Direct Laryngoscopy (DL)
Direct Laryngoscopy (DL) is a core ENT procedure. It gives a direct, clear, magnified view of the larynx and hypopharynx and allows the surgeon to use both hands. DL helps visualise areas that cannot be seen (hidden areas of the larynx) with Indirect Laryngoscopy (IDL) or flexible nasopharyngolaryngoscopy. Because the procedure requires stability and precision, it is usually done under general anaesthesia in the operating room. This controlled environment allows accurate diagnosis and also enables therapeutic procedures during the same sitting. DL is commonly performed as part of a full pan-endoscopy along with esophagoscopy and bronchoscopy, especially during cancer evaluation.

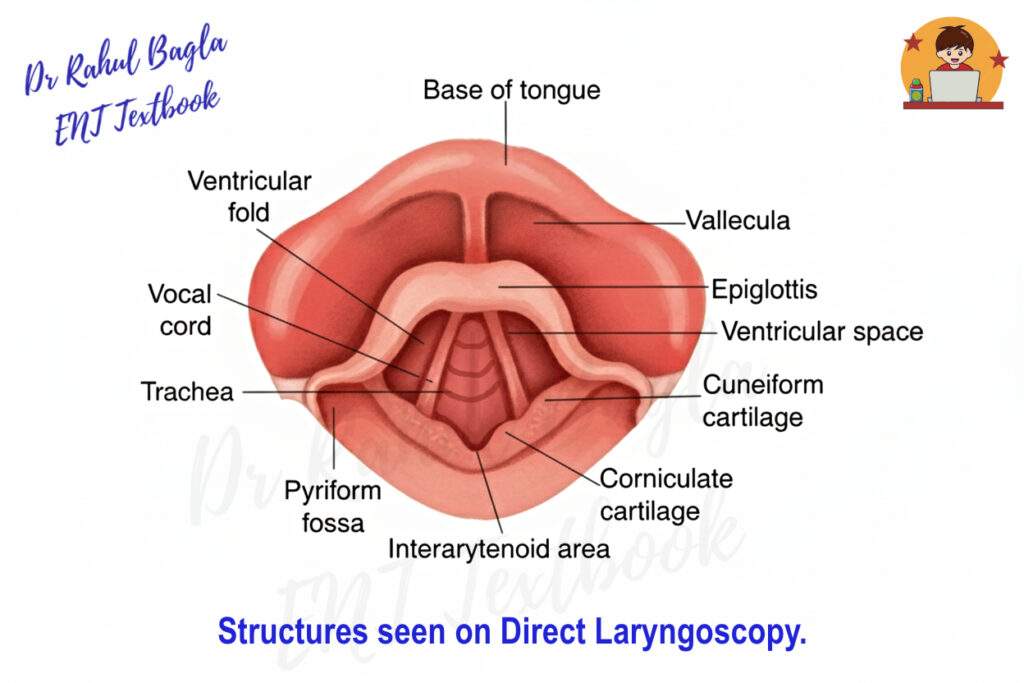
Table: Differences between Direct Laryngoscopy (DL) & Indirect Laryngoscopy (IDL)
| Feature | Direct Laryngoscopy (DL) | Indirect Laryngoscopy (IDL) |
| Age Suitability | All ages, essential in infants/children | Cooperative adults only |
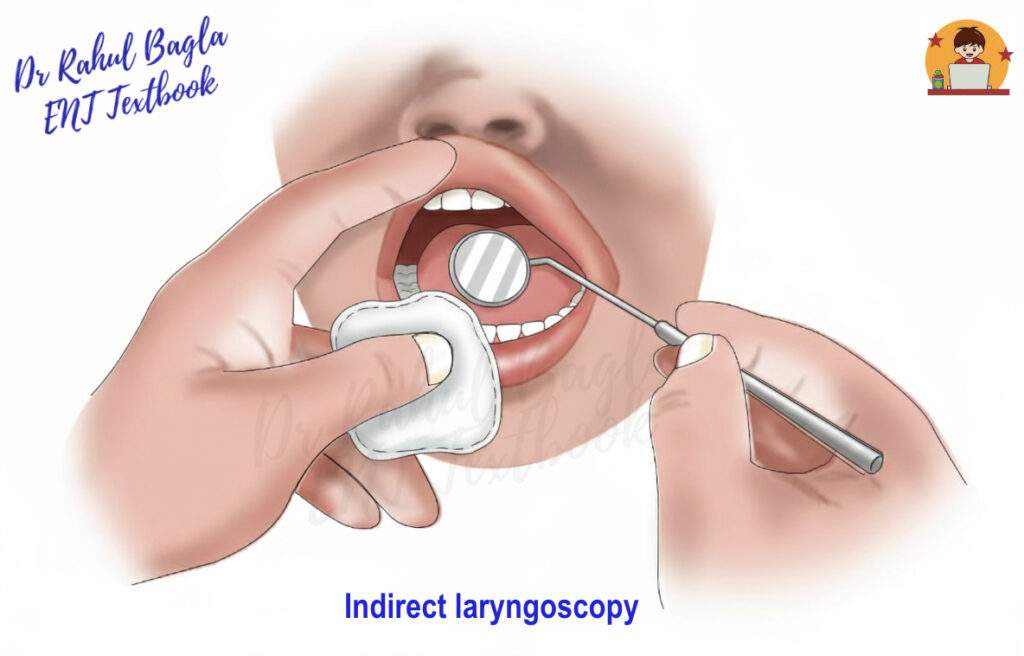
| View | Direct, magnified, bimanual | Indirect (mirror), monocular |
| Anaesthesia | Usually general | Topical/None |
| Setting | Operating theatre | Outpatient clinic |
| Visualization | Full larynx and hypopharynx, including hidden areas (ventricles, subglottis, anterior commissure) | Limited; depends on patient cooperation and anatomy |
| Therapeutic Use | Yes (biopsy, MLS, foreign body removal) | No; mainly diagnostic |
Indications of Direct Laryngoscopy
Diagnostic Indications
- Biopsy of Growth and Staging of Malignancy: To find an accurate assessment of the extent of the growth and to take a biopsy for histopathological diagnosis.
- Evaluation of ‘Hidden Areas’:
