Functional Endoscopic Sinus Surgery (FESS)
Functional Endoscopic Sinus Surgery (FESS) is the gold standard surgical treatment for Chronic Rhinosinusitis (CRS) unresponsive to maximal medical therapy.
- Definition: FESS is an endoscope-guided, minimally invasive procedure aimed at restoring the physiological function of the paranasal sinuses.
- Active Principle: The surgery adheres to the “maximum preservation, minimal removal” philosophy. We remove only the irreversibly diseased, pathological tissue (polyps, infected bone/mucosa) while meticulously preserving the surrounding healthy mucociliary lining.
- Primary Goal: To re-establish patent drainage and ventilation of the sinuses, primarily by clearing the Osteomeatal Complex (OMC). Therefore, a patent OMC allows the sinus mucosa to heal and permits effective delivery of post-operative topical medications.
Relevant Anatomy & Physiologic Basis
Physiology of the Paranasal Sinuses
- The paranasal sinuses (maxillary, frontal, anterior & posterior ethmoid, sphenoid) normally ventilate and drain into the nasal cavity via their ostia.
- Mucociliary clearance moves secretions toward the natural ostia; any blockage causes stasis → inflammation/infection.
- FESS aims to restore the normal ventilation and drainage pathways, thereby maintaining mucociliary function and reducing the recurrence of sinusitis.
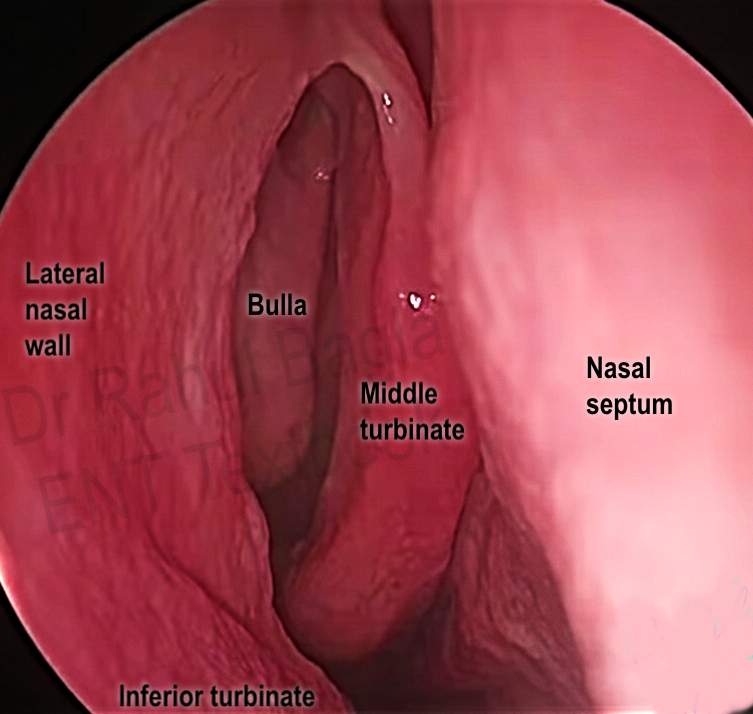
Surgical-Relevant Anatomy & Landmarks
- Uncinate process: a thin curved bone in the lateral wall of the nasal cavity; removal of this opens the infundibulum (often called “infundibulotomy”).
- Ethmoid bulla: the largest and most constant anterior ethmoid air cell; removal helps access the ethmoid air cells..
- Basal (ground) lamella: the bony partition that divides anterior and posterior ethmoid cells; a critical landmark.
- Lamina papyracea: the lateral bony wall of the ethmoid; adjacent to the orbit—injury here leads to orbital complications.
- Sphenoid sinus ostium & walls: within the sphenoid sinus, you will see bulges of the internal carotid artery (inferior-posterior) and optic nerve (supero-lateral) — crucial to avoid.
- Frontal recess/agger nasi cells: the drainage pathway of the frontal sinus; high-risk area for stenosis after surgery.
Indications of Functional Endoscopic Sinus Surgery (FESS):
1. Core Functional Indications (Aim: Restore Mucociliary Clearance). These are the classical FESS indications.
- Chronic Rhinosinusitis (CRS): With or without nasal polyps, refractory to at least 12 weeks of maximal medical therapy (including antibiotics, topical/systemic steroids, and saline irrigation).
- Fungal Sinusitis:
- Allergic Fungal Rhinosinusitis (AFRS): Requires extensive clearance and post-operative surveillance.
- Sinus Mycetoma (Fungus Ball): Removal of the concentrated fungal mass, often in the maxillary sinus.
- Sinus Mucoceles: Especially Frontoethmoidal Mucoceles, which require drainage and marsupialization.
2. Other Endoscopic Nasal and Skull Base Surgeries (Approach: Endoscopic Access). These use the nasal corridor but are not solely for restoring sinus function.
- Orbital Access:
- Endoscopic Dacryocystorhinostomy (DCR): To bypass Nasolacrimal Duct Obstruction (NLDO).
- Orbital Decompression: For compressive neuropathy (e.g., Graves’ Ophthalmopathy).
- Vascular/Tumour/Trauma Management:
- Endoscopic Sphenopalatine Artery Ligation (ESPAL): Definitive control for severe posterior epistaxis.
- Excision of Select Tumours: e.g., Inverted Papilloma, juvenile nasopharyngeal angiofibroma (JNA).
- Skull Base:
- CSF Leak Repair: Endoscopic repair of defects (e.g., cribriform plate).
- Transsphenoidal Hypophysectomy: Access to the pituitary gland.
Contraindications of FESS
- Absolute: Unfit for anaesthesia (severe cardiac/pulmonary disease), Uncontrolled bleeding disorder/coagulopathy, Acute severe sinus infection with complications (orbital/intracranial spread), Lack of proper facilities/surgical expertise
- Relative: Acute URTI, Pregnancy (elective cases), Revision FESS / distorted anatomy (higher risk), Poor compliance with follow-up and nasal douching
Preoperative Assessment/ Workup
- Detailed history + ENT examination
- Diagnostic Nasal Endoscopy (DNE)
- CT Scan PNS (Coronal + Axial) – Gold standard
- Routine investigations: CBC, sugar, renal function, PT/INR
- ECG / Chest X-ray (as required)
- Trial of maximal medical therapy before surgery
- Anaesthesia fitness + informed consent
Anaesthesia and Position of FESS
- Anaesthesia: Topical anaesthesia is standard. Therefore, the nose is packed with cotton patties for 4-5 minutes, soaked in a solution containing a local anaesthetic (e.g., 4% Lignocaine/Xylocaine) and a vasoconstrictor (e.g., Adrenaline 1:1000 or Oxymetazoline).
