Cortical Mastoidectomy
Cortical mastoidectomy (CM), also known as Schwartz mastoidectomy or simple mastoidectomy, involves the complete surgical removal of infected air cells within the mastoid bone. It’s an essential first step in many complex middle ear and skull base surgeries. The procedure aims to eradicate disease while preserving the posterior meatal wall and middle ear structures, including the tympanic membrane and ossicles. Consequently, hearing is often maintained or even improved.
Indications for Cortical Mastoidectomy
- Acute coalescent mastoiditis. When the patient does not respond to antibiotics. Presence of intracranial complications. Development of abscesses (e.g. Postauricular abscess, Bezold’s abscess, Zygomatic abscess)
- Masked mastoiditis. Chronic, silent form of mastoiditis that presents late.
- Tubercular mastoiditis.
- Prior to Other Surgeries: It serves as the initial step for various transmastoid approaches, including:
- Cochlear implantation
- Facial nerve decompression
- Endolymphatic sac decompression
- Translabyrinthine or retrolabyrinthine approaches to the internal auditory meatus and cerebellopontine angle.
Contraindications
There are no absolute contraindications for cortical mastoidectomy, especially when it’s a life-saving procedure. However, a surgeon may delay or modify the surgery if the patient has uncontrolled systemic diseases, which can increase anaesthetic and surgical risks.
Surgical Technique: Step-by-Step Procedure
1. Patient Positioning and Anaesthesia. The patient lies in a supine position with their head turned to the opposite side. This arrangement allows for a clear view of the mastoid process. The foot of the table is often lowered by about 20 degrees, which helps to reduce the intraoperative bleeding and orient the plane of the middle fossa dura vertically, thereby reducing the risk of injury. While local anaesthesia can be used in some cases, general anaesthesia is the standard for this procedure.
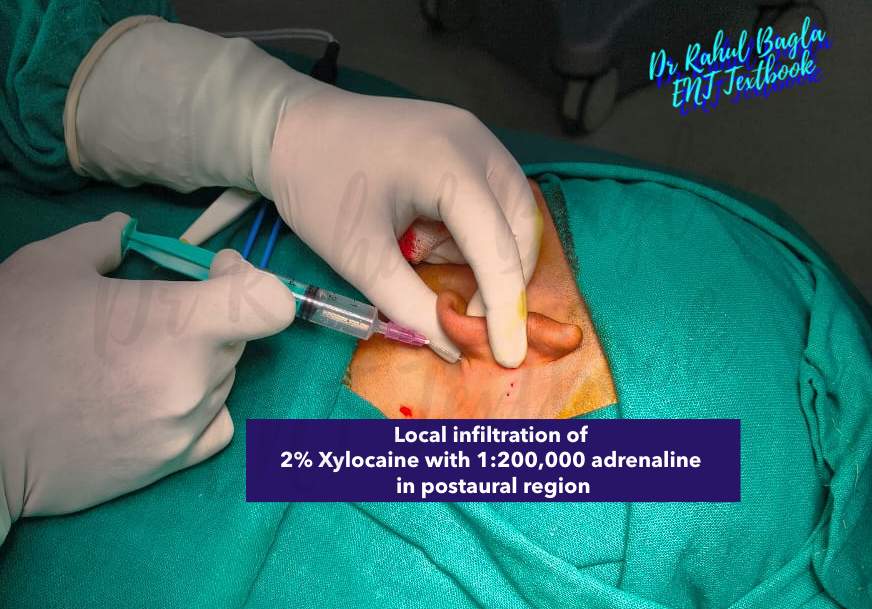
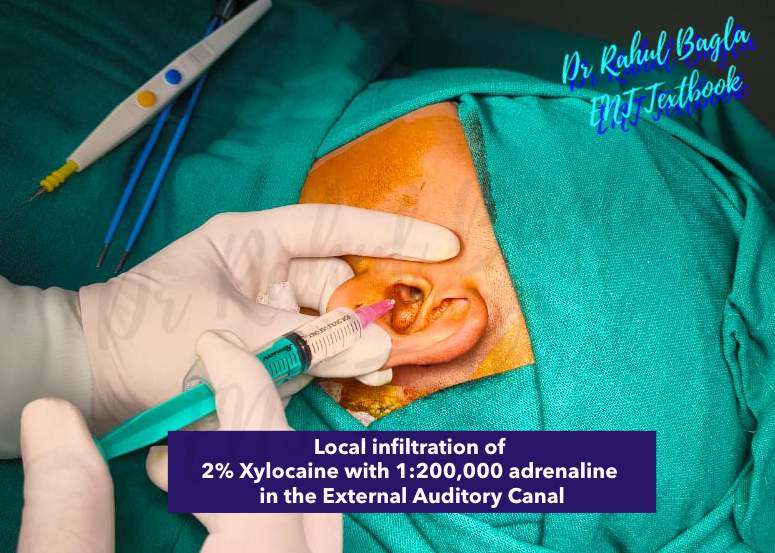
2. Local Infiltration for Haemostasis and Anaesthesia. Following general anaesthesia, local anaesthesia is given in the postaural region and into the external auditory canal. We typically inject a solution of 2% Xylocaine with 1:200,000 adrenaline. This not only provides prolonged pain relief but also causes vasoconstriction, minimising blood loss. We specifically target several key nerves:
