|
The following CBME core competencies are covered in this chapter.
|
Introduction to Audiometry & Objective Tests for Hearing Assessment
Building upon the foundational clinical and tuning fork tests, advanced audiometric and objective assessments provide precise, quantitative data crucial for comprehensive hearing diagnostics. These sophisticated tools enable clinicians to pinpoint the type, degree, and specific site of auditory lesions, guide rehabilitative strategies, and monitor treatment outcomes. This chapter delves into the intricacies of these advanced tests, essential for MBBS and ENT PG students to achieve strong conceptual clarity and excel in their examinations.
- Subjective Audiometry Tests (Most Commonly Used) – Pure Tone Audiometry (PTA), Speech Audiometry, Bekesy Audiometry. They are the standard methods for assessing a person’s hearing and communication abilities.
- Objective Tests for Middle Ear Function and Reflexes – Impedance Audiometry (Tympanometry, Acoustic (Stapedial) Reflex, Eustachian Tube Function Tests). They check how well the middle ear transfers sound energy and if the reflex pathways are working normally.
- Objective Tests for Inner Ear Hair Cell Function – Otoacoustic Emissions (OAE). OAE tests measure the tiny sounds (echoes) produced by outer hair cells in a healthy cochlea.
- Objective Assessment of the Neural Pathway (Auditory Evoked Potentials) – Electrocochleography (ECoG), Auditory Brainstem Response (ABR/BERA), Auditory Steady State Response (ASSR). These tests record the electrical responses of the hearing nerve and brainstem after a sound is played. They are non-invasive and give detailed information about where the problem lies — from the cochlea up to the brainstem.
- Special Diagnostic Tests – Whether the hearing loss is cochlear (inner ear) or retrocochlear (eighth nerve or brainstem) – Recruitment, Short Increment Sensitivity Index (SISI), Tone Decay Test. These tests help to differentiate the type and site of hearing loss.
- Central Auditory Tests – Dichotic Listening Tests, Distorted Speech Tests. These assess how well the brain processes sounds when both ears are stimulated.
1. Subjective Audiometry Tests
1.1 Pure Tone Audiometry (PTA)
PTA is a subjective test designed to determine the hearing threshold for pure tones, which are sinusoidal waves characterised by a single frequency, amplitude, and phase. Pure Tone Audiometry (PTA) is considered the gold standard for measuring hearing thresholds.
- Instrument: An audiometer generates pure tones and allows the examiner to adjust their intensity and frequency.
- Audiogram: The results are plotted on a graph called an audiogram, which provides a visual representation of hearing ability.
Components of an Audiometer. An audiometer is composed of several key parts:
- Electronic Oscillator: Generates pure tones of different frequencies.
- Intensity Dial: Adjusts the loudness of the tones in 5 dB steps.
- Headphones: For Air Conduction (AC) testing, assessing the entire auditory pathway.
- Bone Conductor: A vibrator placed on the mastoid for Bone Conduction (BC) testing, bypassing the middle ear to test the cochlea directly.
Prerequisites for PTA. For accurate results, PTA should be conducted under specific conditions:
- Sound-Proof Environment: The test should take place in a sound-proof room, with ambient noise levels accepted at less than 35 dB.
- Minimising Distractions: Transient noises, such as sneezing or coughing, should be avoided, as they can interfere with the test results.
- Examiner-Patient Interaction: The patient sits in a soundproof booth while the examiner conducts the audiometry from outside. Communication can occur via intercom or face-to-face to observe the patient’s reactions.
Procedure of PTA. The testing process follows a standardised sequence to ensure reliability. The testing process typically begins with the better ear.
- Air Conduction (AC) Testing: The thresholds for pure tones are measured in the following order: 1000 Hz, 2000 Hz, 4000 Hz, and 8000 Hz, followed by 500 Hz and 250 Hz. If there is a difference of 20 dB or more between contiguous frequencies, inter-octave frequencies (750 Hz, 1500 Hz, 3000 Hz, and 6000 Hz) will also be tested. The procedure is then repeated for the other ear.
- Bone Conduction (BC) Testing: After completing AC testing for both ears, conduct bone conduction testing if an air-bone gap (ABG) is suspected or to confirm sensorineural thresholds. BC thresholds are typically measured at 500 Hz, 1000 Hz, 2000 Hz, and 4000 Hz. There’s usually no need to retest 1000 Hz for BC if it was the initial AC frequency.
Bracketing Technique (Modified Hughson-Westlake Method)
The bracketing technique, also known as the 10 dB down, 5 dB up method, involves delivering each test signal at an audible level (e.g., 30 dB HL), then reducing the volume in 10 dB steps until the signal becomes inaudible. The volume is then increased in 5 dB increments until the patient can perceive the sound again. Repeat this down-10, up-5 sequence to find the hearing threshold.
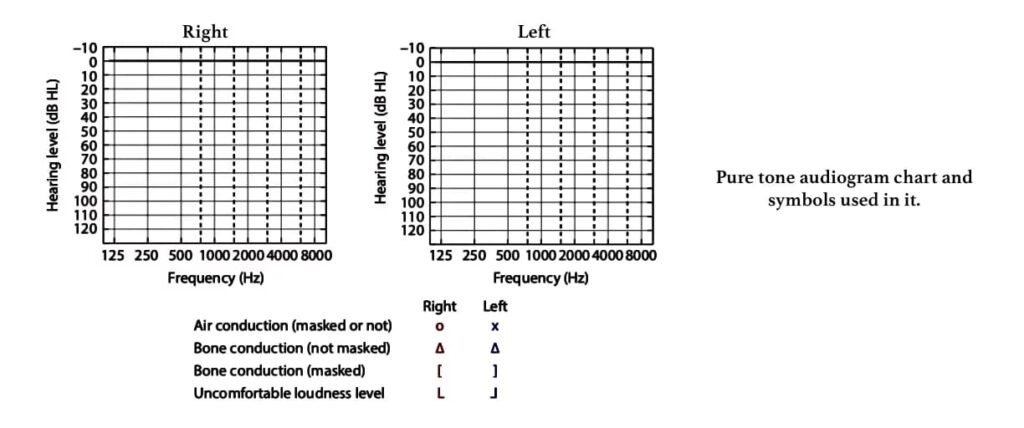
Pure Tone Audiogram is a graphical representation of hearing detection thresholds in each ear across different frequencies.
- X-axis: Represents frequency (Hz), typically ranging from 125 Hz to 8000 Hz.
- Y-axis: Represents hearing level (dB HL), with lower (negative) dB values indicating better hearing and higher dB values indicating poorer hearing.
- Symbols: Standardized symbols denote air conduction (AC) and bone conduction (BC) for each ear (e.g., Red ‘O’ for Right AC, Blue ‘X’ for Left AC; Red ‘<‘ for Right BC unmasked, Blue ‘>’ for Left BC unmasked; Red ‘[‘ for Right BC masked, Blue ‘]’ for Left BC masked).
Masking is the process of introducing a noise (a masker) to the non-test ear to prevent it from hearing the sound intended for the test ear. This is important, especially when there’s a significant difference in hearing between the two ears.
- Principle: When a sound is presented to one ear, it can cross over (transcranially) to the opposite cochlea if it’s loud enough. This phenomenon is called cross-hearing or transcranial transmission. The amount of sound energy lost as it travels from one ear to the other is called interaural attenuation (IA).
