Proptosis
Proptosis refers to the forward displacement or protrusion of the eyeball from the orbit. As the orbit has rigid bony walls, any space-occupying lesion within the orbit increases intraorbital pressure, consequently pushing the globe forward. However, the globe may also deviate medially, laterally, upward, or downward depending on the location of the lesion within the orbit. Therefore, the direction of displacement often provides important diagnostic clues. When the protrusion is specifically due to thyroid eye disease, it is often termed exophthalmos, though the terms are used interchangeably in general practice.

Clinical Definition: Proptosis is measured using Hertel’s exophthalmometer, which determines the distance from the lateral orbital rim to the corneal apex.
- Normal proptosis: Less than 21 mm from the lateral orbital rim to the corneal apex.
- Significant proptosis: >21 mm or asymmetry >2 mm between eyes.
- Racial variations exist (Black: up to 23 mm, Asian: lower values).
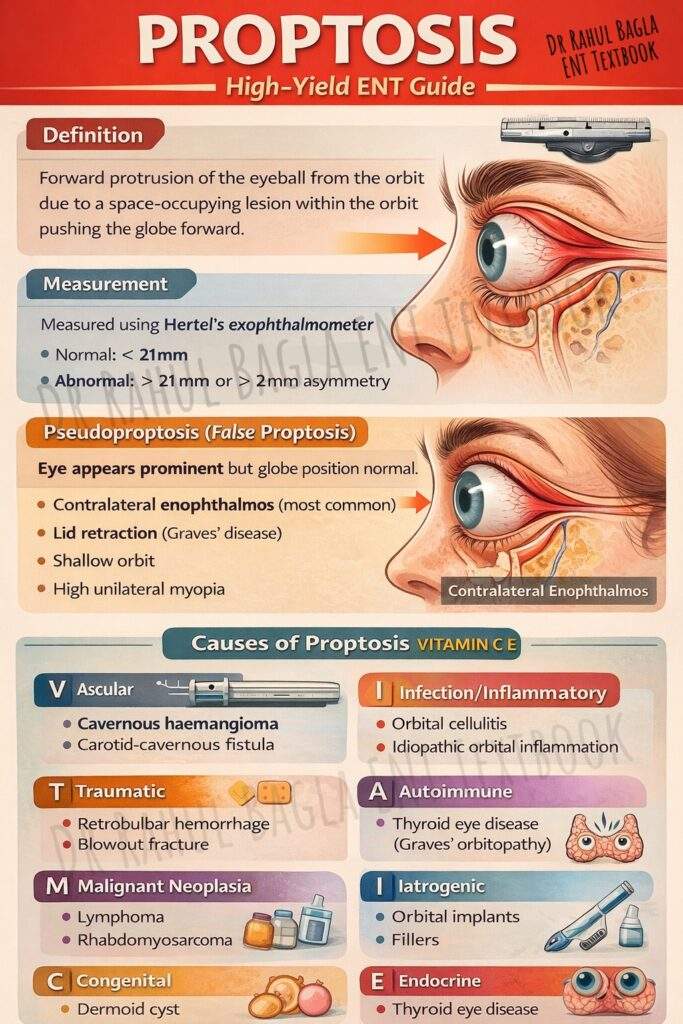
Pseudoproptosis. Proptosis should be differentiated from pseudoproptosis, a gimmick condition that makes an eye appear to be protruding when it is actually normal.
Causes of Pseudoproptosis:
- Asymmetry of Bony Orbits: Conditions like a shallow orbit on one side can make the eye appear more prominent.
- Contralateral Enophthalmos: This is the most common cause. A sunken eye, for example, from an old, untreated orbital blowout fracture, makes the other, normal eye look proptosed by comparison.
- Lid Retraction: A widened palpebral fissure, as seen in Graves’ disease or neurogenic conditions, exposes more of the globe, creating an illusion of proptosis.
- High Unilateral Myopia: An abnormally long eyeball can push the orbital contents forward, mimicking true proptosis.