- Greater auricular nerve: Located behind the auricle, it supplies the skin of the auricle and external auditory meatus.
- Auriculotemporal nerve: Supplies the anterior wall of the external auditory meatus and the upper part of the auricle.
- Auricular branch of the vagus nerve: Supplies the posterior wall and floor of the external auditory meatus.
3. Incisions: Postauricular vs. Endaural. Surgeons use one of two primary incisions to access the mastoid bone.
- Postauricular Incision (Wilde’s Incision): This is the most common and preferred incision for mastoid access. It provides the best exposure, particularly in well-pneumatized mastoids. The incision is made about 8-10 mm behind the postauricular crease. It heals rapidly and leaves a cosmetically acceptable scar. For children under two, the incision is placed more horizontally, just above the auricle, to access the more superiorly located mastoid antrum. This also avoids injury to the facial nerve, which is superficial in the lower part of the mastoid. When placed more posteriorly, it provides wider exposure necessary for translabyrinthine, retrolabyrinthine, and retrosigmoid approaches to the CP angle.
- Endaural Incision (Lempert’s Incision): This incision is less common and is mainly used for temporal bones with limited pneumatization. While it offers a more limited exposure, it can be useful for specific cases. (Read more)
4. Flap Elevation. Incision cuts through the subcutaneous tissue and muscle. We then incise the periosteum in a T-, Y-, or U-shape and elevate it with a Farabeuf’s periosteal elevator or Freer’s elevator. A self-retaining mastoid retractor is applied to expose the underlying mastoid bone.
5. Identifying Anatomical Landmarks. Once the bone is exposed, we identify critical surface landmarks:
- Spine of Henle: A small projection at the superoposterior margin of the external auditory meatus.
- MacEwen’s Triangle (Suprameatal Triangle): A triangular depression posterosuperior to the meatus, which serves as a key surgical landmark. The mastoid antrum lies 12–15 mm deep to the outer mastoid cortex in adults.
- Posterior bony margin of the external auditory meatus.