- Larynx: Anterior commissure (common site for early glottic cancer), laryngeal ventricles, infrahyoid epiglottis, and the subglottic region.
- Hypopharynx: Base of tongue, vallecula, and the entire pyriform fossa.
- Failed or Incomplete Indirect Laryngoscopy (IDL): IDL may not provide a proper view due to factors such as excessive gag reflex, a large overhanging epiglottis, trismus, or anatomical variations. In infants and young children, IDL is generally not possible. Any child with hoarseness, stridor, breathing difficulty, or swallowing problems should be assessed further. Flexible laryngoscopy is preferred for initial evaluation, and DL is performed when a more detailed examination or intervention is required.
Therapeutic Indications
- Microlaryngeal Surgery (MLS): This is the most common therapeutic use, involving the removal of benign lesions of the larynx, like vocal nodules, polyps, cysts, and recurrent respiratory papillomatosis (RRP) under microscopic control.
- Foreign Body (FB) Removal from larynx and hypopharynx.
- Management of Laryngeal Stenosis: DL is used for dilatation of laryngeal or subglottic strictures, typically followed by steroid injection or laser treatment.
- Laser Surgery: For excision of early laryngeal cancers or complex benign lesions using CO2 laser.
Contraindications to Direct Laryngoscopy
- Complete supraglottic or glottic obstruction. DL cannot be done when the airway is fully blocked, as introducing the scope may worsen the obstruction.
- Cervical spondylosis or cervical spine ankylosis. DL requires neck extension (“barking-dog position”). This is unsafe in cervical spine disease or injury because it can cause neurological damage, including quadriplegia.
