|
The following CBME core competencies are covered in this chapter.
|
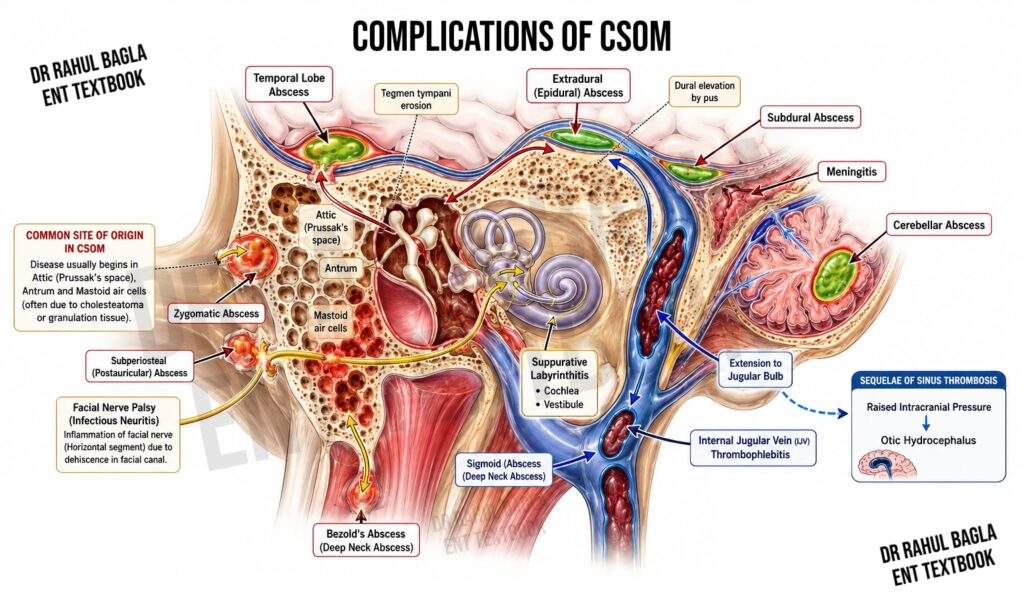
Complications of CSOM
Complications of Chronic Suppurative Otitis Media (CSOM) develop when a persistent middle ear infection spreads beyond the confines of the middle ear cleft to involve the temporal bone or intracranial structures. Although the widespread use of antibiotics has markedly reduced their incidence, these complications continue to cause significant morbidity and mortality, particularly in resource-limited settings and in patients with delayed diagnosis, cholesteatoma, antibiotic-resistant infections, or inadequate treatment.
CSOM complications are broadly classified as intratemporal (extracranial) and intracranial. They range from relatively localised conditions, such as acute mastoiditis and facial nerve paralysis, to life-threatening emergencies including meningitis, lateral sinus thrombosis, and otogenic brain abscess. Therefore, prompt recognition, early diagnosis, appropriate antimicrobial therapy, and timely surgical intervention are essential to prevent permanent hearing loss, neurological deficits, and death.
This chapter provides a comprehensive, CBME-aligned review of the complications of CSOM for MBBS students, ENT postgraduates, and candidates preparing for NEET PG, INI-CET, FMGE, and university examinations. It covers the pathogenesis, routes of infection spread, classification, clinical features, investigations, management, high-yield tables, mnemonics, clinical pearls, viva questions, and exam-oriented revision points, making it a complete standalone resource for both conceptual learning and rapid revision.
Factors Contributing to Complications in Chronic Suppurative Otitis Media
The progression of CSOM to severe complications is influenced by a combination of host-related, environmental, and pathogen-specific factors. The following are key contributors to the development of complications in CSOM:
- Age: Young children, whose immune systems are still developing, and elderly individuals, who often experience age-related immune decline, are at heightened risk.
- Socioeconomic Conditions: Poor living conditions, including overcrowding, inadequate sanitation, and limited access to healthcare services, are strongly associated with a higher prevalence of CSOM and its complications.
- Virulent Pathogens and Antibiotic Resistance: The emergence of antibiotic-resistant strains of bacteria, such as Pseudomonas aeruginosa, Streptococcus pneumoniae, Haemophilus influenzae, and Methicillin-resistant Staphylococcus aureus (MRSA), complicates the management of CSOM. These pathogens are often implicated in severe or recurrent infections that are refractory to standard treatments.
- Immunocompromised States: Underlying conditions that impair immune function, such as diabetes mellitus, HIV/AIDS, malignancies, and the use of immunosuppressive therapies, increase the likelihood of severe infections and complications.
- Preformed Pathways for Infection Spread: Anatomical abnormalities or defects in the temporal bone, whether congenital (e.g., Mondini malformation) or acquired (e.g., dehiscence of the facial canal, temporal bone fractures, or surgical defects), provide direct routes for the spread of infection beyond the middle ear cleft.
- Cholesteatoma: The presence of cholesteatoma, a destructive and expansile lesion of the middle ear, exacerbates the risk of complications. Cholesteatoma induces osteitis and granulation tissue formation, leading to bone erosion and facilitating the spread of infection to adjacent structures.
- Inadequate Management of Ear Infections: Delayed or inappropriate treatment of acute, subacute, or chronic ear infections significantly increases the risk of complications. This highlights the importance of early diagnosis, appropriate antimicrobial therapy, and surgical intervention when necessary.
Mechanisms of Infection Spread in Chronic Suppurative Otitis Media (CSOM)
The spread of infection in Chronic Suppurative Otitis Media (CSOM) can occur through several distinct mechanisms, each contributing to the potential for severe complications. Understanding these pathways is critical for clinicians to anticipate and manage the progression of the disease effectively. The primary mechanisms of infection spread include direct bone erosion, venous thrombophlebitis, and preformed anatomical pathways.
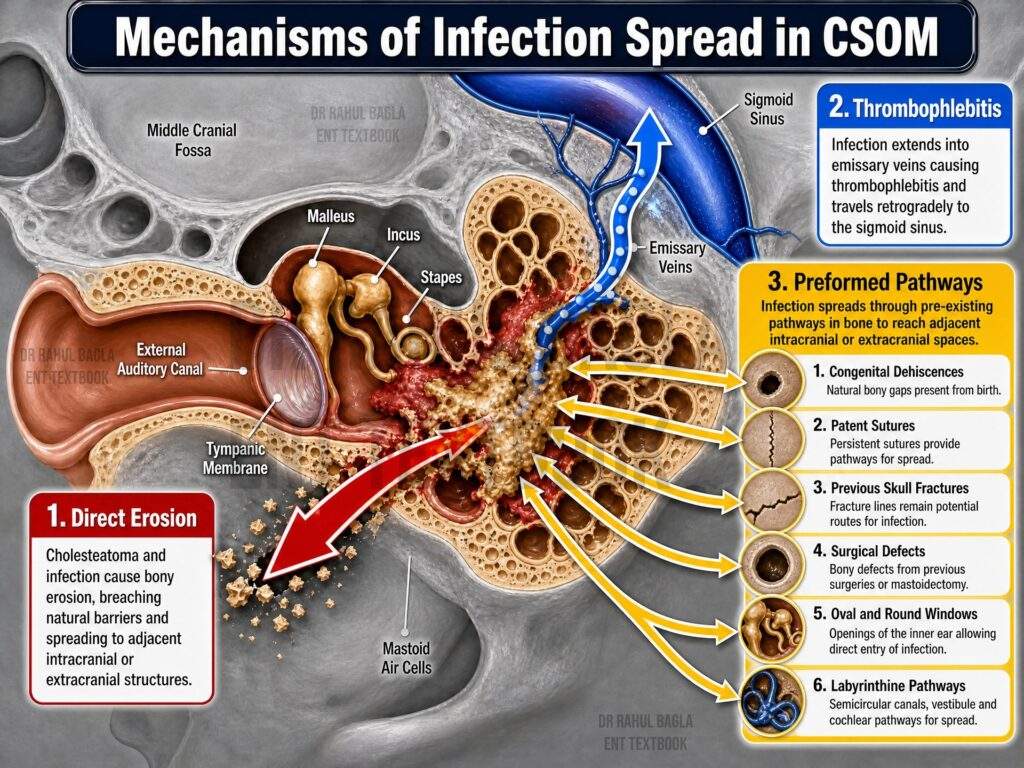
1. Direct Bone Erosion
In CSOM, bone erosion is a significant pathway for the spread of infection. In acute infections, hyperaemic decalcification of the bone facilitates the spread of infection. In chronic infections, osteitis (inflammation of the bone), erosion caused by cholesteatoma, or granulation tissue formation can lead to bone destruction. Cholesteatoma, in particular, is highly destructive, as it induces bone resorption, enabling the infection to penetrate deeper structures.
2. Venous Thrombophlebitis
The venous system of the temporal bone provides another route for infection spread. The veins of the Haversian canals, which are interconnected with dural veins and dural venous sinuses, can transmit infection from the mastoid bone to intracranial structures. This process, known as thrombophlebitis, is more common in acute infections. Small emissary veins can carry infection through the bone and dura to larger venous sinuses, such as the lateral (sigmoid) and superior petrosal sinuses. From these sinuses, infection can spread to the cerebellum (via the lateral sinus) or the temporal lobe (via the superior petrosal sinus), leading to serious intracranial complications.
3. Preformed Pathways
Preformed anatomical pathways, whether congenital, acquired, or iatrogenic, provide direct routes for infection to spread beyond the middle ear. These pathways include:
- Congenital Dehiscences: Defects such as a dehiscent bony facial canal or a thin floor of the middle ear overlying the jugular bulb.
- Patent Sutures: Openings such as the petrosquamous suture, which may persist into adulthood.
- Previous Skull Fractures: Fracture sites that heal with fibrous scar tissue, creating a potential route for infection.
- Surgical Defects: Procedures such as stapedectomy, fenestration, or mastoidectomy, which may expose the dura or create fistulas.
- Oval and Round Windows: Normal anatomical structures that can serve as conduits for infection.