Classifications of Proptosis
1. Based on Onset
- Acute proptosis (minutes to hours): Retrobulbar haemorrhage, Orbital emphysema, Carotid-cavernous fistula.
- Subacute proptosis (days to weeks): Orbital cellulitis, Idiopathic orbital inflammation, Rhabdomyosarcoma, Neuroblastoma.
- Chronic proptosis (months to years): Thyroid eye disease, Benign tumours (haemangioma, dermoid), Malignant tumours (lymphoma, meningioma), Mucocele.
2. Based on Laterality
- Unilateral proptosis: Orbital tumours, Orbital cellulitis, Idiopathic orbital inflammation, Trauma.
- Bilateral proptosis: Thyroid eye disease (most common), Lymphoma, Leukaemia, Systemic granulomatous diseases (Sarcoidosis, GPA), Metastasis.
3. Based on the Direction of Displacement
- Axial (direct forward): Intraconal space lesions – Cavernous haemangioma, Optic nerve glioma.
- Downward and medial: Lacrimal gland region (superolateral) – Lacrimal gland tumours.
- Downward and lateral: Ethmoid sinus (medial) – Ethmoidal mucocele, Sinus tumours.
- Upward: Maxillary sinus (inferior) – Maxillary carcinoma invading orbit.
- Lateral: Ethmoid sinus (medial) – Aggressive ethmoid tumours.
- Pulsatile: Vascular or bony defect – Carotid-cavernous fistula, Neurofibromatosis with sphenoid dysplasia.
- Intermittent/Positional: Venous origin – Orbital varix (increases with Valsalva).
Causes of Proptosis (VITAMIN CE)
- V – Vascular: Cavernous haemangioma, Capillary haemangioma, Orbital varix, Carotid-cavernous fistula, Cavernous sinus thrombosis.
- I – Inflammatory/Infectious: Orbital cellulitis, Subperiosteal abscess, Idiopathic orbital inflammation (orbital pseudotumor), Sarcoidosis, Granulomatosis with polyangiitis (GPA), IgG4-related disease.
- T – Traumatic: Retrobulbar haemorrhage, Orbital emphysema, Foreign body, Carotid-cavernous fistula (traumatic).
- A – Autoimmune: Thyroid eye disease (Graves ophthalmopathy).
- M – Metabolic: Aggressive IV rehydration (orbital compartment syndrome) – rare.
- I – Iatrogenic: Orbital implants, Fillers, Post-surgical haematoma.
- N – Neoplastic (Benign): Cavernous haemangioma, Dermoid cyst, Meningioma, Optic nerve glioma, Inverted papilloma, Angiofibroma.
- N – Neoplastic (Malignant): Rhabdomyosarcoma, Lymphoma, Leukaemia, Neuroblastoma, Sinonasal malignancies, Metastasis.
- C – Congenital: Dermoid cyst, Encephalocele, Neurofibromatosis.
- E – Endocrine: Thyroid eye disease (also in A).
1. Thyroid Eye Disease (Graves Ophthalmopathy)
Thyroid eye disease (Graves ophthalmopathy) is the most common cause of proptosis in adults, and it causes about 90% of bilateral proptosis cases. The disease develops due to an autoimmune reaction in the orbit. In this condition, T-cells enter the orbital tissues and activate fibroblasts. These fibroblasts produce glycosaminoglycans, which attract and retain water. As a result, extraocular muscles become swollen and orbital fat increases in volume. The inferior rectus and medial rectus muscles enlarge most commonly. Consequently, the orbital contents expand and push the eyeball forward, producing axial proptosis.
Clinically, lid retraction is the most common sign. Patients often show lid lag when they look downward. Proptosis usually occurs along the axis of the eye and is commonly bilateral, although it may appear asymmetric. In addition, patients may develop chemosis, periorbital oedema, and restricted eye movements. The restricted movement occurs due to fibrosis of the extraocular muscles, which often causes diplopia. Severe cases may lead to exposure keratopathy because the eyelids fail to close completely. Furthermore, about 5% of patients develop compression of the optic nerve, which can cause visual loss. Most patients (80–90%) have hyperthyroidism. However, some patients remain euthyroid or hypothyroid; normal thyroid tests do not rule out thyroid eye disease.