- When to Mask for AC? When the interaural hearing difference (AB gap) in AC thresholds between the two ears exceeds 40 dB (with headphones) or 55 dB (with insert phones). This is done to avoid transcranial transmission/ interaural attenuation/ cross-hearing and accurately measure hearing in each ear.
- When to Mask for BC? Always. Bone-conducted sound vibrates the entire skull, stimulating both cochleae simultaneously.
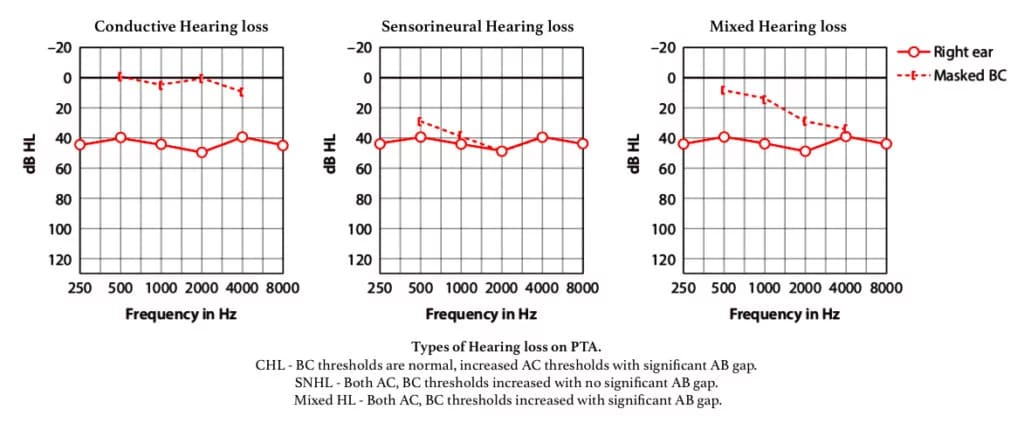
Interpretation of PTA Results
|
Type of Hearing Loss |
Air Conduction (AC) |
Bone Conduction (BC) |
Air-Bone Gap (ABG) |
|
Normal |
≤ 20 dB HL |
≤ 20 dB HL |
No |
|
Conductive |
> 20 dB HL |
Normal (≤ 20 dB HL) |
Yes (> 10 dB) |
|
Sensorineural |
> 20 dB HL |
> 20 dB HL (Same as AC) |
No (≤ 10 dB) |
|
Mixed |
> 20 dB HL |
> 20 dB HL (But worse than normal) |
Yes (> 10 dB) |
Utilisation of PTA. PTA serves multiple purposes in audiology:
- Determining Hearing Loss: It helps identify the type, degree, and configuration (shape of the audiogram, e.g., sloping, flat) of hearing loss. The air conduction pure tone audiogram primarily measures the degree of hearing loss, while the bone conduction audiogram differentiates between conductive and sensorineural hearing loss.
- Medicolegal Assessment: PTA can confirm the degree of hearing impairment for legal and insurance purposes.
- Hearing Aid Prescription: The audiogram is crucial for accurately prescribing hearing aids.
- Speech Reception Threshold: PTA also assists in determining the speech reception threshold of the subject.
Disadvantages of PTA. It is subjective, prone to malingering, and unreliable in very young children, under the age of seven, as it depends on cognitive development and cooperation.
1.2 Speech audiometry.
Speech audiometry is an essential tool for evaluating a patient’s hearing ability and understanding of spoken words. It provides critical functional information beyond pure tones. The results of this test are plotted on a graph. The test is also useful for detecting retrocochlear pathology and non-organic hearing loss.
- Speech Reception Threshold (SRT): SRT is the lowest speech intensity at which a patient can correctly repeat 50% of spondee words. It is important to distinguish SRT from the Speech Awareness Threshold (SAT), which is a separate measure where the patient simply indicates awareness of speech (detection) without needing to repeat words. SAT is typically 5–10 dB better than SRT and is not the same as SRT.
- Procedure: The test involves delivering recorded tapes or monitored voice of spondee words (two-syllable words with equal stress on each syllable, such as “pancake,” “hardware,” “playground”) through headphones or speakers in a soundproof room. The intensity of these words is varied in 5 dB steps until the patient correctly identifies half of them.
- Interpretation and Reliability: For a normal adult, the SRT should be within 10 dB of the pure tone average (500, 1000, and 2000 Hz). An SRT that is better than the pure tone average by more than 10 dB suggests functional hearing loss or an unreliable pure tone audiogram.
- Speech Discrimination Score (SDS):
- Also known as the speech recognition or word recognition score, SDS measures the patient’s ability to understand speech clearly.
- A list of 25 to 50 phonetically balanced words (single-syllable words such as “pin,” “sin,” “day,” “bus”) is presented to each ear separately at 30–40 dB above the patient’s SRT using pre-recorded material.
- The percentage of words correctly identified by the patient is recorded.
- In normal hearing and conductive hearing loss, a high score of 90–100% is typical.
Table : Ability to understand speech and its relation to speech discrimination (SD) score. A list of 50 PB words is presented. The number of words correctly heard is multiplied by 2 to obtain the percentage score.
| SD score | Ability to understand speech |
| 90–100% | Normal (Excellent) |
| 76–88% | Slight difficulty (Good) |
| 60–74% | Moderate difficulty (Fair) |
| 40–58% | Poor |
| <40% | Very poor |
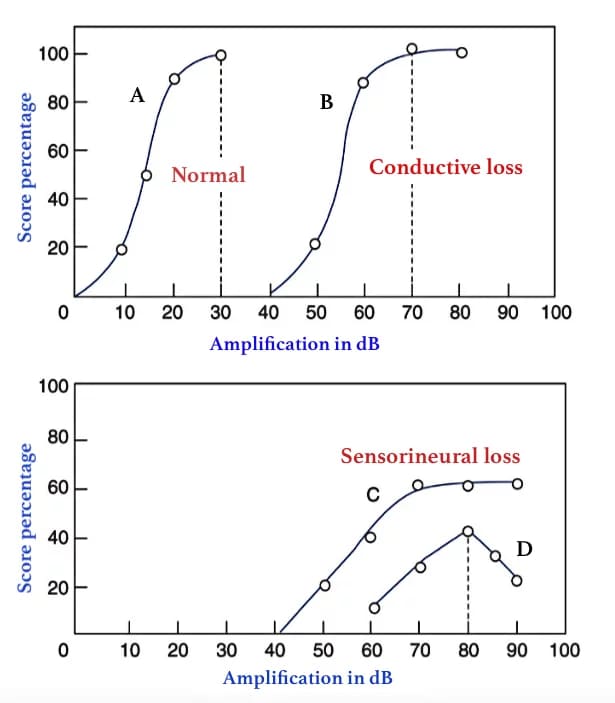
Interpretation of Speech Discrimination Scores
- Conductive Hearing Loss: Patients typically show improved recognition scores when the speech signal intensity is increased.
- Sensorineural Hearing Loss: Patients usually do not show improved recognition scores with increased intensity because louder sounds can distort the speech signal.