- Penetrating trauma to the upper airway. Instrumentation may worsen bleeding, introduce infection, or disrupt injured structures.
- Trismus (TMJ ankylosis, OSMF). The mouth cannot open enough to insert the rigid laryngoscope.
- Aortic aneurysm. Instrumentation can trigger a hypertensive response and risk aneurysm rupture.
- Micrognathia or macroglossia. Visualisation becomes extremely difficult, increasing the risk of oral and dental trauma.
- Recent myocardial infarction. Stress and sympathetic stimulation during DL may provoke another cardiac event.
- Severe cardiac decompensation. The patient may not tolerate anaesthesia or procedural stress. DL can be done only after stabilising the cardiac condition.
Equipment
- Rigid Laryngoscopes: Available in different sizes; the Kleinsasser laryngoscope is most commonly used.
- Camera and monitor (preferred): A high-resolution camera attached to the laryngoscope allows the procedure to be viewed on a monitor. This provides better visualisation, helps the surgical team follow the procedure, and enables documentation and teaching.
- Operating Microscope: A 400-mm lens microscope provides high magnification and binocular vision during Microlaryngeal Surgery (MLS).
- Light Source: Fibre-optic cable with a strong external light source provides bright, cool illumination.
- Suspension Laryngoscope Holder: A chest-supported holder (Lewy or Holinger type) keeps the laryngoscope steady and frees both hands for surgery.
- Dental Guard/Protector: Foam, gauze, or plastic guard are used to prevent iatrogenic injury to the upper incisors, which act as a fulcrum during lifting.
- Instrumentation: Suction apparatus (essential), 70° telescopes for viewing the subglottis and undersurface of the cords, long, fine microsurgical instruments (forceps, scissors), and biopsy instruments.
Anaesthesia
- General anaesthesia with muscle relaxation and endotracheal intubation is the standard for DL.
- Local anaesthesia with heavy sedation may be used for short diagnostic procedures in uncooperative adults.
- Neonates and infants: Diagnostic DL may sometimes be performed without anaesthesia.
Position (Sniffing, Barking-Dog, Sword Swallowing Position)
The patient lies supine. A 10–15 cm head ring is placed under the head to flex the neck on the chest. The head is then extended at the atlanto-occipital joint. This alignment straightens the oral, pharyngeal, and laryngeal axis to provide a clear, direct view during DL.
Steps of Direct Laryngoscopy
- Pre-operative Checks: Ensure the patient is in the sniffing position and the dental protector is in place.
- Introduction of the laryngoscope: The surgeon holds the laryngoscope in the left hand. The scope is introduced from the right corner of the mouth, pushing the tongue to the left side. This approach avoids the bulk of the tongue initially.
- Visualisation of the Epiglottis: The tip of the laryngoscope is gently advanced along the groove between the tongue and the alveolar ridge until the epiglottis comes into view.
- Elevation of Epiglottis: The tip of the laryngoscope is advanced into the vallecula (the space between the base of the tongue and the epiglottis) is lifted upwards and forwards along the axis of the handle, without levering on the teeth. This upward lift pulls the tongue-epiglottis complex forward, exposing the glottis.
- Serial Examination: Once the glottis is visible, a methodical examination is performed:
- Hypopharynx: Base of tongue, vallecula, bilateral pyriform fossae, and post-cricoid region.
- Larynx: Epiglottis (lingual and laryngeal surfaces), aryepiglottic folds, arytenoids, postcricoid region, false cords, true vocal cords (mobility assessment), anterior commissure, and ventricles.
- Subglottis: Often requires an angled 70-degree telescope or a specialised scope (e.g., anterior commissure laryngoscope) to visualise below the cords.
- Biopsy/Procedure: If a lesion is identified, the biopsy is taken using appropriate instruments, taking care to achieve adequate depth.