Radiology: CT scan of the orbit helps in diagnosis. It typically shows spindle-shaped enlargement of the muscle belly with sparing of the tendon, which helps differentiate it from idiopathic orbital inflammation, where both the muscle belly and tendon are involved.
2. Idiopathic Orbital Inflammation (Orbital Pseudotumor)
Idiopathic orbital inflammation, also called orbital pseudotumor, is a non-infectious inflammatory disease of the orbit with an unknown cause. The condition usually develops suddenly or within a few days to weeks. The inflammation may involve the entire orbit or may affect specific orbital structures. These structures include:
- Extraocular muscles → called orbital myositis
- Lacrimal gland → called dacryoadenitis
- Sclera → called scleritis
- Optic nerve sheath → called perineuritis
Clinical Features: The most important symptom is dull orbital pain, which becomes more severe during eye movements. This painful eye movement helps to differentiate idiopathic orbital inflammation from thyroid eye disease, which usually causes painless proptosis. About 70–80% of patients develop proptosis. In addition, patients often show periorbital oedema, redness (erythema), and restricted eye movements. Because of muscle involvement, diplopia may occur. In some cases, patients may also develop ptosis or visual loss, especially if the optic nerve becomes involved.
Radiology: CT scan with contrast helps confirm the diagnosis. The scan usually shows enlargement of the involved orbital structures. An important diagnostic feature is the involvement of both the extraocular muscle and its tendon attachment to the globe. This feature helps doctors distinguish idiopathic orbital inflammation from thyroid eye disease, where only the muscle belly enlarges while the tendon remains normal. Another helpful finding is the absence of bone erosion, which helps rule out malignant tumours of the orbit.
Management: Corticosteroids form the main treatment. Start oral corticosteroids, which produce a rapid and dramatic improvement in most patients. Reduce the steroid dose slowly to prevent recurrence of the disease. If patients do not respond to steroids, doctors may use other treatments such as Radiotherapy or Immunosuppressive drugs, including Rituximab, Cyclophosphamide or Cyclosporine.
3. Orbital Cellulitis and Subperiosteal Abscess
Orbital cellulitis is the most common cause of proptosis in children and is a medical emergency that requires immediate treatment. The infection usually spreads from the paranasal sinuses, especially the ethmoid sinus, through the thin lamina papyracea. This route accounts for about 90% of cases. In preseptal cellulitis, infection remains anterior to the orbital septum and involves only the eyelids. However, in orbital cellulitis, infection spreads behind the orbital septum, and proptosis becomes the key clinical feature.
Clinical features: Patients usually develop marked eyelid swelling and redness, along with chemosis and severe orbital pain. Eye movements often increase the pain. In addition, restricted eye movements (ophthalmoplegia) commonly occur. Many patients also show fever and systemic toxicity. If the infection affects the optic nerve, patients may develop visual loss and relative afferent pupillary defect (RAPD), which indicates a serious complication requiring urgent treatment.
Chandler’s Classification of Orbital Infections:
- Stage I – Preseptal cellulitis: Eyelid oedema/erythema, NO proptosis, normal vision and motility.
- Stage II – Orbital cellulitis: Proptosis + chemosis, restricted motility, normal or impaired vision.
- Stage III – Subperiosteal abscess: Proptosis + motility restriction, abscess on imaging, vision may be normal.
- Stage IV – Orbital abscess: Severe proptosis, complete ophthalmoplegia, vision loss, and abscess within the orbit.
- Stage V – Cavernous sinus thrombosis: Bilateral symptoms, cranial nerve palsies III, IV, VI, V₁, meningismus, sepsis.
