Caldwell-Luc’s surgery (or Anterior Antrostomy)
Definition
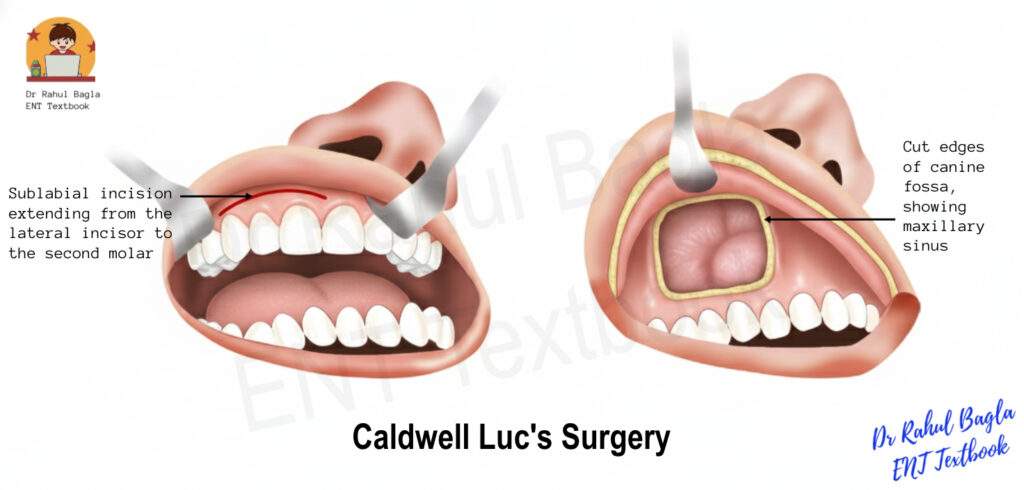
It is an external surgical procedure. In Caldwell-Luc surgery, an incision is made inside the upper lip (sublabial incision) just below the gingivobuccal sulcus to reach the anterior wall of the maxillary sinus. This wall is then opened through the canine fossa to remove disease inside the maxillary sinus, such as infected mucosa, tumours, or foreign bodies. The canine fossa is a key entry point. It’s a thin, depressed area in the anterior maxillary wall, found below the infraorbital foramen and lateral to the canine tooth root. This thin bone allows easy surgical access to the sinus.
Historical Background
The Caldwell–Luc procedure was first used to treat chronic maxillary sinusitis. The goal was to remove the infection and strip away the diseased sinus lining (mucosa). However, with a better understanding of sinus function and drainage, and following the development of Functional Endoscopic Sinus Surgery (FESS), the Caldwell-Luc surgery has become largely outdated for routine treatment of sinusitis. Nevertheless, although largely superseded by endoscopic techniques, it still holds value in specific indications—such as tumour access, foreign body removal, orbital floor repair, or surgical approaches to the pterygopalatine fossa.
Surgical Anatomy of Maxillary Sinus
The maxillary sinus is the largest paranasal sinus. It drains through the natural ostium into the middle meatus via the hiatus semilunaris.
Relations
- Roof: Orbit (orbital floor)
- Floor: Alveolar process (upper molar roots)
- Anterior wall: Facial surface of maxilla (canine fossa)
- Posterior wall: Infratemporal fossa
- Medial wall: Lateral nasal wall
Current Indications for Caldwell–Luc Surgery
While FESS manages most routine sinus issues, the Caldwell–Luc approach is necessary when a transantral approach or wide exposure is required.
1. Transantral Approach Indications:
- To the pterygopalatine or infratemporal fossa for tumour excision (e.g., JNA).
- For ligation of the internal maxillary artery and its branches in posterior epistaxis.
- Transantral ethmoidectomy approach to the ethmoid and sphenoid sinuses (e.g., Horgan’s ethmoidectomy).
- For Vidian neurectomy: A surgical procedure to cut a nerve for severe, intractable running nose – vasomotor rhinitis.
2. Disease removal Indications:
- Excision of dental cysts (e.g., dentigerous cysts) located high in the antrum.