- Retrocochlear Pathology: Patients may exhibit a reduction in recognition scores with increased intensity, known as the “rollover” effect, which suggests a lesion in the eighth cranial nerve. In this scenario, as speech intensity increases beyond a certain level, the word recognition score declines rather than stabilising as it does in cochlear sensorineural hearing loss.
Performance Intensity Function for PB Words
- PB Max: It is beneficial to plot PB scores against various speech intensity levels to determine the maximum score (PB max) a person can achieve, rather than using a single suprathreshold intensity of 30–40 dB above the SRT. The intensity at which PB max is achieved is noted, and the maximum volume of a hearing aid should be set below this level.
Benefits of speech audiometry :
- To measure the speech reception threshold which determines actual disability & not hearing impairment.
- To differentiate organic from nonorganic(functional) hearing loss.
- To find the intensity at which a hearing aid/cochlear implants fits and assessing rehabilitation outcome.
- To differentiate a cochlear from a retrocochlear sensorineural hearing loss.
1.3 Bekesy audiometry.
It is an older, self-recording audiometric technique based on sweep and fixed frequency testing. In this method, various pure tone frequencies automatically shift from low to high, while the patient controls the intensity using a button. Two tracings are obtained: one with a continuous tone and the other with a pulsed tone. These tracings help differentiate between cochlear and retrocochlear hearing loss as well as between organic and functional hearing loss. However, Bekesy audiometry is seldom performed in contemporary practice.
The types of tracings obtained in Bekesy audiometry include:
- Type I: Continuous and pulsed tracings overlap, indicating normal hearing or conductive hearing loss.
- Type II: Continuous and pulsed tracings overlap up to 1000 Hz, after which the continuous tracing falls. This pattern is seen in cochlear loss.
- Type III: The continuous tracing falls below the pulsed tracing at 100–500 Hz, sometimes up to 40–50 dB. This pattern is indicative of a retrocochlear or neural lesion.
- Type IV: The continuous tracing falls below the pulsed tracing at frequencies up to 1000 Hz by more than 25 dB. This pattern is also seen in retrocochlear or neural lesions.
- Type V: The continuous tracing is above the pulsed tracing, which is characteristic of nonorganic hearing loss.
2. Objective Tests for Middle Ear Function and Reflexes – Impedance audiometry.
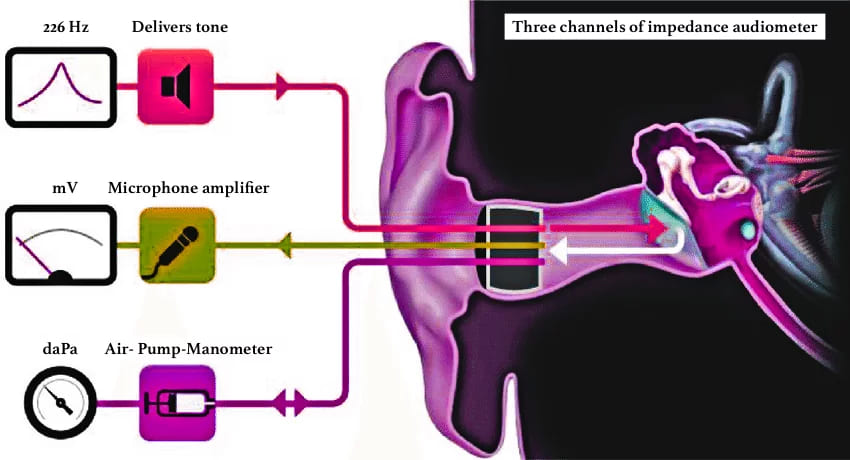
It is an objective test used to assess middle ear function and mobility of the tympanic membrane. The word ‘impedance’ means resistance to the flow of acoustic energy, expressed in ohms and compliance is expressed in cubic centimetre of air. It provides valuable otological and neurological information about the nature and site of a lesion. The middle ear functions as the ‘impedance matching device’. Any pathology in the middle ear may cause impedance mismatching and vary the amount of sound reflected back from the tympanic membrane leading to conductive deafness. Impedance audiometry measures the efficiency of the middle ear to perform this function.

Impedance audiometer consists of a handheld probe which is hermetically sealed into the external auditory meatus forming a leak-free seal from the probe tip to the eardrum and has three channels: (i) first channel delivers a tone of 220 or 226 Hz, (ii) the second channel allows the reflected sound from the tympanic membrane to pass through a microphone amplifier assembly for processing (iii) the third channel is attached to air- pump-manometer system to bring about changes in air pressure in the ear canal from positive to normal and then negative(+300 to -600 mm of water pressure).
- Tympanometry
- Eustachian tube function test
- Acoustic/ stapedial reflex measurements
2.1 Tympanometry.
It is the measurement of the change of impedance in the middle ear due to varying air pressure in the sealed external auditory meatus. A non-compliant/ stiff tympanic membrane tends to reflect back more sound energy as compared to a compliant TM. This reflected sound pressure is measured at the tip of the probe and charted in the graphical form of with impedance of the middle ear/compliance of TM on Y-axis and the air pressure on X-axis, called the tympanogram.
| Impedance is the opposition/ resistance to the flow of energy, admittance is the ease of movement with which the flow of energy occurs. For ease of measurement most clinical impedance audiometers measure the acoustic admittance. Admittance is reciprocal of impedance just like compliance is the reciprocal of stiffness. |
Procedure:
- Otoscopy is done to exclude scarring or perforation in the tympanic membrane
- Remove wax /discharge, if present and choose a well-fitted ear probe tip to create an air-tight seal.
- Mild sedation may be used in uncooperative patients and children.
- A probe is inserted into the ear. Increase the pressure to +200 mm of H2O. Reduce the pressure serially to 100, 50, 0 up to 400 mm of H2O to test the compliance at various pressures. Draw a graph with pressure on the X-axis and compliance on the Y-axis. The normal middle ear pressure is ± 25 mm of H2O, but for practical purposes, ± 100 mm of H2O is taken as normal.
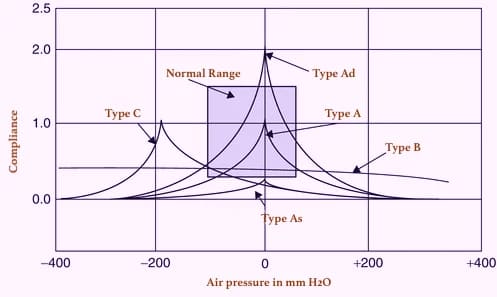
Types of tympanogram:
| Type A | Normal tympanogram (the peak is near zero pressure) |
| Type As | Compliance is lower at or near ambient air (zero) pressure. Hypo-mobile admittance is observed in otosclerosis, tympanosclerosis or malleus fixation. |
| Type Ad | High compliance at or near ambient pressure. Hypermobile admittance is observed in discontinuity of ossicular chain or thin, flaccid tympanic membrane. |
| Type B | A flat or dome-shaped graph. No change is seen in compliance with changes in pressure. This curve is seen in middle ear fluid, adhesive otitis media, thick or perforated TM, or grommet in situ. |
| Type C | Maximum compliance occurs with negative pressure in excess of 100 mm H2O. Seen in retracted tympanic membrane, fluid in middle ear. |
| Type D | A notched graph, seen in scarred and flaccid TM |
| Type E | An undulating graph, seen when an 8000 Hz sound is presented. This is seen in thick grafts after myringoplasty or in any mass. |
2.2 Eustachian tube function test.
Tympanometry can be used to assess eustachian tube function and confirm the integrity of the auditory system. Eustachian tube dysfunction plays a dominant role in the pathogenesis of suppurative and non-suppurative otitis media. The prognosis and treatment of both types of otitis media are dependent upon the eustachian tube function. Tests which can be done are: (a) William’s test (b) Toynbee’s test (c) Acoustic immittance.
