|
The following CBME core competencies are covered in this chapter.
|
Anatomy and Physiology of the Facial Nerve
Introduction
The facial nerve (seventh cranial nerve) is an embryological derivative of the second branchial arch. The facial nerve is a mixed nerve containing motor, sensory, and parasympathetic fibres. It contains approximately 7000–9000 motor fibres and 3000–5000 sensory and parasympathetic fibres. The motor fibres control the muscles of facial expression. The sensory and parasympathetic fibres travel in the nervus intermedius (nerve of Wrisberg) and carry taste sensation from the anterior two‑thirds of the tongue, secretomotor fibres to the lacrimal and salivary glands, and general sensation from the external auditory canal.
The facial nerve has a motor root and a sensory/parasympathetic root (the nervus intermedius). The motor fibres arise from the facial nerve nucleus, while parasympathetic fibres arise from the superior salivatory and lacrimal nuclei. The sensory fibres terminate in the nucleus tractus solitarius and the spinal nucleus of the trigeminal nerve in the CNS.
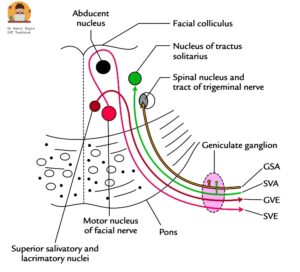
Diagram: Cross-section through the pons, showing nuclei related to the facial nerve
Facial Nerve Nuclei and Central Connections
The facial nerve is a mixed nerve containing motor, sensory, and parasympathetic fibres. Four nuclei in the brainstem contribute to its formation.
- Facial nerve nucleus (principal nucleus or branchiomotor nucleus): It is located in the lower part of the pons. It gives rise to special visceral efferent (SVE) fibres of the facial nerve. It supplies all the muscles derived from the second branchial arch, i.e. the muscles of facial expression, buccinator, stapedius, platysma, the posterior belly of digastric and stylohyoid. It is responsible for facial expression and assists in movements related to swallowing and elevation of the hyoid bone. The motor neurons supplying the forehead muscles receive bilateral corticobulbar input from both cerebral hemispheres, which explains why forehead movement is preserved in supranuclear (upper motor neuron) lesions. The motor neurons supplying the lower face receive mainly contralateral input. Emotional expressions (smiling, crying) are preserved in supranuclear palsy because they are mediated by thalamonuclear fibres that bypass the corticobulbar tract.
- Superior salivatory nucleus and lacrimal nucleus: They are also located in the lower pons. They give rise to parasympathetic fibres (general visceral efferent [GVE] fibres). It supplies the lacrimal glands, the salivary glands (submandibular and sublingual), and the smaller secretory glands in the nasal mucosa and the palate. They are preganglionic parasympathetic fibres.
- Nucleus of tractus solitarius (gustatory nucleus): It is located in the medulla oblongata. It receives sensory fibres (special visceral afferent [SVA] fibres) from the facial nerve. It carries taste sensation from the anterior two-thirds of the tongue via the chorda tympani and soft and hard palate via the greater petrosal nerve.
- Spinal nucleus of the trigeminal nerve: It is located in the medulla oblongata. It receives general somatic afferent (GSA) fibres carrying touch, pain, and temperature sensation from the posterosuperior aspect of the external auditory canal, the concha, and the tympanic membrane. This explains the severe pain of Ramsay Hunt syndrome and the anaesthesia over the posterior meatal wall (Hitzelberger’s sign) seen in acoustic neuroma.
Mnemonic: “Face Tears Taste Touch”
- Face → Facial nerve nucleus → Facial expression
- Tears → Superior salivatory and lacrimal nuclei → Lacrimation and salivation
- Taste → Nucleus tractus solitarius → Taste from anterior two-thirds of tongue
- Touch → Spinal nucleus of trigeminal nerve → Touch, pain, and temperature sensation from ear regions
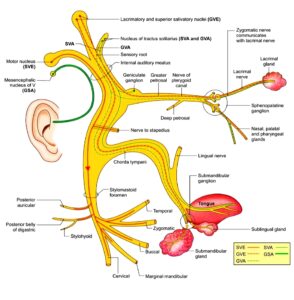
Diagram: Nuclei of the facial nerve
Course and Segments of the Facial Nerve
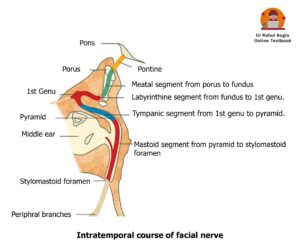
The facial nerve follows a complex course that is traditionally divided into intracranial (cisternal), intratemporal, and extratemporal (extracranial) parts. The intratemporal portion is further subdivided into meatal, labyrinthine, tympanic, and mastoid segments.