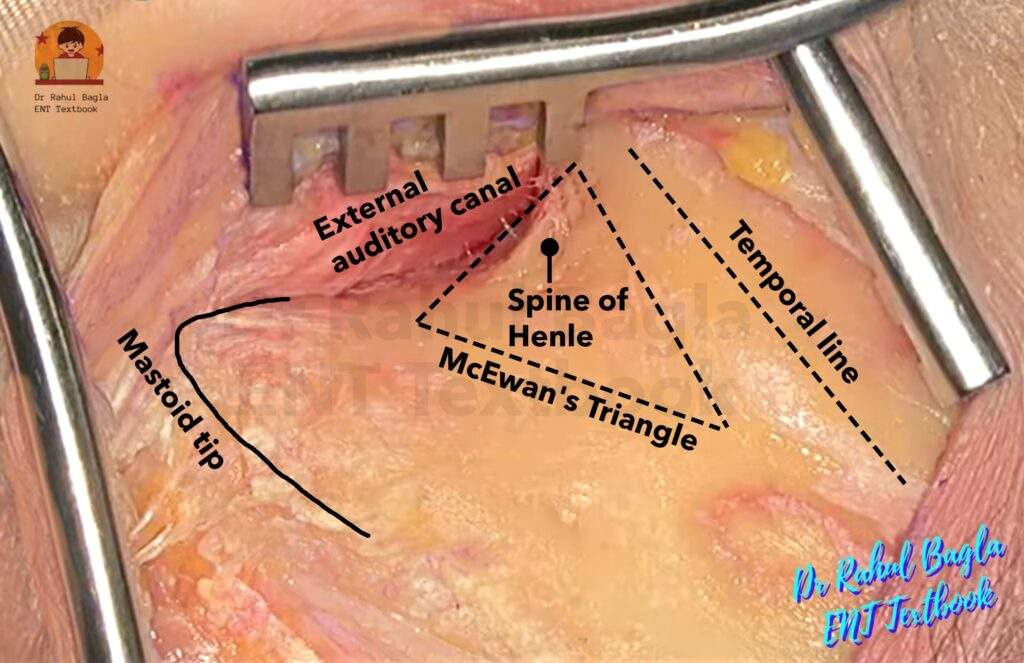
6. Opening the Mastoid Cortex. Using a large cutting burr, we carefully drill away the mastoid’s outer layer, or cortex, focusing on the area within Macewen’s triangle. This is your entry point to find the mastoid antrum, which lies about 12-15 cm deep in adults. To start, you’ll drill a precise outline for the mastoidectomy. Begin by following the temporal line, then curve downward along the external auditory canal towards the mastoid tip. Finally, connect the mastoid tip back to the temporal line along the anticipated path of the sigmoid sinus.
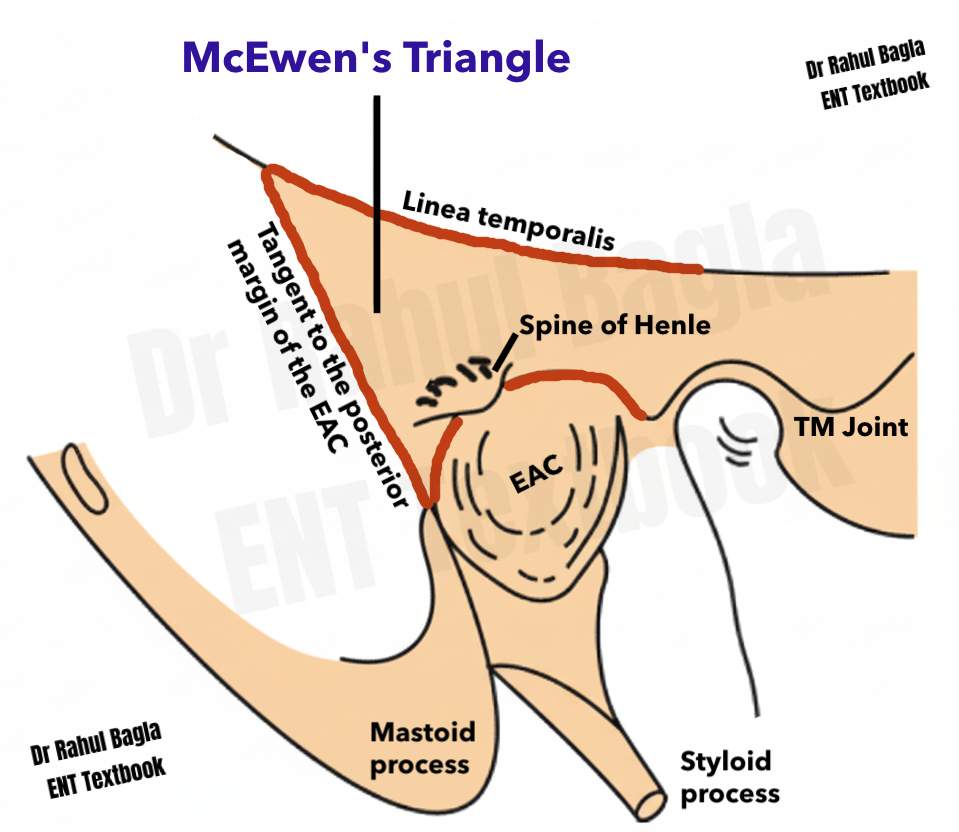
Boundaries of MacEwen’s Triangle (Suprameatal Triangle)
- Superiorly: The linea temporalis (temporal line), a ridge of bone extending posteriorly from the zygomatic process, which marks the lower border of the temporalis muscle and approximates the floor of the middle cranial fossa.