Radiology. CT scan of the orbit with contrast is the investigation of choice. It helps to confirm the diagnosis, identify subperiosteal or orbital abscess, detect sinus infection and assess spread to the orbit or intracranial structures.
Management. Admit the patient, start intravenous antibiotics immediately.
- Medical treatment. Intravenous ceftriaxone, Vancomycin to cover resistant organisms and Metronidazole for anaerobic bacteria
- Surgical treatment. Perform surgical drainage in the following situations: Abscess diameter greater than 10 mm, no improvement after 48 hours of antibiotics, Development of visual impairment, Intracranial extension or suspected fungal infection. The preferred surgical procedure is endoscopic sinus surgery with drainage of the subperiosteal abscess. Early treatment prevents complications such as blindness, intracranial infection, and cavernous sinus thrombosis.
4. Rhinocerebral Mucormycosis
Rhinocerebral mucormycosis is a severe and life-threatening fungal infection that causes high morbidity and mortality. The disease became more common after the COVID-19 pandemic, especially in diabetic and immunocompromised patients. The infection occurs due to angioinvasive fungi belonging to the order Mucorales. The most common organisms include Rhizopus and Mucor species. These fungi invade blood vessels, cause thrombosis, and lead to tissue necrosis. Diabetic ketoacidosis (DKA) is the most important risk factor. The acidic environment in DKA promotes rapid fungal growth. Other risk factors include immunosuppression, high-dose steroid therapy, haematological malignancies and iron overload states.
Clinical features. The clinical presentation is dramatic, with rapidly progressive proptosis developing over hours to days. Patients develop periorbital oedema, complete ophthalmoplegia, and vision loss from optic nerve infarction. A black necrotic eschar on the palate or turbinates represents a pathognomonic late finding that should immediately alert the clinician. Facial pain and numbness along the trigeminal nerve distribution frequently accompany these symptoms. Diagnosis requires a KOH mount demonstrating broad, aseptate, ribbon-like hyphae branching at right angles, though a tissue biopsy confirming vascular invasion is essential.
Radiology. CT and MRI reveal sinus opacification, orbital invasion, and bony erosion. Management follows four essential pillars: urgent surgical debridement, removing all necrotic tissue, intravenous liposomal amphotericin B as first-line antifungal therapy, reversal of risk factors through strict glycaemic control, and supportive care. Despite aggressive treatment, mortality remains 50 to 80 percent.
5. Vascular Causes
- Cavernous haemangioma is the most common benign orbital tumour in adults, typically affecting women aged 40 to 60 years. It presents as painless, slowly progressive, unilateral axial proptosis. CT reveals a well-defined, intensely enhancing intraconal mass. Asymptomatic lesions may be observed, while symptomatic lesions require surgical excision through lateral orbitotomy.
- Capillary haemangioma represents the most common orbital tumour in infants, presenting at birth with rapid growth during the first year followed by spontaneous involution by age five to seven. Associated cutaneous strawberry naevi may be present. Oral propranolol is first-line treatment for vision-threatening lesions.
- Orbital varix characteristically causes intermittent proptosis that increases with Valsalva manoeuvre, diagnosed through CT venography with provocative testing. Carotid-cavernous fistula presents with the classic triad of pulsatile proptosis, audible bruit, and arterialized conjunctival vessels. Direct fistulas follow trauma, while indirect fistulas occur spontaneously in older women. Digital subtraction angiography is the gold standard for diagnosis, guiding endovascular embolization. Cavernous sinus thrombosis presents with bilateral proptosis, complete ophthalmoplegia, and fever, typically arising from midface or dental infections.
6. Benign Neoplastic Causes
- Dermoid cyst is the most common benign orbital tumour in children, arising from ectodermal tissue trapped along suture lines. Deep dermoids cause slowly progressive, painless proptosis with globe displacement. CT shows a cystic lesion with fat density and bony remodelling. Complete surgical excision with intact capsule is essential.