- Purpose: The packing achieves two goals: local anaesthesia for patient comfort and nasal decongestion to shrink the mucosa, which creates better working space.
- Position: Patient in supine position with head elevated 15°–30° (reverse Trendelenburg) to reduce venous congestion. Head turned slightly toward the surgeon.
Surgical Technique: FESS Steps
FESS is usually performed step by step, starting at the front (anterior) and progressing to the back (posterior). Read 🔗Anatomy of Internal Nose:
The main steps in FESS are:
Step 1: Uncinectomy (Infundibulotomy)
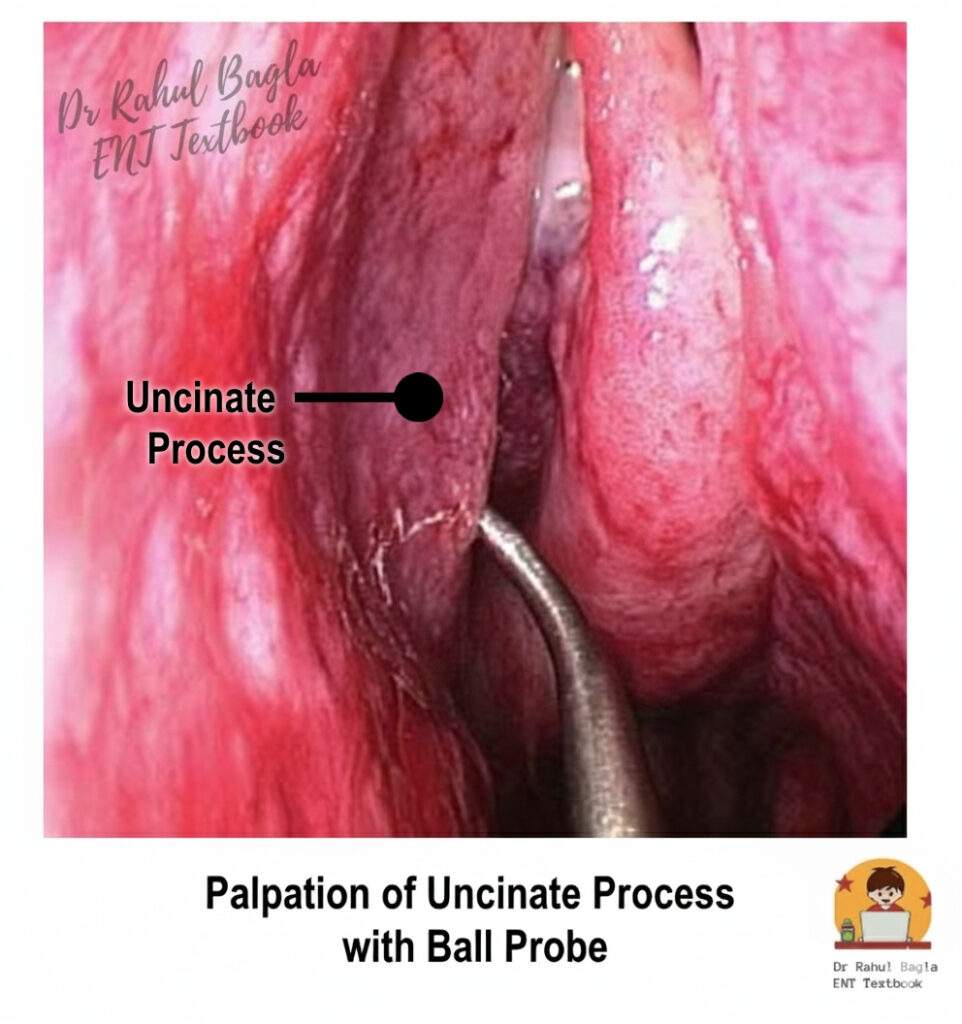
- First, palpate around the edge of the uncinate process with a ball probe or Freer’s elevator.
- Begin with the removal of the uncinate process to open the ethmoid infundibulum. Two approaches:
- Antegrade (anterior → posterior) using a sickle knife.
- Retrograde (posterior → anterior) using back-biting forceps (safer).

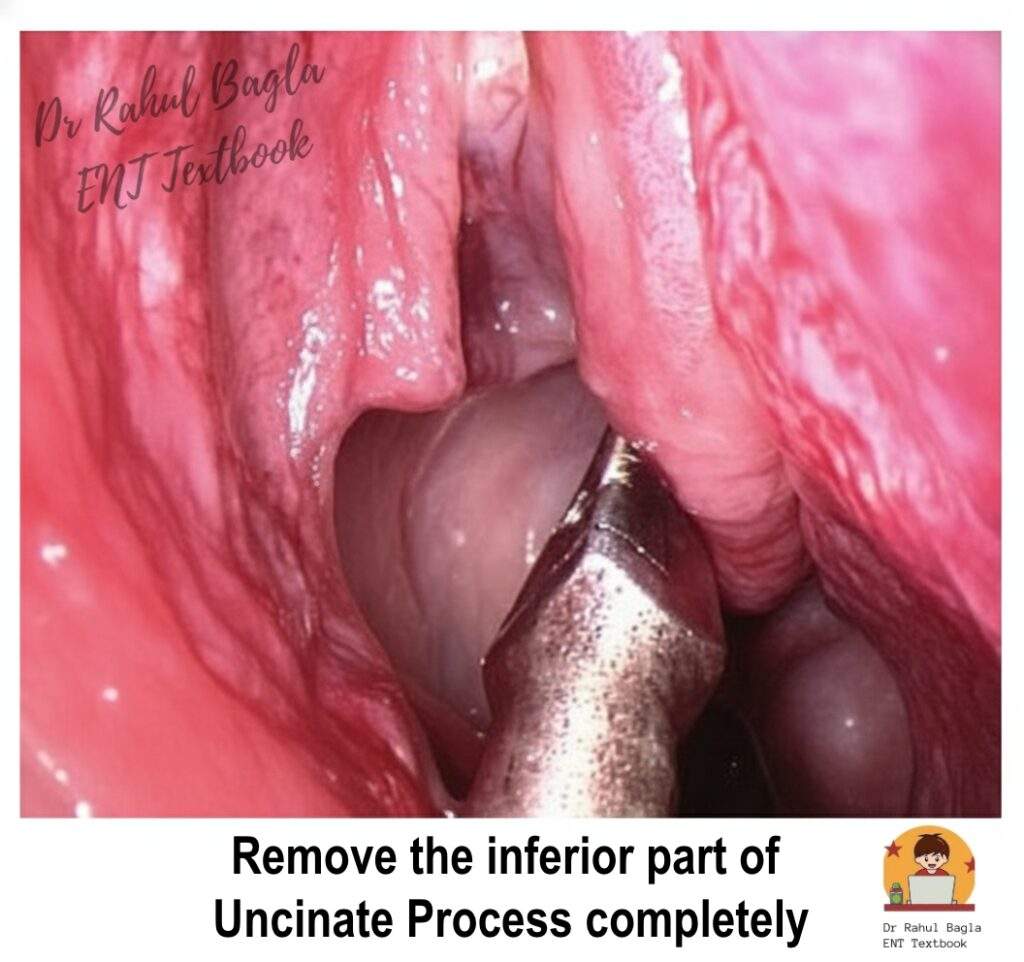
- Using back-biting forceps, take the first bite as low as possible near the base of the uncinate. This ensures the orbit (laterally) and the skull base (superiorly) are protected.