- Removal of foreign bodies (e.g., bullets, displaced tooth roots, or dental material) from the antrum that cannot be retrieved endoscopically.
- Removal of the large, antral base of an antrochoanal polyp when it cannot be approached endoscopically via the natural ostium.
3. Orbital Indications:
- Repair of orbital floor fractures (blow-out fractures).
- Orbital decompression (e.g., for severe thyroid ophthalmopathy to relieve pressure on the orbit).
4. Fistula Repair: Used to fix a large hole between the mouth and the sinus (oroantral fistula).
5. Biopsy/Staging: It gives wide access for a biopsy in cases of suspected cancer (malignancy) in the maxilla or as an initial step for extensive cancer surgery (medial maxillectomy).
Contraindications for Caldwell–Luc Surgery
- Age: Generally contraindicated in children below 7 years of age (some sources say 17 years) due to the risk of damage to permanent tooth buds and disturbance of maxillary growth.
- Acute Infection: Acute infection or severe cellulitis over the maxilla.
Surgical Steps of Caldwell Luc’s Surgery
- Anaesthesia: Surgery is performed under general anaesthesia with a cuffed endotracheal tube and a pharyngeal pack; however, local anaesthesia is an option.
- Position: Patient lies supine with face turned slightly to the opposite side. The head-end of the table is raised.
- Incision: The upper lip is retracted superiorly with the help of a retractor. An incision is made in the gingivobuccal sulcus (sublabial incision), extending from the lateral incisor to the second molar. Thus, this provides a wide mucosal flap.
- Flap Elevation: The incision is deepened to the bone. The surgeon elevates the mucoperiosteal flap with the help of a periosteal elevator from the anterior maxilla wall in a subperiosteal plane.
- Nerve Identification: The infraorbital nerve is identified at the infraorbital foramen and preserved. This prevents postoperative cheek numbness.
- Canine Fossa Access: Canine fossa is identified, and using an osteotome, gouge and hammer, or a cutting burr, the thin bone of the canine fossa is removed, and the antrum is entered.
- Antrostomy Enlargement: The canine fossa opening (antrostomy) is enlarged using a Kerrison’s punch or a bone nibbler. This provides adequate visualisation and access to the pathology.
- Pathology Removal: The underlying pathology (e.g., cyst, tumour, foreign body) is removed, and the sinus is meticulously cleaned.
- Closure: The sublabial incision is closed with absorbable sutures.
Historical Step: Inferior Meatal Antrostomy (IMA)
- Past Practice: Surgeons commonly performed Inferior Meatal Antrostomy (IMA) along with Caldwell–Luc’s surgery to provide drainage and remove packing.
- Current Understanding: This step is now obsolete for drainage. We now understand that the natural mucosal ciliary action propels mucus toward the middle meatus (the natural ostium), not the inferior meatus. IMA does not improve drainage of antral secretions and is unnecessary unless specifically required for access (e.g., packing removal).
Complications of Caldwell–Luc Surgery
1. Sensory Nerve Injury:
- Infraorbital Nerve Injury: It causes anaesthesia or paresthesia of the cheek, upper lip, and gingiva. This is the most common sensory complication, often due to stretch injury during flap elevation. It may be temporary or permanent.
- Superior Alveolar Nerve Branches Injury: It causes numbness of the canine and premolar teeth and gingiva.
2. Vascular and Wound Issues:
- Facial Swelling/Oedema: The most common postoperative complication overall, due to tissue manipulation.
- Bleeding/Haemorrhage.
- Oroantral Fistula: It may occur if the sublabial wound breaks down.
- Osteomyelitis of the maxilla (rare).
3. Structural Damage:
- Injury to the Orbit: Possible during enlargement of the superior aspect of the antrostomy, especially during orbital floor repair.
- Injury to the Nasolacrimal Duct (NLD): Possible if an aggressive IMA is performed, hence leading to epiphora.
- Trauma to Tooth Buds/Roots: Risk of disturbing developing permanent teeth in children or damaging roots in adults.