(a) William’s test. It is done in an intact tympanic membrane. The impedance audiometer is programmed to measure the middle ear pressure in three conditions (i) the middle ear pressure at the beginning of the test (resting pressure), (ii) after swallowing (with the nose pinched and mouth closed) and (iii) after performing Valsalva.
Inference:
- Normal ET function: Middle ear pressure is the same as atmospheric pressure at rest, during swallowing or Valsalva.
- Impaired ET function: Pressure becomes negative during swallowing. It does not become positive on Valsalva or vice versa.
- Grossly impaired ET function. Pressure does not change at all in either of the situations.
(b) Toynbee’s test. is done in patients having a perforation in the tympanic membrane or grommet-in -situ. The test is similar to William’s test, where negative or positive pressure (−250 or +250 mm H2O) is created in the middle ear, and the person is asked to swallow five times in 20 seconds. The test is carried out for a fixed duration of time, e.g., 40 seconds (minimum) or 160 seconds (maximum). The ability to equilibrate the pressure with every act of swallowing indicates whether the patient is having normal tubal function or not.
(c) Acoustic immittance can also measure the physical volume of air between the probe tip and the tympanic membrane. Normally, it is up to 1.0 mL in children and 2 mL in adults. Any increase in volume >2 mL in children and >2.5 mL in adults indicates perforation of the tympanic membrane (because middle ear volume is added up to the volume of the external ear canal). This has also been used to find patency of the ventilation tube.
2.3 Acoustic (stapedial) reflex.
It is based on the fact that a loud sound 70–100 dB above the hearing threshold of one ear causes bilateral contraction of the stapedius muscle (which pulls the stapes slightly outward and upward) & and the tensor tympani muscle (pulls the tympanic membrane slightly inward). The effect is more pronounced on the stapedius muscle than on the tensor tympani. Stapedial reflex threshold (SRT): Minimal intensity of sound that produces stapedial reflex. (bilateral reflex)
Reflex arc:
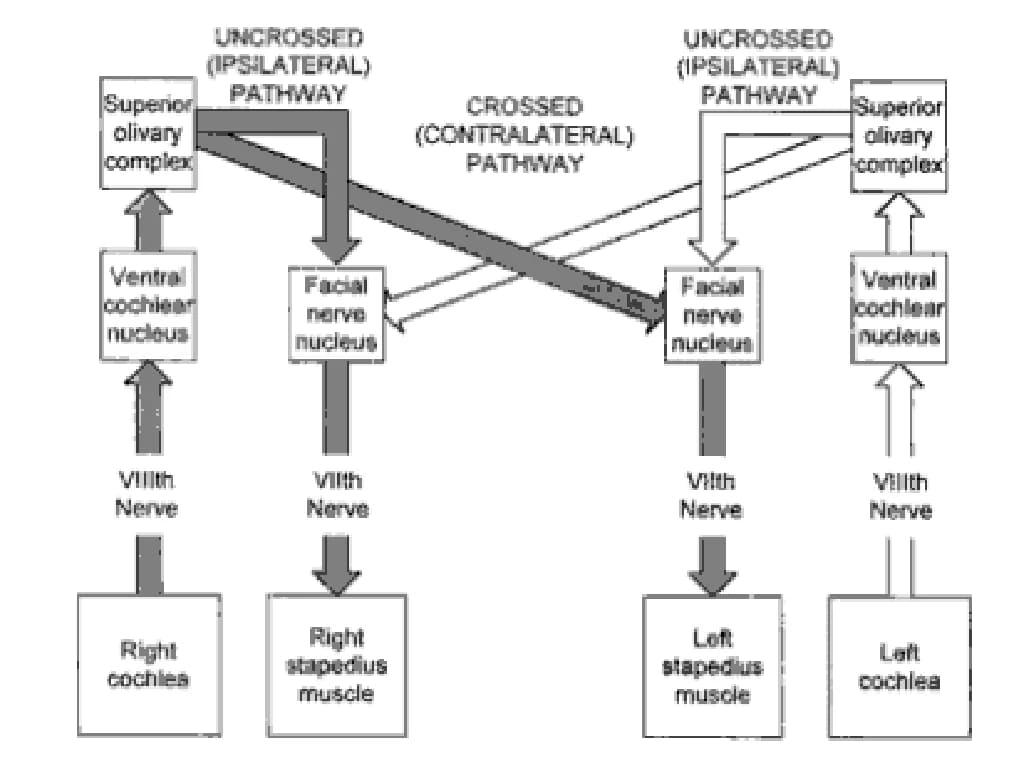
Ipsilateral ear: CN VIII → ventral cochlear nucleus → CN VII nucleus → ipsilateral stapedius muscle.
Contralateral ear: CN VIII → ventral cochlear nucleus → contralateral medial superior olivary nucleus → contralateral CN VII nucleus → contralateral stapedius muscle
Uses of acoustic reflex: It is very simple to perform, requires only a few minutes, and is a non-invasive objective test (it does not depend upon subjective responses from the patient)
Acoustic reflex tests help the otolaryngologist/neurologist :
- To test the hearing in infants, young children and uncooperative patients.
- To assess middle ear function accurately.
- To differentiate cochlear and retro-cochlear pathology. In cochlear lesion, the stapedial reflex is present at lower intensities, e.g. 40–60 dB, than the usual 70 dB(recruitment phenomenon)
- To detect brain-stem pathologies: If the ipsilateral reflex is present but the contralateral reflex is absent, the lesion is in the area of crossed pathways in the brainstem.
- To detect non-organic hearing loss: A malingerer does not give any response on pure tone audiometry but shows a positive stapedial reflex.
- To identify the level of lesion in facial nerve paralysis: Absence of stapedial reflex when hearing is normal indicates a lesion of the facial nerve, proximal to the nerve to stapedius. The reflex can also be used to find the prognosis of facial paralysis, as the appearance of the reflex after it was absent indicates return of function and a favourable prognosis.
- To detect VIIIth nerve lesion: If a sustained tone of 500 or 1000 Hz, delivered 10 dB above acoustic reflex threshold, for a period of 10 s, brings the reflex amplitude to 50%, it shows abnormal adaptation and is indicative of VIIIth nerve lesion (stapedial reflex decay).
3. Objective Tests for Inner Ear Hair Cell Function – Otoacoustic emissions (OAEs).
An ever-evolving, fast, easy-to-obtain, minimally invasive screening test used for screening for hearing loss in early life. OAE tests play an important role in monitoring ototoxicity and noise-induced hearing loss (NIHL) because OAEs can detect outer hair cell dysfunction earlier than a pure tone audiogram can.
Pathophysiology: OAEs are the sounds of low intensity produced by the outer hair cells of a normal cochlea and recorded from the external auditory canal with the help of a sensitive microphone placed in the external ear canal. The sound produced by the outer hair cells travels in a reverse direction: outer hair cells → basilar membrane → perilymph → oval window → ossicles → tympanic membrane → ear canal.
