|
The following CBME core competencies are covered in this chapter.
|
Rehabilitation of the Hearing Impaired
What is Aural Rehabilitation?
Hearing loss rehabilitation (aural rehabilitation) is the process of restoring communication abilities in individuals with hearing impairment through a combination of instrumental devices (hearing aids, cochlear implants, BAHA, ABI) and training programs (auditory training, speech reading, speech conservation). Aural rehabilitation is essential for individuals with hearing loss to improve communication and quality of life. It encompasses a combination of instrumental devices and training programs tailored to the individual’s needs.
Components of Aural Rehabilitation
1. Instrumental Devices
a. Hearing Aids
- Conventional Hearing Aids: Amplify sound for individuals with residual hearing.
- Bone-Anchored Hearing Aids (BAHA): Transmit sound via bone conduction, ideal for conductive or mixed hearing loss and single-sided deafness.
- Implantable Hearing Aids: Surgically implanted devices that enhance sound transmission, suitable for moderate to severe hearing loss.
b. Implants
- Cochlear Implants: Directly stimulate the auditory nerve, enabling sound perception for individuals with severe-to-profound sensorineural hearing loss.
- Auditory Brainstem Implants (ABI): Used for individuals with non-functional auditory nerves, stimulating the brainstem directly.
c) Assistive Devices for the Deaf. Include devices like FM systems, infrared systems, and captioning tools to improve accessibility in various environments.
2. Training Programs
- Speech (Lip) Reading. Teaches individuals to interpret visual cues from lip movements, facial expressions, and gestures to understand speech.
- Auditory Training. Focuses on improving the ability to recognise and interpret sounds, especially for new hearing aid or cochlear implant users.
- Speech Preservation (Speech Conservation). Helps individuals maintain clear speech by practising articulation, pitch, and volume control – used mainly in post-lingually deafened adults.
Conventional Hearing Aids
How Hearing Aids Work
A hearing aid is an electronic device designed to amplify sounds for individuals with hearing loss. It consists of three essential components: (1) a microphone, which captures sound and converts it into electrical signals; (2) an amplifier, which increases the strength of these signals (amplification); and (3) a receiver, which transforms the amplified signals back into sound. This sound is then delivered to the ear through an ear mould, enhancing the user’s ability to hear.
Conventional hearing aids may be classified as analog or digital. Analog hearing aids amplify all incoming sounds equally and provide limited flexibility for individual hearing loss patterns. Digital hearing aids convert sound into digital signals, allowing frequency-specific amplification, noise reduction, feedback suppression, speech enhancement, and programmable settings according to the patient’s audiogram. Modern hearing aids are almost exclusively digital because they provide superior speech understanding and listening comfort, particularly in noisy environments.
Modern digital hearing aids incorporate several advanced features, including directional microphones, digital noise reduction, feedback cancellation, automatic environmental adaptation, frequency-specific amplification, and Bluetooth connectivity. Bluetooth-enabled hearing aids can connect wirelessly to smartphones, televisions, computers, and remote microphones, allowing direct audio streaming and improved speech understanding in challenging listening environments. Many contemporary hearing aids also use rechargeable lithium-ion batteries, eliminating the need for frequent battery replacement.
Types of Hearing Aids
Hearing aids are broadly categorised into two types: air conduction and bone conduction.
- Air conduction hearing aids transmit amplified sound through the ear canal to the tympanic membrane, making them suitable for most users.
- Bone conduction hearing aids use a bone vibrator placed on the mastoid to directly stimulate the cochlea, making them ideal for individuals with conditions like actively draining ears, otitis externa, or ear canal atresia, where traditional ear inserts cannot be worn.
Types of Air Conduction Hearing Aids
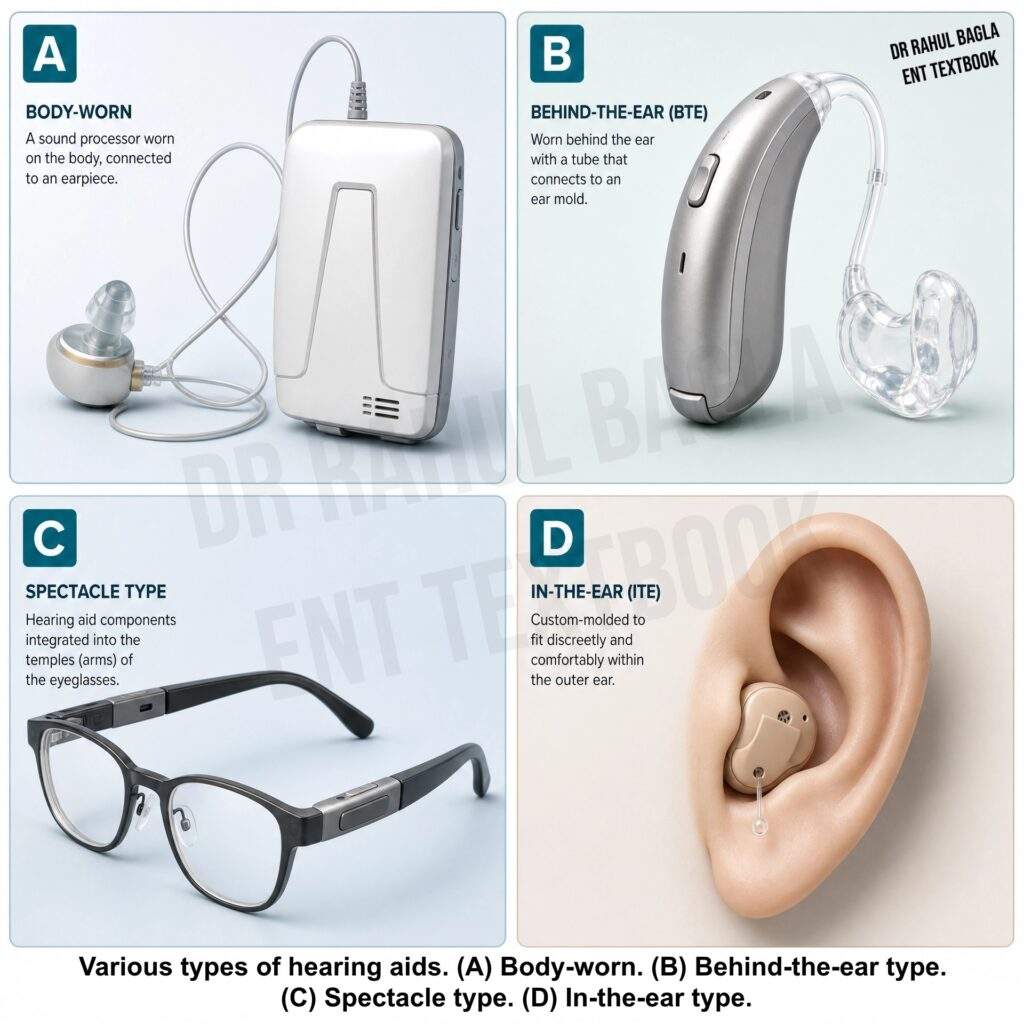
- Body-Worn Hearing Aids: The microphone, amplifier, and battery are housed in a case worn at chest level, while the receiver is placed at ear level. These hearing aids offer high amplification with minimal feedback, making them suitable for severe hearing loss or congenital deafness in children.