Postoperative care of Caldwell–Luc Surgery
- Apply ice packs over the cheeks during the first 24 hours to reduce oedema, hematoma formation, and patient discomfort.
- Packing placed in the sinus and nasal cavity may be removed after 24 to 48 hours, depending on the surgical procedure and the surgeon’s preference.
- Prophylactic antibiotics are prescribed for 5 to 7 days to prevent postoperative infection.
- The patient should avoid blowing the nose for 2 weeks to prevent surgical emphysema and disruption of the surgical site.
———End of Chapter———-
High-Yield Points for Quick Revision (NEET PG)
- Most Common Sensory Complication: Infraorbital Nerve Paresthesia (Numb cheek/lip).
- Most Common Overall Complication: Facial Swelling/Oedema.
- Key Access Landmark: Canine Fossa.
- Nerve Protected: Infraorbital Nerve.
- Absolute Contraindication: Acute infection/cellulitis over the maxilla.
- Age Contraindication: Children below 7 years (due to tooth bud risk).
- Key Modern Indication: Transantral access to the Pterygopalatine Fossa (e.g., for Internal Maxillary Artery Ligation).
Clinical Case Scenarios
1. Case 1
A 24-year-old male has recurrent unilateral epistaxis and nasal obstruction. Imaging suggests a vascular mass extending into the pterygopalatine fossa.
Most likely diagnosis: Juvenile nasopharyngeal angiofibroma (JNA),
Best surgical approach using Caldwell–Luc: Transantral approach to pterygopalatine fossa,
Key step to reduce bleeding: Preoperative embolisation + internal maxillary artery control,
2. Case 2
A 35-year-old male underwent dental extraction 2 weeks ago. He now complains of fluid regurgitation from mouth into nose while drinking and foul smell.
Most likely diagnosis: Oroantral fistula with maxillary sinus infection,
Best management: Caldwell–Luc with sinus clearance + fistula closure,
3. Case 3
A 40-year-old patient has unilateral chronic maxillary sinusitis not improving with antibiotics and FESS. CT scan shows a radio-opaque object in the sinus floor.
Most likely diagnosis: Retained foreign body (dental material),
Best management: Caldwell–Luc removal of foreign body,
4. Case 4
A 30-year-old patient with thyroid ophthalmopathy develops severe proptosis and optic nerve compression.
Most likely management option: Orbital decompression,
Role of Caldwell–Luc: Provides access for decompression through maxillary sinus route,
Multiple Choice Questions (MCQs) (NEET PG Style)
- The Inferior Meatal Antrostomy (IMA) step in Caldwell–Luc surgery is now considered obsolete primarily because: A. It frequently causes Nasolacrimal Duct injury. B. It has a high rate of failure in removing packing. C. Mucociliary clearance occurs physiologically towards the middle meatus. D. The opening closes rapidly with scarring.
- Which of the following nerves is most commonly associated with temporary sensory complications following the Caldwell–Luc procedure? A. Facial nerve B. Infraorbital nerve C. Superior laryngeal nerve D. Trigeminal nerve (V3 branch)
- The optimal surgical access point for entering the maxillary sinus during a Caldwell–Luc procedure is the: A. Infraorbital foramen B. Inferior meatus C. Canine fossa D. Zygomatic recess
- A major current specialized indication for the Caldwell–Luc procedure is: A. Chronic rhinosinusitis refractory to medical therapy. B. Acute bacterial maxillary sinusitis. C. Transantral ligation of the Internal Maxillary Artery. D. Treatment of simple maxillary retention cysts.
- The absolute contraindication for a planned Caldwell–Luc surgery is: A. Age 10 years B. History of asthma C. Acute infection/cellulitis over the maxilla D. Presence of a large nasal polyp
- Why is the Caldwell-Luc procedure generally avoided in children under 7 years of age? A. Maxillary artery is too small to ligate. B. High risk of epiphora. C. Risk of damage to developing permanent tooth buds. D. Increased bone density compared to adults.