OAEs are present in healthy outer hair cells, which help to test the functional status of the cochlea. OAEs are present in healthy outer hair cells and can be recorded in virtually all individuals with normal cochlear function and a normal middle ear. OAEs are absent in lesions of the cochlea (when hearing loss exceeds approximately 30 dB), middle ear disorders (as sound travelling in the reverse direction cannot be picked up), and in the presence of significant ambient noise. It is important to note that OAEs are typically present in normal-hearing individuals.
Types of OAEs:
(i) Spontaneous OAE’s are seen in persons with normal hearing or when hearing loss is < 30 dB.
(ii) Evoked OAE’s. Depending on the sound stimulus used, evoked OAE may be:
- Transient evoked OAEs (TEOAEs): A series of click stimuli is presented at 80–85 dB SPL (sound pressure level), and the response is recorded. TEOAEs can be recorded from 500–4000Hz, but are more sensitive to hearing loss at 500 and 1000 Hz.
- Distortion product OAEs (DPOAEs): Two continuous tones of moderate intensity, e.g. 55 and 65dB SPL, are presented to the cochlea at the same time to produce distortion. They are used to test hearing in the range of 1000–8000 Hz, but have a better clinical performance for hearing loss at 4000 Hz.
Uses of OAE’s
- OAEs are used to distinguish between deafness caused by cochlear and retro-cochlear lesions. OAEs are absent in cochlear lesions, e.g. ototoxic sensorineural hearing loss.
- DPOAEs may be used to monitor ototoxicity effects earlier than pure tone audiometry.
- It may also be used in non-cooperative or mentally unwell patients, in non-organic hearing loss after giving sedation. Sedation does not affect OAEs.
Disadvantages:
- It is advisable to do tympanometry with OAEs because the middle ear pathology may interfere with the recording of OAEs. There are chances that the clinicians may misinterpret the absence of OAEs as a sensorineural hearing loss if they are unaware of the existence of middle ear pathology.
- OAEs may not diagnose auditory neuropathy in the neonates. Auditory neuropathy is a hearing disorder characterised by abnormal or absent auditory brainstem response in the presence of normal outer hair cell function. Therefore, AABR is the best method in the NICU/SCBU population to detect auditory neuropathy.
OAE test results are affected by the ambient noise level and the patient’s internal noise level (e.g. breathing or body movements. Therefore, the results of OAE tests should be interpreted in conjunction with pure tone audiometry, tympanometry, etc.
4. Objective Assessment of the Neural Pathway (Auditory Evoked Potentials)
Auditory Evoked Potentials (AEPs) are objective tests that record the electrical potentials (brain waves) generated by various parts of the auditory pathway in response to auditory stimulation. An averaging computer is essential to extract these tiny potentials from the larger background electrical activity of the brain (EEG). While many AEP components exist, two have gained significant clinical acceptance: Electrocochleography (ECoG) and Brainstem Auditory Evoked Response (BAER/ABR).
4.1 Electrocochleography (ECoG)
ECoG measures the electrical potentials generated specifically by the cochlea and the auditory nerve (CN VIII) in response to an auditory stimulus.
Potentials Measured: It records three main potentials:
- Cochlear Microphonics (CM): An alternating current (AC) potential generated primarily by the outer hair cells of the cochlea, which mirrors the waveform of the stimulus.
- Summating Potential (SP): A direct current (DC) potential reflecting the summed response of inner hair cells and possibly outer hair cells.
- Action Potential (AP): A compound action potential generated by the synchronized firing of many auditory nerve fibers (CN VIII).
Procedure: ECoG is an objective test providing a reasonably accurate measurement of hearing thresholds between 1000 Hz and 8000 Hz. It typically requires inserting a thin, needle-like active recording electrode through the tympanic membrane and placing it onto the promontory or round window (transtympanic ECoG). Reference and ground electrodes are placed on the mastoid process and forehead, respectively. This procedure is usually done under sedation or local anesthesia due to its invasive nature. (Non-invasive extratympanic ECoG also exists, with electrodes in the ear canal, but provides smaller responses).
Uses of ECoG:
- Diagnosing Meniere’s Disease: A significantly enlarged SP/AP ratio (typically > 0.4 in transtympanic ECoG) is a highly characteristic finding in Meniere’s disease, indicative of endolymphatic hydrops. This is a key diagnostic marker.
- Detecting Hearing Thresholds in Difficult-to-Test Populations: It can estimate hearing thresholds (within 5-10 dB) in young infants, children, and uncooperative patients.
- Differentiating Cochlear from Eighth Nerve Lesions: By analyzing the characteristics of CM, SP, and AP, ECoG helps pinpoint the site of lesion within the inner ear or auditory nerve.
- Intraoperative Monitoring: Surgeons use ECoG to monitor the function of the cochlea and cochlear nerve during neurotological surgical procedures (e.g., acoustic neuroma removal, vestibular neurectomy) to preserve hearing.
4.2 Brainstem Auditory Evoked Response (BERA)
ABR (Auditory Brainstem Response), also widely known as BAER or BERA, is an objective, non-invasive electrophysiological test that assesses the structural integrity and functional status of the auditory pathway from the spiral ganglia (distal CN VIII) to the level of the lateral lemniscus in the midbrain. Jewett and Williston introduced this test.
Principle: A series of very small electrical potentials are generated by the activation of different parts of the auditory system in response to brief auditory stimuli (clicks or tone bursts). These potentials are recorded by surface electrodes placed on the scalp. Since these neurogenic potentials are extremely small and “buried” in the background spontaneous electrical activity of the brain (EEG waves) and muscle activity (myogenic potentials), an averaging computer is required to summate the responses to hundreds or thousands of stimuli, effectively filtering out noise and revealing the consistent AEPs.
Procedure:
- Environment: Conduct the test in a quiet, sound-attenuating room.
- Patient State: The patient lies in a supine position, relaxed, with eyes closed, and preferably asleep (especially for children or uncooperative adults) to reduce myogenic potentials. Accurate assessment in children often requires mild sedation.
- Testing Protocol: Test one ear at a time.
- Electrode Placement: Three surface electrodes are typically used:
- Active Electrode: Placed on the vertex of the scalp (the best location) or, if not feasible, on the top of the forehead just below the hairline.
- Reference Electrode: Placed on the earlobe or mastoid of the tested ear.
- Ground Electrode: Placed on the earlobe or mastoid of the opposite ear.
- Stimulus: A series of 1000-2000 clicks (broadband stimuli, effective for higher frequencies) are delivered at a rapid rate (e.g., 11.1 clicks/second) at an intensity of typically 60-80 dB nHL (normalized hearing level, which correlates to average normal hearing). Tone bursts can be used for more frequency-specific information.
- Recording Window: The neurogenic potentials elicited are recorded for the first 10-15 milliseconds after stimulus onset. This specific time window captures the electrical responses as they travel through the brainstem alone.
- Waveforms: In a normal-hearing person, ABR typically produces seven distinct waves (I-VII) in the first 10-15 milliseconds. Waves I, III, and V are the most stable and clinically significant for interpretation.