- Withdrawal: The laryngoscope is withdrawn slowly and carefully, examining the lips, teeth, and tongue for any signs of injury.
Postoperative Care of Direct Laryngoscopy
- Airway and positioning. Place the patient in the lateral (“coma”) position to prevent aspiration of blood or secretions.
- Observation. Monitor closely for laryngeal oedema, especially after long or traumatic procedures. Warning signs include stridor and breathing difficulty.
- Oral care. Advise cold liquids or ice chips to reduce throat discomfort and swelling. Prescribe analgesics as needed.
Complications of Direct Laryngoscopy
- Laryngeal oedema. May cause respiratory distress; treat with IV steroids, nebulization, and rarely emergency tracheostomy.
- Dental injury. The most common complication ranges from contusions to fractured or dislodged teeth. Prevent with a dental guard.
- Lip/tongue injury. Occurs when soft tissue gets caught between the laryngoscope and teeth.
- Bleeding. Usually mild but can be significant after extensive biopsies.
- Cardiac events. MI or arrhythmias due to sympathetic stimulation during the procedure.
- Aspiration. Occurs in the immediate postoperative period due to blood or secretions.
———–End of the Chapter ———–
High-Yield Points for Quick Revision
- Position: Sniffing Position (Flexion of neck, Extension of head).
- Gold Standard: DL is the gold standard for assessing the subglottis and the anterior commissure (Laryngeal blind areas).
- Laryngoscope Handling: Always hold the scope in the left hand.
- Fulcrum: The upper incisor teeth act as the fulcrum; the dental guard protects them.
- Lifting: Lift upwards and forwards along the axis of the handle; never lever on the teeth.
- Therapeutic Gold Standard: Microlaryngeal Surgery (MLS) is the most frequent therapeutic application.
- Most Common Complication: Dental Injury.
- Life-Threatening Complication: Laryngeal Oedema (Monitor for stridor).
- Best View for Subglottis: 70° Telescope used through the laryngoscope.
- Contraindication: Cervical Spondylosis (Risk of quadriplegia from extension).
Frequently Asked Questions in Viva
- What is the primary difference between Direct and Indirect Laryngoscopy? Direct Laryngoscopy (DL) provides a magnified, bimanual, and full view under general anaesthesia for diagnostic and therapeutic purposes, while Indirect Laryngoscopy (IDL) provides an indirect, monocular, limited view using a mirror or flexible scope, primarily for diagnosis in an outpatient setting.
- What is the ‘Sniffing Position’ in Direct Laryngoscopy? The Sniffing Position, achieved by flexing the patient’s neck on the chest and extending the head at the atlanto-occipital joint, is crucial because it aligns the oral, pharyngeal, and laryngeal axes into a straight line for a clear view.
- Which dental structure must be protected during Direct Laryngoscopy? The upper incisor teeth must be protected using a dental guard because they act as the fulcrum for the laryngoscope during the necessary upward and forward lift to expose the glottis.
- What are the two most important ‘blind areas’ of the larynx seen by DL but missed by Indirect Laryngoscopy (IDL)? The two most important ‘blind areas’ are the anterior commissure (the junction of the vocal cords anteriorly) and the subglottic region (the area immediately below the vocal cords).
- Why is Direct Laryngoscopy contraindicated in severe cervical spondylosis? Severe cervical spondylosis is a contraindication because the mandatory neck extension required for the procedure risks causing acute spinal cord injury or neurological damage, including quadriplegia.
- What is the most common therapeutic use of Direct Laryngoscopy? The most common therapeutic use of Direct Laryngoscopy is Microlaryngeal Surgery (MLS), which involves the removal or treatment of benign and early malignant laryngeal lesions under microscopic magnification.
- Which instrument is used to visualise the subglottis during Direct Laryngoscopy? A 70-degree angled telescope, passed through the barrel of the rigid laryngoscope, is used to effectively visualize the subglottic region and the undersurface of the vocal cords, which are otherwise poorly seen.