- Labyrinthine Pathways: Infection from the labyrinth can travel along the internal acoustic meatus or the aqueducts of the vestibule and cochlea to reach the meninges.
Classification of Complications of COM
Complications of otitis media are broadly categorised into two groups based on their anatomical location: Intratemporal (extracranial) and intracranial.
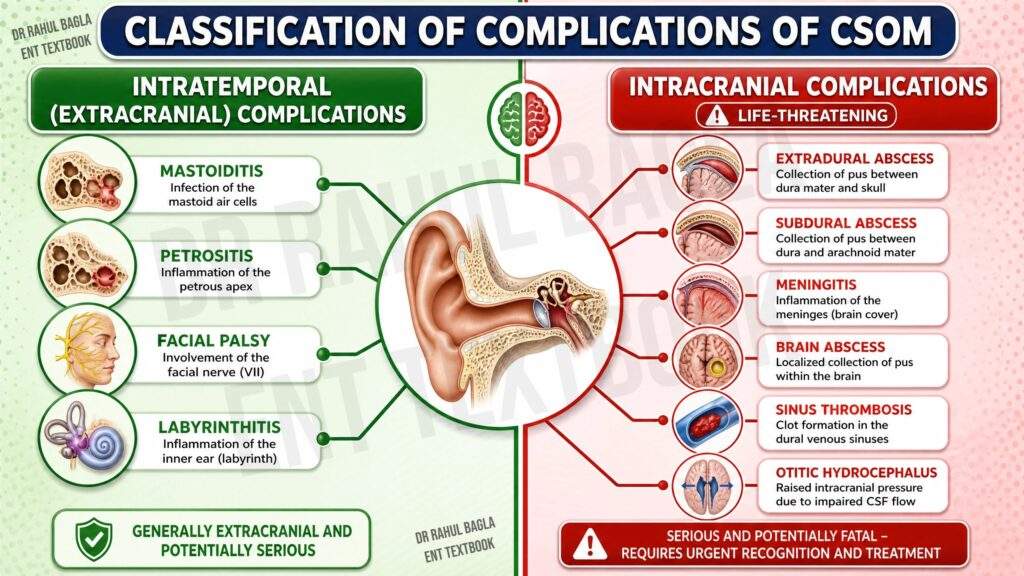
A. Intratemporal Complications (Within the Temporal Bone)
i. Acute Mastoiditis: Inflammation or infection of the mastoid antrum and associated mastoid air cells.
ii. Subacute (masked) Mastoiditis. Slow destruction of mastoid air cells but without the acute signs and symptoms.
iii. Petrositis: Infection of the petrous part of the temporal bone.
iv. Facial Paralysis: Resulting from facial nerve involvement due to infection or compression.
v. Labyrinthitis: Inflammation of the inner ear structures, leading to hearing loss and vertigo.
B. Intracranial Complications
i. Extradural Abscess: Collection of pus between the dura and the skull.
ii. Subdural Abscess: Collection of pus between the dura and arachnoid mater.
iii. Meningitis: Inflammation of the meninges due to infection.
iv. Brain Abscess: Focal collection of pus within the brain parenchyma.
v. Lateral Sinus Thrombophlebitis: Thrombosis and inflammation of the lateral venous sinus.
vi. Otitic Hydrocephalus: Increased intracranial pressure secondary to otitis media.

Incidence of Complications
The incidence of these complications varies:
- Extracranial complications account for approximately 32% of cases.
- Intracranial complications occur in about 56% of cases.
- Combined intracranial and extracranial complications are observed in 12% of cases.
Historically, mucosal-type CSOM was considered “safe” due to a perceived lower risk of complications compared to squamosal-type CSOM. However, recent studies have challenged this notion, revealing that extracranial complications occur in 59% of mucosal-type cases and 41% of squamosal-type cases. Similarly, intracranial complications are observed in 59% of squamosal-type cases and 41% of mucosal-type cases. As a result, the terms “safe” and “unsafe” CSOM are no longer used in clinical practice.
Sequelae of Otitis Media
Sequelae are long-term consequences of middle ear infections and should be distinguished from acute complications. They result from the direct effects of infection and inflammation on the middle and inner ear structures. Common sequelae include:
a. Perforation of the Tympanic Membrane: Persistent or recurrent perforations due to chronic infection.
b. Ossicular Erosion: Destruction of the ossicles, leading to conductive hearing loss.
c. Atelectasis and Adhesive Otitis Media: Collapse of the tympanic membrane and adhesion to middle ear structures.
d. Tympanosclerosis: Calcification and scarring of the tympanic membrane and middle ear.
e. Cholesteatoma Formation: Abnormal growth of keratinising squamous epithelium in the middle ear.
f. Conductive Hearing Loss: Resulting from ossicular erosion or fixation.
g. Sensorineural Hearing Loss: Due to inner ear damage from infection or inflammation.
h. Speech Impairment: Often secondary to hearing loss, particularly in children.
i. Learning Disabilities: Associated with hearing loss during critical developmental stages in infants and children.
Intratemporal Complications (Within the Temporal Bone)
1. Acute Mastoiditis
Acute mastoiditis is an inflammatory condition involving the mucosal lining of the mastoid antrum and air cell system, often occurring as a complication of acute otitis media (AOM). While inflammation of the mastoid air cells is a common feature of AOM, the term “mastoiditis” is specifically used when the infection extends beyond the mucosa to involve the bony walls of the mastoid air cell system. This condition is more prevalent in children and is frequently associated with well-pneumatized mastoids.
Previously thought to occur 10–14 days after AOM, acute mastoiditis can now manifest as early as 2 days following the onset of AOM. This condition predominantly affects children, with the majority of cases occurring in those under 4 years of age, likely due to heightened inflammatory responses in this population.
Aetiology of Acute Mastoiditis
Acute mastoiditis typically arises as a sequel to acute suppurative otitis media. The development of mastoiditis is influenced by factors such as the virulence of the infecting organism and the host’s immune status. Predisposing conditions include measles, exanthematous fevers, malnutrition, and systemic diseases such as diabetes. The most common causative organisms are Beta haemolytic streptococcus, Streptococcus pneumoniae, Streptococcus pyogenes, Pseudomonas aeruginosa, and Staphylococcus aureus. Anaerobic organisms are also frequently implicated, necessitating targeted antibacterial therapy.
Pathology of Acute Mastoiditis
The pathological progression of acute mastoiditis involves two primary mechanisms:
- Production of Pus Under Tension: The extension of inflammation to the mucoperiosteal lining of the mastoid air cells results in increased pus production due to the large surface area involved. Drainage of this pus through a small tympanic membrane perforation or the eustachian tube becomes inadequate, leading to accumulation of pus under pressure. Swelling of the mucosa in the antrum and attic further obstructs drainage, exacerbating the condition.
- Hyperaemic Decalcification and Osteoclastic Resorption: Hyperaemia and mucosal engorgement cause calcium dissolution from the bony walls of the mastoid air cells, a process known as hyperaemic decalcification. This, combined with osteoclastic activity, leads to the destruction and coalescence of air cells, forming a single irregular cavity filled with pus (empyema of the mastoid). In advanced cases, pus may erode the mastoid cortex, resulting in subperiosteal abscess formation or even a discharging fistula.
Stages of Acute Mastoiditis
The progression of acute mastoiditis can be divided into three stages:
- Acute Otitis Media with Mastoid Mucosal Inflammation: Inflammation is confined to the mucosa of the mastoid air cells, with no clinical signs of mastoiditis.
- Acute Mastoiditis with Periostitis: Periosteal inflammation leads to ironing of the mastoid crease and mild swelling over the mastoid process. The pinna may be pushed forward, but abscess formation has not yet occurred.
- Acute Mastoiditis with Osteitis: Increased inflammation causes mucosal oedema, obstructing natural drainage and leading to pus accumulation under pressure. Hyperaemic decalcification of the bony septa results in the formation of a common mastoid cavity filled with pus. Erosion of the inner and outer mastoid cortex may lead to abscess formation around the ear.

Symptoms of Acute Mastoiditis
The symptoms of acute mastoiditis often resemble those of acute suppurative otitis media but exhibit specific changes that indicate disease progression:
- Pain Behind the Ear: Pain is a common symptom in acute otitis media (AOM), typically subsiding with the establishment of a tympanic membrane perforation or following appropriate antibiotic treatment. However, in the context of acute mastoiditis, it is the persistence or worsening of pain, particularly at night due to venous congestion, an increase in the intensity of pain, or the recurrence of pain after it had previously subsided are hallmark features that suggest the development of acute mastoiditis. Pain is more severe in cases with an intact but bulging tympanic membrane caused by pus under tension. In some cases, surgical intervention, such as myringotomy, may be required to release the pus and alleviate pain.
- Fever: Persistent or recurrent fever despite antibiotic treatment is a significant indicator of mastoiditis. The fever is typically low-grade and intermittent, resulting from toxin absorption from trapped pus under pressure.
- Ear Discharge: Discharge becomes profuse and more purulent. In some cases, discharge may cease due to obstruction, accompanied by worsening pain and fever. Persistence of discharge beyond three weeks in AOM suggests mastoiditis.
- Hearing Loss: Mild-to-moderate conductive hearing loss is common and persists until the pus resolves and mucosal oedema subsides.
- Postauricular Swelling: Swelling over the mastoid process is observed in 80–90% of cases.
- Systemic Toxicity: Affected children often appear ill and toxic, requiring hospitalisation.
Signs of Acute Mastoiditis
- Mastoid Tenderness: Tenderness over the mastoid process is a key clinical sign of acute mastoiditis. It is elicited by applying firm pressure over the suprameatal (Macewen’s) triangle (overlying the mastoid antrum), the body of the mastoid, and the mastoid tip. Tenderness should always be compared with the opposite (unaffected) side to assess its significance.