- Anteriorly: The posterosuperior margin of the external auditory canal (EAC) along with the suprameatal spine of Henle.
- Posteriorly: A vertical line drawn tangent to the posterior margin of the EAC.
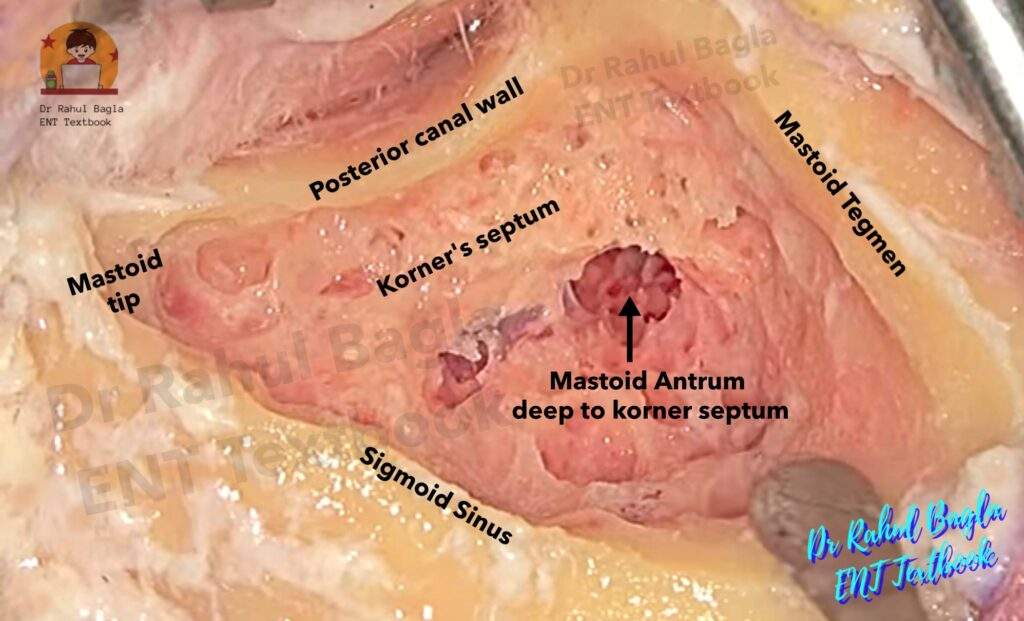
7. Finding the Mastoid Antrum. The antrum is located superiorly and posteriorly to the external auditory meatus. The mastoid antrum is the largest and most consistent mastoid air cell. In a sclerosed mastoid, the antrum may appear contracted. In a sclerosed mastoid, surgeons must identify the dural and sinus plates before locating the mastoid antrum to avoid injury to the horizontal semicircular canal and facial nerve. Korner’s septum is a bony plate, which appears as a whitish-blue, hard bone ridge, that may create a shallow false cavity mimicking the antrum, while the true antrum lies below it. The true antrum has proper depth (same as the middle ear) and communicates with the aditus, whereas the false antrum does not.