- Behind-the-Ear (BTE) Hearing Aids: All components are integrated into a single unit worn behind the ear, connected to the ear canal via tubing and an ear mould. These are ideal for mild to moderate hearing loss, particularly high-frequency loss. In children, BTE hearing aids are the preferred choice because they accommodate growing ear canals, provide greater amplification, and are compatible with FM systems and other assistive listening devices.
- Receiver-in-Canal (RIC) hearing aids: They are similar in appearance to Behind-the-Ear (BTE) hearing aids, but the receiver (speaker) is placed inside the external auditory canal and connected to the main body by a thin wire. This design reduces sound distortion, improves sound quality, minimises acoustic feedback, and provides better cosmetic appearance. RIC hearing aids are currently among the most commonly prescribed hearing aids for adults with mild to severe sensorineural hearing loss.
- Spectacle Hearing Aids: The hearing aid is embedded in the frame of eyeglasses. These are useful for individuals requiring both vision correction and hearing assistance, though less popular today.
- In-the-Ear (ITE) Hearing Aids: The entire device is housed within a custom earmould that fits inside the ear. Popular for mild to moderate hearing loss due to its cosmetic appeal.
- Canal Hearing Aids (ITC and CIC): Compact devices that fit entirely within the ear canal, with two subtypes: In-the-Canal (ITC) and Completely-in-the-Canal (CIC). Suitable for mild to moderate high-frequency hearing loss (1-4KHz), requiring a wide ear canal and user dexterity for operation.
Indications for Hearing Aids
Hearing aids are recommended for individuals with hearing loss that cannot be addressed medically or surgically. Key indications include:
- Sensorineural Hearing Loss: For those whose daily activities are affected, though some may experience sound distortion or recruitment.
- Deaf Children: Early fitting of binaural aids (one for each ear) is crucial for speech and language development, often combined with lip-reading training. Children with permanent bilateral hearing loss should be fitted with bilateral hearing aids as early as possible, preferably before 6 months of age, to facilitate normal speech, language and cognitive development. Family participation and auditory-verbal rehabilitation are essential for optimal outcomes.
- Conductive Hearing Loss: Used when surgery is refused, not feasible, or unsuccessful.
Fitting a Hearing Aid
The fitting process considers several factors:
- Degree and configuration of hearing loss (type of frequencies affected).
- Type of hearing loss (conductive or sensorineural).
- Presence of recruitment or uncomfortable loudness levels.
- Patient’s age, dexterity, and cosmetic preferences.
- Condition of the outer and middle ear.
- Type of ear mould and fitting (monoaural, binaural, or contralateral routing of signals).
- Bilateral hearing aids are preferred over unilateral fitting, especially in patients with bilateral hearing loss. Bilateral amplification improves sound localisation, speech perception in noisy environments, overall hearing performance, and listening comfort while reducing the amount of amplification required in each ear.
Disadvantages of Conventional Hearing Aids
- Cosmetic Concerns: Visibility of the device may be undesirable.
- Acoustic Feedback: Whistling sounds due to sound leakage.
- Spectral Distortion: Altered sound quality.
- Occlusion Effect: Blockage of the ear canal, leading to discomfort and wax buildup.
- Skin Sensitivity: Irritation from ear moulds.
- Discharging Ears: Difficult to use in cases of active ear discharge.
CROS Hearing Aids
Contralateral Routing of Signals (CROS) aids are designed for individuals with unilateral severe hearing loss. A microphone fitted on the deaf ear transmits sound to a receiver fitted in the better-hearing ear, which helps in sound localisation coming from the side of the deaf ear. However, in noisy environments, bone-anchored hearing aids are often preferred as they offer superior speech recognition.