1. Intracranial course (pontine or cisternal segment – 24-25 mm)
This segment extends from the origin of the facial nerve from the pons to the internal acoustic meatus. The motor fibres arise from the facial nerve nucleus located in the lower part of the pons. Unlike most cranial nerve motor fibres, which pass directly forwards to leave the brainstem, the motor fibres of the facial nerve first pass backwards towards the abducens nucleus (VIth nerve), loop around it, and then turn forwards to exit the brainstem at the cerebellopontine angle. Fibres from the superior salivatory nucleus, lacrimal nucleus, nucleus tractus solitarius, and spinal nucleus of the trigeminal nerve also emerge at the cerebellopontine angle. After emerging from the brainstem, these fibres form two roots. The first root contains the motor fibres of the facial nerve, while the second root contains the parasympathetic and sensory fibres called the nervus intermedius (nerve of Wrisberg). The nervus intermedius joins the motor root to form the facial nerve. The facial nerve then travels through the posterior cranial fossa and enters the internal acoustic meatus through its medial opening called the porus acusticus.
 2. Intratemporal course
2. Intratemporal course
The facial nerve passes through the internal acoustic meatus, enters the facial canal (Fallopian canal), traverses the middle ear cavity, and exits the skull through the stylomastoid foramen. The intratemporal course of the facial nerve is divided into four segments: meatal, labyrinthine, tympanic, and mastoid segments.
- Meatal segment (8–10 mm): This segment extends from the porus acusticus (medial end) to the fundus (lateral end) of the internal acoustic meatus. The internal acoustic meatus is located on the posterior surface of the petrous part of the temporal bone. Within the internal acoustic meatus, the facial nerve lies in the anterosuperior quadrant. The superior vestibular nerve lies in the posterosuperior quadrant, the cochlear nerve lies in the anteroinferior quadrant, and the inferior vestibular nerve lies in the posteroinferior quadrant. This anatomical relationship is important for understanding the sequence of cranial nerve involvement in cerebellopontine angle tumours such as vestibular schwannoma.
- Labyrinthine segment (4 mm): This segment extends from the fundus of the internal acoustic meatus to the geniculate ganglion, where the first genu of the facial nerve is formed. From the fundus, the facial nerve enters the bony facial canal and passes anteriorly towards the geniculate ganglion, which lies at the anterosuperior part of the medial wall of the middle ear. At the geniculate ganglion, the nerve makes a sharp hairpin turn of about 75° posteriorly, forming the first genu (anterior genu). The labyrinthine segment is the shortest and narrowest part of the intratemporal facial nerve, with a diameter of about 0.61–0.68 mm. Because of its narrow size, oedema or inflammation can easily compress the nerve in this segment and produce facial paralysis. This segment is also more vulnerable to ischemia and vascular compression because it has poor arterial anastomosis.
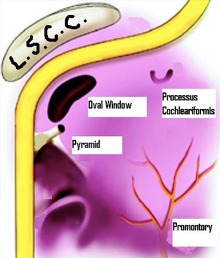
- Tympanic segment (11 mm): This segment extends from the first genu at the geniculate ganglion to the pyramidal eminence. From the geniculate ganglion, the facial nerve passes posteroinferiorly along the medial wall of the middle ear cavity to reach the area just above the pyramidal eminence. In this segment, the nerve runs medial to the incus, posterosuperior to the cochleariform process, above the oval window, and below the lateral semicircular canal. Dehiscence of the fallopian canal is common in the tympanic segment and is seen in about 10–40% of individuals. Because of this incomplete bony covering, the tympanic segment is the most common site of facial nerve injury during middle ear surgery.