- Optic nerve glioma affects children aged two to eight years and is strongly associated with Neurofibromatosis type one. Patients present with slowly progressive axial proptosis accompanied by early visual loss. CT demonstrates fusiform optic nerve enlargement. Observation is appropriate for stable lesions. Optic nerve sheath meningioma affects middle-aged women, presenting with gradual visual loss and proptosis. The pathognomonic triad includes visual loss, optic atrophy, and optociliary shunt vessels. CT shows tram-track calcification. Radiotherapy is used for progressive tumours. Lacrimal gland pleomorphic adenoma causes downward and medial globe displacement, requiring complete excision through lateral orbitotomy.
7. Malignant Neoplastic Causes
- Rhabdomyosarcoma is the most common primary malignant orbital tumour in children, peaking at six to seven years. Rapidly progressive proptosis developing over days to weeks is the key feature. CT reveals an irregular enhancing mass with bony erosion. Treatment combines chemotherapy with the VAC regimen and radiotherapy, achieving 90 percent five-year survival for localized disease.
- Lymphoma is the most common malignant orbital tumour in adults, typically affecting women aged 50 to 70 years. Painless, slowly progressive proptosis with anterior salmon-patch conjunctival lesions is characteristic. CT shows a homogeneous mass moulding to contours without bone erosion. Isolated lesions respond to radiotherapy, while systemic disease requires R-CHOP chemotherapy. Metastatic tumours most commonly originate from breast cancer in women and lung cancer in men, presenting with rapidly progressive proptosis and pain. Sinonasal malignancies, particularly squamous cell carcinoma, invade the orbit through the lamina papyracea or orbital floor, causing proptosis with direction-specific globe displacement.
8. Sinus-Related Causes
Mucocele is a benign expansile lesion from obstructed sinus ostium, most commonly affecting the frontal sinus followed by the ethmoid. Slowly progressive, painless proptosis with globe displacement occurs as the lesion erodes into the orbit. CT demonstrates an expansile mass with sinus opacification and bony remodelling. Endoscopic marsupialization establishing wide nasal drainage is the treatment of choice. Juvenile nasopharyngeal angiofibroma affects adolescent males, spreading from the pterygopalatine fossa to the orbit and presenting with proptosis, nasal obstruction, and epistaxis.
9. Traumatic Causes
Retrobulbar haemorrhage is an ophthalmic emergency presenting with acute, painful proptosis developing over minutes to hours. The orbit feels rock-hard on palpation, and rapid vision loss occurs from optic nerve compression. Immediate lateral canthotomy and cantholysis provides emergency decompression, supplemented by intravenous mannitol and acetazolamide. Orbital emphysema results from air entering the orbit through a sinus fracture, causing proptosis after nose blowing that is usually self-limiting.
——– End of the Chapter——–
NEET PG-Style MCQs with Answers
1. A 45-year-old female presents with bilateral proptosis, lid retraction, and lid lag. On CT scan, there is enlargement of the extraocular muscles. Which of the following findings would most strongly suggest Graves’ ophthalmopathy over orbital pseudotumor?
- a) Involvement of the lateral rectus muscle
- b) Involvement of the muscle tendon
- c) Sparing of the muscle tendon
- d) Presence of pain on eye movements
Answer: c) Sparing of the muscle tendon
2. A 6-year-old boy presents with rapidly progressive, painless proptosis of the right eye over 2 weeks. What is the most likely diagnosis?