NEET PG-Style Multiple Choice Questions (MCQs)
- The single most common complication of Direct Laryngoscopy is: A) Laryngeal oedema B) Aspiration pneumonia C) Dental injury D) Cardiac arrhythmia
- The anatomical position required for a clear view during Direct Laryngoscopy is best described as: A) Trendelenburg position B) Rose position C) Sniffing position D) Prone position with neck flexion
- The primary reason for a contraindication to Direct Laryngoscopy in a patient with severe cervical spine ankylosis is: A) Increased risk of aspiration B) Inability to pass the endotracheal tube C) Risk of spinal cord injury and quadriplegia D) Inability to achieve adequate muscle relaxation
- A 70-degree angled telescope is primarily used during Direct Laryngoscopy to visualize the: A) Anterior commissure B) Vocal cord mobility C) Base of tongue D) Subglottic region and undersurface of cords
- Which of the following is NOT typically considered one of the ‘hidden areas’ that necessitates Direct Laryngoscopy for complete evaluation? A) Laryngeal ventricle B) Anterior commissure C) Apex of the pyriform fossa D) Posterior wall of the oropharynx
- The instrument used to maintain the laryngoscope position and free the surgeon’s hands during Microlaryngeal Surgery is the: A) Negus esophagoscope B) Holinger suspension holder C) Jackson bronchoscope D) Boyle-Davis mouth gag
- While performing Direct Laryngoscopy, the upward and forward lifting force should be applied along the axis of the handle to avoid levering on the teeth. Which of the following acts as the fulcrum in this procedure? A) Mandibular incisors B) Maxillary molars C) Thyroid cartilage D) Maxillary incisors
- Direct Laryngoscopy is most commonly combined with which procedure as part of a pan-endoscopy for cancer workup? A) Tonsillectomy and Adenoidectomy B) Esophagoscopy and Bronchoscopy C) Tracheostomy and Neck Dissection D) Maxillectomy and Laryngectomy
- In a patient who develops inspiratory stridor immediately post-Direct Laryngoscopy, the most likely immediate cause is: A) Aspiration of gastric contents B) Laryngeal oedema C) Vocal cord paralysis D) Post-operative epistaxis
- Which of the following is the most frequent therapeutic application of Direct Laryngoscopy? A) Laser ablation of laryngeal stenosis B) Removal of cricopharyngeal bar C) Foreign body retrieval from the bronchus D) Microlaryngeal Surgery (MLS) for benign vocal cord lesions
Answers and Explanations
- C) Dental injury. This is the most frequently reported complication due to the rigid scope using the teeth as a fulcrum. Proper use of a dental guard is key to prevention.
- C) Sniffing position. This specific combination of neck flexion and head extension (atlanto-occipital extension) aligns the axes for a direct view.
- C) Risk of spinal cord injury and quadriplegia. The mandatory hyperextension of the head/neck is unsafe in pre-existing cervical spine disease.
- D) Subglottic region and undersurface of cords. The 70° scope allows the surgeon to look ‘around the corner’ below the true vocal cords, which is difficult with the rigid straight laryngoscope.
- D) Posterior wall of the oropharynx. The oropharynx is typically well-visualised with IDL or flexible laryngoscopy; the other three are the classic ‘hidden areas’ of the larynx/hypopharynx.
- B) Holinger suspension holder. This holder is designed to keep the laryngoscope steady and suspended, freeing both the surgeon’s hands for bimanual MLS.
- D) Maxillary incisors. The upper (maxillary) incisor teeth are the structures that most commonly bear the lifting force and, thus, must be protected by the dental guard.
- B) Esophagoscopy and Bronchoscopy. This trio is the standard definition of a pan-endoscopy, performed for synchronous primary tumours, especially during the workup of a squamous cell carcinoma.
- B) Laryngeal oedema. Stridor is the clinical sign of upper airway obstruction; after DL, this is most commonly caused by trauma-induced laryngeal or subglottic swelling/oedema.