- Mastoid or vertical segment (13 mm): This segment extends from the pyramidal eminence to the stylomastoid foramen. Posterior to the pyramidal eminence, the tympanic segment turns inferiorly through an angle of about 95–125°, forming the second genu, and continues as the mastoid segment. The facial nerve then descends vertically along the posterior wall of the middle ear cavity and exits the skull through the stylomastoid foramen. The mastoid segment is the longest part of the intratemporal course of the facial nerve. The second genu is an important surgical landmark and is the most common site of facial nerve injury during mastoid surgery.
Mnemonic: “Porus Finds Genie’s Pyramid Secret”
- Porus → Fundus = Meatal segment (8–10 mm)
- Fundus → Geniculate ganglion = Labyrinthine segment (4 mm)
- Geniculate ganglion → Pyramidal eminence = Tympanic segment (11 mm)
- Pyramidal eminence → Stylomastoid foramen = Mastoid segment (13 mm)
3. Extracranial course
It extends from the stylomastoid foramen to the termination of its peripheral branches. The facial nerve exits from the stylomastoid foramen, travels anterior to the posterior belly of the digastric and lateral to the styloid process. Then it enters the parotid gland high up on its posteromedial surface and divides within the gland. It usually divides just behind and superficial to the retromandibular vein and external carotid artery (ECA). The length from the stylomastoid foramen to the initial intra-parotid bifurcation ranges between 8 – 22 mm.
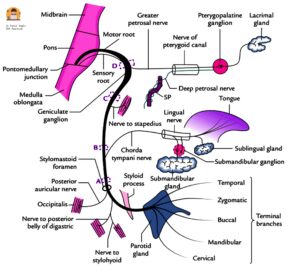
Diagram: Branches of facial nerve
Branches of the Facial Nerve
From the geniculate ganglion (1st Genu)
- Greater petrosal nerve: It is the first branch of the facial nerve and carries preganglionic parasympathetic fibres to the lacrimal gland and to the nasal and palatine glands via the pterygopalatine ganglion.
From the mastoid segment
- Nerve to Stapedius: It arises from the mastoid (vertical) segment and supplies the stapedius muscle.
- Chorda tympani: It arises from the middle of the mastoid segment, 5-6 mm above the stylomastoid foramen. It enters the middle ear through the posterior canaliculus at the junction of the lateral and posterior walls of the middle ear. It runs on the medial surface of the tympanic membrane between its mucosal and fibrous layers. It runs medially just below the neck of the malleus and above the attachment of the tendon of the tensor tympani. It further continues forward and leaves the middle ear through the anterior canaliculus (canal of Huguier). It carries taste fibres from the anterior two-thirds of the tongue and parasympathetic fibres to the submandibular and sublingual glands.
At the stylomastoid foramen
- Posterior Auricular Nerve: After exiting the stylomastoid foramen, the facial nerve gives off a posterior auricular branch, which supplies auricular muscles (superior & posterior) and occipitalis muscle and communicates with the auricular branch of vagus.
- Nerve to stylohyoid: It innervates the stylohyoid muscle (a suprahyoid muscle of the neck). It elevates the hyoid bone.
- Nerve to posterior belly of digastric: It innervates the posterior belly of the digastric muscle (a suprahyoid muscle of the neck). It elevates the hyoid bone.
- Small Muscular Branches.
Communicating Branch
It joins the auricular branch of vagus and supplies the concha, posterior auricular groove, posterior meatus and the outer surface of the tympanic membrane.
Peripheral Branches to the face
It forms two divisions:
- Upper temporofacial part (further divided into temporal, zygomatic, and upper buccal branches).
- Lower cervicofacial part (further divided into lower buccal, mandibular and cervical branches).
Both divisions together form pes anserinus (goose-foot). Muscles supplied by the peripheral branches of the facial nerve are:
- Temporal branches: supply the frontalis, orbicularis oculi and corrugator supercilli muscles.
- Zygomatic branches: supply the orbicularis oculi muscle.
- Buccal branches: supply the orbicularis oris, buccinator and zygomaticus muscles.
- Marginal mandibular branch: supplies the depressor labii inferioris, depressor anguli oris and mentalis muscles.
- Cervical branch: supplies the platysma muscle in the neck.