Bone-Anchored Hearing Aid (BAHA)
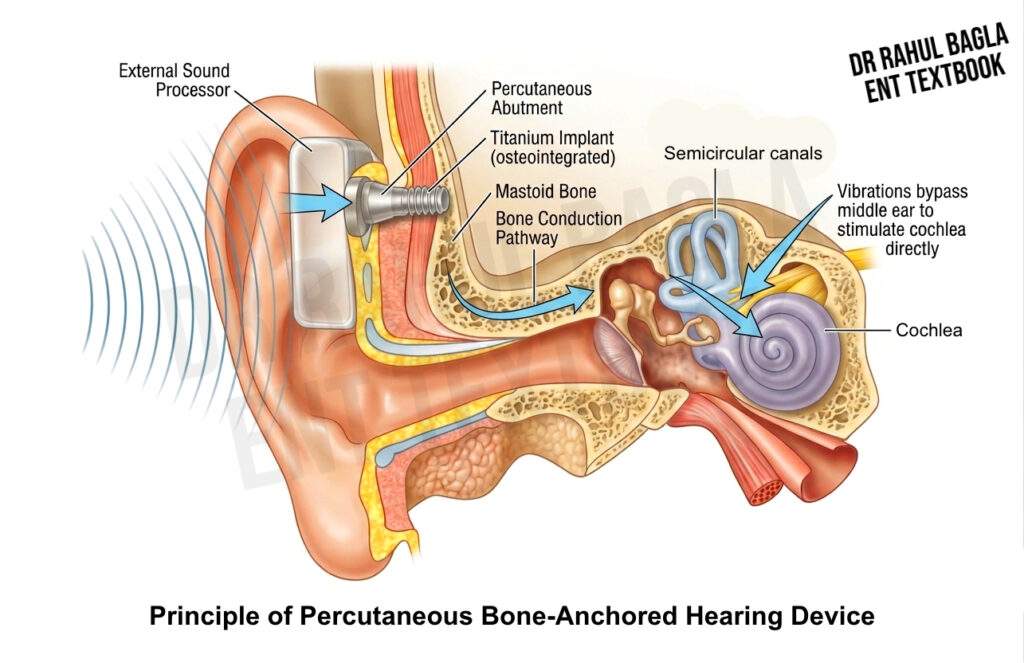
The Bone-Anchored Hearing Aid (BAHA) is a specialised hearing device that operates on the principle of bone conduction. It is particularly beneficial for individuals with conductive hearing loss, mixed hearing loss or unilateral hearing loss, who are unable to use traditional “in-the-ear” or “behind-the-ear” hearing aids. By bypassing the external auditory canal and middle ear, BAHA directly transmits sound vibrations through the skull bone to the cochlea, offering an effective auditory solution for those with specific hearing impairments.
Types of Bone-Anchored Hearing Devices
Bone-anchored hearing devices are broadly classified into two types:
- Percutaneous Bone-Anchored Hearing Devices: These devices consist of a titanium implant fixed within the skull bone, connected to an external sound processor through a skin-penetrating abutment. Sound vibrations are transmitted directly from the processor to the skull, providing excellent sound transmission. However, local skin infection, soft tissue overgrowth, and failure of osseointegration may occur around the abutment.
- Transcutaneous Bone-Anchored Hearing Devices: These devices transmit sound through intact skin using magnetic coupling between the implanted internal magnet and the external sound processor. As there is no skin-penetrating abutment, transcutaneous systems have superior cosmetic appearance and significantly lower rates of skin infection and soft tissue complications. However, transmission efficiency may be slightly lower due to attenuation by the intervening skin and soft tissues.
How BAHA Works
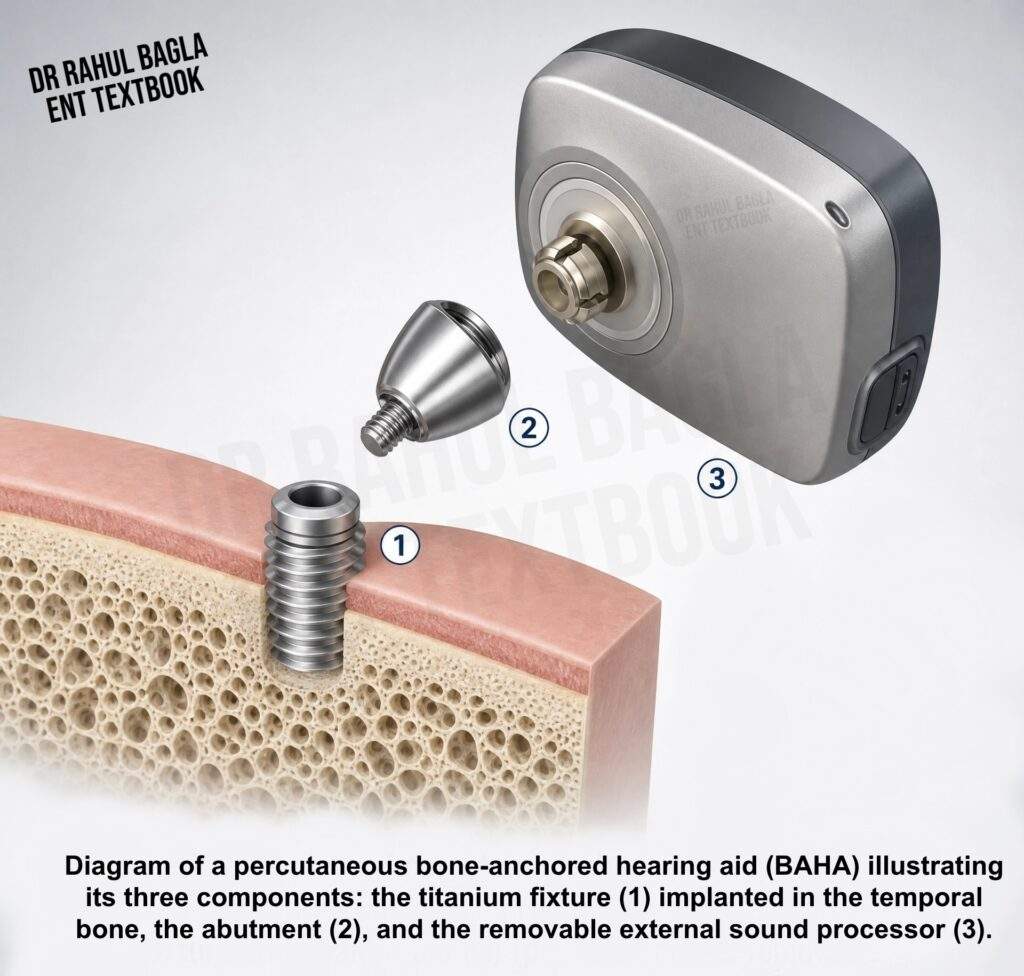
The BAHA system consists of three key components:
- Titanium Fixture: Surgically implanted into the skull bone.