- Ear Discharge: Mucopurulent or purulent discharge is commonly observed, often appearing pulsatile (referred to as the “light-house effect”) when seen through a central perforation of the pars tensa. This pulsatile discharge is indicative of pus under pressure in the middle ear. This discharge has the tendency to fill up again after dry mopping or suction (referred to as the “Reservoir sign”).
- Sagging of the Posterosuperior Meatal Wall: This sign results from periostitis of the bony wall separating the antrum from the deeper posterosuperior part of the bony ear canal. Sagging is a direct consequence of inflammation and swelling in this region.
- Perforation of the Tympanic Membrane: A small perforation in the pars tensa is typically observed, often accompanied by congestion of the surrounding tympanic membrane. Perforation occurs due to necrosis of the tympanic membrane tissue by pus under tension in the middle ear. In some cases, the perforation may appear as a nipple-like protrusion. In patients who have received inadequate antibiotic treatment, the tympanic membrane may remain intact but appear dull and opaque due to necrosis caused by pus under tension.
- Swelling Over the Mastoid: Initially, swelling results from periosteal oedema, giving the mastoid a smooth, “ironed out” appearance. As the condition progresses, the retroauricular sulcus becomes obliterated, and the pinna is pushed forward and downward. In advanced cases, pus may erode the bony cortex, leading to the formation of a subperiosteal fluctuant abscess.
- Hearing Loss: Conductive hearing loss is invariably present due to the accumulation of pus in the middle ear and associated mucosal oedema.
- General Findings: Patients often appear ill and toxic, with systemic signs of infection such as low-grade fever. In children, fever is typically higher, accompanied by an elevated pulse rate, reflecting the severity of the condition.
Investigations of Acute Mastoiditis
To confirm the diagnosis of acute mastoiditis and guide appropriate treatment, the following investigations are essential:
- X-ray of the Mastoid: X-ray imaging reveals clouding of the mastoid air cells due to pus accumulation. As the disease progresses, destruction of the bony septa of the mastoid air cells may be observed, leading to the formation of a single, irregular cavity (empyema of the mastoid).
- Blood Count: A complete blood count typically shows leukocytosis (elevated white blood cell count) and an increased erythrocyte sedimentation rate (ESR), both of which are indicative of an active infection.
- Pus Culture and Sensitivity: A sample of the ear discharge is sent for culture and sensitivity testing to identify the causative organisms and determine their antibiotic sensitivity.
Treatment of Acute Mastoiditis
The management of acute mastoiditis involves a combination of medical and surgical interventions, depending on the severity of the condition.
1. Hospitalisation: Patients with acute mastoiditis are typically hospitalised for close monitoring and aggressive treatment.
2. Antibiotics: Empirical antibiotic therapy is initiated promptly, even before culture results are available. First-line antibiotics such as amoxicillin or ampicillin are commonly used. Once the culture and sensitivity report is available, the antibiotic regimen is adjusted to target the specific pathogens. Since anaerobic organisms are frequently involved, chloramphenicol or metronidazole is often added to the treatment plan.
3. Myringotomy: In cases where pus is under tension in the middle ear, a wide myringotomy is performed to relieve pressure and facilitate drainage. This procedure is typically done in the posteroinferior quadrant of the tympanic membrane, as this is the most dependent part of the middle ear cavity. Early cases of acute mastoiditis may respond well to conservative treatment with antibiotics alone or in combination with myringotomy.
4. Incision and Drainage: Any abscesses in or around the ear require prompt incision and drainage to prevent further spread of infection.
5. Cortical Mastoidectomy: Surgical intervention in the form of cortical mastoidectomy is indicated in the following scenarios:
- Presence of a subperiosteal abscess.
- Sagging of the posterosuperior meatal wall.
- Positive reservoir sign (i.e., the ear canal rapidly refills with pus after being cleaned).
- Lack of improvement or worsening of the patient’s condition despite 48 hours of adequate medical treatment.
- Development of complications such as facial paralysis, labyrinthitis, or intracranial infections.
- Masked mastoiditis (slow destruction of mastoid air cells but without the acute signs and symptoms).
The goal of cortical mastoidectomy is to exenterate all infected mastoid air cells and remove any pockets of pus. Postoperatively, antibiotic therapy is continued for at least 5 days to ensure complete eradication of the infection.
Differential Diagnosis of Acute Mastoiditis
Accurate diagnosis of acute mastoiditis requires careful differentiation from other conditions that may present with similar clinical features. The following conditions should be considered in the differential diagnosis:
1. Suppuration of Mastoid Lymph Nodes: Enlargement and suppuration of mastoid lymph nodes can occur secondary to scalp infections, leading to abscess formation. However, this condition can be distinguished from acute mastoiditis by the absence of a history of preceding otitis media, ear discharge, or hearing loss. Additionally, the abscess in suppurative lymphadenitis is typically superficial and not associated with middle ear pathology.
2. Otitis Externa: Otitis externa, an infection of the external ear canal, can mimic acute mastoiditis but can be differentiated based on the following features:
- Absence of Preceding Acute Otitis Media: Unlike mastoiditis, otitis externa is not preceded by middle ear infection.
- Positive Tragal Sign: Pain is elicited by pressing the tragus or pulling the pinna, which is characteristic of otitis externa.
- Localized Swelling: Swelling is confined to the cartilaginous portion of the external ear canal.
- Nature of Discharge: Discharge in otitis externa is never mucoid or mucopurulent, as the external ear lacks mucus-secreting glands. Mucoid discharge is indicative of middle ear involvement.
- Lymph Node Enlargement: Pre- or postauricular lymph nodes may be enlarged in otitis externa.
- Hearing Loss: Conductive hearing loss, if present, is mild and results from occlusion of the ear canal rather than middle ear pathology.
- Tympanic Membrane Appearance: A normal-appearing tympanic membrane excludes the possibility of acute mastoiditis.
- X-ray Findings: Clear mastoid air cells on X-ray imaging rule out acute mastoiditis. However, haziness due to soft tissue swelling in cases of furunculosis may complicate interpretation.
3. Infected Sebaceous Cyst: An infected sebaceous cyst over the mastoid region may present with localised swelling and tenderness. However, it lacks the systemic symptoms, ear discharge, and hearing loss associated with acute mastoiditis.
Abscesses Associated with Mastoid Infections
Mastoid infections, particularly acute mastoiditis, can lead to the formation of abscesses in various anatomical locations. These abscesses arise due to the spread of infection from the mastoid air cells to surrounding tissues.
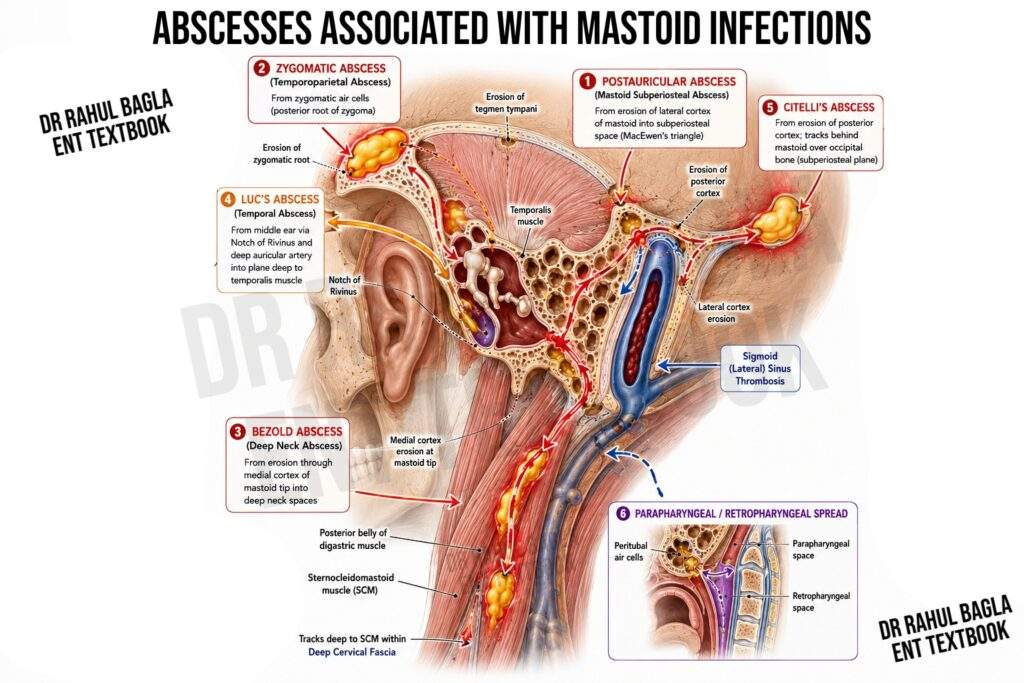
1. Postauricular Abscess. The postauricular abscess is the most common type of abscess associated with mastoid infections. It typically forms over the mastoid process, specifically in MacEwen’s triangle.
Clinical Features: Swelling over the mastoid process pushes the pinna anteriorly and inferiorly. The abscess may erode the lateral mastoid cortex, leading to skin perforation and the formation of a postauricular fistula.
Treatment: Antibiotics: Broad-spectrum intravenous antibiotics are initiated. Cortical or Modified Radical Mastoidectomy: Surgical drainage of the mastoid air cells is performed. Incision and Drainage: The abscess is incised and drained to remove pus.
2. Zygomatic Abscess (Temporoparietal Abscess). This abscess results from infection of the zygomatic air cells located at the posterior root of the zygoma.
Clinical Features: Swelling appears anterior and superior to the pinna. Associated oedema of the upper eyelid may be present. Often occurs in conjunction with a postauricular abscess.
Treatment: Antibiotics: Intravenous antibiotics are administered. Cortical or Modified Radical Mastoidectomy: Surgical intervention is required to address the underlying mastoid infection. Incision and Drainage: The abscess is drained surgically.
3. Bezold Abscess. A Bezold abscess occurs when pus from acute coalescent mastoiditis erodes the thin medial cortex of the mastoid tip and tracks into the neck.