- Remove the inferior part completely in order to expose the maxillary sinus ostium.
- Avoid injury to the nasolacrimal duct (anteriorly) and lamina papyracea (laterally).
- The superior part of the UP’s attachment is the crucial landmark for the Frontal Recess and should be removed only if frontal sinus work is required.
- Anatomical variation: In ~70% the uncinate attaches to the lamina papyracea/lateral nasal wall, in ~30% it attaches to the skull base or the middle turbinate “armpit” area; in the latter, you need not remove it high unless the frontal recess is targeted.
- Benefit: By uncinectomy, you increase surgical access and ease of approaching the sinuses.
Step 2: Maxillary Ostium Widening (Middle Meatal Antrostomy)
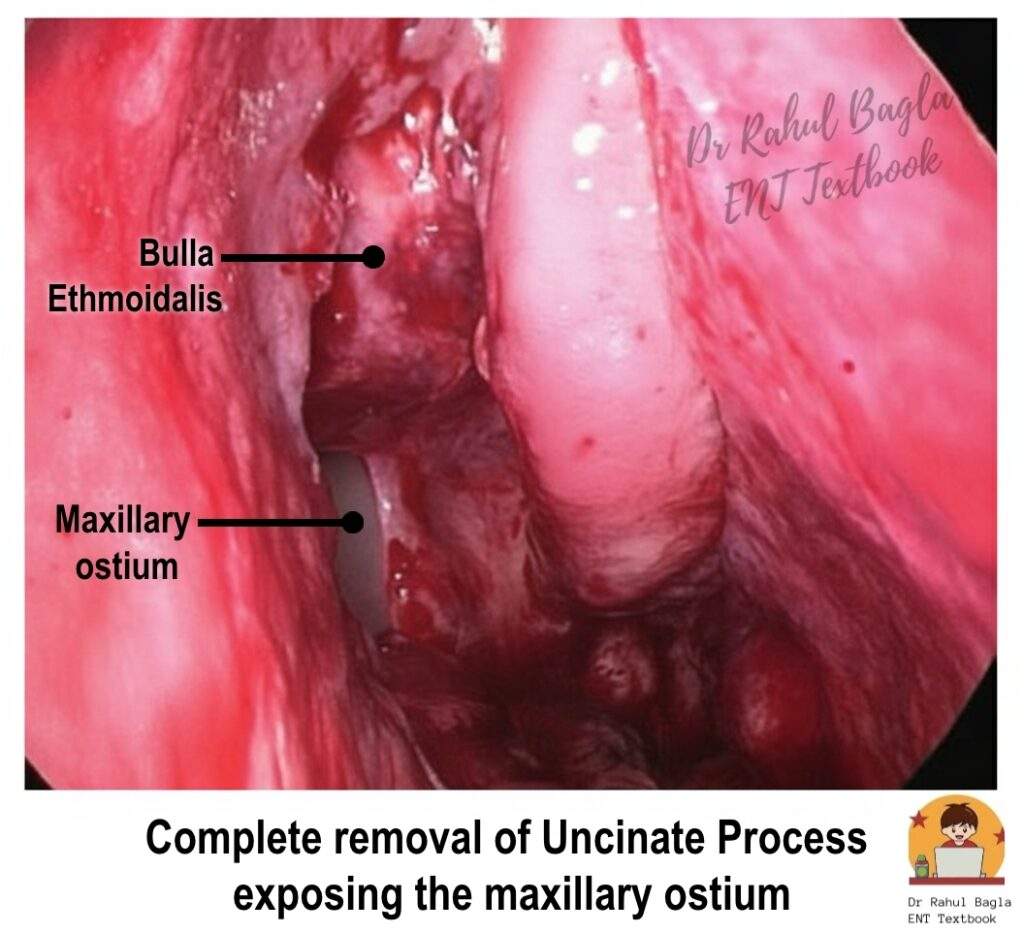
- After uncinectomy, identify the natural maxillary ostium in the ethmoid infundibulum.
- Enlarge it using a curved suction tip, cut forceps or microdebrider.
- Anterior extent is limited by the nasolacrimal duct; posterior enlargement may extend toward the posterior maxillary wall, depending on the disease.
- If an accessory ostium is present, merge it with the natural ostium to avoid “recirculation” of secretions.
- Use of a 30° endoscope allows visualisation into the maxillary sinus (the floor of the orbit, infra-orbital nerve bulge).