- Titanium Abutment: Attached to the fixture and protruding through the skin.
- Sound Processor: Externally attached to the abutment.
The titanium fixture undergoes osseointegration, a process where it fuses with the surrounding bone tissue over 2–6 months. Once osseointegration is complete, the sound processor is connected to the abutment. The device captures sound waves, converts them into vibrations, and transmits these vibrations through the skull to the cochlea, enabling sound perception.
BAHA Surgical Procedure
- Adults: BAHA implantation is usually performed as a single-stage procedure, in which the titanium implant is placed during one operation, followed by attachment and activation of the sound processor after adequate osseointegration.
- Children: A two-stage approach is recommended. The titanium fixture is implanted in the first stage, followed by a second procedure 6 months later to connect the abutment.
Complications
While BAHA is generally safe, potential complications include:
- Failure of osseointegration.
- Localised infections or inflammation at the implant site.
Candidacy for BAHA
BAHA is recommended for individuals who meet the following criteria:
- Chronic Ear Conditions: Patients with persistent ear canal infections or inflammation that prevent the use of conventional air-conduction hearing aids.
- Congenital Malformations: Children with microtia or canal atresia (malformed or absent outer ear and ear canals).
- Single-Sided Deafness (SSD): Individuals with hearing loss in one ear. For patients with SSD, BAHA offers a significant advantage over traditional CROS hearing aids in noisy environments. Unlike CROS aids, which have limitations in performance, BAHA is implanted on the deaf side and transmits sound via bone conduction to the functional cochlea on the opposite side. This eliminates the “head shadow” effect, improving speech recognition in both quiet and noisy environments.
- Trial with soft band: Before permanent implantation, patients should undergo a trial with a softband or headband bone-conduction hearing device whenever feasible. This trial allows assessment of expected hearing benefit, patient comfort, and acceptance of the device before surgery.
Indications for BAHA
BAHA is indicated in the following scenarios:
1. When Air-Conduction Hearing Aids Are Ineffective:
- Children with microtia or canal atresia (malformed or absent outer ear and ear canals).
- Chronic ear discharge is unresponsive to treatment.
- Discomfort or excessive feedback from air-conduction devices.
2. Conductive, Mixed, and Selected Mild-to-Moderate Sensorineural Hearing Loss: Bone-anchored hearing devices are indicated in patients with conductive hearing loss, mixed hearing loss, and selected patients with mild-to-moderate sensorineural hearing loss who cannot obtain adequate benefit from conventional hearing aids or are unable to wear them.
3. Single-Sided Deafness: To restore binaural hearing and improve auditory localisation.
Implantable Hearing Aids
Implantable middle ear hearing aids represent an innovative category of hearing devices that operate on the principle of direct drive. Unlike traditional hearing aids, which deliver sound acoustically through the ear canal, these devices use mechanical vibrations to directly stimulate the ossicular chain, leaving the ear canal open. This approach offers a unique solution for individuals with moderate-to-severe sensorineural hearing loss who seek an alternative to conventional hearing aids.
Types of Implantable Middle Ear Devices
Implantable hearing devices are broadly classified into two types based on their mechanism of action:
1. Piezoelectric Devices: These devices utilize a piezoceramic crystal that changes shape when an electric current is applied, generating vibrations. The crystal is coupled to the ossicles, directly driving the ossicular chain by vibrations. Examples include the Envoy, Middle-Ear Transducer (MET), Rion, and Totally Integrated Cochlear Amplifier (TICA).
2. Electromagnetic Devices: These devices function by passing an electric current through a coil, creating a magnetic field that drives an adjacent small magnet attached to one of the ossicles. This magnet transmits vibrations to the cochlea. A well-known example is the Vibrant Sound bridge, manufactured by MED-EL.
The Vibrant Sound Bridge Device.
The Vibrant Sound bridge is a semi-implantable system consisting of two main components:
- Internal Component (VORP): This includes a receiver, a Floating Mass Transducer (FMT), and a conductor link between the receiver and FMT. The FMT is surgically attached to the incus, enabling direct vibration of the ossicular chain.
- External Component (Audio Processor): Worn behind the ear, this component captures sound via a microphone and transmits it as radiofrequency signals to the internal component receiver.
Candidacy for Implantable Hearing Aids
Ideal candidates are adults aged 18 and older with moderate-to-severe sensorineural hearing loss having dissatisfaction with traditional hearing aids due to issues such as:
- Poor sound quality.
- Discomfort from the occlusion effect.
- Frequent wax build-up in the ear canal or hearing aid mould.
- Sensitivity of the ear canal skin.
- Persistent acoustic feedback.
Surgical Procedure
The implantation of the internal device is performed under general anaesthesia. The receiver is placed under the skin over the mastoid bone using a cortical mastoidectomy and posterior tympanotomy approach. The FMT is attached to the long process of the incus without modifying the middle ear structures, preserving the patient’s residual hearing. After 6–8 weeks, the external audio processor is fitted and programmed.
Advantages of Direct Drive Systems
Direct drive hearing devices offer several benefits over conventional hearing aids:
- Improved Sound Quality: By delivering mechanical energy directly to the ossicles, these devices provide clearer sound, especially in noisy environments.
- Elimination of Common Issues: Problems such as occlusion, feedback, discomfort, and wax build-up are avoided, as the ear canal remains open.
- Enhanced Comfort: The absence of ear canal obstruction makes these devices more comfortable for long-term use.
Cochlear Implants
Cochlear implants are advanced electronic devices designed to provide hearing for children and adults with severe to profound sensorineural hearing loss. The cochlear implant provides direct electrical stimulation to the auditory nerve, bypassing the damaged parts of the inner ear and degenerated hair cells in the cochlea, which are damaged to such a point that amplification provided by hearing aids is no longer effective. The auditory nerve then carries the signals to the auditory cortex in the brain for hearing perception.

Components and Mechanism of a Cochlear Implant
A cochlear implant consists of two main components: an external unit and an internal unit.