The surgeon must constantly be aware of the “three dangers”:
- Low-lying dura: The middle fossa dura can descend, placing it in the path of the burr. Normally, dural plate appears as a pink coloured thin plate of bone.
- Forward-lying sigmoid sinus: The sigmoid sinus can be very close to the entry point of the mastoid. The sigmoid sinus is clearly identified by its bluish colour.
- Facial nerve: The facial nerve is at risk, particularly in the medial and anterior aspects of the dissection.
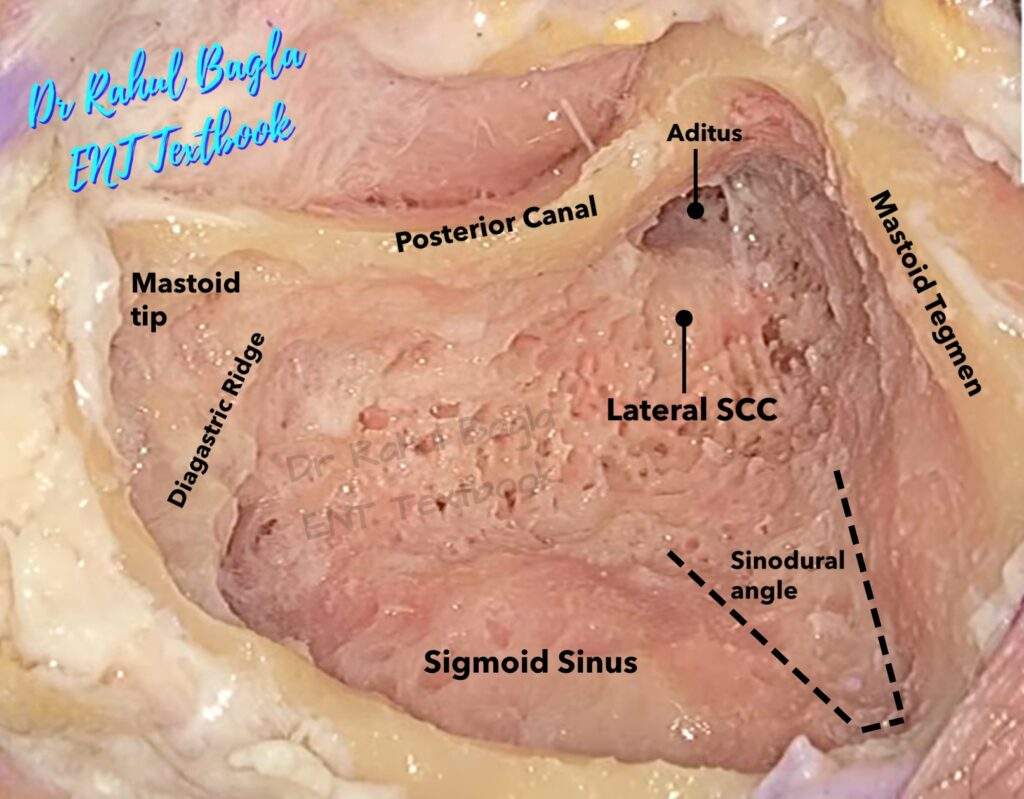
8. Identification of the Horizontal (lateral) Semicircular Canal.
9. Checking patency to the attic. It is essential to widen the aditus for proper drainage and ventilation of the mastoid cavity, taking care not to dislocate the incus during the process. Patency to the attic is confirmed by saline irrigation or gently probing anteriorly with a Dundas Grant probe or cell seeker, which will slip into the aditus.
