|
The following CBME core competencies are covered in this chapter.
|
Malignant Tumours of Nose and Paranasal Sinuses
Introduction: Why Sinonasal Malignancies Matter in Clinical Practice
Sinonasal malignancies are rare but clinically critical cancers that every ENT student must master. These tumours account for less than 3% of all aerodigestive tract cancers and approximately 0.44% of all body cancers in India. However, their importance in ENT practice extends far beyond these numbers. The real challenge lies in their deceptive presentation – they initially mimic chronic rhinosinusitis so perfectly that patients often receive repeated medical treatment for months before the correct diagnosis emerges. Consequently, the average diagnostic delay reaches 6 to 8 months, and this delay directly worsens the prognosis. Furthermore, these tumours frequently invade the orbit, skull base, cranial nerves, and oral cavity by the time of diagnosis, making them surgically challenging and prognostically ominous.
Fundamentals and Epidemiology
The sinonasal tract exhibits remarkable histological diversity because it contains respiratory epithelium, olfactory epithelium, minor salivary glands, melanocytes, and lymphoid tissue. This diversity explains why so many different malignant tumour types arise in this region, ranging from carcinoma to melanoma to sarcoma. Sinonasal malignancies most commonly affect men in their 5th to 6th decades of life, though specific tumour types show different age distributions. Among the paranasal sinuses, the maxillary sinus is the most frequent site, accounting for 70% of cases. The ethmoid sinus follows at 20%, while the sphenoid and frontal sinuses together constitute the remaining 10% (3% and 1% respectively). Therefore, when a clinician suspects a sinonasal malignancy, the maxillary sinus deserves the closest attention.
Aetiology
The aetiology is strongly linked to environmental and occupational exposures:
- Wood Dust: Hardwood exposure (e.g., beech, oak) is specifically linked to Adenocarcinoma of the ethmoid sinuses and upper nasal cavity, whereas softwood exposure is associated with Squamous Cell Carcinoma. African mahogany appears to be the most carcinogenic wood species. Interestingly, Bantu tribe men who burn this wood have the highest incidence of maxillary sinus cancer worldwide.
- Industrial Chemicals: Workers in nickel refining, leather tanning, and those exposed to chromium, mustard gas, or isopropyl oil face a significantly higher risk.
- Other Factors: Smoking, chronic radiation exposure, and viral infections (such as HPV and EBV) play contributory roles.
- Racial predilection: Whites show a higher incidence compared to other races.
Histological Types of Sinonasal Malignancy
The sinonasal tract produces an extraordinary variety of malignant tumours, but one type dominates clinical practice. Squamous cell carcinoma constitutes 80% of all sinonasal malignancies. These are common and important tumours:
- Squamous cell carcinoma (most common)
- Adenocarcinoma
- Adenoid cystic carcinoma
- Sinonasal undifferentiated carcinoma (SNUC)
- Esthesioneuroblastoma (olfactory neuroblastoma)
- Mucosal malignant melanoma
- Lymphomas (especially NK/T-cell lymphoma)
- Sarcomas (chondrosarcoma, rhabdomyosarcoma, osteosarcoma)
Table: Histological Types of Sinonasal Malignancy
| Tumour Type | Percentage | Key Feature | Prognostic Note |
| Squamous Cell Carcinoma | 80% | Most common overall | Better prognosis than most others |
| Adenocarcinoma | 5-10% | Woodworker’s tumour | Radioresistant, needs surgery |
| Adenoid Cystic Carcinoma | 5-10% | Perineural spread | Good 5-year, poor 20-year survival |
| Malignant Melanoma | <5% | Anterior septum location | 28% 5-year survival |
| Esthesioneuroblastoma | 3-5% | Olfactory epithelium origin | Bimodal age peaks |
| Lymphoma | 6% | EBV-associated (T/NK type) | Variable by subtype |
| Chondrosarcoma | Rare | Septum or alveolus origin | Indolent but relentless |
1. Squamous Cell Carcinoma:
Squamous cell carcinoma arises from three distinct sites within the nasal cavity, and each site shows characteristic behaviour patterns.
- Vestibular Squamous Cell Carcinoma arises from the lateral wall of the nasal vestibule and may extend into the columella, nasal floor, and upper lip. Metastases typically spread to parotid nodes rather than cervical nodes, a unique feature that students must remember for examinations.
- Septal Squamous Cell Carcinoma arises mostly from the mucocutaneous junction and causes burning and soreness in the nose. Physicians often term this “nose-picker’s cancer” because chronic trauma may contribute to its development. Fortunately, it usually demonstrates low-grade malignancy and carries a relatively favourable prognosis.