- Types of antrostomy (sinusotomy):
| Type | Description |
| Type 1 | Natural ostium enlarged posteriorly ≤ 1 cm. |
| Type 2 | Antrostomy diameter ≤ 2 cm, extended posteriorly & inferiorly. |
| Type 3 | Extended close to the posterior wall of the maxillary antrum, anterior to the lacrimal sac, and inferior to the base of the inferior turbinate. |
Step 3: Removal of Ethmoid Bulla & Anterior Ethmoidectomy
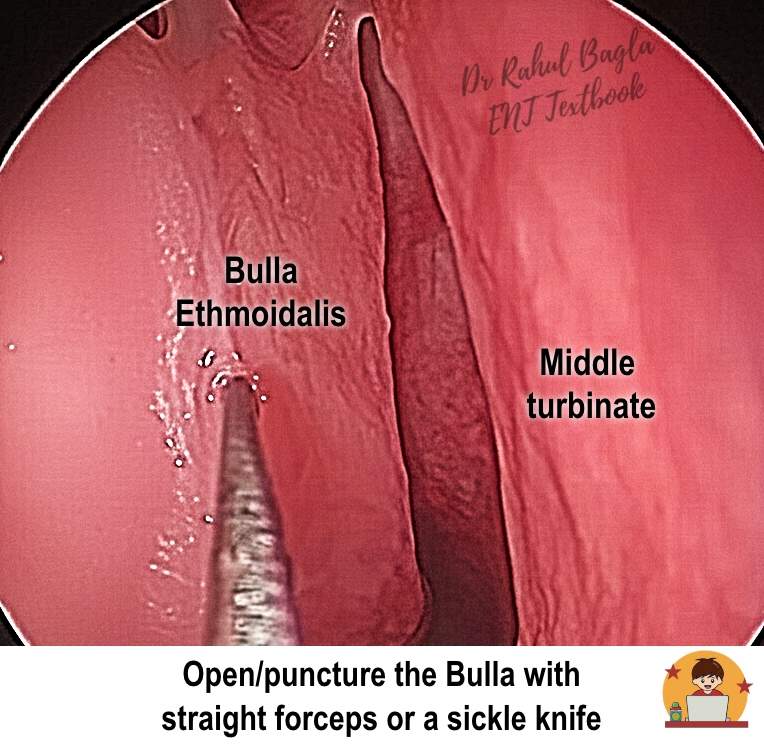
- Identify the ethmoid bulla (the largest and most constant anterior ethmoid air cell).
- Open/puncture it with straight forceps or a sickle knife.
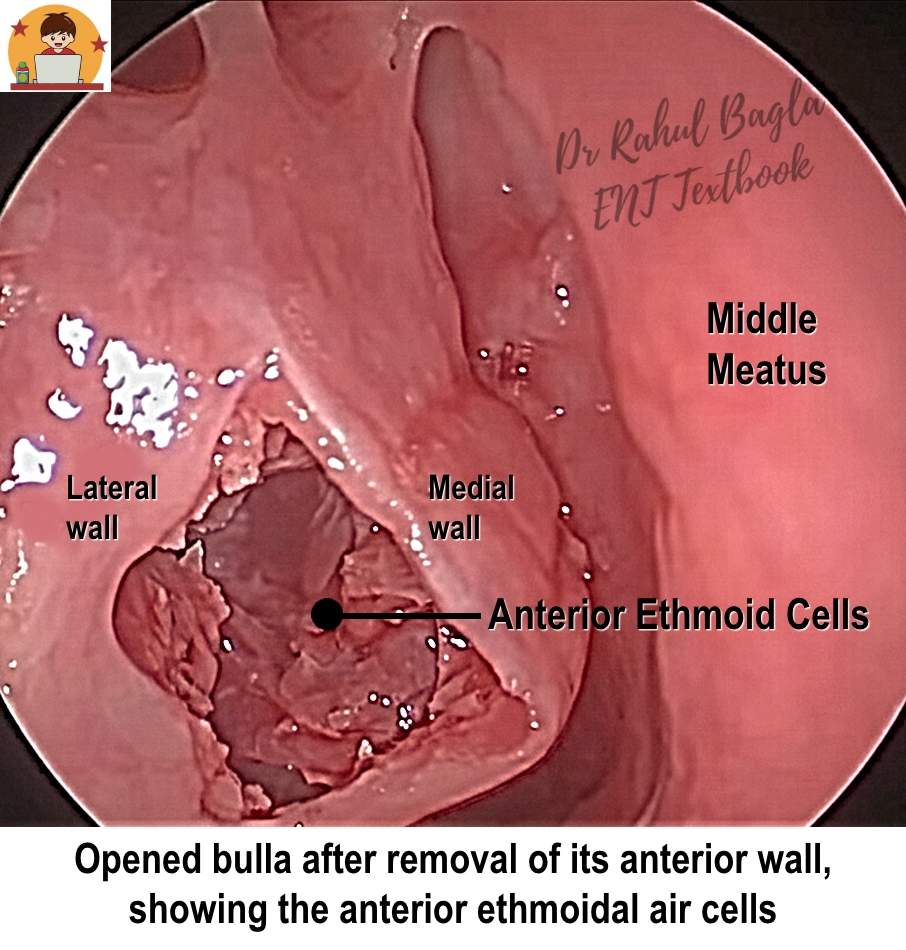
- Remove the medial and anterior wall of the bulla via an inferior-medial approach.
- Avoid dissection of the lateral wall as it is formed by the lamina papyracea, which is the medial wall of the orbit; hence, it can lead to injury to the orbit.
- Continue removing surrounding anterior ethmoid air cells until the basal (ground) lamella is reached.
- Recognise that the number and size of air cells vary according to the degree of pneumatization.