Clinical Features: Sudden onset of pain, fever, and tender swelling in the neck. Torticollis (neck stiffness) may be present. History of purulent otorrhea is common. The abscess may present in various locations:
- Deep to the sternocleidomastoid muscle.
- Along the posterior belly of the digastric muscle.
- In the upper posterior triangle of the neck.
- In the parapharyngeal space or along the carotid sheath.
Differential Diagnosis: Acute upper jugular lymphadenitis, Parotid gland abscess or mass, Infected branchial cyst, Parapharyngeal abscess, Jugular vein thrombosis.
Diagnostic Workup: Contrast-Enhanced CT Scan of the Neck: Essential to evaluate the extent of the abscess. High-Resolution CT (HRCT) of the Temporal Bone: Assesses mastoid and middle ear involvement.
Treatment: Intravenous Antibiotics: Guided by culture and sensitivity results from pus obtained during surgery. Cortical Mastoidectomy: Drains pus from the mastoid air cells and middle ear. Osteitic bone and granulations are removed. Drainage of Neck Abscess: A separate incision is made to drain the abscess, and a suction drain is placed.
4. Temporal Abscess (Luc’s Abscess). This rare abscess forms deep to the temporalis muscle and is unrelated to the mastoid process.
Pathogenesis: Infection spreads from the middle ear via the notch of Rivinus and the deep auricular artery.
Treatment: Incision and Drainage: The abscess is drained surgically or through repeated aspiration. Intravenous Antibiotics: Administered to control infection. Temporary Grommet Insertion: May be required if pus is under tension in the middle ear.
5. Citelli’s Abscess. This abscess forms behind the mastoid, closer to the occipital bone, and is distinct from the postauricular abscess.
Pathogenesis: Pus tracks from the mastoid tip along the posterior belly of the digastric muscle or through fascial planes.
Treatment: Intravenous Antibiotics: Initiated to control infection. Drainage: The abscess is drained surgically.
6. Parapharyngeal or Retropharyngeal Abscess. This abscess results from the involvement of peritubal air cells, with pus tracking into the retropharyngeal or parapharyngeal spaces.
Pathogenesis: Infection spreads from the mastoid via the peritubal air cells.
Treatment: Antibiotics: Broad-spectrum intravenous antibiotics are essential. Surgical Drainage: The abscess is drained, and the underlying mastoid infection is addressed through mastoidectomy.
2. Subacute (Masked) Mastoiditis
Masked mastoiditis, unlike acute mastoiditis, is a subclinical condition marked by infection and inflammation of the mucosal lining and slow, gradual destruction of the mastoid air cells, despite an intact tympanic membrane. It lacks acute symptoms such as pain, fever, discharge, or swelling, making it difficult to diagnose clinically. However, surgical exploration reveals significant pathological changes, including air cell destruction, granulation tissue, and dark gelatinous material in the mastoid cavity. Advanced cases may show erosion of the tegmen tympani and sinus plate, sometimes with extradural or perisinus abscess formation.
Aetiology
The development of subacute mastoiditis is frequently attributed to inadequate antibiotic therapy, particularly in terms of dosage, frequency, and duration of administration. This condition typically arises as a sequela of incompletely treated acute otitis media (AOM), where obstruction of the aditus ad antrum—due to mucosal oedema and granulation tissue—leads to persistent, isolated inflammation within the mastoid air cell system. This smouldering infection may remain clinically silent for weeks, months, or even years, resulting in progressive bony destruction. The condition often resolves spontaneously, though it may also lead to severe complications if left untreated. A common contributing factor is the use of oral penicillin for acute otitis media, which may alleviate acute symptoms but fails to fully eradicate the infection, allowing it to persist within the mastoid.
Clinical Features
Masked mastoiditis primarily affects children, who may exhibit nonspecific symptoms like mild malaise, subtle ear discomfort, or persistent hearing loss. Otoscopic examination reveals a thickened, opaque tympanic membrane, though it remains intact. Mild mastoid tenderness may be present.
Investigations
Audiometry typically shows conductive hearing loss, while impedance audiometry remains normal due to the absence of middle ear fluid. X-rays reveal clouding of mastoid air cells, and high-resolution computed tomography (HRCT) is crucial for assessing bony destruction and intratemporal complications.
Treatment
Cortical mastoidectomy to drain pus and restore aditus patency, combined with a full course of antibiotics. This approach resolves the infection, often restoring normal tympanic membrane appearance and improving hearing. Early diagnosis and intervention are essential to prevent complications and preserve auditory function.
3. Petrositis
Petrositis refers to the spread of infection from the middle ear and mastoid to the petrous portion of the temporal bone. This condition can occur in association with acute coalescent mastoiditis, latent mastoiditis, or chronic middle ear infections.
Pathology
The petrous bone can be classified into three types based on its structure:
- Pneumatized: Characterised by air cells extending to the petrous apex, observed in approximately 30% of cases.
- Diploic: Composed of marrow spaces without air cells.
- Sclerotic: Dense and compact bone with minimal air cells or marrow spaces.
In pneumatized petrous bones, infection typically spreads through two primary cell tracts:
- Posterosuperior Tract: Originates in the mastoid and extends behind or above the bony labyrinth to the petrous apex. In some cases, cells may pass through the arch of the superior semicircular canal to reach the apex.
- Anteroinferior Tract: Begins at the hypotympanum near the eustachian tube, curves around the cochlea, and extends to the petrous apex.
The infective process follows these tracts, leading to the formation of an epidural abscess at the petrous apex. Due to the petrous bone’s proximity to vascular and neurological structures, infections in this region can have severe consequences, including meningeal irritation and cranial nerve involvement (abducens nerve and trigeminal ganglion).
Clinical Features
The classical presentation of petrositis is Gradenigo syndrome, characterised by the triad of:
- Diplopia: Due to abducens nerve (VI) palsy.
- Deep-seated ear or retro-orbital pain: Resulting from trigeminal nerve (V) involvement.
- Persistent ear discharge.
However, the full triad is rarely observed in modern clinical practice. Other clinical features include:
- Persistent ear discharge, often accompanied by deep-seated pain, despite adequate surgical intervention such as cortical or modified radical mastoidectomy.
- Systemic symptoms such as fever, headache, vomiting, and neck rigidity.
- Facial paralysis and recurrent vertigo due to involvement of the facial and vestibulocochlear nerves.
Differential Diagnosis
Petrositis must be differentiated from other conditions affecting the petrous apex, including: Cholesteatoma, Meningioma, Extension of acoustic neuroma, Metastatic carcinoma and Histiocytosis X.
Diagnosis
Accurate diagnosis requires both a CT scan and an MRI. A CT scan provides detailed visualisation of the bony structures and air cells in the petrous apex, while an MRI helps differentiate between marrow-containing diploic bone and fluid or pus accumulation. These imaging modalities also help rule out other intracranial complications.
Treatment
1. Medical Management: Intravenous antibiotics are the mainstay of treatment, typically administered for 2–3 weeks. High initial doses are recommended, with therapy continued for 4–5 days after symptom resolution. Most cases of acute petrositis can be effectively managed with antibiotics alone, highlighting the importance of early diagnosis and appropriate medical therapy.
2. Surgical Intervention:
- Surgery is rarely required but may be necessary in cases of associated mastoiditis. Procedures such as cortical, modified radical, or radical mastoidectomy may be performed to identify and enlarge fistulous tracts for adequate drainage.
- The posterosuperior cell tract is often located in Trautmann’s triangle or the attic, while the anteroinferior tract is situated near the tympanic opening of the eustachian tube, anterior to the cochlea.
4. Facial Nerve Paralysis
Facial nerve paralysis is a significant complication of both acute otitis media (AOM) and chronic otitis media (COM). The facial nerve, though typically protected within its bony canal, can be exposed due to congenital dehiscence (absence of bony covering) in 30-40% of individuals, particularly in the tympanic segment above the oval window. This anatomical vulnerability increases the risk of nerve involvement during middle ear infections.
In acute otitis media
Facial paralysis is rare (0.005%) but can occur due to:
- Raised middle ear pressure: Pus accumulation in the middle ear, especially with an intact tympanic membrane, increases pressure on the nerve.
- Osteitis: Inflammation of the bone surrounding the nerve.
- Tschiassny’s theory: Direct infectious spread through dehiscence or neurovascular connections between the nerve and the inflamed mucosa.
These factors cause nerve oedema within the tight bony canal, leading to conduction defects.
Management: It includes intravenous antibiotics and steroids to control infection and reduce inflammation. Myringotomy with grommet insertion is performed to drain pus and relieve pressure. Early intervention typically results in full recovery, and surgical procedures like mastoidectomy or nerve decompression are rarely needed.
In chronic otitis media
Facial paralysis is often caused by cholesteatoma, granulation tissue, or direct involvement of a dehiscent nerve. Cholesteatoma erodes the bony canal, compressing the nerve, which is further aided by oedema of the associated inflammatory process, while granulation tissue can invade the nerve sheath. Paralysis in COM is usually insidious and progressive.
Management: Facial paralysis in chronic otitis media requires urgent surgical intervention. The facial canal is carefully explored from the geniculate ganglion to the stylomastoid foramen. If cholesteatoma or granulation tissue invades the canal, uncapping of the canal (decompression) is performed, and overlying tissue is meticulously removed under microscopic or otoendoscopic magnification. Granulations or polyps from the facial sheath should be carefully excised under magnification rather than avulsed. Granulations invading the nerve sheath are left undisturbed to prevent further damage. Nerve resection and grafting are deferred until infection resolution and fibrosis maturation to optimise recovery and minimise complications.
5. Labyrinthitis
Labyrinthitis refers to inflammation of the labyrinth, which can occur secondary to acute otitis media or chronic ear disease. The infection typically spreads via the round window or through preformed fistulae, such as those caused by cholesteatoma or post-stapedectomy complications. Labyrinthitis is classified into four types: circumscribed, diffuse serous, diffuse suppurative, and healed labyrinthitis.