1. External Component: It consists of
- Speech Processor: This can be worn behind the ear or on the body, with the behind-the-ear type being more common. It captures sound through a microphone, processes it, converts it into digitally coded signals, and sends them to the transmitter coil. The speech processor converts sound into electrical pulses using a variety of advanced coding strategies, such as the Simultaneous Analogue Strategy (SAS), Continuous Interleaved Sampling (CIS), Spectral Peak (SPEAK), and Advanced Combination Encoder (ACE).
- Transmitter coil: The external transmitter sends digitally coded signals to the receiver-stimulator package via radiofrequency waves.

2. Internal Component:
- Receiver-Stimulator package: It consists of a magnet, which holds the external transmitter in place, and an electronic system that decodes signals received from the external transmitter, converts them into electrical impulses, and transmits them to the electrode array using a coding strategy.
- Intracochlear electrode Array: It is a thin, flexible wire inserted into the scala tympani of the basal turn of the cochlea (the entire length of the cochlear duct). This array contains multiple electrodes that deliver electrical impulses to the spiral ganglion cells in the cochlea. These cells are bipolar neurons that connect the cochlea to the auditory nerve. When the electrodes stimulate the spiral ganglion cells, the auditory nerve carries these signals to the auditory cortex in the brain, where they are interpreted as sound. Speech perception with a cochlear implant depends on the spectral resolution provided by the electrode array, the number of surviving spiral ganglion cells, and central auditory processing — not on any specific minimum number of nerve fibres. This ensures that the brain receives sufficient information to get good speech perception and distinguish speech sounds, especially in noisy environments.

Candidacy for Cochlear Implants
Cochlear implants are suitable for both children and adults who meet specific criteria:
- Severe to Profound Sensorineural Hearing Loss.
- Fracture of the cochlea following temporal bone fracture.
- Auditory neuropathy or dyssynchrony (ANDS) patients.
- Inability to achieve functional hearing with conventional devices.
- No medical contraindications for fitness for surgery and general anaesthesia.
- Realistic Expectations: Understanding the potential outcomes and limitations.
- Strong family and social support for post-implantation rehabilitation.
- Adequate Cognitive Function: Ability to use and adapt to the device.
Candidates are categorised as prelingual (deafened before acquiring speech) or postlingual (deafened after acquiring speech). Early intervention is critical for prelingual children, as auditory deprivation during early development can lead to degeneration of central auditory pathways, limiting the benefits of implantation.
Outcomes of Cochlear Implantation
The success of cochlear implantation depends on several factors:
1. Prior Auditory Experience: Postlingual patients or those with prior hearing aid use tend to achieve better outcomes.
2. Age at Implantation: Younger children, especially those implanted before 12 months, show improved speech and language development.
3. Duration of Deafness: Shorter periods of deafness correlate with better outcomes.
4. Neural Plasticity: Early diagnosis and rehabilitation (ideally before age 3) are critical for prelingually deaf children due to neural plasticity. Neural plasticity is the brain’s ability to adapt to new auditory stimuli. Without early stimulation, the brain’s auditory areas may be repurposed for other functions, limiting the potential for speech and language development.
- Postlingual patients often achieve significant benefits, including the ability to understand speech without visual cues and use the telephone.
- Prelingual children who receive early intervention also develop speech and language skills over time, though this requires consistent auditory-verbal therapy.
- Prelingual adults with no prior auditory experience may gain only sound awareness, with limited open-set speech understanding.
Evaluation for Cochlear Implantation
A thorough evaluation is essential to determine candidacy and set realistic expectations. The evaluation process includes:
1. Medical Evaluation:
- Detailed history and physical examination to assess fitness for surgery.
- Preoperative tests and vaccinations, particularly against meningitis-causing organisms: pneumococcus (PCV13/15/20), Haemophilus influenzae type b, and meningococcus (MenACWY and MenB).
- Check for any ear infections. Pt should be free from all ear infections. Myringoplasty or mastoid exploration, if required, should be performed at least 3 months before the cochlear implant surgery.
2. Imaging Studies:
- HRCT of Temporal Bone: Identifies inner ear abnormalities, cochlear lumen obliteration, middle ear pathology, and anatomical variations (e.g., low-lying dura, anterior sigmoid sinus). It detects conditions like cochlear hypoplasia, enlarged vestibular aqueduct, and labyrinthitis ossificans, which can impact surgical planning and candidacy for cochlear implants (CI).
- MRI: Diagnoses cochlear nerve aplasia, a contraindication for CI, necessitating an Auditory Brainstem Implant (ABI) instead.
3. Audiological Evaluation:
- Pure tone audiometry, speech discrimination tests, tympanometry, otoacoustic emissions (OAE), auditory brainstem responses (ABR), and auditory steady-state responses (ASSR).
- A mandatory hearing aid trial to assess the extent of benefit from conventional devices.
4. Speech and Language Evaluation: Assesses the patient’s current communication abilities and identifies any developmental delays or disorders.
5. Psychological Evaluation: Evaluates cognitive function and identifies any additional disabilities, helping to set realistic expectations for post-implantation outcomes.
Surgical Steps of Cochlear Implant Surgery
Cochlear implant surgery is performed under general anaesthesia and involves the following steps:
1. Patient Positioning: The surgery is performed under general anaesthesia, with the patient in a supine position and the head turned 45-60 degrees from the surgeon.
2. Incision: A C-shaped postauricular incision is made.
3. Flap Elevation and Mastoidectomy: The skin flap , subcutaneous tissue, and part of the temporalis muscle (palva flap) are elevated. A cortical mastoidectomy is performed, preserving overhanging edges. 

4. Formation of the well. A subperiosteal pocket is made in the posterior and superior to the mastoidectomy cavity. A bony well is created for the receiver-stimulator placement.
5. Posterior Tympanotomy: The middle ear is accessed via the facial recess, and the round window niche is visualized.


6. Cochleostomy: A cochleostomy is created anteroinferior to the round window membrane using a small diamond burr. The opening is gently enlarged, and the electrode array is inserted into the scala tympani. Many surgeons now prefer round window insertion whenever feasible because it minimises intracochlear trauma and preserves residual hearing.