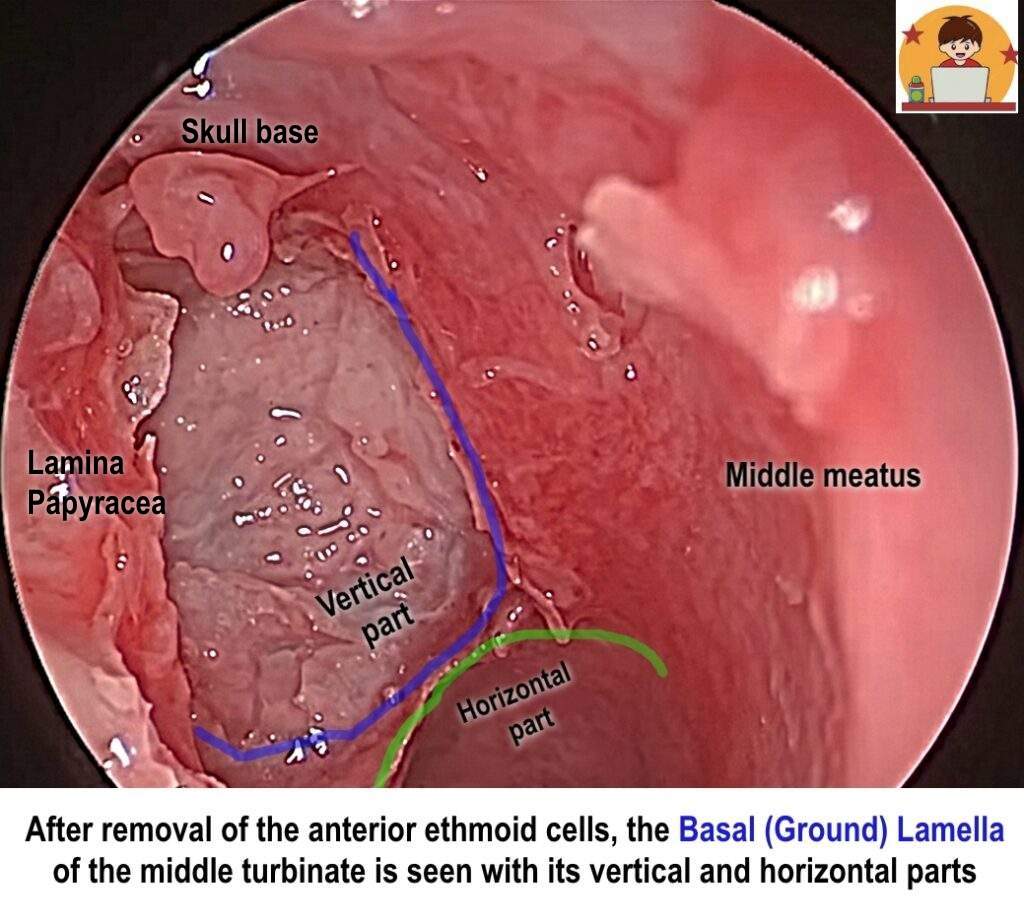
Step 4: Posterior Ethmoidectomy
- The basal lamella (the bony partition that divides anterior and posterior ethmoid cells) is removed to access the posterior ethmoid cells. The Basal Lamella (Ground Lamella) is a strong bony septum that represents the lateral attachment of the middle turbinate and separates the anterior and posterior ethmoid cells. It appears as an oblique, thin bony plate.
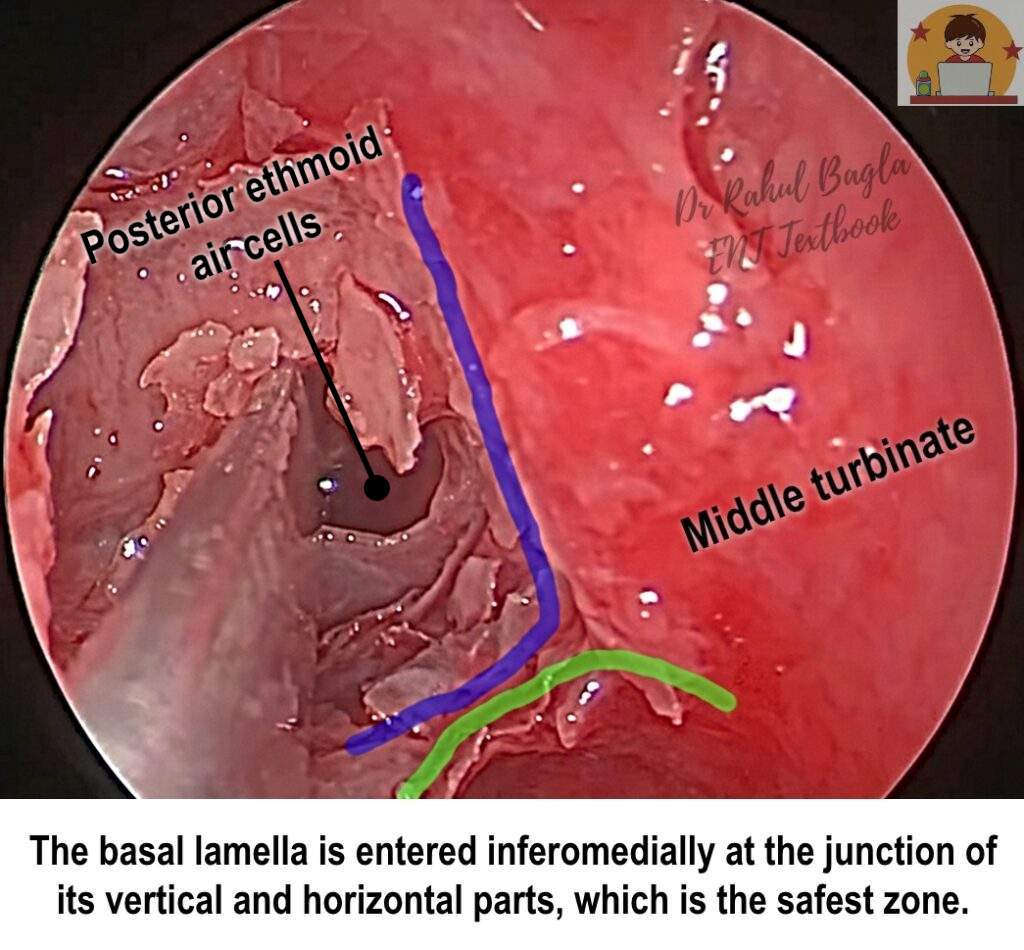
- The basal lamella is entered inferomedially at the junction of its vertical and horizontal parts, which is the safest zone, away from the skull base.