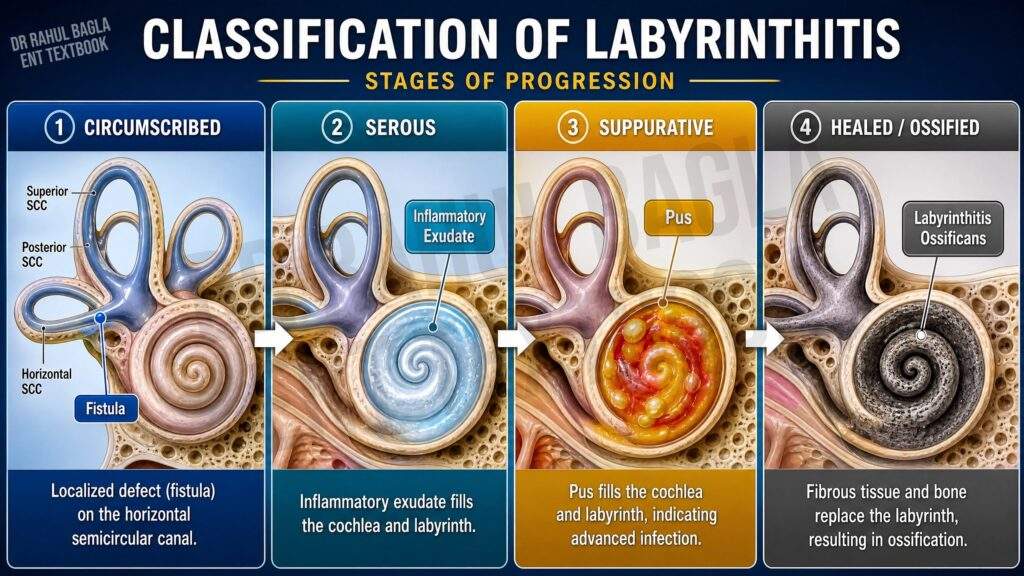
1. Circumscribed Labyrinthitis (Fistula of Labyrinth)
This condition involves thinning or erosion of the bony labyrinth, often affecting the horizontal semicircular canal. It is commonly caused by chronic suppurative otitis media with cholesteatoma, neoplasms of the middle ear, or surgical or accidental trauma to the labyrinth.
Clinical features. Exposure of the membranous labyrinth leads to transient vertigo, triggered by pressure changes (e.g., tragal pressure, ear cleaning, Valsalva manoeuvre). Vertigo is also induced by sound stimuli due to increased labyrinthine sensitivity (Tulio’s phenomenon).
Diagnosis is confirmed using the fistula test, which induces vertigo and nystagmus upon applying pressure to the tragus or using Siegel’s speculum, with the quick component directed towards the affected ear under positive pressure and towards the healthy ear under negative pressure.
Treatment involves mastoid exploration, removal of cholesteatoma, and covering the fistula with a graft (e.g., temporalis fascia, perichondrium or cartilage) with tissue glue reinforcement. During surgery, the cholesteatoma matrix is carefully lifted from the fistula without suctioning. Systemic antibiotics are administered pre- and postoperatively to prevent further infection.
2. Diffuse Serous Labyrinthitis
This reversible condition involves diffuse inflammation of the labyrinth without pus formation. It often arises from circumscribed labyrinthitis, acute middle ear infections, or post-surgical complications (e.g., following stapedectomy or fenestration procedures).
Clinical features. Symptoms include vertigo, nausea, vomiting, and mild to moderate sensorineural hearing loss.
Treatment includes bed rest with head immobilisation, antibiotics, labyrinthine sedatives (e.g., prochlorperazine, dimenhydrinate), steroids (to prevent hearing loss), myringotomy (if ASOM with bulging TM) and vestibular rehabilitation (Cawthorne-Cooksey exercises) post-recovery. Surgical intervention – Cortical mastoidectomy for acute mastoiditis and modified radical mastoidectomy in CSOM or cholesteatoma.
3. Diffuse Suppurative Labyrinthitis
Characterised by pus formation within the labyrinth, this condition leads to permanent loss of vestibular and cochlear function. It results from untreated serous labyrinthitis or pyogenic infections.
Clinical features. Symptoms include very severe vertigo with nausea and vomiting due to acute vestibular failure, spontaneous nystagmus (quick component towards the healthy ear), and total hearing loss. Relief from vertigo is seen after 3–6 weeks due to adaptation. Patients appear toxic and systemically unwell.
Treatment is the same as that of serous labyrinthitis, with rare cases requiring labyrinthine drainage to prevent intracranial complications (e.g. meningitis or brain abscess).
4. Healed Labyrinthitis
This stage follows successful control of suppurative infection, resulting in fibrous tissue formation, calcification, and ossification of the labyrinth (labyrinthitis ossificans). It leads to complete loss of vestibular and auditory function.
Intracranial Complications
1. Extradural abscess
An extradural abscess is characterised by the collection of pus between the bone and the dura mater. It is the most common intracranial complication of both acute and chronic middle ear infections.
Pathology
In acute otitis media, the bone overlying the dura is destroyed by hyperaemic decalcification. In contrast, in chronic otitis media, destruction is caused by cholesteatoma, allowing pus to come into direct contact with the dura. Infection can also spread via venous thrombophlebitis, in which case the bone remains intact. Extradural abscesses often precede complications such as lateral sinus thrombophlebitis or brain abscess. The abscess may develop in relation to the dura of the middle or posterior cranial fossa or outside the dura of the lateral venous sinus (perisinus abscess). As the abscess enlarges, it strips the dura from the bone, forming a sizable mass that exerts pressure on the brain. The affected dura may appear discoloured or covered with granulations.
Clinical Features
Extradural or perisinus abscesses are often asymptomatic and discovered incidentally during mastoidectomy. However, their presence may be suspected in cases of:
- Persistent headache on the side of the affected ear.
- Severe ear pain.
- General malaise with low-grade fever.
- Pulsatile purulent ear discharge.
- Relief of headache following spontaneous drainage of pus.
- Gradenigo’s syndrome (facial pain, diplopia, and aural discharge) due to irritation of the trigeminal (V) and abducens (VI) nerves.
- Subperiosteal abscess or Pott’s puffy tumour if the outer table of the bone erodes.
Diagnosis is confirmed using contrast-enhanced CT or MRI.
Treatment
- Surgical Intervention: Cortical, modified radical, or radical mastoidectomy is performed to address the underlying disease. The abscess is evacuated by removing the overlying bone until healthy dura is exposed. If the tegmen tympani or sinus plate is intact but an abscess is suspected, the bony plate is deliberately removed to drain the pus.
- Antibiotic Therapy: Broad-spectrum antibiotics are administered for 4–6 weeks, and the patient is closely monitored for further intracranial complications such as sinus thrombosis, meningitis, or brain abscess.
2. Subdural Abscess
A subdural abscess is a collection of pus between the dura mater and the arachnoid mater, typically caused by non-hemolytic streptococci, particularly microaerophilic bacteria.
Pathology
Infection spreads from the ear either through bone and dura erosion or via thrombophlebitis, where the intervening bone remains intact. The dura, being a tough barrier, initially prevents infection from reaching the brain. However, prolonged exposure leads to granulation formation and subsequent dural fibrosis. Necrosis of fibrosed dura may allow infection to penetrate. Pus rapidly spreads in the subdural space, accumulating against the cerebral hemisphere’s convex surface, causing pressure symptoms. Initially localised, the abscess can enlarge and extend to the falx cerebri, tentorium cerebelli, and intra-hemispheric spaces, leading to rapid clinical deterioration.
Clinical Features
Symptoms arise from:
- Meningeal Irritation: Headache, high fever (≥102°F), malaise, drowsiness, neck rigidity, and positive Kernig’s sign.
- Cortical Venous Thrombophlebitis: Thrombophlebitis of cerebral veins causes aphasia, hemiplegia, hemianopia, and Jacksonian epilepsy, potentially progressing to status epilepticus.
- Raised Intracranial Tension: Papilloedema, ptosis, dilated pupil (IIIrd nerve involvement), and other cranial nerve deficits.
Diagnosis
Contrast-enhanced CT scan is the primary diagnostic tool. MRI is more reliable if CT findings are equivocal. Lumbar puncture is contraindicated due to the risk of brainstem herniation from raised intracranial pressure.
Treatment
Early diagnosis and prompt surgical and medical management are critical to prevent severe neurological sequelae and improve outcomes in subdural abscess cases. Subdural abscess is a neurological emergency requiring immediate intervention:
- Surgical Drainage: Burr holes or craniotomy are performed to evacuate the empyema.
- Antibiotics: Intravenous antibiotics are administered to control infection.
- Ear Disease Management: Once the infection is controlled, the underlying ear disease is addressed, often requiring mastoidectomy.
3. Meningitis
Meningitis is the inflammation of the pia-arachnoid (leptomeninges) caused by bacterial, viral, fungal, or tubercular infections in the cerebrospinal fluid (CSF) within the subarachnoid space. Common causative organisms include Haemophilus influenzae type B and Streptococcus pneumoniae.
Pathology
The inflammatory process begins with the infiltration of white blood cells into the CSF, followed by bacterial multiplication and the formation of a sticky exudate. This exudate can obstruct CSF flow and spread to the Virchow-Robin spaces, potentially leading to brain abscess formation.
Mode of Infection
In infants and children, meningitis is often blood-borne or typically follows acute otitis media, while in adults, it usually results from chronic ear disease spreading via bone erosion or retrograde thrombophlebitis. In the latter case, it may coexist with extradural abscesses or granulation tissue. Approximately one-third of meningitis cases are associated with other intracranial complications.
Clinical Features
Symptoms and signs arise from infection, raised intracranial tension, and meningeal and cerebral irritation. These include:
- High fever (102–104°F) with chills and rigors.
