distortion of smell, often unpleasant. Rule out intracranial tumours in a new onset.
- Phantosmia: Olfactory hallucination (smell without stimulus).
Multiple Choice Questions (MCQs)
- Which of the following functions is primarily associated with the nasal cycle? a) Regulation of systemic blood pressure b) Alternating airflow between nasal chambers c) Secretion of digestive enzymes d) Control of pupil dilation
Answer: b) Alternating airflow between nasal chambers. Explanation: The nasal cycle involves rhythmic congestion and decongestion of the nasal mucosa, leading to alternating dominance of airflow between the two nostrils, which is crucial for efficient respiratory function. - A newborn presenting with severe respiratory distress that improves with crying should immediately raise suspicion for: a) Adenoid hypertrophy b) Bilateral choanal atresia, c) Nasal polyps d) Rhinitis medicamentosa
Answer: b) Bilateral choanal atresia. Explanation: Newborns are obligate nasal breathers. Choanal atresia, especially bilateral, blocks the nasal airway, causing severe distress that can temporarily improve when the baby cries (as the mouth opens for crying). - The mucociliary clearance mechanism in the nose is primarily responsible for clearing particles as small as: a) 50 μm b) 3 μm c) 0.5 μm d) 0.05 μm
Answer: c) 0.5 μm. Explanation: While nasal vibrissae trap larger particles (up to 3 μm), the mucus blanket and ciliary action are highly efficient in trapping finer particles down to 0.5 μm, protecting the lower airways. - Which enzyme found in nasal secretions plays a crucial role in destroying bacteria and viruses? a) Amylase b) Lipase c) Lysozyme d) Pepsin
Answer: c) Lysozyme. Explanation: Lysozyme (muramidase) is an antibacterial enzyme present in nasal secretions, contributing significantly to the nose’s protective functions against pathogens. - A patient with chronic nasal obstruction begins to develop a muffled speech quality, particularly when pronouncing ‘M’, ‘N’, and ‘NG’ sounds, which are perceived as ‘B’, ‘D’, and ‘G’, respectively. This phenomenon is known as: a) Hypernasality b) Denasalization c) Hoarseness d) Aphonia
Answer: b) Denasalization. Explanation: Denasalization occurs when nasal airflow is obstructed, preventing proper resonance for nasal consonants (M, N, NG), causing them to sound like their oral counterparts (B, D, G). - The conscious perception of smell occurs in which part of the olfactory pathway? a) Olfactory bulb b) Cribriform plate c) Prepyriform cortex d) Thalamus
Answer: c) Prepyriform cortex. Explanation: After processing in the olfactory bulb, olfactory signals are primarily transmitted to the prepyriform cortex (and amygdaloid nucleus), where conscious perception and interpretation of smells take place. - Which of the following conditions is characterised by the perception of a smell in the absence of an actual odour stimulus? a) Anosmia b) Hyposmia c) Dysosmia d) Phantosmia
Answer: d) Phantosmia. Explanation: Phantosmia refers to olfactory hallucinations, where an individual perceives an odor that is not actually present. - In Kartagener Syndrome, the triad of symptoms includes: a) Nasal polyps, asthma, eczema b) Chronic rhinosinusitis, bronchiectasis, situs inversus c) Otitis media, conductive hearing loss, cleft palate d) Epistaxis, headache, visual disturbances
Answer: b) Chronic rhinosinusitis, bronchiectasis, situs inversus. Explanation: Kartagener Syndrome is a primary ciliary dyskinesia characterised by this classic triad due to defective ciliary function. - What is the approximate relative humidity of inspired air achieved by the nose before it reaches the lungs? a) 25% b) 50% c) 75% or more d) 100%
Answer: c) 75% or more. Explanation: The nose efficiently humidifies inspired air, raising its relative humidity to 75% or more to prevent ciliary damage and maintain optimal lung function. - Prolonged breathing of dry air can lead to cessation of ciliary function within: a) 1-2 minutes b) 3-5 minutes c) 8-10 minutes d) 15-20 minutes
Answer: c) 8-10 minutes. Explanation: Ciliary function is highly sensitive to humidity; if the relative humidity drops to 50%, cilia can cease beating within 8-10 minutes, increasing susceptibility to respiratory infections.
Clinical Scenarios
Here are some clinically based questions to prepare you for practical exams and viva sessions.
- Scenario: A 5-day-old neonate presents with severe respiratory distress, especially during feeding, which improves when the baby cries. Physical examination reveals bilateral nasal obstruction.
- Questions: What is the likely diagnosis? How would you confirm it? What is the immediate management?
- Discussion Points (Viva): This classic presentation points towards bilateral choanal atresia. Confirmation involves attempting to pass a small feeding tube (e.g., 6 Fr) through each nostril, which will meet resistance. Nasal endoscopy or a CT scan with contrast (showing bony or membranous obstruction) can definitively diagnose it. Immediate management for severe distress includes inserting an oral airway (McGill catheter) to secure breathing, as newborns are obligate nasal breathers. Definitive management is surgical correction. Examiners may ask about unilateral choanal atresia presentation (less severe, often presents later), and complications of untreated choanal atresia.
- Scenario: A 45-year-old male complains of a persistent foul smell that no one else can detect. He describes food tasting “off” and generally unpleasant. He denies any recent cold or nasal discharge but had a head injury about 6 months ago.