10. Mastoidectomy Proper (Removing Air Cells). Once the antrum is located, we systematically follow the air cell tracts to their termination using a burr. The goal is to exenterate all diseased cells in all directions:
- Inferiorly: We follow the vertical tract down to the mastoid tip, taking care to avoid the facial nerve, which lies at the anterior end of the digastric ridge.
- Posteriorly: We follow the cells toward the sigmoid sinus, defining the sinus plate.
- Superiorly: We clean the cells toward the tegmen mastoideum (the roof), defining the tegmen plate.
- Anteriorly: We remove cells extending into the root of the zygomatic process.
11. Confirmation and Closure. The procedure is complete when all cell tracts have been exenterated and the key landmarks—the tegmen plate, sigmoid sinus plate, and the horizontal semicircular canal—are clearly defined. The final cavity has a smooth transition between the tegmen plate, sinus plate, and the dura of the posterior fossa, also known as Trautmann’s triangle. A finished cavity should have bevelled edges so that soft tissue can easily sit in and obliterate the cavity.
12. Wound Closure. The wound is then irrigated with saline to remove bone dust. The wound is closed in two layers. A rubber drain may be left at the lower end of the incision for 24–48 h in case of infection or excessive bleeding. A meatal pack should be kept to avoid stenosis of the ear canal. Mastoid dressing is applied.
Postoperative care
- Antibiotics started preoperatively are continued postoperatively for at least 1 week. A culture swab taken from the mastoid during the operation may dictate a change in the antibiotic.
- Drain, if put, is removed in 24–48 h, and a sterile dressing is done.
- Stitches are removed on the sixth day.
Complications:
Intraoperative Complications
- Facial Nerve Injury: The most feared complication. The facial nerve (vertical part) runs through the mastoid bone, and it can be injured by the heat from the burr (thermal injury) or direct trauma. Using constant saline irrigation and suction during drilling is a key preventive measure.
- Sigmoid Sinus Injury: Injury to the sigmoid sinus or other venous structures can cause profuse bleeding. This can be controlled with pressure, packing, or bone wax. In rare cases, it can lead to a dangerous air embolism.
- Dural Injury: The tegmen mastoideum separates the mastoid from the middle and posterior cranial fossae. Damage to the dura can lead to a cerebrospinal fluid (CSF) leak, increasing the risk of meningitis.
- Injury to the horizontal semicircular canal. Patient will have postoperative giddiness and nystagmus.
- Dislocation of the incus. Dislocation or removal of the incus results in severe, permanent conductive hearing loss.
Postoperative Complications
- Persistent Ear Discharge
- Infection or Hematoma: Poor surgical technique or a difficult case can lead to a postoperative wound infection or hematoma, which can delay healing.
- Conductive Hearing Loss: This can occur if the ossicles (especially the incus) are accidentally dislocated or removed during the procedure.
- High-Tone Hearing Loss: The drilling process can sometimes cause a temporary or permanent high-tone hearing loss, particularly in the 4-8 kHz range, due to acoustic trauma.
——– End of the chapter ——–
High-Yield Points for NEET PG and University Exams
Here are some high-yield facts you must remember for your exams.
- Schwartz mastoidectomy and Simple mastoidectomy are synonyms for cortical mastoidectomy.
- The procedure is conservative because it preserves the posterior and superior bony ear canal wall.
- Macewen’s triangle is the key surface landmark for the mastoid antrum.
- The mastoid antrum is the only constant air cell in the mastoid bone and is a crucial anatomical landmark.
- The horizontal semicircular canal is the most reliable internal landmark for the facial nerve. Remember that the nerve is located just anterior and medial to this structure.
- Korner’s septum is a common anatomical variation that can mislead a surgeon into creating a false antrum.