- Headache and neck rigidity due to irritation of upper cervical nerve roots. Kernig’s and Brudzinski’s signs are positive.
- Photophobia and mental irritability, progressing to drowsiness, delirium, or coma.
- Nausea and vomiting (sometimes projectile due to raised intracranial pressure).
- Cranial nerve palsies, hemiplegia, and, rarely, epileptic fits or focal neurological signs.
Examination reveals neck rigidity, positive Kernig’s and Brudzinski’s signs, exaggerated or sluggish tendon reflexes, and papilloedema in the late stages.
Diagnosis
Contrast-enhanced CT or MRI is used for diagnosis, with MRI being more sensitive for detecting early exudates and adhesions. Lumbar puncture and CSF analysis confirm the diagnosis, showing turbid CSF, elevated cell count (predominantly polymorphs), increased protein, and reduced sugar and chloride levels. Polymerase chain reaction (PCR) can detect bacterial DNA, and CSF culture identifies causative organisms and their antibiotic sensitivity.
Treatment
- Medical Management: High-dose systemic antibiotics, effective against aerobic and anaerobic organisms and capable of crossing the blood-brain barrier, are the cornerstone of treatment. Third-generation cephalosporins, often combined with vancomycin for resistant strains, are commonly used. Dexamethasone is administered along with the antibiotics to reduce neurological sequelae and hearing loss.
- Surgical Management: For meningitis following acute otitis media, myringotomy or cortical mastoidectomy may be required. In cases related to chronic otitis media with cholesteatoma, radical or modified radical mastoidectomy is performed once the patient’s condition stabilises. Surgery is prioritised if there is no response to medical treatment.
4. Otogenic Brain Abscess
Otogenic brain abscesses account for 50% of brain abscesses in adults and 25% in children. The temporal lobe is the most common site for otogenic abscesses, while cerebellar abscesses are predominantly otogenic in origin. In adults, these abscesses typically arise from chronic suppurative otitis media (CSOM) with cholesteatoma, whereas in children, they often result from acute otitis media (AOM).
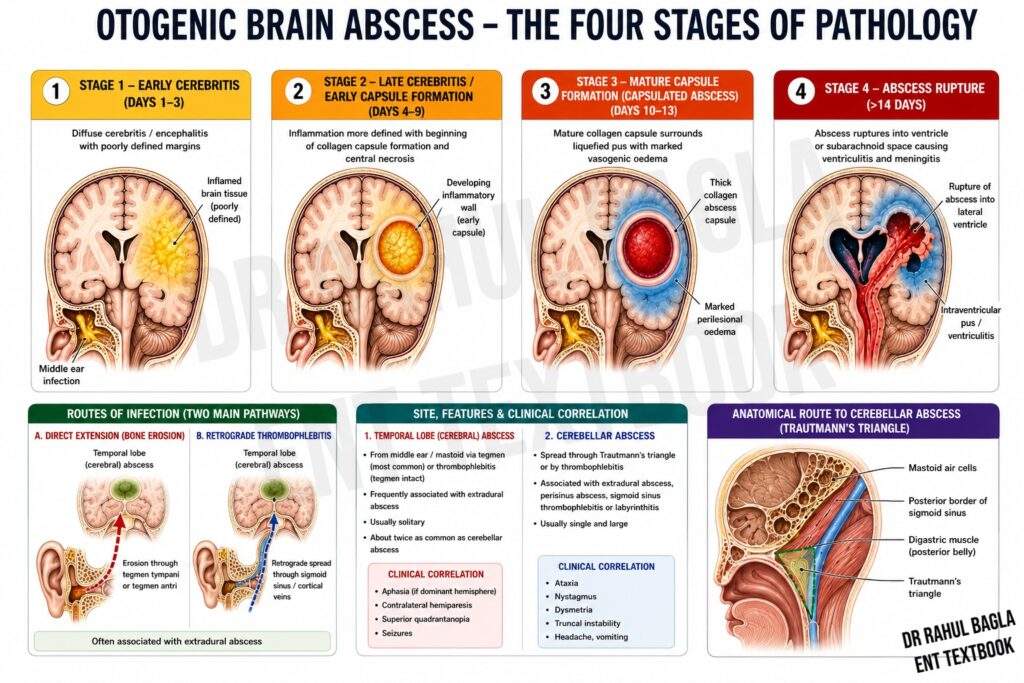
Route of Infection
Brain abscesses develop through direct extension of middle ear infections or retrograde thrombophlebitis.
- Temporal Lobe (cerebral) Abscess:
- Infection spreads from the middle ear or mastoid through the tegmen antri and tympani or via thrombophlebitis where the tegmen remains intact.
- Often associated with extradural abscesses.
- Cerebral abscesses are usually multiple and occur twice as commonly as cerebellar abscesses
- Cerebellar Abscess:
- Infection spreads through Trautmann’s triangle or thrombophlebitis.
- Associated with extradural abscesses, perisinus abscesses, sigmoid sinus thrombophlebitis, or labyrinthitis.
- Cerebellar abscesses are typically single and large.

Bacteriology
Otogenic brain abscesses involve both aerobic and anaerobic organisms:
- Aerobic: Staphylococcus pyogenes, Streptococcus pneumoniae, Streptococcus haemolyticus, Proteus mirabilis, Escherichia coli, and Pseudomonas aeruginosa.
- Anaerobic: Peptostreptococcus and Bacteroides fragilis.
- Haemophilus influenzae is rarely involved.
Pathology
Brain abscesses progress through four stages:
- Stage of Invasion (Initial Encephalitis): The infection spreads into brain tissue, triggering inflammation. Symptoms include mild headache, low-grade fever, malaise, and drowsiness, often going unnoticed.
- Stage of Localisation (Latent Abscess Formation): The body attempts to localize the infection by forming a capsule around the abscess. Symptoms persist with continued headache and fever. This stage may last for several weeks.
- Stage of Enlargement (Manifest Abscess Formation): The abscess grows, leading to significant brain edema. Symptoms worsen, including severe headache, projectile vomiting, papilledema, altered consciousness, and slow pulse. If untreated, herniation and death may result.
- Stage of Termination (Rupture of Abscess): If the abscess ruptures into the ventricles or subarachnoid space, overwhelming meningitis and rapid deterioration follow, often proving fatal.
Clinical Features
Symptoms arise from raised intracranial tension (ICT) and localised brain involvement.
1. Raised Intracranial Tension:
- Severe headache (worse in the morning).
- Nausea and projectile vomiting (more common in cerebellar abscesses).
- Altered consciousness: lethargy → drowsiness → stupor → coma.
- Papilledema (late in cerebral abscesses, early in cerebellar abscesses).
- Slow pulse and subnormal temperature.
2. Localising Features:
Temporal Lobe Abscess:
- Nominal Aphasia: Patients struggle to name objects but can describe their use.
- Homonymous Hemianopia: Loss of vision in the visual field opposite the lesion.
- Contralateral Motor Paralysis: The face is affected first, followed by arm and leg involvement.
- Epileptic Seizures: Hallucinations of taste and smell, involuntary lip and tongue movements.
- Pupillary Changes and Oculomotor Palsy: Signifies transtentorial herniation.
Cerebellar Abscess:
- Gait Disturbances and Incoordination: Ipsilateral weakness and difficulty in walking.
- Spontaneous Nystagmus: Irregular eye movements directed toward the lesion.
- Ipsilateral Hypotonia and Ataxia: Staggering gait towards the affected side.
- Past Pointing and Intention Tremor: Identified using the finger-to-nose test.
- Dysdiadochokinesia: Impaired rapid alternating hand movements.
- Suboccipital Headache with Neck Rigidity: Early symptoms indicative of posterior fossa involvement.
Investigations
- CT Scan with Contrast: Shows a hypodense abscess cavity with peripheral enhancement (“ring sign”). It identifies size, location, and associated complications (e.g., extradural abscess, sinus thrombosis).
- MRI: Differentiates abscess from edema or normal brain tissue.
- X-ray/CT of Temporal Bone: Evaluates underlying ear disease.
- Lumbar Puncture: Performed cautiously after reducing ICT. CSF shows elevated pressure, increased protein, normal glucose, and raised white cell count.
Treatment
Medical Management:
- Antibiotics: High-dose intravenous therapy targeting both aerobic and anaerobic pathogens. Commonly used drugs include third-generation cephalosporins, chloramphenicol, and metronidazole. Aminoglycosides (e.g., gentamicin) may be required for Gram-negative coverage.
- Anticonvulsants: Given the high risk of seizures, long-term prophylaxis is necessary for temporal lobe abscesses.
- Intracranial Pressure Management: Dexamethasone (4 mg IV every 6 hours) and mannitol (0.5 g/kg body weight) help reduce cerebral oedema.
- Ear Infection Management: Suction clearance and topical antibiotics address the underlying otologic infection.
Neurosurgical Management:
- Aspiration via Burr Hole: Performed repeatedly to evacuate pus and reduce mass effect.
- Abscess Excision: Complete removal of the abscess in selected cases.
- Open Abscess Drainage: Ensures thorough evacuation and reduces recurrence risk.
- The cerebral abscesses may be drained through Trautman’s triangle.
- Follow-up: Repeat CT/MRI to monitor abscess size.
- Pus Culture: Guides antibiotic therapy.
Otologic Management:
- Acute Otitis Media: Resolves with systemic antibiotics.
- Chronic Otitis Media: Radical mastoidectomy to remove cholesteatoma and infected tissue.
- Timing: Ear surgery is performed after controlling the abscess and reducing ICT.