7. Receiver-Stimulator Placement: The receiver-stimulator is placed tightly in the subperiosteal pocket and the electrode array is passed through the bony well, which is secured with non-absorbable sutures.

8. Electrode Insertion: The electrode array is inserted into the cochlea, either through the cochleostomy or the round window (the latter is preferred for reduced trauma and postoperative complications).
9. Cochleostomy sealing. Temporalis muscle pieces or fat are used to seal the cochleostomy site. Electrophysiological testing is done to confirm proper functioning.
10. Verification and Closure: Neural response telemetry checks electrode functionality. The incision is closed in layers, and a postoperative X-ray (Stenver’s view) is done to confirm the electrode position.
Postoperative Mapping and Rehabilitation
- Device Activation: The implant is activated 3–4 weeks post-surgery.
- Mapping (Programming): The speech processor is programmed to optimize sound perception. Regular adjustments are made during follow-up visits.
- Habilitation: Auditory-verbal therapy is essential for all patients, particularly prelingual children. This therapy focuses on developing listening and speaking skills without relying on visual cues. Consistent effort from the patient, family, and therapists is crucial for successful adaptation.
Cochlear implants have transformed the lives of individuals with severe to profound hearing loss, offering them the opportunity to experience sound and develop communication skills. With careful patient selection, precise surgical techniques, and dedicated postoperative rehabilitation, cochlear implants can provide life-changing benefits, particularly for children who receive early intervention. This technology continues to evolve, promising even greater outcomes for future recipients.
Auditory Brainstem Implant (ABI)
The Auditory Brainstem Implant (ABI) is a groundbreaking device designed to provide auditory stimulation for individuals who cannot benefit from cochlear implants due to the absence or dysfunction of the auditory nerve (CN VIII). Unlike cochlear implants, which stimulate the auditory nerve, the ABI directly targets the cochlear nuclear complex in the brainstem. This makes it a vital option for patients with specific conditions, such as bilateral vestibular schwannomas in neurofibromatosis type 2 (NF2), where the auditory nerve is damaged or severed.
Indications for ABI
The primary indication for an ABI is bilateral damage to the auditory nerve, typically resulting from the surgical removal of vestibular schwannomas (acoustic neuromas). In cases of unilateral acoustic neuroma, an ABI is unnecessary because hearing can still be preserved or restored through the contralateral ear. However, in bilateral cases, such as those seen in NF2, the ABI becomes a critical tool for auditory rehabilitation.
How the ABI Works
The ABI is conceptually similar to a multichannel cochlear implant but differs in its placement and target. Key components include:
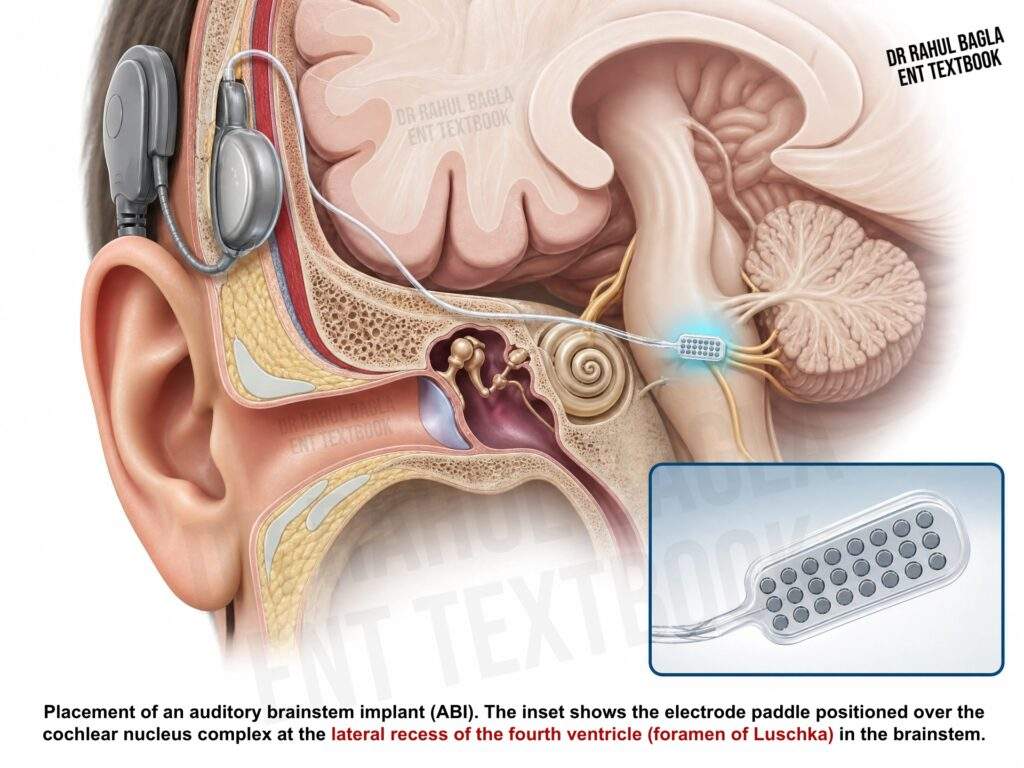
- Multielectrode Array: Attached to a Dacron mesh, which is positioned on the surface of the brainstem within the lateral recess of the fourth ventricle (at the foramen of Luschka).
- Receiver/Stimulator: Contains a removable magnet, allowing patients to safely undergo MRI scans if needed.
The ABI bypasses the cochlea and auditory nerve entirely, delivering electrical stimulation directly to the cochlear nucleus in the brainstem. This enables the brain to perceive sound, albeit with less clarity and precision compared to cochlear implants.
Benefits and Limitations
ABIs provide several functional benefits, including:
- Improved Communication: Enhanced ability to understand speech, especially when combined with lip-reading.
- Environmental Sound Awareness: Better recognition of everyday sounds, such as alarms, doorbells, and approaching vehicles.