Clinical Scenarios and Viva Questions
These scenarios will help you apply your knowledge and prepare for practical and viva exams.
Scenario 1
A 10-year-old boy presents to the emergency room with a 2-week history of a painful ear, fever, and a swollen, tender area behind his ear. His ear canal shows a sagging of the posterosuperior wall. He has not responded to oral antibiotics.
- What is your likely diagnosis? The clinical picture strongly suggests acute coalescent mastoiditis with a subperiosteal abscess. The sagging of the posterosuperior canal wall is a classic sign.
- What is the definitive management? The patient requires a cortical mastoidectomy to drain the abscess and exenterate the infected air cells.
- How would you answer an examiner’s question about the role of antibiotics in this case? You would explain that while antibiotics are the first-line treatment for otitis media, surgical intervention is necessary when the disease has progressed to coalescent mastoiditis with abscess formation, as antibiotics alone cannot penetrate the thick, infected bone.
Scenario 2
During a cortical mastoidectomy, you encounter a sudden, gushing bleed from the posterior part of the mastoid cavity.
- What is the most likely source of bleeding? Injury to the sigmoid sinus is the most probable cause of such profuse bleeding.
- How would you control the bleeding? The immediate step is to apply firm pressure with a gloved finger or gauze. Once controlled, you would use bone wax, absorbable collagen, or a muscle graft to pack the bleeding site.
- What is a serious potential complication associated with this injury, and how would you prevent it? An air embolism can occur if air is sucked into the venous system. You would prevent this by keeping the surgical field constantly flooded with saline and applying immediate pressure to the bleeding vessel.
Multiple Choice Questions (MCQs)
Test your knowledge with these NEET PG-style MCQs.
- The most reliable internal landmark for the facial nerve during a cortical mastoidectomy is: a) The spine of Henle b) The digastric ridge c) The horizontal semicircular canal d) The tympanomastoid suture
- Which of the following is an incorrect statement about a postauricular incision for mastoidectomy? a) It is the most widely used approach. b) It provides the best exposure. c) It is preferred for temporal bones with restricted pneumatization. d) It allows for excellent exposure of the mastoid bone.
- Sagging of the posterosuperior canal wall is a sign of: a) Acute otitis externa b) Acute coalescent mastoiditis c) Chronic suppurative otitis media d) Tympanosclerosis
- A cortical mastoidectomy is considered a conservative procedure because it: a) Involves removal of a limited number of air cells b) Preserves the ossicular chain c) Leaves the superior and posterior bony meatal walls intact d) Does not require a general anesthetic
- The most feared intraoperative complication of a cortical mastoidectomy is: a) Sigmoid sinus injury b) Dural injury c) Facial nerve injury d) Incus dislocation
- All of the following are indications for a cortical mastoidectomy EXCEPT: a) Acute mastoiditis with subperiosteal abscess b) Cholesteatoma of the mastoid c) Endolymphatic sac decompression d) Coalescent mastoiditis unresponsive to antibiotics
- The primary purpose of local infiltration with adrenaline during a mastoidectomy is to: a) Provide general anesthesia b) Increase blood pressure c) Achieve hemostasis d) Block the facial nerve
- The key surface landmark for the mastoid antrum is: a) The digastric ridge b) The spine of Henle c) The mastoid tip d) Macewen’s triangle
- Which of the following nerves is NOT typically anesthetized during local infiltration for mastoid surgery? a) Greater auricular nerve b) Facial nerve c) Auriculotemporal nerve d) Auricular branch of the vagus
- A false antrum can be created due to a well-developed: a) Tegmen plate b) Korner’s septum c) Digastric ridge d) Lateral sinus plate
Answers with Explanations:
- c) The horizontal semicircular canal. It is a constant landmark, and the facial nerve is located just anterior and medial to it.
- c) It is preferred for temporal bones with restricted pneumatization. The endaural incision is more suited for this type of temporal bone.