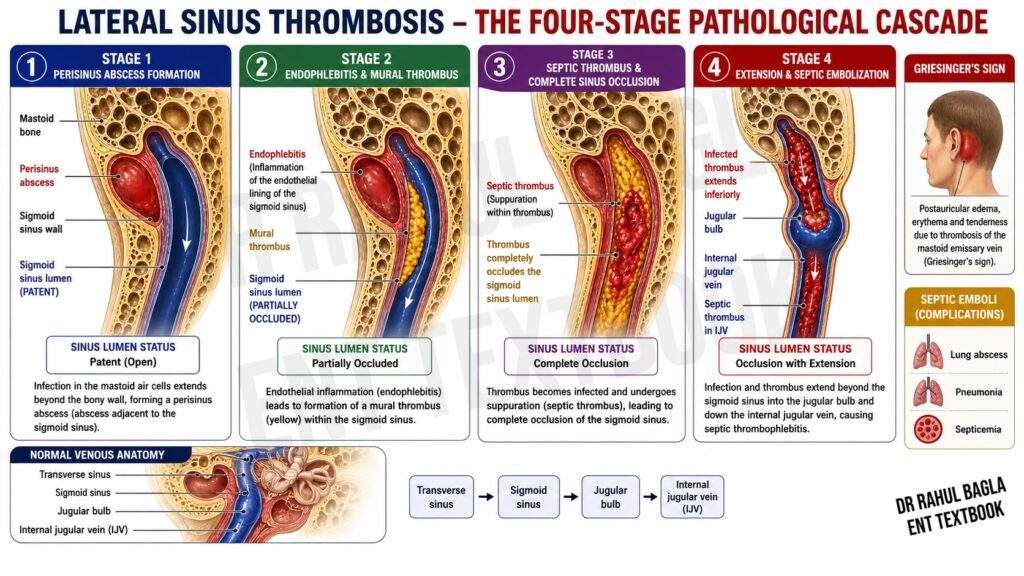
5. Lateral Sinus Thrombophlebitis (Syn. Sigmoid Sinus Thrombosis)
Lateral sinus thrombophlebitis is an inflammation of the inner wall of the lateral venous sinus, accompanied by the formation of an intrasinus thrombus. It is a serious complication of otogenic infections, arising from acute coalescent mastoiditis, masked mastoiditis, or chronic suppurative otitis media with cholesteatoma.
Aetiology
The condition typically results from the spread of infection from the middle ear or mastoid to the lateral sinus. In acute infections, it is often associated with acute coalescent mastoiditis, while in chronic cases, it is linked to cholesteatoma.
Pathology
The pathological progression of lateral sinus thrombophlebitis occurs in four stages:
- Formation of Perisinus Abscess: An abscess forms adjacent to the outer dural wall of the sinus. The overlying bony plate may be eroded by infection or remain intact if the route of spread is thrombophlebitic.
- Endophlebitis and Mural Thrombus Formation: Inflammation of the sinus wall leads to the deposition of fibrin, platelets, and blood cells, forming a mural thrombus.
- Obliteration of Sinus Lumen and Intrasinus Abscess: The thrombus enlarges, occluding the sinus lumen. Bacterial invasion of the thrombus can result in an intrasinus abscess, releasing septic emboli into the bloodstream and causing septicaemia.
- Extension of Thrombus: The thrombus may extend proximally to the confluence of sinuses, superior sagittal sinus, or cavernous sinus, and distally to the mastoid emissary vein, jugular bulb, or jugular vein.
Bacteriology
- Acute Infections: Commonly caused by Streptococcus haemolyticus, Streptococcus pneumoniae, or Staphylococcus aureus.
- Chronic Infections: Often involve Proteus mirabilis, Pseudomonas aeruginosa, Escherichia coli, and Staphylococcus
Clinical Features
- Hectic Picket-Fence Fever: Irregular fever with spikes, chills, rigors, and profuse sweating, resembling malaria but lacking regularity. Patients may appear well between fever episodes.
- Headache: Mild initially due to perisinus abscess; severe later from raised intracranial pressure.
- Progressive Anaemia and Emaciation: Resulting from chronic infection and septicaemia.
- Griesinger’s Sign: Oedema over the posterior mastoid due to thrombosis of the mastoid emissary vein.
- Papilloedema: Occurs with venous obstruction, more common with right sinus thrombosis or extension to the superior sagittal sinus.
- Tobey–Ayer Test: Compression of the jugular vein on the thrombosed side produces no rise in CSF pressure, while compression on the healthy side causes a rapid increase.
- Crowe–Beck Test: Compression of the healthy jugular vein engorges retinal and supraorbital veins, which subside upon release.
- Tenderness Along Jugular Vein: Indicates thrombophlebitis extending to the jugular vein, often accompanied by lymphadenopathy and torticollis.
Investigations
1. Blood Smear and Culture: To rule out malaria and identify causative organisms.
2. CSF Examination: Normal except for elevated pressure; helps exclude meningitis.
3. Imaging Studies:
- CT Scan: Shows the “delta sign” (rim-enhancing thrombus with central low density).
- MRI/MR Venography: Better delineates the thrombus and assesses progression.
4. Ear Swab Culture: Identifies pathogens and guides antibiotic therapy.
Complications
- Septicaemia and metastatic abscesses in the lungs, bones, joints, or subcutaneous tissue.
- Meningitis and subdural abscess.
- Cerebellar abscess.
- Jugular bulb and vein thrombosis with cranial nerve involvement (IX, X, XI).
- Cavernous sinus thrombosis (chemosis, proptosis, papilloedema).
- Otitic hydrocephalus due to sagittal sinus thrombosis.
Treatment
1. Medical Management:
- Antibiotics: High-dose intravenous antibiotics based on culture and sensitivity.
- Anticoagulants: Rarely used, except for extending thrombosis to the cavernous sinus.
- Supportive Care: Blood transfusions for anaemia and improved resistance.
2. Surgical Management:
Mastoidectomy:
- Cortical or modified radical mastoidectomy to address the underlying ear disease.
- Removal of the sinus bony plate to expose and drain the perisinus abscess.
- Incision of the sinus dura to evacuate infected clots or abscesses, with packing above and below the sinus to control bleeding.
Ligation of Internal Jugular Vein: Rarely required; indicated for uncontrolled embolic phenomena or spreading jugular vein tenderness.
3. Postoperative Care:
- Packs are removed 5–6 days postoperatively, and the wound is closed secondarily.
- Antibiotics are continued for at least one week post-surgery.
6. Otitic Hydrocephalus
Otitic hydrocephalus is a condition characterised by raised intracranial pressure (ICP) with normal cerebrospinal fluid (CSF) findings. It typically occurs in children and adolescents with acute or chronic middle ear infections. The condition arises due to lateral sinus thrombosis, which obstructs venous return. If the thrombosis extends to the superior sagittal sinus, it further impairs the function of arachnoid villi, reducing CSF absorption. These factors collectively lead to increased intracranial tension.
Symptoms
Clinically, patients present with severe, sometimes intermittent headaches, often accompanied by nausea and vomiting. Diplopia due to abducens nerve (VI) palsy and blurred vision from papilloedema or optic atrophy are common.
Examination
Reveals significant papilloedema (5–6 diopters), sometimes with exudates and haemorrhages, and nystagmus due to raised ICP. Lumbar puncture shows elevated CSF pressure (>300 mm H₂O), though the fluid is otherwise normal in cell count, protein, sugar content, and sterility.
Treatment
Focuses on reducing CSF pressure to prevent optic atrophy and blindness. Medical management includes acetazolamide and corticosteroids, along with repeated lumbar punctures or placement of a lumbar drain. In refractory cases, a lumboperitoneal shunt may be necessary to divert CSF into the peritoneal cavity. The underlying middle ear infection requires antibiotic therapy, and mastoid exploration may be needed to address sinus thrombosis. Early intervention is crucial to prevent permanent visual and neurological damage.
———— End of the chapter ————
High-Yield Points for NEET PG & University Exams
- Most common intracranial complication of CSOM: Extradural abscess
- Most common site of otogenic brain abscess: Temporal lobe
- Gradenigo’s syndrome: Triad of diplopia (VI nerve palsy), deep-seated ear/retro-orbital pain (V nerve involvement), and persistent ear discharge
- Bezold abscess: Pus tracking from mastoid tip into neck along sternocleidomastoid or digastric muscle
- Griesinger’s sign: Oedema over posterior mastoid due to mastoid emissary vein thrombosis
- Tobey-Ayer test: Positive when jugular compression on thrombosed side produces no CSF pressure rise
- Fistula test: Induces vertigo and nystagmus with positive pressure (towards affected ear) and negative pressure (towards healthy ear)
- Reservoir sign: Ear canal rapidly refills with pus after cleaning
- Delta sign: Rim-enhancing thrombus with central low density on CT – seen in lateral sinus thrombosis
- Most common organism in acute mastoiditis: Streptococcus pneumoniae
- Most common organism in chronic mastoiditis: Pseudomonas aeruginosa
- Sagging of posterosuperior meatal wall: Pathognomonic of acute mastoiditis
- Masked mastoiditis: Subclinical gradual destruction of mastoid air cells without acute symptoms
- “Ring sign” on CT: Characteristic of brain abscess
- Tulio’s phenomenon: Vertigo induced by sound in circumscribed labyrinthitis
- Labyrinthitis ossificans: End-stage labyrinthitis with ossification of inner ear
- Temporal lobe abscess: Causes nominal aphasia, homonymous hemianopia, contralateral motor paralysis
- Cerebellar abscess: Causes ataxia, intention tremor, dysdiadochokinesia, suboccipital headache
- Pott’s puffy tumour: Subperiosteal abscess with frontal bone osteomyelitis
- Citelli’s abscess: Abscess behind mastoid, closer to occipital bone
NEET PG-Style MCQs with Answers & Explanations
- The most common intracranial complication of chronic suppurative otitis media is: A. Meningitis B. Brain abscess C. Extradural abscess D. Lateral sinus thrombophlebitis.
- Gradenigo’s syndrome includes all EXCEPT: A. Diplopia B. Retro-orbital pain C. Persistent ear discharge D. Facial paralysis.
- The fistula test is positive in: A. Diffuse suppurative labyrinthitis B. Circumscribed labyrinthitis C. Diffuse serous labyrinthitis D. Otitic hydrocephalus.