- Lateral Wall Squamous Cell Carcinoma represents the most commonly involved site. The tumour easily extends into the ethmoid or maxillary sinuses and grossly presents as a polypoid mass. Unlike other head and neck squamous cell carcinomas, metastases remain rare in early stages.
Treatment and Prognosis for Squamous Cell Carcinoma: Combined radiotherapy and surgery form the mainstay of treatment. For poorly differentiated or undifferentiated sinonasal carcinomas, chemoradiation alone may prove curative. However, when the nasal septum or columella serves as the primary site, the prognosis becomes particularly poor due to the possibility of bilateral metastatic spread to cervical nodes.
2. Adenocarcinoma: The Woodworker’s Tumour
Adenocarcinoma shows a well-recognised association with occupational exposure, with over 30% of patients being woodworkers. These tumours usually arise in the middle meatus and spread into the ethmoid sinus. They may also spread anteriorly to present as a mass in the glabella or posteriorly into the sphenoethmoidal recess and nasopharynx. Differentiation ranges from high to low grade with commensurate effects on outcome. Adenocarcinoma is generally rather radioresistant, so combined therapy is usually offered. Many patients require craniofacial resection, though selected cases have been treated successfully by endoscopic resection.
3. Adenoid Cystic Carcinoma
Adenoid cystic carcinoma is well known for its propensity to spread along perineural lymphatics, which compromises attempts at curative excision. It can also embolize along these routes and produce blood-borne metastases, classically to the lung, while lymphatic spread remains rare. The natural history can be deceptively long, with good five-year survival figures reaching 70-80%. However, progressive loss occurs with time, and at 20 years, survival drops to 5% or less. Therefore, all patients eventually die from this disease unless some other event intervenes first. Treatment generally combines surgery and radiotherapy, though evidence that radiotherapy adds any additional chance of cure remains lacking; rather, it delays recurrence.
4. Malignant Melanoma
Malignant melanoma typically affects persons around 50 years of age with equal sex distribution. Within the nasal cavity, the anterior nasal septum is the most frequent site, followed by the middle and inferior turbinates. The tumour spreads by both lymphatics and bloodstream, and cervical nodal metastases may be present at initial examination.
Key Clinical Feature: The tumour exhibits an immunological symbiosis with its host, meaning some patients may survive for extended periods with residual disease while others become overwhelmed within weeks. Consequently, endoscopic resection proves to be as effective as more radical procedures, and craniofacial resection is contraindicated. The role of radiotherapy remains debated but may confer a small advantage. Five-year actuarial survival is approximately 28%, falling to 20% at ten years.
5. Esthesioneuroblastoma: The Olfactory Tumour
Esthesioneuroblastoma, also called olfactory neuroblastoma, arises from the olfactory epithelium in the upper third of the nose and shows bimodal incidence peaks at 10-20 years and 50-60 years. The most common symptoms include unilateral nasal obstruction and epistaxis. When the tumour invades the orbit and surrounding structures, additional symptoms like proptosis, headache, epiphora, diplopia, and blurred vision may arise. Lymph node metastases in the neck occur in 10-15% of cases.
- Examination Findings: Intranasal endoscopic examination reveals a friable, cherry-red, polypoidal mass in the upper third of the nasal cavity. Because this is a highly vascular tumour, biopsy should never be attempted unless imaging studies have been completed first.
- Diagnostic Imaging: High-resolution CT shows the extent of the lesion and may demonstrate destruction or erosion of the cribriform plate or orbital wall. MRI with contrast reveals extension into the orbit or intracranial compartment.
- Treatment Protocols: Treatment protocols vary between institutions but generally include craniofacial resection with adjuvant radiation, preoperative radiation followed by craniofacial resection, or preoperative chemotherapy and radiation followed by craniofacial resection for advanced lesions extending to the orbit, cribriform plate, and intracranial compartment. Neck nodes, if present, are also irradiated.
6. Lymphoma
Lymphomas comprise approximately 6% of malignant sinonasal tumours, though less than 1% of all lymphomas occur in this area. B-cell tumours present as an infiltrating indurated mass often affecting the external nose and soft tissues. T/NK-cell tumours associate with Epstein-Barr virus exposure and therefore appear more common in the Far East and parts of India. They produce aggressive, destructive lesions of the midface, previously referred to as “midline granuloma.”
Diagnostic Challenge: The most important consideration is obtaining representative tissue and alerting the pathologist about the suspected diagnosis, as this can prove difficult in the presence of significant inflammation and necrosis. Once diagnosed, full staging is undertaken, and treatment follows established chemoradiotherapy regimes depending on the extent of spread.