- b) Acute coalescent mastoiditis. This is a classic sign of mastoiditis as pus builds up in the mastoid bone, leading to swelling and a prolapse of the canal wall.
- c) Leaves the superior and posterior bony meatal walls intact. This is the defining feature of a conservative mastoidectomy, which helps to maintain the normal anatomy of the external auditory meatus.
- c) Facial nerve injury. While all are serious, facial nerve injury can result in permanent facial paralysis, which is psychologically devastating for the patient.
- b) Cholesteatoma of the mastoid. Cholesteatoma requires a more extensive procedure like a modified radical mastoidectomy or a canal wall down procedure to ensure complete removal of the disease.
- c) Achieve hemostasis. The adrenaline causes vasoconstriction, which significantly reduces bleeding during the surgery.
- d) Macewen’s triangle. This is a reliable surface landmark that indicates the location of the underlying mastoid antrum.
- b) Facial nerve. The facial nerve should be avoided during infiltration; a nerve block is not required and could cause temporary paralysis.
- b) Korner’s septum. This is a bony plate that can be mistaken for the mastoid antrum, leading to a false antrum and incomplete exenteration of the air cells.
Frequently Asked Questions in Viva
Here are some common questions about cortical mastoidectomy, perfect for your viva prep.
- What is the difference between simple and modified radical mastoidectomy? A simple (cortical) mastoidectomy preserves the bony external auditory canal and middle ear structures, whereas a modified radical mastoidectomy involves removing the posterior bony canal wall and exteriorizing the mastoid cavity and middle ear into a common cavity.
- Why is the mastoid antrum so important? The mastoid antrum is the central, largest, and most constant air cell in the mastoid. It serves as the gateway to all other mastoid air cells, making it the primary target for a surgeon seeking to exenterate diseased tissue.
- What does “coalescent mastoiditis” mean? This term describes the process where inflammation and infection lead to the breakdown of the bony septa between the mastoid air cells, causing them to “coalesce” into a single abscess cavity.
- How do you prevent facial nerve injury during mastoidectomy? We prevent this by using a meticulous surgical technique, constantly irrigating the burr with saline to prevent thermal injury, and identifying all key anatomical landmarks, especially the horizontal semicircular canal, to protect the nerve.
- Is cortical mastoidectomy a cure for otitis media? No, it is a treatment for mastoiditis, which is a complication of otitis media. The underlying otitis media must be managed concurrently.
- What is the purpose of a mastoid dressing? A mastoid dressing provides gentle compression to the surgical site, which helps to reduce swelling, prevent hematoma formation, and support the healing flap.
Download the full PDF Link:
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.

Dr. Rahul Bagla MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi) Fellow Rhinoplasty & Facial Plastic Surgery. Renowned Teaching Faculty Mail: msrahulbagla@gmail.com India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Learn cortical mastoidectomy with indications, surgical steps, complications, and high-yield points for NEET PG and ENT exams. Cortical mastoidectomy, Mastoidectomy surgery, Simple mastoidectomy, Schwartz mastoidectomy, Mastoid bone surgery, Mastoiditis surgery, Cortical mastoidectomy procedure, Indications of cortical mastoidectomy, Mastoidectomy surgical steps, Postauricular incision mastoidectomy, Complications of cortical mastoidectomy, Macewen’s triangle mastoid landmark, Conservative mastoidectomy surgery, Difference between simple and modified radical mastoidectomy, Step-by-step cortical mastoidectomy technique, High yield points for mastoidectomy NEET PG, Cortical mastoidectomy indications and contraindications, Complications after mastoidectomy surgery, Role of cortical mastoidectomy in otitis media complications, Schwartz mastoidectomy exam preparation notes, Mastoid antrum importance in mastoidectomy, How to prevent facial nerve injury during mastoidectomy, Cortical mastoidectomy vs radical mastoidectomy differences, Cortical mastoidectomy viva questions for exams