Characteristics of ABR Waves: The interpretation of ABR relies on analyzing three main characteristics:
- Latency:
- Absolute Latency: The time interval (in milliseconds) between the onset of the stimulus and the peak of a specific wave.
- Inter-wave Latency (Interpeak Latency): The time interval between two different waves in the same ear and the same ABR tracing (e.g., I-III interval, III-V interval, I-V interval). This reflects conduction time between specific brainstem nuclei.
- Interaural Latency Difference: The difference in the absolute latency of the same wave (most commonly Wave V) between the two ears. A significant interaural difference (e.g., > 0.2-0.3 ms for Wave V) can indicate unilateral pathology.
- Amplitude: The peak-to-trough voltage of each wave. (Less stable and less clinically used than latency).
- Morphology: The shape and clarity of the waves.
Upper Limits of Normal ABR Values (Approximate):
- Latency of Wave V: ~5.5 – 5.9 ms
- I–V Inter-wave Interval: ~4.0 – 4.4 ms
- I–V Interaural Latency Difference: < 0.3 ms
Anatomical Generators of ABR Waves (EE COLI Mnemonic for NEET PG):
- Wave I: Distal portion of the VIIIth Cranial Nerve (Auditory Nerve), near the cochlea.
- Wave II: Proximal portion of the VIIIth Cranial Nerve, near the brainstem.
- Wave III: Cochlear Nucleus (in the pons).
- Wave IV: Superior Olivary Complex (in the pons).
- Wave V: Lateral Lemniscus (at the level of the inferior colliculus in the midbrain). This is the most robust and clinically important wave, often used for threshold estimation.
- Waves VI and VII: Inferior Colliculus and higher brainstem pathways.
- Mnemonic (EE COLI): Eighth nerve (distal), Eighth nerve (proximal), Cochlear nucleus, Olivary complex, Lateral Iemniscus, Inferior colliculus. (Compare with E COLI-MA in pathways of hearing, indicating how the mnemonic maps to the pathway).
| Wave I | Distal part of CN VIII |
| Wave II | Proximal part of CN VIII near the brainstem |
| Wave III | Cochlear nucleus |
| Wave IV | Superior olivary complex |
| Wave V | Lateral lemniscus |
| Waves VI and VII | Inferior colliculus |
As per latest studies these are anatomic site of neural generators for various waves.
Uses of ABR: ABR is a versatile test with numerous applications:
- Objective Hearing Assessment: It is the gold standard objective test for estimating hearing thresholds in infants, young children, non-cooperative adults, malingerers, and comatose/unconscious patients. It requires minimal patient cooperation.
- Diagnosing Retrocochlear Pathologies: ABR is highly sensitive (around 90-95%) for detecting lesions of the auditory nerve or brainstem, particularly acoustic neuromas (vestibular schwannomas). Prolongation of absolute latencies (especially Wave V), prolongation of inter-wave latencies (e.g., I-V interval), or a significant interaural latency difference strongly suggests a retrocochlear lesion.
- Diagnosing Brainstem Pathology: It can help identify the site of lesions within the brainstem, such as those caused by multiple sclerosis or pontine tumors, which affect neural conduction.
- Intraoperative Monitoring: Surgeons use ABR to monitor and preserve the auditory nerve (CN VIII) during complex neurotological surgeries, such as the removal of acoustic neuromas or other cerebellopontine angle tumors. This helps prevent iatrogenic hearing loss.
Disadvantages and Limitations of ABR:
- Not Frequency-Specific: ABR, especially when using clicks, primarily reflects high-frequency hearing (2000-4000 Hz) due to the transient nature of the click stimulus. It does not give precise frequency-specific information across the entire audiometric range, and low-frequency hearing losses are often undetectable. Therefore, additional tests like ASSR are needed for a comprehensive frequency-specific audiogram in objective assessments.
- Sensitivity for Small Tumors: While highly sensitive for detecting large tumors, ABR may miss small acoustic neuromas (<1 cm). Therefore, MRI remains a more sensitive and specific test for definitive diagnosis of acoustic neuroma.
- Effect of Hearing Loss: ABR waves are typically absent or severely distorted in patients with severe or profound hearing loss (>75 dB HL). Conductive hearing loss also attenuates cochlear stimulation and prolongs ABR wave latencies, necessitating careful interpretation and often masking.
- No “Gold Standard” Standardisation: While widely used, there isn’t a single universal standardisation for ABR interpretation across all clinics.
- Age and Consciousness: While valuable for non-cooperative patients, ABR testing itself requires the patient to be relatively still and quiet. Although sedation does not affect the ABR waves, it may be needed for accurate assessment in infants and young children, adding complexity.
- Wave I Identification: Wave I is often not easily identifiable, particularly at lower stimulus intensities, which can make I-III and I-V interval calculations challenging.
4.3 Auditory Steady State Response
It is an electrophysiological test to predict the frequency-specific hearing thresholds. The steady-state pure tone signals(modulated in amplitude and frequency) are used in ASSR unlike, the transient signals of tone bursts or clicks used in ABR producing a frequency-specific audiogram.
Uses :
- Hearing loss of more than 80 dB can be detected. It can help in the early detection of the children who need cochlear implantation.
- ASSR can be done in all ages, any mental state, and any degree of hearing loss.
- Multiple frequencies can be assessed at the same time, as long as their carrier frequencies utilize different modulation rates.
- ASSR is an objective test that can be analysed and interpreted easily using statistical methods.
5. Special Diagnostic Tests
5.1 Recruitment
Recruitment is a phenomenon where a sound of a particular intensity becomes abnormally loud and intolerable to a patient. Patients with recruitment experience an inability to hear low-intensity sounds in the affected ear, but high-intensity sounds are perceived as equally loud or even louder than in a normal hearing ear. Recruitment is commonly seen in patients with cochlear dysfunction, making them poor candidates for hearing aids.
The Alternate Binaural Loudness Balance (ABLB) test is used to detect recruitment in unilateral cases. In this test, a tone, such as 1000 Hz, is played alternately to the normal and affected ear, with the intensity in the affected ear adjusted to match the loudness in the normal ear. The test begins at 20 dB above the threshold of the deaf ear and is repeated at every 20 dB increase until the loudness is matched or the limits of the audiometer are reached. In cases of conductive and neural deafness, the initial difference is maintained throughout, while in cochlear lesions, partial, complete, or over-recruitment may be observed.
5.2 Short Increment Sensitivity Index (SISI)
The Short Increment Sensitivity Index (SISI) test assesses a patient’s ability to detect small changes in the intensity of pure tones. Patients with cochlear lesions can better appreciate these small changes compared to normal subjects or those with conductive or retro-cochlear dysfunction. Thus, the SISI test is used to differentiate cochlear from retro-cochlear lesions.
Procedure: A continuous, supra-threshold tone (20 dB above the hearing threshold) is presented to the patient for 2 minutes. The tone is then increased by 1 dB every 5 seconds, with 20 such increments. The patient is instructed to count the number of increments they hear.
Interpretation:
- Conductive deafness: SISI score < 15%
- Nerve deafness: SISI score 0–20%
- Cochlear deafness: SISI score 70–100%
Disadvantages: Patients with severe deafness (above 85 dB) cannot be tested with most clinical audiometers, and the test requires active cooperation from the patient.