7. Chondrosarcoma
Chondrosarcomas arise in the nasal cavity, often from the septum or maxillary alveolus, and spread superiorly into the skull base and inferiorly into the palate. They may be multifocal and often pursue an indolent course of frequent recurrence over many years. The term “chondroma” should not be used because these tumours are associated with high morbidity as cranial nerves become involved, sometimes bilaterally, and death results from uncontrolled local intracranial disease. The age range includes both young and old, and the tumour is generally more aggressive in younger patients. Craniofacial resection usually offers the best oncologic approach, particularly because these tumours are not radiosensitive.
Mesenchymal Chondrosarcoma: This particularly aggressive and fortunately rare form can affect the nose and sinuses. It affects the young, metastasises to nodes and bone, and despite radical medical and surgical oncologic treatment, few survivors exist.
Patterns of Spread of Sinonasal Malignancies
Understanding spread patterns proves essential for accurate staging and treatment planning. Sinonasal malignancies spread through three primary routes: direct extension, lymphatic dissemination, and hematogenous metastasis.
- Lymphatic Spread Pattern. The anteroinferior part of the nasal cavity and the skin of the nasal vestibule drain into the facial, parotid, and submandibular lymph nodes. Therefore, tumours in this region may present with enlarged nodes in these areas. The remainder of the posterior nasal cavity and paranasal sinuses drain into the retropharyngeal nodes, which subsequently drain to the upper deep cervical chain. Consequently, cervical nodal metastases typically appear late in the disease course because the retropharyngeal nodes remain inaccessible to palpation.
- Hematogenous Metastasis. Distant metastasis can occur to bone, brain, liver, lung, and skin. These metastases usually manifest in advanced stages and significantly worsen the prognosis.
- Direct Extension Routes. Each sinus has characteristic spread patterns that produce specific clinical syndromes. The maxillary sinus, being most commonly involved, demonstrates the most well-described patterns, which we will cover in detail in the clinical presentation section.
Clinical Presentation – From Early Symptoms to Late Signs
The Diagnostic Challenge: Why Diagnosis Is Often Delayed
The clinical presentation evolves from early nonspecific symptoms to late characteristic findings depending on the direction of tumour spread. Recognising this evolution helps in early diagnosis. Initial symptoms mimic chronic rhinosinusitis so closely that clinicians often miss the malignant diagnosis. These early symptoms include unilateral nasal obstruction, intermittent epistaxis (blood-stained nasal discharge), epiphora (watering from the eye), cheek swelling or discomfort, and loosening of teeth or poor fitting of dentures.
Therefore, any unilateral sinusitis that fails to respond to appropriate medical therapy should raise suspicion for malignancy, especially in older patients with occupational risk factors.
Late Features Based on Spread Direction (Maxillary Sinus Carcinoma)
- Medial Spread into Nasal Cavity: When the tumour spreads medially, it produces progressive nasal obstruction, persistent nasal discharge, and recurrent epistaxis. The tumour may also extend into the anterior and posterior ethmoid sinuses, creating an antroethmoidal tumour complex.
- Anterior Spread: Anterior extension causes swelling of the cheek, which may later ulcerate or fungate through the facial skin. This presentation often prompts earlier medical attention, paradoxically leading to earlier diagnosis despite representing advanced local disease.
- Posterior Spread: Posterior extension into the pterygopalatine and infratemporal fossa involves the pterygoid muscles, leading to trismus (difficulty opening the mouth). This finding indicates advanced disease and suggests a poor prognosis because complete surgical resection becomes nearly impossible.
- Inferior Spread: Inferior extension produces palatal swelling, ulceration, or fungation. Dental manifestations include pain, gum swelling, loosening of teeth, and poor fitting of dentures. These symptoms often lead patients to consult dentists first, creating an opportunity for early diagnosis if the dentist maintains appropriate suspicion.
- Superior Spread: Superior extension into the orbit causes proptosis (forward displacement of the eyeball), diplopia (double vision), ocular pain, swelling, and epiphora. Spread to the foramen rotundum involves the maxillary nerve, producing cheek anaesthesia. Further involvement of the orbital apex leads to vision loss, representing very advanced disease.
- Intracranial Spread: Intracranial extension occurs most commonly through the ethmoid sinus and cribriform plate, involving the anterior cranial fossa. Alternatively, spread through the sphenoid sinus can reach the middle cranial fossa. Intracranial extension generally precludes curative resection.