- a) Cavernous Hemangioma
- b) Retinoblastoma
- c) Dermoid Cyst
- d) Rhabdomyosarcoma
Answer: d) Rhabdomyosarcoma
3. Which of the following is the most common benign orbital tumour in adults?
- a) Cavernous Hemangioma
- b) Capillary Hemangioma
- c) Pleomorphic Adenoma of the lacrimal gland
- d) Schwannoma
Answer: a) Cavernous Hemangioma
4. A patient presents with pulsatile proptosis and a bruit on auscultation over the eye. The most likely diagnosis is:
- a) Orbital varix
- b) Carotid-cavernous fistula
- c) Optic nerve glioma
- d) Frontal mucocele
Answer: b) Carotid-cavernous fistula
5. On CT scan, a lesion causing fusiform enlargement of the medial rectus muscle, including its tendon. The most likely diagnosis is:
- a) Graves’ ophthalmopathy
- b) Orbital pseudotumor
- c) Lymphoma
- d) Rhabdomyosarcoma
Answer: b) Orbital pseudotumor
6. A 60-year-old female presents with painless, gradually progressive proptosis. Examination reveals a firm, non-tender mass in the superior orbit. CT shows a well-defined, round, intraconal mass that enhances with contrast. What is the most appropriate management?
- a) Immediate radiotherapy
- b) Lateral orbitotomy and excision
- c) Systemic corticosteroids
- d) Endoscopic biopsy
Answer: b) Lateral orbitotomy and excision
7. An 8-year-old child presents with a slowly growing mass at the outer aspect of the right eyebrow, causing downward and medial displacement of the globe. It is firm, non-tender, and non-pulsatile. The most likely diagnosis is:
- a) Dermoid cyst
- b) Capillary hemangioma
- c) Rhabdomyosarcoma
- d) Lymphangioma
Answer: a) Dermoid cyst
8. A known case of breast carcinoma presents with unilateral proptosis. The most likely mechanism is:
- a) Direct extension from a sinus tumour
- b) Metastasis to the orbit
- c) Secondary infection causing orbital cellulitis
- d) Paraneoplastic syndrome
Answer: b) Metastasis to the orbit
9. Which of the following is a feature of orbital pseudotumor?
- a) Fusiform enlargement of extraocular muscles with tendon involvement
- b) Bilateral, symmetric proptosis
- c) Dramatic response to radiotherapy
- d) Association with hyperthyroidism
Answer: a) Fusiform enlargement of extraocular muscles with tendon involvement
10. The first-line treatment for a confirmed case of idiopathic orbital inflammation (orbital pseudotumor) is:
- a) Broad-spectrum antibiotics
- b) Surgical debulking
- c) Oral corticosteroids
- d) Observation alone
Answer: c) Oral corticosteroids
Clinical Case Scenarios for Viva or Practical Exams
Scenario 1: A 55-year-old male, a known diabetic for 15 years with poor control, presents with progressive proptosis, periorbital swelling, and blackish discolouration of the skin over the nose. He complains of diplopia and has reduced vision.
Question: What is your most probable diagnosis and why?
Answer: Rhinocerebral Mucormycosis. This is a life-threatening fungal infection seen in immunocompromised hosts, especially uncontrolled diabetics. The blackish discolouration (eschar) is a sign of tissue necrosis due to angioinvasion by the fungus. Urgent endoscopic debridement and systemic antifungals (Amphotericin B) are required.
Scenario 2: A 30-year-old woman presents with a 3-month history of discomfort and protrusion of her left eye. On examination, you note left axial proptosis. There is mild pain on eye movements. A CT scan shows a diffusely enhancing lesion in the intraconal space with enlargement of the lateral rectus muscle, involving both the belly and its tendon.
Question: What are your top two differential diagnoses, and how would you differentiate them?
Answer: The top two are Orbital Pseudotumor and Graves’ Ophthalmopathy. The key differentiator is the tendon involvement. Since the CT shows tendon involvement, this strongly favours Orbital Pseudotumor. Graves’ disease spares the tendons. A thyroid function test (TFT) would be normal or show euthyroid or hypothyroid status in pseudotumor, whereas it is often abnormal in Graves’. A trial of oral steroids would also be diagnostic, as pseudotumor responds dramatically.
Scenario 3: A 65-year-old female presents with gradually progressive, painless proptosis of the right eye. On examination, a firm, smooth mass is palpable just above the medial canthus. Her vision is normal. CT scan shows a well-defined, extraconal mass with no bone erosion.
Question: What is the most likely diagnosis, and what is the next step in management?