- D) Microlaryngeal Surgery (MLS) for benign vocal cord lesions. While laser surgery and FB removal are therapeutic, MLS (removal of nodules, polyps, cysts) constitutes the bulk of therapeutic DL cases.
Clinical Case Scenarios (Viva & Practical Prep)
- Case: The Voice Coach A 45-year-old female voice coach presents with 6 months of persistent hoarseness. IDL shows a small, smooth, bilateral swelling at the junction of the anterior one-third and posterior two-thirds of the vocal cords. Her gag reflex is hyperactive.
-
- Viva Question 1: What is the most likely diagnosis, and what is the definitive procedure for both diagnosis and treatment?
- Viva Answer: Vocal Nodules. The definitive procedure is Direct Laryngoscopy (DL) with Microlaryngeal Surgery (MLS) for precise, atraumatic excision and histopathological confirmation.
- Case: The Smoking Male A 68-year-old male with a 40-pack-year smoking history presents with progressive hoarseness and mild pain on swallowing for 3 months. Flexible nasopharyngolaryngoscopy reveals a growth on the right true vocal cord, but the extent of subglottic involvement is unclear.
-
- Viva Question 2: Why is Direct Laryngoscopy mandatory here, and what is a crucial piece of equipment you would need in addition to the standard laryngoscope?
- Viva Answer: DL is mandatory for biopsy (to confirm malignancy) and accurate staging (to determine the true extent of the tumour, especially the hidden subglottis). The crucial additional equipment is a 70-degree angled telescope to visualize the subglottis.
- Case: The RTA Victim A 28-year-old male involved in a Road Traffic Accident (RTA) sustained a maxillofacial injury and has a known C5-C6 cervical spine fracture, immobilized in a neck collar. He has increasing stridor. An urgent airway procedure is required.
-
- Viva Question 3: Would you perform Direct Laryngoscopy or an emergency tracheostomy? Justify your choice based on the key contraindication.
- Viva Answer: An emergency tracheostomy is the safer choice. Direct Laryngoscopy is strongly contraindicated due to the unstable cervical spine fracture. The mandatory hyperextension/positioning risks transecting the spinal cord, leading to catastrophic neurological damage (quadriplegia).
———–End———–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Master Direct Laryngoscopy! Essential ENT notes for MBBS/PG. Indications, steps, viva Q&A, and high-yield MCQs aligned with the CBME curriculum, This comprehensive guide on Direct Laryngoscopy (DL) is meticulously structured for MBBS and ENT PG students, aligning perfectly with the CBME curriculum. We aim to provide a high-yield, standalone resource covering all aspects necessary for university theory exams, viva’s, practical’s, and NEET PG MCQs. Therefore, we focus on conceptual clarity, easy-to-recall mnemonics, and clinical relevance, Direct Laryngoscopy procedure steps and indications, Direct Laryngoscopy complications and contraindications, Direct Laryngoscopy viva questions for ENT PG, NEET PG MCQs on Direct Laryngoscopy, What is Direct Laryngoscopy, Direct Laryngoscopy CBME curriculum notes, Sniffing position Direct Laryngoscopy, Microlaryngeal surgery procedure guide, Laryngeal foreign body removal steps, DL vs IDL comparison table, Direct Laryngoscopy high-yield revision, ENT notes Direct Laryngoscopy PDF, Direct Laryngoscopy exam guide, Direct Laryngoscopy steps, Direct Laryngoscopy indications, Direct Laryngoscopy complications, DL for MBBS students, Direct Laryngoscopy procedure video, Direct Laryngoscopy viva questions, Direct Laryngoscopy CBME, Direct Laryngoscopy NEET PG notes, Direct Laryngoscopy vs Indirect Laryngoscopy table, Microlaryngeal Surgery procedure, Sniffing position laryngoscopy, Laryngeal oedema after DL management, vocal cord biopsy procedure.