5.3 Threshold Tone Decay Test
The Threshold Tone Decay Test measures auditory nerve fatigue or adaptation, specifically assessing how long a patient can continuously perceive a tone presented near their threshold.
Principle: Normally, a pure tone presented slightly above the absolute hearing threshold can be heard continuously for at least 60 seconds. However, in cases of retrocochlear lesions affecting the auditory nerve, the nerve’s ability to sustain firing decreases rapidly, causing the patient to stop hearing the tone much sooner.
Procedure:
- Present a tone at a frequency of 4000 Hz (or other frequencies) at an intensity 5 dB above the patient’s hearing threshold.
- Instruct the patient to indicate as long as they hear the tone, up to 60 seconds.
- If the patient stops hearing the tone before 60 seconds, increase the intensity by another 5 dB, and repeat the process.
- Continue this 5 dB incremental increase until the patient can hear the tone continuously for 60 seconds, or until the maximum output of the audiometer is reached.
- The total increase in intensity required to sustain the tone for 60 seconds (or the amount of decay observed) is measured in “decibels of decay.”
Interpretation:
- Normal Hearing/Conductive Loss/Cochlear Loss: Decay is typically less than 15-20 dB.
- Cochlear Hearing Loss: A decay between 15 and 20 dB may indicate cochlear hearing loss (often related to recruitment).
- Retrocochlear Lesion: A decay of more than 25 dB (significant tone decay) is highly diagnostic of a retrocochlear lesion (e.g., acoustic neuroma, auditory neuropathy), indicating auditory nerve fatigue or pathology.
6. Central Auditory Tests
Useful in children with language delay and adults with cortical lesions.
- Dichotic Listening Tests: Two different signals to each ear.
- Distorted Speech Tests: Check processing ability under degraded conditions.
———— End of the chapter ————
High-Yield Points for Exam Revision
- PTA Gold Standard: PTA is subjective; BC masking is always required.
- SRT vs. PTA: A significant discrepancy (>10 dB) suggests non-organic hearing loss.
- Type B Tympanogram: Think “Fluid, Perforation, or Wax.”
- Acoustic Reflex: Its presence with a “dead ear” on PTA = non-organic hearing loss. Reflex decay = VIIIth nerve lesion.
- OAEs: Represent outer hair cell function. Absent in cochlear loss >30dB, but present in Auditory Neuropathy.
- ABR Waves (EE COLI): Wave V is the most robust. A prolonged I-V interval is classic for a retrocochlear lesion (e.g., acoustic neuroma).
- ECoG in Meniere’s: An SP/AP ratio >0.4 is diagnostic.
- Recruitment: Pathognomonic of cochlear lesions.
- Significant Tone Decay: Pathognomonic of retrocochlear lesions.
NEET PG & University Exam-Style MCQs
- A 45-year-old female presents with unilateral tinnitus and hearing loss. An ABR test reveals a prolonged I-V interwave interval on the affected side. The most likely diagnosis is: A) Meniere’s disease B) Otosclerosis C) Acoustic neuroma D) Noise-induced hearing loss
- In a patient with suspected otosclerosis, which of the following tympanogram patterns is most likely to be found? A) Type A B) Type As C) Type Ad D) Type B
- Otoacoustic emissions (OAEs) are generated by which of the following structures? A) Inner hair cells B) Stria vascularis C) Outer hair cells D) Tympanic membrane
- A newborn fails the OAE screening test but passes the ABR test. What is the most likely diagnosis? A) Congenital aplasia of the cochlea B) Auditory Neuropathy Spectrum Disorder (ANSD) C) Middle ear effusion D) Severe sensorineural hearing loss
- The acoustic stapedial reflex arc involves all of the following EXCEPT: A) Cochlear nucleus B) Medial geniculate body C) Superior olivary complex D) Facial nerve nucleus
- A patient has a unilateral sensorineural hearing loss. On performing the SISI test, the score is 90%. This indicates a lesion at the: A) Middle ear B) Cochlea C) Eighth cranial nerve D) Brainstem
- In Electrocochleography, an enlarged Summating Potential/Action Potential (SP/AP) ratio is most characteristic of: A) Acoustic neuroma B) Otosclerosis C) Meniere’s disease D) Presbycusis
- Masking is routinely used in bone conduction testing because: A) It prevents the test ear from hearing the signal. B) The bone vibrator is less efficient than headphones. C) Bone-conducted sound stimulates both cochleae. D) It improves patient comfort during the test.
- A patient with a perforated tympanic membrane is most likely to show which type of tympanogram? A) Type A B) Type As C) Type B D) Type C
- The Speech Detection Threshold (SDT) is expected to most closely correspond to the pure-tone threshold at which frequency? A) 250 Hz B) 500 Hz C) 1000 Hz D) 2000 Hz
Answers & Explanations:
- C) Acoustic neuroma. A prolonged I-V interval is a classic finding in retrocochlear pathology like a vestibular schwannoma.
- B) Type As. Otosclerosis causes fixation of the ossicles, leading to reduced compliance (a shallow, Type As tympanogram).
- C) Outer hair cells. OAEs are sounds produced by the motile activity of healthy outer hair cells.
- B) Auditory Neuropathy Spectrum Disorder (ANSD). OAEs are present (normal outer hair cells), but ABR is absent/abnormal (neural dys-synchrony). Middle ear effusion (C) is also common but would typically affect both tests.
- B) Medial geniculate body. The reflex arc is a brainstem-level phenomenon and does not reach the thalamus (Medial Geniculate Body).
- B) Cochlea. A high SISI score (>70%) is highly suggestive of a cochlear lesion due to the phenomenon of recruitment.
- C) Meniere’s disease. The enlarged SP is due to the mechanical distortion of the basilar membrane in endolymphatic hydrops.
- C) Bone-conducted sound stimulates both cochleae. This is the fundamental reason why masking is always necessary in BC testing to isolate the test ear.
- C) Type B. A perforation leads to a large, non-compressible volume, resulting in a flat (Type B) tympanogram.
- B) 500 Hz. The SDT typically correlates best with the pure-tone average in the lower frequencies, especially 500 Hz.
Clinical Case Scenarios for Viva Voce
Case 1: The Newborn Refer
- Scenario: A newborn is referred after failing the universal hearing screening. The OAE test was “absent,” but the ABR test shows clear and repeatable waves with normal latencies.
- Question: What is the most likely diagnosis, and what is the pathophysiological basis?
- Answer: Auditory Neuropathy Spectrum Disorder (ANSD). The absent OAEs could be due to a mild middle ear issue or severe cochlear loss, but the normal ABR is contradictory. In true ANSD, OAEs are typically present (normal outer hair cells) but ABR is absent (neural dys-synchrony). This case highlights the importance of a test battery. The next step would be a diagnostic ABR with threshold estimation.
Case 2: The Imbalance and Hearing Loss
- Scenario: A 55-year-old man presents with episodic vertigo, aural fullness, tinnitus, and fluctuating hearing loss in his right ear.
- Question: Which objective test is most specific for confirming the diagnosis, and what finding are you looking for?
- Answer: Electrocochleography (ECoG). The clinical picture is classic for Meniere’s disease. The key finding on ECoG is an enlarged SP/AP ratio (>0.4), which indicates endolymphatic hydrops.