Answer: Given the age, painless progression, and anterior location, the most likely diagnosis is Orbital Lymphoma. While a dermoid is possible, it is less common at this age. The next step is to perform a biopsy of the lesion for histopathological and immunohistochemical analysis to confirm the diagnosis and subtype the lymphoma. Following the biopsy, a systemic workup is needed to rule out systemic disease before planning radiotherapy or chemotherapy.
Frequently Asked Questions in Viva
- What is the difference between proptosis and exophthalmos? Proptosis is the general term for forward displacement of the eye. Exophthalmos is often used specifically to describe proptosis caused by Graves’ disease (thyroid eye disease), though the terms are frequently used interchangeably in clinical practice.
- What is the VEIN mnemonic for causes of proptosis? VEIN stands for: Vascular (for example, hemangioma), Endocrine (Graves’ disease), Inflammatory (orbital pseudotumor), and Neoplastic (for example, lymphoma, rhabdomyosarcoma). It is a useful way to remember the broad categories.
- How can you clinically differentiate between true proptosis and pseudoproptosis? Look for signs of contralateral enophthalmos (sunken eye from old trauma) or lid retraction. A simple test is to ask the patient to look up; in true proptosis, sclera becomes visible above the cornea, which is not typically seen in pseudoproptosis due to a wide palpebral aperture.
- Which investigation is best for diagnosing the cause of proptosis? A CT scan of the orbit is the initial investigation of choice. It provides excellent detail of bony structures, helps localise the lesion (intraconal versus extraconal), and can differentiate between conditions like Graves’ disease and orbital pseudotumor based on muscle involvement.
- What is the most common cause of bilateral proptosis? Graves’ ophthalmopathy (Thyroid Eye Disease) is overwhelmingly the most common cause of bilateral proptosis in adults.
- What are the differences between orbital pseudotumor and Graves’ ophthalmopathy on CT scan? In Graves’ disease, there is fusiform enlargement of the extraocular muscle bellies with sparing of the tendons. In orbital pseudotumor (myositis variant), both the muscle belly and its tendon are enlarged and inflamed.
- When is orbital decompression surgery required? Orbital decompression is indicated primarily for two reasons in Graves’ ophthalmopathy: 1) to relieve pressure on the optic nerve (compressive optic neuropathy) causing vision loss, and 2) to allow the eye to settle back into the orbit to treat severe exposure keratopathy (corneal drying and ulceration) from extreme proptosis.
——– End——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Proptosis Ent Notes For Mbbs Students, Proptosis Causes Mnemonic Vein, Proptosis Ent Exam Guide, Proptosis Differential Diagnosis Mbbs, Proptosis Evaluation Steps Ent, Proptosis Measurement Exophthalmometer Notes, Proptosis Neet Pg Mcqs, Proptosis Clinical Features And Causes, Proptosis Orbit Tumors Summary, Proptosis Ent Viva Questions, Proptosis Orbital Cellulitis Notes, Proptosis Graves Ophthalmopathy Notes, Proptosis Cavernous Hemangioma Ent, Proptosis Dermoid Cyst Orbit, Proptosis Rhabdomyosarcoma Ent Exam, Proptosis Sinus Tumors Orbit, Proptosis Diagnosis Ct Mri Orbit, Proptosis Management Ent Residents Guide, Proptosis High Yield Revision Notes, Proptosis Mbbs Ent Short Notes, Proptosis causes mnemonic, Exophthalmos vs proptosis, Proptosis evaluation and management, Proptosis differential diagnosis, Proptosis NEET PG questions, Orbital pseudotumor vs Graves disease, Orbital tumors in children, Cavernous hemangioma orbit, Rhabdomyosarcoma proptosis, Orbital lymphoma treatment, Proptosis clinical case presentation, Proptosis viva questions, Thyroid eye disease proptosis, Unilateral proptosis causes, Proptosis CBME notes, Proptosis imaging CT MRI, Carotid cavernous fistula proptosis, Orbital cellulitis proptosis, Proptosis surgery decompression, Proptosis high yield points.