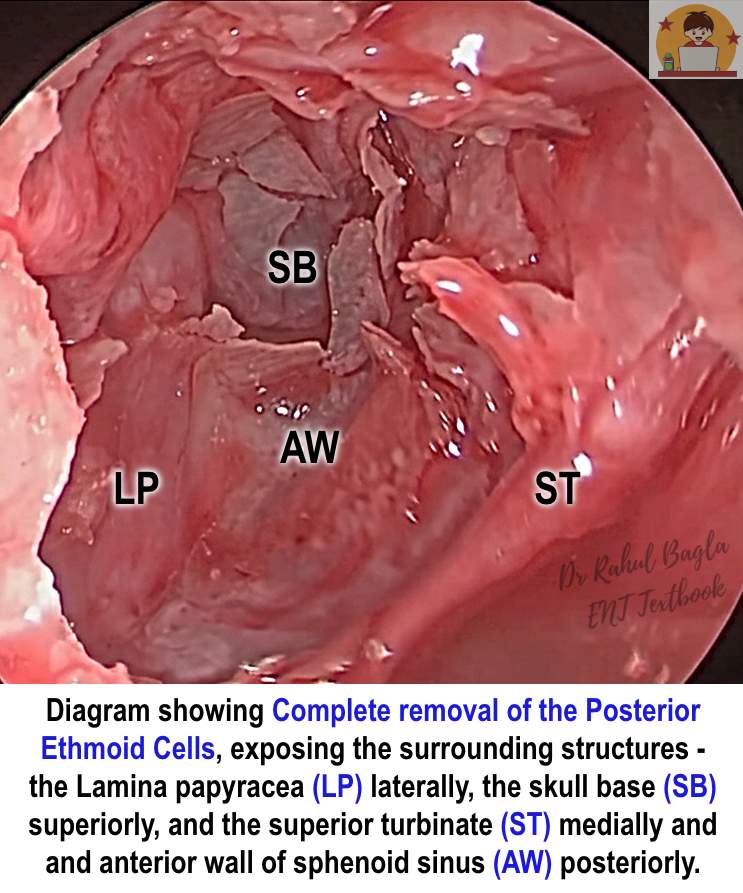
- Remove posterior ethmoid air cells to completely expose: lamina papyracea laterally, skull base (fovea ethmoidalis) superiorly, superior turbinate medially and anterior wall of sphenoid sinus posteriorly.
Step 5: Sphenoidotomy
- The sphenoid sinus lies posterior-most beneath the skull base, typically at the level of the superior turbinate, ~1–1.5 cm above the posterior choana.
- Open the face (anterior wall) of the sphenoid sinus is entered inferomedially. Never enter laterally as the Lateral wall of the sphenoid sinus contains optic nerve and internal carotid artery – injury can be fatal. The lateral wall contains the neurovascular bulges:
- Optic Nerve (ON): Superior and Lateral.
- Internal Carotid Artery (ICA): Inferior and Posterior to the ON.
- An Onodi Cell (spheno-ethmoid cell) is a posterior ethmoid cell that pneumatizes superolaterally over the sphenoid sinus, placing the Optic Nerve directly within its bony septa. Injury here is a risk for blindness.
- The sphenoid is usually opened when there is isolated sphenoid disease (aspergillosis, purulent infections, polyps), mucocele, inverted papilloma, or skull-base access.
- Sphenoidal sinusotomy types:
- I: Identify the sphenoidal ostium only.
- II: Open the inferior half of the sphenoid sinus wall and extend upward to the skull base.
- III: Extend the opening to the floor of the sinus and laterally to vital structures.
Step 6: Frontal Sinus Surgery (If Indicated)
- This is technically the most difficult step due to the narrow, convoluted anatomy of the Frontal Recess and the proximity of the anterior skull base.
- It involves clearing the cells obstructing the recess (e.g., Agger Nasi cells and Frontal Cells). At this point, the surgeon must respect the location of the Anterior Ethmoidal Artery (AEA).
- Remove agger nasi cells and widen the frontal recess.
- Caution: The area is high risk for stenosis and complications such as injury to the anterior ethmoidal artery or skull base breach.
- Evidence suggests only selected cases (e.g., aspirin-sensitive nasal polyposis, recurrent frontal disease) benefit from extensive frontal drainage.
- Frontal recess surgery (if done) increases the risk of stenosis; only perform if indicated.
Step 7: Haemostasis, Nasal Packing, Final Check
- Achieve meticulous haemostasis – check for bleeding from sphenopalatine/ethmoidal arteries, orbital walls, skull base.
- Place nasal packs (absorbable or non-absorbable) as required.
- Final endoscopic inspection to ensure patency of ostia and no significant residual debris.
- Post-operative benefit: FESS improves delivery of topical sprays/irrigations into ethmoid, frontal and sphenoid sinuses. Corticosteroid irrigations reduce polyp recurrence.
Complications of Functional Endoscopic Sinus Surgery (FESS):
Common / Minor Complications
- Nasal bleeding (common).
- Synechiae formation (adhesions between the middle turbinate and lateral wall/ septum).
- Crusting, delayed mucosal healing.
- Middle turbinate lateralisation.
- Nasolacrimal duct injury (esp. near antrostomy/uncinectomy).
Major / Severe Complications
- Orbital injury: hematoma, extra-ocular muscle damage, vision loss.
- Optic nerve injury.
- Internal carotid artery injury (especially during sphenoid surgery).
- CSF leak (cribriform plate injury) → risk of meningitis.
- Skull base breach, intracranial complications.
- Frontal recess stenosis (following frontal sinus surgery).
Table: Complications of FESS
| Structure at Risk | Result of Injury | Management Protocol |
| Anterior Ethmoidal Artery (AEA) | Orbital Haematoma (MC complication requiring urgent intervention). | Immediate Lateral Canthotomy and Inferior Cantholysis to decompress the orbit and save vision. |
| Lamina Papyracea | Orbital Fat Prolapse/Injury → Diplopia. | Careful dissection; repair defects with fascia or bone if large. |
| Cribriform Plate/Fovea Ethmoidalis | CSF Leak → Meningitis. | Endoscopic repair (fat graft, fascia lata) with post-operative lumbar drain if needed. |
| Optic Nerve (ON) | Blindness (Most dreaded complication next to ICA). | Usually related to sphenoid or Onodi cell surgery. Steroids + Decompression. |
| Internal Carotid Artery (ICA) | Massive Haemorrhage/Death (Most dreaded life-threatening complication). | Direct packing/cautery not advised. Angiography → Embolisation → Vessel repair. |
Post-Operative Complications
- Synechiae Formation: Scarring between the Middle Turbinate and the lateral nasal wall or septum.