Mnemonic: “To Zanzibar By Motor Car”. Temporal Zygomatic Buccal Marginal mandibular Cervical
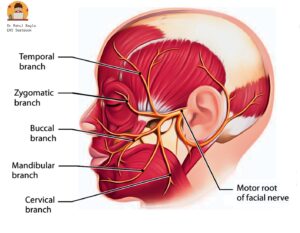
Diagram : Peripheral branches of facial nerve
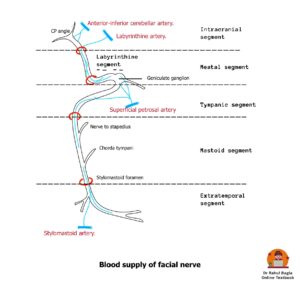
Blood Supply of the Facial Nerve
The facial nerve receives a segmental blood supply from branches of both the vertebrobasilar system and the external carotid artery system.
The principal arteries supplying the facial nerve are:
- Labyrinthine artery — usually a branch of the anterior inferior cerebellar artery (AICA)
- Petrosal branch of the middle meningeal artery (superficial petrosal artery)
- Stylomastoid artery — usually a branch of the posterior auricular artery, occasionally from the occipital artery
Table: Segmental Blood Supply
| Segment | Arterial Supply |
| Cerebellopontine angle | Branches of the anterior-inferior cerebellar artery. |
| Meatal and labyrinthine segments | Labyrinthine artery |
| Geniculate ganglion | Petrosal branch of the middle meningeal artery |
| Tympanic and mastoid segments | Anastomotic network between the superficial petrosal branch of the middle meningeal artery and the stylomastoid branch of the posterior auricular artery. |
| Stylomastoid foramen to parotid segment | Stylomastoid artery |
| Temporofacial and cervicofacial branches | Collaterals from the superficial temporal, transverse facial, facial, and maxillary arteries |
The labyrinthine segment has limited collateral circulation and lacks significant anastomosing arterial channels, making it particularly vulnerable to ischemia, oedema, and vascular compression within the narrow fallopian canal. This vascular vulnerability is considered an important factor in the pathogenesis of Bell’s palsy.
Veins accompany the arteries within the fallopian canal, while lymphatic vessels are present in the epineurial layer of the nerve.
Surgical Landmarks of the Facial Nerve
For middle ear and mastoid surgery
- Processus cochleariformis: It is an important landmark for the geniculate ganglion, which lies just anterior and superior to it. The tympanic (horizontal) segment of the facial nerve begins at this level.
- Oval window and lateral semicircular (horizontal) canal: The tympanic segment of the facial nerve runs above the oval window (stapes footplate) and below the lateral semicircular canal.
- Short process of incus: At the level of the aditus, the facial nerve lies medial to the short process of the incus.
- Pyramidal eminence (pyramid): The vertical (mastoid) segment of the facial nerve descends posterior to the pyramidal eminence and posterior tympanic sinus.
- Tympanomastoid suture: In the mastoid segment, the facial nerve runs just deep/anterior to the tympanomastoid suture, making it an important external landmark.
- Digastric ridge: The facial nerve exits the stylomastoid foramen just anterosuperior to the digastric ridge.
Surgical landmarks of the facial nerve in middle ear and mastoid surgery.
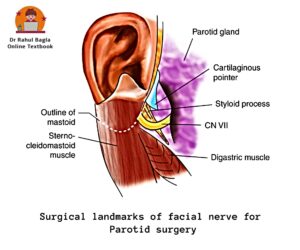
For parotid surgery
- Tragal pointer: The main trunk of the facial nerve lies approximately 1 cm medial and slightly antero-inferior to the tragal pointer. The Tragal pointer is a sharp triangular piece of pinna cartilage, and it “points” to the nerve.
- Posterior belly of digastric: During retrograde dissection, the posterior belly of the digastric muscle is traced superiorly up to its attachment at the mastoid process. The facial nerve is identified passing between the mastoid and styloid processes. Near the mastoid attachment of the digastric muscle, the facial nerve lies just superior to the upper border of the posterior belly of the digastric muscle.
- Tympano-mastoid suture: The facial nerve trunk can be identified about 6–8 mm deep to the inferior end (“drop-off”) of the tympanomastoid suture.
- Styloid process: The facial nerve passes lateral to the styloid process after exiting the stylomastoid foramen.