- Which instrument is typically used to enlarge the opening made in the canine fossa? A. Killian’s nasal speculum B. Kerrison’s punch C. Bayonet forceps D. Sickle knife
- The most common overall postoperative complication of the Caldwell-Luc procedure is: A. Oroantral fistula B. Injury to the tooth roots C. Facial swelling and edema D. Permanent paresthesia
- An aggressive Inferior Meatal Antrostomy (IMA) carries a high risk of injury to which adjacent structure? A. Optic nerve B. Nasolacrimal duct (NLD) C. Eustachian tube D. Sphenopalatine artery
- Which condition necessitates a transantral approach to perform Vidian Neurectomy? A. Chronic otitis media B. Sinus malignancy C. Intractable vasomotor rhinitis D. Choanal atresia
Answers and Explanations:
- C. The cilia sweep mucus toward the middle meatus (natural ostium), making IMA non-physiological for drainage.
- B. The Infraorbital nerve exits the foramen superior to the antrostomy site and is prone to stretch injury during flap retraction.
- C. The canine fossa is the thinnest, most accessible part of the anterior maxillary wall.
- C. This procedure requires wide access to the pterygopalatine fossa, a modern key indication.
- C. Performing an elective procedure through an acutely infected site risks spreading the infection (e.g., osteomyelitis or orbital cellulitis).
- C. The developing tooth germs are highly susceptible to damage during the bone removal in the canine fossa area.
- B. Kerrison’s punch or bone nibblers are used to expand the initial bony opening (antrostomy).
- C. Tissue manipulation is unavoidable, leading to temporary swelling/edema in almost all cases.
- B. The NLD runs in the lateral wall of the inferior meatus, making it vulnerable during IMA.
- C. Vidian Neurectomy is performed to address severe, medication-resistant running nose caused by parasympathetic overactivity.
Frequently Asked Questions in Viva
- What is the Caldwell-Luc surgery? It is an external surgical procedure using a sublabial incision and an opening through the canine fossa to access and treat diseases within the maxillary sinus.
- Why is Caldwell-Luc surgery rarely performed today for routine sinusitis? It is largely obsolete for routine sinusitis because Functional Endoscopic Sinus Surgery (FESS) is less invasive and respects the natural physiological drainage pathway toward the middle meatus.
- What is the most common sensory complication after the procedure? Paresthesia (numbness or tingling) of the cheek and upper lip due to temporary injury or stretching of the infraorbital nerve during the surgery.
- Where is the key entry point in the maxilla for the operation? The key entry point is the canine fossa, a thin bone area below the infraorbital foramen and lateral to the canine tooth root.
- What are two major modern indications for the Caldwell-Luc procedure? Two major modern indications are the repair of orbital floor fractures (blow-out fractures) and surgical access to the pterygopalatine fossa for tumor excision or artery ligation.
———–End———–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Caldwell Luc surgery, canine fossa antrostomy, Caldwell-Luc indications, Caldwell Luc technique steps, modified Caldwell Luc without IMA, infraorbital nerve injury in Caldwell Luc, endoscopic vs Caldwell Luc, maxillary sinus tumors approach Caldwell-Luc, Caldwell Luc complications, CBME ENT Caldwell Luc, ENT topics for NEET PG, MBBS ENT notes maxillary sinus, Caldwell–Luc surgery indications, Complications of Caldwell–Luc, Canine fossa surgical approach, Transantral artery ligation, Orbital floor fracture repair ENT, Caldwell–Luc vs FESS, Caldwell–Luc surgery current indications, Complications of Caldwell–Luc procedure, Canine fossa approach maxillary sinus, Infraorbital nerve injury Caldwell–Luc, Caldwell–Luc vs FESS for sinusitis, Transantral ligation of Internal Maxillary Artery, Caldwell–Luc surgery for orbital floor fracture, Why is IMA obsolete in Caldwell–Luc surgery, ENT topics for NEET PG Caldwell–Luc, Sublabial incision Caldwell–Luc procedure.