Case 3: The Asymmetric Hearing Loss
- Scenario: A 40-year-old woman has a slowly progressive, asymmetric sensorineural hearing loss on the left. Tuning fork tests (Rinne) are positive bilaterally, but Weber lateralizes to the right.
- Question: What is the most concerning diagnosis, and which is the most sensitive objective audiological test to order first?
- Answer: The concern is a retrocochlear lesion, such as a vestibular schwannoma. The most sensitive initial audiological test is the Auditory Brainstem Response (ABR). You would look for a prolonged I-V interwave interval or an interaural latency difference in Wave V on the affected side. An MRI is the definitive diagnostic test.
Case 4: The Factory Worker
- Scenario: A factory worker on aminoglycoside antibiotics for a resistant infection is concerned about ototoxicity.
- Question: Which test can detect ototoxicity before it becomes evident on a standard pure-tone audiogram?
- Answer: High-Frequency Distortion Product Otoacoustic Emissions (DPOAEs). Ototoxicity typically affects the outer hair cells in the high-frequency basal region of the cochlea first. DPOAEs can detect this dysfunction earlier than conventional PTA, which only goes up to 8000 Hz.
Frequently Asked Questions (FAQ) in Exams
- What is the difference between conductive and sensorineural hearing loss on an audiogram? Conductive loss shows an Air-Bone Gap (BC normal, AC elevated), while sensorineural loss shows both AC and BC elevated with no significant gap.
- Why is masking necessary in audiometry? Masking prevents the non-test ear from participating in the test, ensuring that the thresholds recorded are truly from the ear being tested, especially when there is a significant difference in hearing between the two ears.
- What does a flat (Type B) tympanogram indicate? A Type B tympanogram indicates no point of maximum compliance, suggesting a condition that restricts tympanic membrane movement, such as middle ear fluid (effusion), a perforation, or impacted wax.
- How does ABR help in diagnosing an acoustic neuroma? ABR helps by showing a delay in the neural conduction along the auditory nerve and brainstem, specifically seen as a prolonged I-V interwave interval or a significant delay in Wave V latency in the affected ear.
- Can OAE tests diagnose all types of hearing loss? No, OAE tests are excellent for detecting cochlear (outer hair cell) dysfunction but are normal in Auditory Neuropathy and cannot diagnose retrocochlear or central auditory processing disorders. They also cannot be recorded if there is middle ear pathology.
- What is the clinical significance of recruitment? Recruitment is the abnormal growth of loudness and is a hallmark of cochlear hearing loss. It makes patients poor candidates for hearing aids because soft sounds are inaudible, but loud sounds quickly become intolerable.
- Which test is best for newborn hearing screening? Most universal newborn hearing screening programs use a two-tiered approach: OAE followed by ABR for those who refer. OAE is fast and sensitive, while ABR is used to confirm the loss and rule out Auditory Neuropathy.
Learning Aids & Mnemonics
- ABR Wave Generators (EE COLI): A must-know for exams.
- Eighth nerve (distal) -> Eighth nerve (proximal) -> Cochlear Nucleus -> Olivary Complex -> Lateral Lemniscus -> Inferior Colliculus.
- When to Mask for Air Conduction: Remember the number 40. Mask if the interaural difference is >40 dB with headphones. (For insert phones, it’s 55 dB).
- Tympanogram Types:
- A = Acceptable (Normal).
- As = Stiff (e.g., Otosclerosis).
- Ad = Discontinuity.
- B = Bad/Blocked (Fluid, Perforation).
- C = Congested (Negative Pressure).
Viva Tip: When presented with an audiogram, follow a structured approach: 1) Identify the symbols, 2) Describe AC and BC thresholds for each ear, 3) Identify the type of loss (Conductive, Sensorineural, Mixed), 4) Comment on the degree and configuration (e.g., moderately-severe sloping SNHL). This systematic method impresses examiners.
———— End of the chapter ————
Download full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page:https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Juvenile Angiofibroma. https://www.entlecture.com/juvenile-angiofibroma/
- Please read. Tumours of Hypopharynx . https://www.entlecture.com/tumours-of-the-hypopharynx/
- Please read. Anatomy of Oesophagus. https://www.entlecture.com/anatomy-of-oesophagus/
Keywords: Pure tone audiometry notes for MBBS students, What is PTA in ENT exam guide, How to interpret audiogram in pure tone audiometry, Speech audiometry SRT and SDS explained, Bekesy audiometry summary for ENT PG, Tympanometry and acoustic reflex test explained for medical students, Otoacoustic emissions (OAE) test basics for hearing screening, ABR BERA test procedure and interpretation for MBBS, Auditory Brainstem Response waves significance (I-V) MCQ prep, ASSR test for cochlear implant candidacy – explained, Eustachian tube function test (Toynbee, Valsalva) ENT revision notes, SISI test vs tone decay test to differentiate cochlear vs retrocochlear hearing loss, Central auditory processing tests (dichotic, distorted speech) explained, Hearing assessment chapter summary PDF for ENT students, MCQs on audiometry and objective hearing tests for NEET PG, Revision notes audiometry and objective tests for ENT practical exam, ENT CBME curriculum hearing test notes, Clinical case hearing loss + audiometry interpretation for MBBS exam, Hearing test flowchart and mnemonics for students, Audiometry and OAE vs ABR comparison guide for beginners, Master Pure Tone Audiometry: Easy ENT Notes, Understand Tympanometry & Reflex Testing Quickly, OAE & ABR Hearing Test Guide for MBBS/ENT PG, Audiometry & Objective Tests: Complete Revision Sheet, ABR (BERA) Interpretation – Clear & Concise Guide, Hearing Assessment MCQs & Revision Notes for NEET PG, Audiogram Interpretation Made Simple for Students, Otoacoustic Emissions Explained for Beginners, Tympanometry Types & Meaning – Student Cheat-Sheet, ENT Hearing Tests: Complete Exam Guide 2025, Dive into advanced audiometry for ENT professionals. This chapter covers Pure Tone Audiometry, Speech Audiometry, Impedance Audiometry, OAEs, ABR, and ASSR, with high-yield points, MCQs, and clinical scenarios for robust exam preparation. Pure Tone Audiometry (PTA), Audiogram Interpretation, Masking in Audiometry, Speech Audiometry SRT SDS, Rollover Effect Hearing, Bekesy Audiometry Types, Impedance Audiometry Principles, Tympanometry Types A B C, Eustachian Tube Function Test, Acoustic Reflex Test, Acoustic Reflex Arc, Recruitment Hearing, SISI Test Interpretation, Threshold Tone Decay, Auditory Evoked Potentials (AEPs), Electrocochleography (ECoG), Meniere’s Disease ECoG, Brainstem Auditory Evoked Response (ABR), ABR Wave Generators, Auditory Brainstem Response Uses, Auditory Steady State Response (ASSR), Otoacoustic Emissions (OAEs), Newborn Hearing Screening, Outer Hair Cell Function, Central Auditory Processing Disorder (CAPD), Objective Hearing Tests, Subjective Hearing Tests, Hearing Loss Diagnosis, Auditory Pathway Assessment, Conductive Hearing Loss Diagnosis, Sensorineural Hearing Loss Diagnosis, Mixed Hearing Loss Diagnosis, ENT Topics for NEET PG, MBBS ENT Notes Hearing Assessment, ENT Viva Questions Hearing Tests