- Prevention: Proper packing, stenting, and topical use of Mitomycin-C (an anti-fibroblastic agent).
- Recurrence: Especially common in patients with Samter’s Triad (Aspirin-Exacerbated Respiratory Disease – AERD).
Postoperative care of FESS
- Head elevation, monitor bleeding
- Remove nasal pack after 24–48 hours (if non-absorbable)
- Analgesics + antibiotics (5–7 days if required)
- Saline nasal irrigation (most important)
- Intranasal steroids/steroid irrigation
- Regular endoscopic suction cleaning/debridement
- Avoid nose blowing, heavy exertion, sneezing with mouth closed (1–2 weeks)
- Follow-up for synechiae and recurrence
———–End of the Chapter———–
High-Yield Points for Quick Revision
- CBME Focus: FESS aims for physiological restoration, not radical tissue removal.
- First Step: Uncinectomy (Infundibulotomy).
- Safest Technique: Retrograde Uncinectomy with back-biting forceps.
- Posterior Limit: The Basal Lamella separates anterior (draining into the middle meatus) and posterior (draining into the superior meatus) ethmoid cells.
- Most Dangerous Area: The Lateral Wall of the Sphenoid Sinus (housing the ICA and ON). Onodi Cell presence poses a high risk to the Optic Nerve.
- MC Major Complication: Orbital Haematoma (due to AEA injury).
- Life-Saving Intervention: Lateral Canthotomy for orbital compartment syndrome due to haematoma.
- Post-Op Must-Do: Steroid Irrigation reduces polyp recurrence, especially in eosinophilic CRS.
Learning Aids & Mnemonics
The FESS Sequence Mnemonic (For Steps 1-5): Under My Arm Pit Springs
- Uncinectomy
- Maxillary Antrostomy (MMA)
- Anterior Ethmoidectomy
- Posterior Ethmoidectomy
- Sphenoidotomy
Sphenoid Sinus Neurovascular Relation (Crucial for VIVA)
- ON: Out and Nice (Superior and Lateral)
- ICA: In and Central/Close (Inferior and Posterior)
Frequently Asked Questions in Viva
- Q: What is the main aim of FESS, and why is it called “functional”? Ans: The main aim is to restore the natural drainage and ventilation of the paranasal sinuses by opening the Osteomeatal Complex, which allows the sinus mucosa to return to its normal, non-inflamed, functional state.
- Q: What is the significance of the Basal Lamella in FESS? Ans: The Basal Lamella is a crucial surgical landmark that separates the anterior ethmoid air cells from the posterior ethmoid air cells, serving as a landmark before accessing the posterior sinuses and sphenoid sinus.
- Q: How do you manage a massive bleed during sphenoidotomy? Ans: If a massive bleed occurs, the surgeon must pack the area firmly to control the haemorrhage, confirm the injury via angiography, and then proceed with either embolisation or direct vessel repair of the Internal Carotid Artery (ICA).
- Q: What is an Onodi cell, and why is it dangerous? Ans: An Onodi cell is a posterior ethmoid air cell that has pneumatized laterally and superiorly to envelop the Optic Nerve, placing the nerve directly within its bony septa, which increases the risk of blindness during posterior ethmoid or sphenoid surgery.
- Q: What is the “maximal medical therapy” required before FESS? Ans: Maximal medical therapy typically includes a trial of systemic antibiotics (e.g., for 3-4 weeks), prolonged use of topical or systemic corticosteroids, and daily, high-volume saline nasal irrigations, usually for a minimum duration of 12 weeks.
NEET PG / University Exam MCQs
- The primary aim of Functional Endoscopic Sinus Surgery (FESS) is to: A. Remove all visible mucosal disease. B. Radical removal of the turbinates. C. Re-establish patent drainage and ventilation, primarily by clearing the Osteomeatal Complex (OMC). D. Ligation of the Sphenopalatine Artery for epistaxis.
- Which of the following is considered the safest approach for Uncinectomy in FESS? A. Antegrade approach using a sickle knife. B. Retrograde approach using back-biting forceps. C. Dissection with a high-speed drill. D. Removal of the superior part first.
- The most critical surgical landmark separating the anterior from the posterior ethmoid air cells in FESS is the: A. Uncinate Process. B. Ethmoid Bulla. C. Lamina Papyracea. D. Basal (Ground) Lamella.
- The most common major complication following FESS, requiring immediate intervention, is: A. Synechiae formation. B. Cerebrospinal fluid (CSF) leak. C. Orbital Haematoma. D. Blindness due to Optic Nerve injury.
- What is the immediate management protocol for a diagnosed Orbital Haematoma resulting in vision loss after FESS? A. Immediate systemic antibiotics. B. High-dose systemic steroids only. C. Immediate Lateral Canthotomy and Inferior Cantholysis. D. Direct packing of the anterior ethmoidal artery.
- Which neurovascular structure is located superior and lateral to the sphenoid sinus ostium, making the lateral wall the most dangerous area during sphenoidotomy? A. Internal Carotid Artery (ICA). B. Maxillary Artery. C. Optic Nerve (ON). D. Anterior Ethmoidal Artery (AEA).
- Which condition is associated with the highest rate of recurrence of nasal polyps following FESS? A. Sinus Mycetoma. B. Chronic Rhinosinusitis without polyps. C. Samter’s Triad (Aspirin-Exacerbated Respiratory Disease – AERD). D. Isolated Maxillary Sinus Mucocele.
- Which anatomical structure is the anterior limit for a safe Middle Meatal Antrostomy (MMA)? A. Posterior wall of the maxillary sinus. B. Nasolacrimal Duct (NLD). C. Inferior Turbinate head. D. Inferior Meatus.
- In the context of FESS complications, the “Halo Sign” on filter paper is pathognomonic for: A. Orbital Haematoma. B. Internal Carotid Artery injury. C. Cerebrospinal Fluid (CSF) leak. D. Post-operative epistaxis.
- An Onodi cell is a pneumatized air cell that poses a risk to the: A. Maxillary sinus. B. Frontal sinus drainage. C. Optic Nerve. D. Internal Carotid Artery.