Anomalies of the Facial Nerve
Nerve anomalies are more common in congenitally malformed ears; hence, the clinician should be careful while operating on such ears.
- Bony dehiscence: The most common site of absence or dehiscence of bony cover is the tympanic segment over the oval window. Other sites are: near the geniculate ganglion or in the area of retrofacial mastoid cells. A dehiscent nerve is likely to be injured during surgery and infections of the middle ear or mastoid.
- Prolapse of nerve: The dehiscent nerve may prolapse over the stapes, creating difficulty in stapes surgery or ossicular reconstruction surgery.
- Hump: The nerve at times makes a hump posteriorly near the horizontal canal, hence vulnerable to injury during mastoid surgery.
- Bifurcation and trifurcation. The vertical part of the facial nerve bifurcates or trifurcates; each may occupy different canals and exit through individual foramina.
- Bifurcation and enclosing the stapes. The nerve bifurcates proximal to the oval window—one of the branches passes above and the other below it, and then both reunite.
- Between oval and round windows. Just before the oval window, the nerve crosses the middle ear between the oval and the round windows.

Diagram: Anomalies of the Facial Nerve
Histology of the Facial Nerve
The facial nerve is a peripheral nerve and is covered by three connective tissue layers:
- Endoneurium – the innermost layer; surrounds each individual nerve fibre.
- Perineurium – the middle layer; surrounds a bundle of nerve fibres (fascicle).
- Epineurium – the outermost layer; surrounds multiple fascicles and forms the outer covering of the nerve.
These layers provide support, protection, and strength to the nerve. The main supporting cells of peripheral nerves are Schwann cells, which form the myelin sheath and help nourish and repair the nerve.
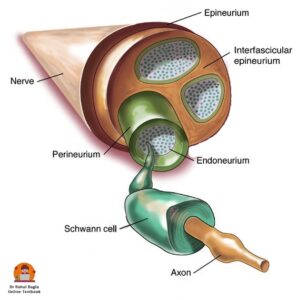
Diagram: Showing the cross-sectional structure of the facial nerve
Pathophysiology of Nerve Injury
Understanding the classification of nerve injury is essential for predicting recovery and planning intervention.
Seddon Classification
In 1941, Seddon introduced a classification of nerve fibre injury based on the types of nerve fibre injury and the continuity of the nerve.
- Neuropraxia (Mild injury): There is a temporary conduction block due to compression or ischaemia of the nerve. There is no Wallerian degeneration. Release of the pressure results in a rapid and complete recovery of function (6-8 weeks). This is the typical pathology in early Bell’s palsy.
- Axonotmesis (Moderate injury): There is partial sectioning or excessive compression of the nerve. Axons are disrupted, but all three connective tissue layers are preserved. Wallerian degeneration occurs distal to the site of injury over a period of 72-96 hours following injury. Regeneration occurs at 1 mm per day, but recovery is often incomplete due to misdirection of regenerating fibres, leading to synkinesis.
- Neurotmesis (Severe injury): There is complete nerve transection of the nerve due to severe contusion, stretch or laceration. There is a complete loss of sensory and motor function. Spontaneous recovery does not occur, and surgical repair is required.
Sunderland Classification
Sir Sydney Sunderland, in 1951, expanded Seddon’s classification into five degrees, and his classification is now widely accepted. Lower-grade injuries (1st–3rd degree) are more commonly seen in viral and inflammatory disorders, whereas 4th- and 5th-degree injuries are usually associated with trauma, surgery, or neoplasms.