- Safety and Orientation: Increased awareness of surroundings, contributing to improved quality of life.
However, ABIs are not as effective as multichannel cochlear implants. The sound perception they provide is often less refined, and users may not achieve the same level of speech recognition. Despite these limitations, ABIs represent a significant advancement for individuals who have no other options for hearing restoration.
Surgical Procedure
The ABI is surgically implanted during the removal of a vestibular schwannoma. The procedure involves:
- Accessing the Brainstem: The lateral recess of the fourth ventricle is exposed.
- Placing the Electrode Array: The Dacron mesh with the multielectrode array is carefully positioned on the cochlear nucleus.
- Securing the Receiver/Stimulator: The internal device is placed under the skin, and the electrode array is connected.
Postoperative imaging and electrophysiological testing are performed to ensure proper placement and functionality.
Technological Developments
ABIs are still relatively rare, with a limited number of procedures performed worldwide. Ongoing research and technological advancements aim to improve their effectiveness, particularly in enhancing speech perception and sound quality. Innovations in electrode design, signal processing, and surgical techniques are expected to expand the potential of ABIs in the future. The Auditory Brainstem Implant (ABI) is a specialized solution for individuals with bilateral auditory nerve damage, particularly those with NF2. While it does not match the performance of cochlear implants, it offers meaningful auditory benefits, including improved communication and environmental sound awareness. As technology continues to evolve, ABIs hold promise for further enhancing the quality of life for patients with profound hearing loss due to brainstem-level auditory pathway damage.
Assistive Devices
Vibrotactile Hearing Aids
Vibrotactile hearing aids convert sound into tactile vibrations that are perceived through the skin. They are reserved for patients with profound hearing loss who derive little or no benefit from conventional hearing aids and are either unsuitable for or unwilling to undergo cochlear implantation. Although largely replaced by cochlear implants, vibrotactile devices may still have a limited role in selected patients with combined deafness and blindness (deaf-blind individuals), where tactile cues can supplement environmental awareness.
———— End of the chapter ————
High-Yield Points for Quick Revision
- CBME Focus: Rehabilitation is a team effort involving the ENT surgeon, Audiologist, Speech Pathologist, and Educator.
- Best Outcome CI: Postlingual adults and prelingual children implanted before 12 months of age.
- Imaging for CI: HRCT (Labyrinthitis Ossificans, Bony Anatomy), MRI (Auditory Nerve Integrity).
- CI Contraindication: Auditory Nerve Aplasia (requires ABI).
- BAHA Indication: Conductive/Mixed loss (e.g., atresia, chronic discharge) and Single-Sided Deafness (SSD).
- ABI Indication: Bilateral CN VIII damage (e.g., NF2 post-surgery).
- CROS: Used for unilateral severe loss with a normal contralateral ear.
- CI Surgery Key Step: Electrode array is inserted into the scala tympani.
- CROS: Used for unilateral severe loss with a normal contralateral ear; non-surgical alternative to BAHA in SSD.
Frequently Asked Questions in Viva
- What is the best age for a Cochlear Implant in a child? The optimal age for cochlear implantation in a prelingual child is before 12 months of age. Implantation before 3 years of age is still associated with good outcomes, and outcomes decline progressively when implantation is performed after 5 years due to reduced neural plasticity.
- What is the difference between a Hearing Aid and a Cochlear Implant? A Hearing Aid amplifies acoustic sound waves delivered through the ear canal to stimulate residual hair cells, whereas a Cochlear Implant bypasses damaged hair cells to directly stimulate the auditory nerve with electrical impulses.
- Which imaging test is mandatory before Cochlear Implant surgery, and why? An MRI of the internal auditory canals is mandatory to confirm the presence and integrity of the auditory nerve (CN VIII), since its absence is a contraindication to a Cochlear Implant.
- What is the CROS hearing aid CROS (Contralateral Routing of Signals) hearing aid transmits sound from a microphone on the deaf ear to a receiver on the better-hearing ear, which is primarily used for unilateral severe hearing loss.
- What is the main indication for an Auditory Brainstem Implant (ABI)? The main indication for an ABI is the bilateral absence or non-functionality of the auditory nerve, commonly seen after the removal of bilateral vestibular schwannomas in Neurofibromatosis Type 2 (NF2).
- What is the main side effect of an improperly fitted conventional hearing aid? The main side effect is acoustic feedback, which is a high-pitched whistling sound caused by sound leaking out of the ear mould and being re-amplified by the microphone.
Clinical Case Scenarios (Practical/Viva)
Case 1: The Deaf Child
A 3-year-old male child is diagnosed with profound bilateral sensorineural hearing loss after failing to respond to speech. He has received no benefit from a 6-month trial of high-power hearing aids. Imaging shows a normal cochlear nerve bilaterally.
1. Diagnosis: Prelingual profound bilateral SNHL.
2. Management Plan (VIVA Presentation):
- First Step: Confirm candidacy for a Cochlear Implant (CI), ensuring all criteria (including imaging and HA trial failure) are met.
- Second Step: Perform Bilateral Cochlear Implantation (preferred for better localisation and hearing in noise).
- Third Step: Post-operatively, mandatory, rigorous Auditory-Verbal Therapy (AVT) for habilitation and speech/language development.
Case 2: The Draining Ear
A 45-year-old patient presents with a 10-year history of chronic suppurative otitis media (CSOM) with a persistent, actively draining right ear and a maximal conductive hearing loss. He wants hearing restoration but is not fit for mastoid surgery due to comorbidities. The left ear is normal.
1. Diagnosis: Unilateral severe Conductive Hearing Loss due to active CSOM.
2. Management Plan (Examiner Question: Why not a regular HA?):
- A conventional air-conduction HA is contraindicated due to the active discharge, as the ear mould and moisture will worsen the infection.
- The ideal solution is a Bone-Anchored Hearing Aid (BAHA). The BAHA bypasses the middle ear and ear canal, transmitting sound via bone conduction to the cochlea, which is perfect for an actively draining ear.