Answers and Explanations:
- C. The principle is functional, focusing on restoring the natural drainage pathways, mainly the OMC.
- B. The retrograde approach is safer as the first bite is low, protecting the superior (skull base) and lateral (orbit) vital structures.
- D. The Basal Lamella is the key bony partition; entering it transitions the surgeon from the anterior to the posterior ethmoid system.
- C. Orbital Haematoma, usually from the Anterior Ethmoidal Artery (AEA), is the most common major and urgent complication.
- C. Lateral Canthotomy and Inferior Cantholysis immediately decompress the orbit, preventing Ischaemic Optic Neuropathy and potential permanent vision loss.
- C. The Optic Nerve bulge is superolateral; the ICA bulge is inferoposterior.
- C. Samter’s Triad patients have severe eosinophilic inflammation and notoriously high rates of polyp recurrence, often requiring revision FESS and aspirin desensitisation.
- B. The Nasolacrimal Duct runs vertically in the anterior part of the lateral nasal wall; widening the ostium too far anteriorly risks NLD injury and subsequent epiphora (watery eyes).
- C. The Halo Sign (a clear ring of CSF surrounding a central blood spot) is a classic finding for CSF rhinorrhea.
- C. An Onodi cell (spheno-ethmoid cell) puts the Optic Nerve at direct risk due to its superior and lateral pneumatization over the sphenoid.
Clinical Scenario & Viva Questions
Scenario 1: Acute Post-Operative Vision Loss
A 45-year-old male undergoes FESS for refractory CRS with nasal polyps. One hour post-extubation, he complains of severe orbital pain, is found to have marked unilateral proptosis (bulging eye) and chemosis (swelling of the conjunctiva), and reports complete loss of vision in the operated eye.
- Viva Question 1 (Diagnosis): What is the most likely diagnosis and the structure injured?
- Answer: Orbital Haematoma (Orbital Compartment Syndrome), most commonly due to injury to the Anterior Ethmoidal Artery (AEA).
- Viva Question 2 (Immediate Management): Describe the single most crucial, life-saving step in managing this complication.
- Answer: Immediate Lateral Canthotomy and Inferior Cantholysis to relieve the pressure on the optic nerve and restore vision. This must be done urgently to prevent permanent blindness.
- Viva Question 3 (Presentation): If an examiner asks you to present this case, what is your opening line?
- Answer: “Sir/Ma’am, this is a case of a post-operative ophthalmic complication following FESS, specifically an Orbital Haematoma presenting with acute vision loss, which is a surgical emergency.”
Scenario 2: Persistent Clear Nasal Discharge
Three days post-FESS, a 30-year-old female reports a profuse, clear, watery discharge from her nose that increases when she bends forward. The fluid has a slightly salty or sweet taste.
- Viva Question 1 (Diagnosis): What serious complication should you suspect?
- Answer: Cerebrospinal Fluid (CSF) Leak (CSF Rhinorrhea), likely due to a breach of the Cribriform Plate or Fovea Ethmoidalis during ethmoidectomy.
- Viva Question 2 (Confirmatory Test): What non-invasive clinical test can you perform immediately?
- Answer: The Beta-2 Transferrin Assay is the most specific laboratory test. However, the simple “Halo Sign” test (placing the fluid on filter paper) provides immediate, although less specific, suspicion.
- Viva Question 3 (Management Principles): Briefly outline the steps for managing a persistent CSF leak.
- Answer: Initial management is conservative (bed rest, head elevation, stool softeners). If the leak persists, the definitive treatment is endoscopic repair of the defect using a multilayer closure (e.g., fascia lata graft, mucosal flap) and potentially a post-operative lumbar drain to reduce intracranial pressure.
———–End———–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi)
MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Master FESS with this comprehensive guide for MBBS and ENT PG students. Detailed surgical steps, advanced anatomy (Onodi Cell, AEA), complications, flowcharts, high-yield MCQs, and viva scenarios are included for robust exam preparation. Master FESS (Functional Endoscopic Sinus Surgery) for MBBS, ENT PG, and NEET PG. This CBME-aligned guide covers indications, surgical steps (Uncinectomy, Maxillary Antrostomy), complications, high-yield points, MCQs, and viva questions, Functional endoscopic sinus surgery notes, FESS surgery steps MBBS revision, ENT PG FESS MCQs, what is FESS in sinus surgery, FESS indications and complications MBBS, functional endoscopic sinus surgery summary, FESS CBME syllabus ENT, FESS viva questions and answers, endoscopic sinus surgery revision guide, FESS flowchart and mnemonics, endoscopic sinus surgery indications in India, FESS post-operative care guidelines, FESS nasal polyposis management, FESS high yield points NEET PG. Master FESS (Functional Endoscopic Sinus Surgery) for MBBS, ENT PG, and NEET PG. This CBME-aligned guide covers indications, surgical steps (Uncinectomy, Maxillary Antrostomy), complications, high-yield points, MCQs, and viva question, FESS surgical steps, FESS complications, Functional Endoscopic Sinus Surgery notes, FESS VIVA questions, FESS for NEET PG MCQs, Basal Lamella FESS, Uncinectomy technique, Maxillary antrostomy types, Orbital haematoma management FESS, Sphenoidotomy landmarks, CBME ENT notes FESS, High-yield FESS topics, Anterior ethmoidal artery injury, Mitomycin-C in FESS, OMC anatomy and surgery, Functional vs Structural Sinus Surgery, FESS summary and mnemonics, Endoscopic sinus surgery guide. Functional Endoscopic Sinus Surgery notes, FESS surgery steps, FESS indications, FESS complications, FESS procedure pdf, FESS in ENT viva questions, FESS NEET PG MCQs, Functional endoscopic sinus surgery summary, Osteomeatal complex anatomy, FESS for chronic rhinosinusitis, FESS mnemonic, FESS complications table, Postoperative care after FESS, FESS stepwise procedure, FESS surgical anatomy, Functional endoscopic sinus surgery explained, FESS ENT exam guide, FESS MCQs with answers, FESS flowchart, FESS surgery viva preparation.
thank you for detaled informations
Thanks
Very nice. Easy steps of surgery. Thank you so much sir
Thanks
Very nice.helpful.
Thanks
Very nice alot of thanks
Thanks