| Degree | Pathology | Recovery |
| First (Neuropraxia) | Conduction block, no Wallerian degeneration | Complete |
| Second (Axonotmesis) | Axons are disrupted, endoneurium intact. Wallerian degeneration occurs | Good, usually complete |
| Third | Endoneurium is disrupted, and perineurium and epineurium remain intact | Partial, synkinesis is common |
| Fourth | Endoneurium and perineurium disrupted, epineurium intact | Poor, requires surgery |
| Fifth (Neurotmesis) | Complete transection (all three connective tissue layers are disrupted) | Requires surgical repair |
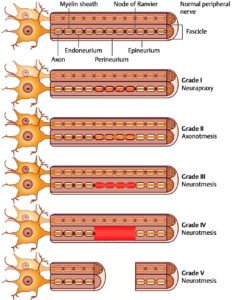
Diagram: Sunderland Classification
———— End of the chapter ————
High-Yield Points
- Facial nerve is derived from the second branchial arch
- Mixed nerve: motor, sensory and parasympathetic fibres
- Nervus intermedius carries sensory and parasympathetic fibres
- Narrowest segment = labyrinthine segment
- Most common surgical injury site = tympanic segment
- Forehead spared in UMN lesions
- Chorda tympani carries taste from anterior two-thirds of tongue
- House-Brackmann grading is used for facial palsy assessment
- Bell’s palsy commonly affects the labyrinthine segment
NEET PG-Style MCQs
- A 45-year-old patient develops sudden onset of left-sided facial weakness. On examination, she cannot raise her left eyebrow or close her left eye completely. The left nasolabial fold is flattened, and the angle of the mouth droops on the left side. Which of the following best localises the lesion? A. Left upper motor neuron lesion B. Left lower motor neuron lesion C. Right upper motor neuron lesion D. Right lower motor neuron lesion.
- The greater petrosal nerve carries which type of fibres and supplies which structure? A. Motor fibres to the stapedius muscle B. Sensory fibres to the posterior meatal wall C. Parasympathetic fibres to the lacrimal gland D. Taste fibres to the anterior two-thirds of the tongue.
- During mastoid surgery, the surgeon identifies the second genu of the facial nerve. Which segment directly follows this genu? A. Labyrinthine segment B. Tympanic segment C. Meatal segment D. Mastoid segment.
- A patient with Bell’s palsy complains that sounds seem abnormally loud on the affected side. Which branch of the facial nerve is most likely involved? A. Chorda tympani B. Nerve to stapedius C. Greater petrosal nerve D. Posterior auricular nerve.
- The narrowest and most ischaemia-prone segment of the intratemporal facial nerve is the: A. Labyrinthine segment B. Tympanic segment C. Mastoid segment D. Meatal segment.
- Within the internal acoustic meatus, the facial nerve lies in which quadrant? A. Posterosuperior B. Posteroinferior C. Anterosuperior D. Anteroinferior.
- Which of the following correctly pairs a facial nerve branch with its function? A. Chorda tympani – parasympathetic to lacrimal gland B. Greater petrosal nerve – parasympathetic to lacrimal gland C. Posterior auricular nerve – taste from anterior tongue D. Nerve to stapedius – motor to posterior belly of digastric.
- A 30-year-old man presents with right-sided facial weakness following a motor vehicle accident. He cannot move any muscle on the right side of his face, including the forehead. The weakness is complete. Which type of nerve injury is most likely, and what is the prognosis without surgery? A. Neuropraxia, complete recovery in 6–8 weeks B. Axonotmesis, good recovery with possible synkinesis C. Sunderland first degree, complete recovery D. Neurotmesis, no spontaneous recovery.
- Which of the following statements about the chorda tympani is correct? A. It arises from the geniculate ganglion B. It carries taste from the posterior one-third of the tongue C. It runs medial to the tympanic membrane D. It supplies parasympathetic fibres to the parotid gland.
- A patient has an upper motor neuron facial palsy due to a right-sided stroke. Which of the following findings would you expect? A. Inability to raise the left eyebrow B. Sparing of the left forehead muscles with lower face weakness C. Complete left-sided facial paralysis including the forehead D. Preservation of voluntary but loss of emotional facial movements.
Answers: 1-B, 2-C, 3-D, 4-B, 5-A, 6-C, 7-B, 8-D, 9-C, 10-B.
Clinical Case Scenarios
Case 1. A 38-year-old woman presents with a sudden onset of left-sided facial weakness that began this morning. She cannot close her left eye completely, and she notices that food collects in her left cheek while eating. She has no weakness in her arms or legs, and she speaks clearly. On examination, she cannot raise her left eyebrow, and the left nasolabial fold is flattened. Her left eye has a dry appearance. Most likely diagnosis: Bell’s palsy (idiopathic peripheral facial palsy). Best initial investigation: Clinical diagnosis; consider MRI or CT only if atypical features are present. Best initial management: Oral prednisolone (1 mg/kg/day for 7–10 days) plus eye protection (artificial tears, nocturnal eye taping).