- Questions: What olfactory disorder is he likely experiencing? What is the probable cause given his history? How would you investigate this?
- Discussion Points (Viva): The patient is likely experiencing dysosmia (specifically cacosmia or parosmia), where odours are distorted and often perceived as foul, possibly phantosmia if the smell occurs in the absence of a stimulus. The history of head injury 6 months prior strongly suggests post-traumatic olfactory dysfunction, possibly due to damage to the olfactory nerve fibres or their central connections. Investigation would include a detailed history of the injury, nasal endoscopy to rule out local pathology, and a high-resolution MRI of the brain and olfactory bulbs to assess for any structural damage along the olfactory pathway. Examiners might ask about other causes of dysosmia/phantosmia (e.g., temporal lobe epilepsy, chronic sinusitis), and the prognosis for post-traumatic olfactory loss.
- Scenario: A 60-year-old female presents with recurrent sinusitis and bronchiectasis. On examination, you notice a complete absence of nasal ciliary movement. She also reports a history of situs inversus totalis (organs on the opposite side of the body).
- Questions: What syndrome is suggested by this triad of symptoms? Explain the underlying physiological defect. How does this impact nasal and bronchial function?
- Discussion Points (Viva): This triad (recurrent sinusitis, bronchiectasis, situs inversus) is highly suggestive of Kartagener Syndrome, a subtype of Primary Ciliary Dyskinesia (PCD). The underlying physiological defect is a congenital abnormality in the structure or function of cilia, specifically dynein arm defects, which are crucial for ciliary beating. This defect severely impairs the mucociliary mechanism in both the nose and bronchi, leading to ineffective clearance of mucus, pathogens, and particles, thus predisposing her to chronic infections (sinusitis, bronchiectasis). In the nose, this results in impaired humidification and filtration. In the bronchi, it leads to chronic inflammation and structural damage (bronchiectasis). Situs inversus occurs because ciliary beating is essential for normal organ rotation during embryonic development. Examiners may ask about diagnostic tests for PCD (e.g., nasal nitric oxide measurement, electron microscopy of ciliary biopsy, genetic testing).
Frequently Asked Questions in Viva
- Q: What is the nasal cycle?
- A: The nasal cycle is a normal physiological phenomenon where blood flow in the nasal mucosa alternates, causing congestion and decongestion between the two sides of the nose, typically lasting 2.5 to 4 hours, ensuring efficient airflow and mucosal recovery.
- Q: Why is nose breathing important for newborns?
- A: Newborns are obligate nasal breathers, meaning they instinctively breathe through their nose, therefore, any nasal obstruction (like choanal atresia) can be life-threatening as they struggle to coordinate mouth breathing.
- Q: How does the nose protect the lower airways from infections?
- A: The nose protects the lower airways through several mechanisms, including filtration by vibrissae and mucus, mucociliary clearance, antibacterial enzymes like lysozyme, immunoglobulins (IgA, IgE), and protective reflexes such as sneezing, thus forming a robust defence.
- Q: What is the difference between anosmia and dysosmia?
- A: Anosmia is the complete loss of the sense of smell, while dysosmia (or parosmia) is a distortion of smell perception, where familiar odours are perceived differently, often unpleasantly.
- Q: Can nasal obstruction affect the lungs?
- A: Yes, chronic nasal obstruction can increase resistance to airflow, potentially leading to pulmonary changes like pulmonary hypertension and, in severe cases, cor pulmonale, highlighting the nose’s systemic impact on respiratory physiology.
- Q: Why is ammonia not used to test smell?
- A: Ammonia is not used because it primarily stimulates the trigeminal nerve (responsible for irritation and touch sensations in the nose), rather than the specific olfactory receptors, thus providing a false positive for smell perception.
- Q: What is Kartagener Syndrome?
- A: Kartagener Syndrome is a genetic disorder characterised by a triad of situs inversus, chronic sinusitis, and bronchiectasis, resulting from a primary ciliary dyskinesia that impairs mucociliary clearance throughout the respiratory tract.
——– End ——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Physiology of the Nose, Nasal Functions, Respiration Nose, Air Conditioning Nose, Mucociliary Clearance, Olfaction Pathway, Nasal Reflexes, Disorders of Smell, Anosmia, Hyposmia, Dysosmia, Phantosmia, Kartagener Syndrome, Choanal Atresia, Vocal Resonance Nose, NEET PG ENT, MBBS ENT Notes, CBME Curriculum ENT, Nose Physiology Summary, High-Yield ENT, ENT MCQs, Clinical Scenarios ENT, Viva ENT, Nose Humidification, Nasal Cycle, Olfactory Receptors, Cribriform Plate, Prepyriform Cortex, Trigeminal Nerve Nose, Lysozyme Nasal Secretions, IgA IgE Nasal, Pulmonary Hypertension Nasal, ENT Revision, Medical Education Nose, Olfactory Agnosia, Presbyosmia, Osmophobia, Nasal Airway Protection, ENT Exam Guide, Medical Mnemonics ENT, Nose Function Explained, Mnemonics for ENT, How does the nose warm air, What is the nasal cycle, Why can’t I smell after cold, Difference between hyponasal and hypernasal voice..
Good and well summarised notes i really enjoyed reading.
Thank you Dr Rahul