Case 3: The NF2 Patient
A 28-year-old patient with Neurofibromatosis Type 2 (NF2) is undergoing surgical removal of a large, bilateral Vestibular Schwannoma, which will inevitably sever both Auditory Nerves.
1. Diagnosis: Hearing loss due to bilateral auditory nerve damage.
2. Management Plan (Examiner Question: CI vs ABI?):
- A Cochlear Implant (CI) is contraindicated because the auditory nerve (CN VIII) will be damaged/removed and cannot transmit signals.
- The patient is a candidate for an Auditory Brainstem Implant (ABI). The ABI electrode array must be placed directly onto the cochlear nuclear complex in the brainstem during the tumor removal surgery to provide sound awareness and assist with lip-reading.
NEET PG/University Exam Multiple Choice Questions (MCQs)
-
The primary mechanism by which a Bone-Anchored Hearing Aid (BAHA) provides sound perception is: A. Direct mechanical stimulation of the incus. B. Amplification of sound waves through the ear canal. C. Direct electrical stimulation of the auditory nerve. D. Transmitting sound vibrations through the skull bone to the cochlea.
-
Which of the following is an absolute contraindication for a Cochlear Implant? A. Labyrinthitis ossificans. B. Profound Sensorineural Hearing Loss. C. Bilateral Auditory Nerve Aplasia. D. Age of 60 years.
-
The main purpose of the mandatory pre-operative MRI in a Cochlear Implant candidate is to: A. Rule out middle ear fluid. B. Assess the integrity of the Auditory Nerve (CN VIII). C. Detect a low-lying dura. D. Identify cochlear lumen obliteration.
-
The most common site for electrode array insertion in Cochlear Implant surgery is the: A. Scala vestibuli. B. Scala media. C. Scala tympani. D. Basilar membrane.
-
Which hearing device is ideally suited for a patient with Single-Sided Deafness (SSD) and a normal contralateral ear? A. Auditory Brainstem Implant (ABI). B. Conventional In-the-Ear (ITE) Hearing Aid. C. CROS Hearing Aid or BAHA. D. Implantable Middle Ear Hearing Aid.
-
The Floating Mass Transducer (FMT) is a key component of which implantable device? A. Cochlear Implant. B. Bone-Anchored Hearing Aid. C. Auditory Brainstem Implant. D. Vibrant Soundbridge (Implantable HA).
-
The whistling sound produced by a conventional hearing aid, often caused by a loose earmould, is termed: A. Spectral Distortion. B. Recruitment. C. Acoustic Feedback. D. Occlusion Effect.
-
Early diagnosis and implantation in prelingually deaf children offer better speech outcomes due to: A. Superior electrode technology. B. Longer life of the battery. C. Neural plasticity of the central auditory pathways. D. Increased patient dexterity.
-
Auditory-Verbal Therapy (AVT) is an essential post-implantation rehabilitation program that focuses on: A. Mastering sign language. B. Developing listening and speaking skills without visual cues. C. Interpreting purely visual cues (lip reading). D. Improving balance and spatial orientation.
-
The surgical approach used to access the round window niche for Cochlear Implantation is the: A. Translabyrinthine approach. B. Transcochlear approach. C. Posterior Tympanotomy (Facial Recess). D. Endoscopic Middle Ear Surgery.
MCQ Answers and Explanations
- D. Transmitting sound vibrations through the skull bone to the cochlea. BAHA is a bone conduction device that bypasses the conductive pathway (external and middle ear).
- C. Bilateral Auditory Nerve Aplasia. Without an auditory nerve, electrical impulses cannot reach the brain, making a CI ineffective and an ABI necessary. Labyrinthitis ossificans (A) is a relative contraindication (makes insertion difficult).
- B. Assess the integrity of the Auditory Nerve (CN VIII). This is a critical step to ensure the nerve is present and intact enough to receive electrical stimulation.
- C. Scala tympani. The electrode array is inserted into the scala tympani, allowing the electrodes to sit near the spiral ganglion cells in the osseous spiral lamina.
- C. CROS Hearing Aid or BAHA. Both are indicated for SSD. BAHA is often preferred for superior performance in noise and aesthetics.
- D. Vibrant Soundbridge (Implantable HA). The FMT is the magnet surgically coupled to an ossicle (usually the incus) to vibrate it directly.
- C. Acoustic Feedback. The classic “whistling” caused by amplified sound leaking out of the ear and being picked up again by the microphone.
- C. Neural plasticity of the central auditory pathways. The young brain’s ability to adapt and rewire itself for new auditory input is highest in early childhood.
- B. Developing listening and speaking skills without visual cues. AVT’s core principle is maximizing the auditory channel for communication, distinguishing it from lip-reading.
- C. Posterior Tympanotomy (Facial Recess). This is the standard, conservative surgical corridor to access the middle ear space and the round window niche without damaging the facial nerve.
———— End ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Gordon B. Hughes, Myles L. Pensak, H. B. Broidy. Textbook of Clinical Otology.
- Mario Sanna. Textbook of Colour Atlas of Endo-Otoscopy Examination–Diagnosis–Treatment.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Master the essential devices, surgical principles, and rehabilitation programs for the hearing impaired. This comprehensive guide covers Hearing Aids, CROS, BAHA, Cochlear Implants, and ABI for MBBS, ENT PG, and NEET PG exam success, Rehabilitation of the hearing impaired notes, cochlear implant surgery steps NEET PG, indications for BAHA vs CROS, Auditory Brainstem Implant ABI mechanism, conventional hearing aids types and components, CBME aural rehabilitation summary, high yield ENT MCQs on hearing aids, viva questions on cochlear implant candidacy, surgical approach to cochlear implantation, best ENT book chapter on hearing rehabilitation, Hearing aids, Cochlear implants, Auditory brainstem implants, Bone-anchored hearing aids, Speech reading, Auditory training, Hearing loss solutions, Assistive listening devices, Hearing rehabilitation, Implantable hearing devices/p>