Case 2. A 55-year-old man with diabetes mellitus presents with severe left ear pain, followed 3 days later by vesicles on his left pinna and ear canal, and then left-sided facial paralysis. He also reports vertigo and hearing loss. Most likely diagnosis: Ramsay Hunt syndrome (herpes zoster oticus). Best investigation: Clinical diagnosis; PCR of vesicular fluid if needed. Best management: Oral valacyclovir (1 g three times daily for 7 days) plus oral prednisolone, and symptomatic treatment for vertigo.
Case 3. A 45-year-old woman presents with progressive right-sided hearing loss over 2 years. She now reports mild right-sided facial weakness and occasional dizziness. On examination, she has reduced hearing on the right side, and the corneal reflex is diminished on the right. Hitzelberger’s sign (hypoaesthesia over the posterior meatal wall) is present. Most likely diagnosis: Vestibular schwannoma (acoustic neuroma). Best initial investigation: MRI brain with contrast (shows enhancing lesion in cerebellopontine angle). Best management: Observation for small tumours, stereotactic radiosurgery, or microsurgical excision.
Case 4. A 25-year-old man presents with an inability to close his left eye and drooling from the left side of his mouth for 2 weeks. He had a similar episode on the same side 2 years ago that resolved completely after 3 months. On examination, he has complete left-sided facial paralysis, including the forehead. When he tries to smile, his left eye partially closes (synkinesis). Most likely diagnosis: Recurrent Bell’s palsy with synkinesis (sequela of axonotmesis with misdirected regeneration). Best investigation: Electroneuronography (ENoG) and electromyography (EMG) to assess nerve degeneration and regeneration. Best management: Facial retraining exercises, botulinum toxin for synkinesis, and eye protection.
Frequently Asked Questions in Viva
- What is the difference between UMN and LMN facial palsy?
- Why is the labyrinthine segment vulnerable in Bell’s palsy?
- What is the function of the chorda tympani nerve?
- What is the House-Brackmann grading system?
- Which segment of the facial nerve is commonly injured during ear surgery?
- What is Hitzelberger’s sign?
- What are the branches of the facial nerve?
- What is the nervus intermedius?
- What is Ramsay Hunt syndrome?
- How does Bell’s palsy present clinically?
———— End ————
Download full PDF Link:
Facial Nerve Paralysis Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck surgery.
- W. Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Salah Mansour, Textbook of Comprehensive and Clinical Anatomy of the Middle Ear.
- Susan Standring, Gray’s Anatomy.
- Orlando Guntinas-Lichius, Textbook of Facial Nerve Disorders and Diseases: Diagnosis and Management.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Anatomy of facial nerve, Facial Nerve Branches, Facial Nerve Palsy, Facial Nerve Course, Facial nerve embryology, Components of facial nerve, Course of facial nerve, Bell’s palsy, Ramsay hunt syndrome, Fractures of temporal bone, Facial nerve grading systems, Understanding Facial Nerve Grading Systems: A Comprehensive Guide, House-Brackmann scale interpretation, How to Interpret the House-Brackmann Scale for Facial Paralysis, Facial nerve palsy ocular symptoms, Recognizing Ocular Symptoms in Facial Nerve Palsy, Facial nerve paralysis rehabilitation exercises, Effective Rehabilitation Exercises for Facial Nerve Paralysis, Facial nerve palsy differential diagnosis, Differential Diagnosis in Facial Nerve Palsy: What to Consider, Facial nerve paralysis grading scales, An Overview of Grading Scales for Facial Nerve Paralysis, Facial nerve palsy ocular complications, Managing Ocular Complications in Facial Nerve Palsy, Facial nerve paralysis treatment options, Exploring Treatment Options for Facial Nerve Paralysis, Facial nerve palsy recovery timeline, What to Expect: Recovery Timeline for Facial Nerve Palsy, Facial nerve anatomy clinical relevance, The Clinical Relevance of Facial Nerve Anatomy.
Wonderful
Thanks
Thank you sir—boon for both PG and MBBS Students.
Thanks
Wonderful job sir.
Thanks
Amazing content sir
Thanks
One thing, it was said that Facial Nerve branches stapedius nerve at 2nd genu, but I don’t see this 2nd genu mentioned anywhere else. What is it exactly?
Amazing notes, this website is my favorite ENT source!