- Sagging of the posterosuperior meatal wall is seen in: A. Otitis externa B. Acute mastoiditis C. Petrositis D. Labyrinthitis.
- The most common organism causing acute mastoiditis is: A. Pseudomonas aeruginosa B. Staphylococcus aureus C. Streptococcus pneumoniae D. Haemophilus influenzae.
- The reservoir sign indicates: A. Cerebrospinal fluid leak B. Pus under tension in mastoid C. Thickened tympanic membrane D. Cholesterol granuloma.
- Which of the following is NOT an intratemporal complication of CSOM? A. Acute mastoiditis B. Petrositis C. Subdural abscess D. Facial paralysis.
- The delta sign on CT is characteristic of: A. Brain abscess B. Extradural abscess C. Lateral sinus thrombophlebitis D. Subdural abscess.
- The most common site of otogenic brain abscess is: A. Frontal lobe B. Parietal lobe C. Temporal lobe D. Cerebellum.
- In lateral sinus thrombosis, compression of the healthy jugular vein causes: A. No change in CSF pressure. B. Rise in CSF pressure C. Fall in CSF pressure D. Fluctuating CSF pressure.
MCQs Answers: 1: C. 2: D. 3: B. 4: B. 5: C. 6: B. 7: C. 8: C. 9: C. 10: B.
Clinical Case Scenarios for Practical Exams & Viva
Case 1: Acute Mastoiditis with Subperiosteal Abscess
A 5-year-old child presents with right-sided earache, fever, and swelling behind the right ear for 3 days. Mother reports that the child had an ear infection 2 weeks ago, which was treated with oral antibiotics. On examination, the child is febrile (101°F). There is a tender, fluctuant swelling over the right mastoid that has pushed the pinna forward and downward. Otoscopy reveals a small central perforation with pulsatile purulent discharge and sagging of the posterosuperior meatal wall.
Most likely diagnosis: Acute mastoiditis with subperiosteal abscess.
Best next step: Hospitalization + IV antibiotics + Cortical mastoidectomy with incision and drainage of subperiosteal abscess.
Viva questions:
- What are the stages of acute mastoiditis?
- What are the indications for cortical mastoidectomy?
- What organisms are most commonly involved?
- How do you differentiate this from otitis externa?
Case 2: Gradenigo Syndrome
A 45-year-old female with known chronic suppurative otitis media presents with severe right-sided headache, retro-orbital pain, and double vision for the past week. She also reports persistent foul-smelling ear discharge. Examination reveals right-sided abducens nerve palsy.
Most likely diagnosis: Petrositis with Gradenigo syndrome.
Best investigation: Contrast-enhanced CT and MRI of temporal bone.
Management: High-dose IV antibiotics (2-3 weeks) + Modified radical mastoidectomy.
Viva questions:
- What is Gradenigo’s syndrome?
- What are the cell tracts involved in petrositis?
- What is the role of imaging in this condition?
Case 3: Otogenic Brain Abscess
A 30-year-old male with long-standing CSOM presents with severe headache, projectile vomiting, and altered consciousness. Examination reveals papilloedema and nominal aphasia. CT scan shows a ring-enhancing lesion in the right temporal lobe.
Most likely diagnosis: Temporal lobe abscess secondary to CSOM.
Best management: IV antibiotics + anticonvulsants + Neurosurgical aspiration/drainage + Radical mastoidectomy (after abscess control).
Viva questions:
- What is the most common site for otogenic brain abscess?
- What are the stages of brain abscess formation?
- What is the role of steroids in brain abscess management?
- When should the ear surgery be performed?
Case 4: Lateral Sinus Thrombophlebitis
A 25-year-old male with acute otitis media develops high-grade fever with chills and rigors. The fever spikes every evening, and the patient appears relatively well between episodes. Examination reveals tenderness over the right mastoid and oedema over the posterior mastoid area. Fundoscopy shows papilloedema.
Most likely diagnosis: Lateral sinus thrombophlebitis.
Best investigation: MRI/MR venography showing thrombus in the sigmoid sinus.
Management: IV antibiotics + Cortical mastoidectomy + Sinus exploration and drainage.
Viva questions:
- What is the characteristic fever pattern?
- What is Griesinger’s sign?
- Describe the Tobey-Ayer test and its significance.
- What are the complications of lateral sinus thrombosis?
Case 5: Meningitis Following CSOM
A 60-year-old diabetic patient with CSOM presents with high fever, severe headache, neck rigidity, and photophobia. Examination reveals positive Kernig’s and Brudzinski’s signs. CSF analysis shows turbid fluid with elevated polymorphs, increased protein, and decreased glucose.
Most likely diagnosis: Acute bacterial meningitis secondary to CSOM.
Best management: High-dose IV antibiotics (covering both aerobic and anaerobic organisms) + Dexamethasone + Address underlying ear disease (myringotomy or mastoidectomy after stabilisation).
Viva questions:
- What organisms are most commonly involved?
- What CSF findings are characteristic?
- What is the role of dexamethasone?
- When should the ear surgery be performed?
Frequently Asked Questions in Viva
- Q: What is the difference between complications and sequelae of CSOM?
A: Complications are acute, life-threatening conditions developing during active infection (like meningitis or brain abscess), while sequelae are long-term consequences of chronic infection (like hearing loss or tympanosclerosis). - Q: Why are the terms “safe” and “unsafe” CSOM no longer used?
A: Recent studies show that both mucosal-type and squamosal-type CSOM carry significant complication risks, with intracranial complications seen in both types. Therefore, these terms are obsolete. - Q: What is the most common intracranial complication of CSOM?
A: Extradural abscess is the most common intracranial complication, often discovered incidentally during mastoidectomy. - Q: What is the first-line treatment for acute mastoiditis?
A: Hospitalization with IV antibiotics (amoxicillin or ampicillin) combined with myringotomy if pus is under tension. Surgical intervention (cortical mastoidectomy) is indicated in severe cases. - Q: How does infection spread from the middle ear to the brain?
A: Infection spreads through three mechanisms: direct bone erosion, venous thrombophlebitis (through emissary veins), and preformed anatomical pathways (congenital dehiscences, surgical defects, or fractures). - Q: What is Gradenigo’s syndrome and what does it indicate?
A: Gradenigo’s syndrome is the triad of diplopia (VI nerve palsy), deep-seated ear/retro-orbital pain (V nerve involvement), and persistent ear discharge. It indicates petrositis. - Q: What is the difference between cortical and modified radical mastoidectomy?
A: Cortical mastoidectomy removes mastoid air cells while preserving middle ear structures. Modified radical mastoidectomy removes disease while preserving hearing structures (ossicular chain) when possible. - Q: When should mastoidectomy be performed in cases of intracranial complications?
A: For meningitis following CSOM, surgery is performed after the patient stabilises. For brain abscess, surgery is performed after abscess control. However, if there is no response to medical treatment, urgent surgery is indicated. - Q: What is the role of lumbar puncture in CSOM complications?
A: Lumbar puncture is crucial for diagnosing meningitis but is contraindicated in cases of brain abscess or suspected raised intracranial pressure due to risk of brainstem herniation. - Q: What is the prognosis of facial nerve paralysis in CSOM?
A: In acute otitis media, prompt treatment usually results in full recovery. In chronic otitis media, the prognosis depends on the extent of nerve damage; decompression and removal of cholesteatoma can improve outcomes. - What are the complications of CSOM? Complications are classified into intratemporal and intracranial complications, including mastoiditis, facial paralysis, labyrinthitis, meningitis, brain abscess, and lateral sinus thrombosis
- Can CSOM cause hearing loss? Yes. CSOM can cause both conductive hearing loss due to tympanic membrane or ossicular damage and sensorineural hearing loss if the labyrinth becomes involved.
- Is CSOM life-threatening? Yes. Untreated CSOM can lead to meningitis, brain abscess, lateral sinus thrombosis, and otitic hydrocephalus, all of which can be life-threatening.
- What is the most common intratemporal complication? Acute mastoiditis.
- What is the most dangerous intracranial complication? Brain abscess.
- What is the biggest risk factor? Cholesteatoma.
- Which imaging is preferred? HRCT temporal bone for temporal bone disease and contrast-enhanced CT or MRI for intracranial complications.
- When is mastoidectomy indicated? Persistent infection despite antibiotics, abscess formation, cholesteatoma, facial paralysis, labyrinthitis, or intracranial complications.
- Can CSOM cause facial paralysis? Yes. Facial nerve paralysis may occur due to cholesteatoma, osteitis, or direct nerve involvement and requires urgent management.
- What is the best way to prevent complications? Early diagnosis, culture-directed antibiotics, regular follow-up, and timely surgical management when indicated.
———— End ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords:Complications of Chronic Suppurative Otitis Media, CSOM complications and treatment, Long-term effects of CSOM, Risks of untreated Chronic Suppurative Otitis Media, CSOM and hearing loss, What are the complications of CSOM? How does CSOM lead to hearing loss? Can CSOM cause brain abscesses? Symptoms of CSOM complications, Is CSOM life-threatening? How to prevent complications of Chronic Suppurative Otitis Media, CSOM and facial nerve paralysis, CSOM and cholesteatoma formation, Best treatment for CSOM complications, CSOM and meningitis risk, Early signs of CSOM complications, How to manage CSOM to avoid complications, CSOM complications in adults vs. children, Can CSOM cause permanent damage? What happens if CSOM is left untreated? CSOM and ear discharge complications, How to diagnose CSOM complications, CSOM and vertigo connection, CSOM and tinnitus causes, Surgical options for CSOM complications”Complications of CSOM: Risks, Symptoms, and How to Prevent Them””Chronic Suppurative Otitis Media (CSOM): Understanding Its Complications and Treatments””CSOM Complications: From Hearing Loss to Life-Threatening Risks””What Happens If CSOM Is Left Untreated? Key Complications Explained””CSOM and Its Long-Term Effects: A Guide to Complications and Prevention” /p>
I like to learn ent