Staging and Classification Systems
Several classification systems help stage sinonasal malignancies, but the AJCC TNM system remains the most clinically useful for treatment planning and prognosis prediction. However, understanding older systems like Ohngren’s classification helps students appreciate prognostic concepts and answer examination questions.
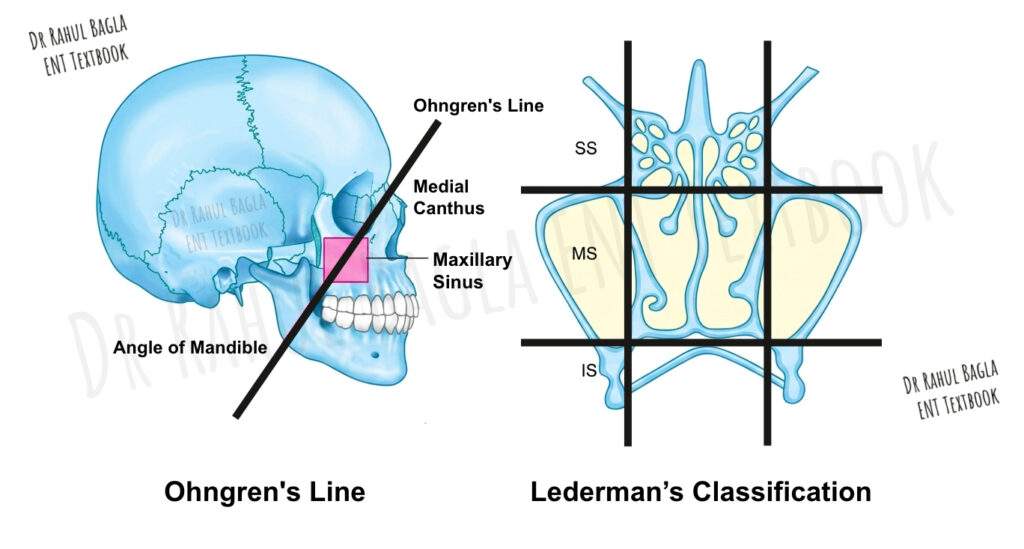
Ohngren’s Classification: The Prognostic Line
Ohngren’s line forms the basis of this clinically useful classification. This imaginary line joins the medial canthus of the orbit to the angle of the mandible, thereby dividing the maxilla into two distinct prognostic zones.
- Suprastructure (Above the line): Tumours lying in the suprastructure carry a poor prognosis because they remain close to vital structures like the orbit and brain. These tumours often present with orbital or intracranial symptoms and have limited surgical options.
- Infrastructure (Below the line): Tumours in the infrastructure have a better prognosis because they remain amenable to surgical treatment and lack proximity to critical structures. These tumours typically present with dental or palatal symptoms and allow more complete resection.
Lederman’s Classification
This system uses two horizontal lines of Sebileau to divide the paranasal sinuses into three parts. The first line passes through the floor of the orbit, and the second line passes through the floor of the nose.
- Suprastructure: Includes the ethmoid, sphenoid, and frontal sinuses, along with the olfactory area of the nose
- Mesostructure: Includes the maxillary sinus and the respiratory part of the nose
- Infrastructure: Contains the upper alveolar processes
Important Note: The suprastructure and infrastructure in Lederman’s classification do not correspond to the same structures in Ohngren’s classification. Students must avoid confusing these two systems, as this is a common examination trap.
Mnemonic to Remember the Difference
- Ohngren’s Line runs Oblique (medial canthus to angle of the mandible)
- Lederman’s Lines run Level (horizontal, through orbital floor and nasal floor)
AJCC TNM Classification for Maxillary Sinus
The American Joint Committee on Cancer provides a detailed TNM system specifically for squamous cell carcinoma of the maxillary sinus. This system does not apply to non-epithelial tumours of lymphoid tissue, soft tissue, cartilage, or bone.
Table: T Categories for Maxillary Sinus
| T Category | Description |
| Tis | Carcinoma in situ |
| T1 | Tumour restricted to any one subsite, with or without bony invasion |
| T2 | Tumour invading two subsites in a single region or extending to involve an adjacent region within the nasoethmoidal complex, with or without bony invasion |
| T3 | Tumour extends to invade the medial wall or floor of the orbit, maxillary sinus, palate, or cribriform plate |
| T4a | Tumour invades anterior orbital contents, skin of nose or cheek, minimal extension to anterior cranial fossa, pterygoid plates, sphenoid, or frontal sinuses |
| T4b | Tumour invades orbital apex, dura, brain, middle cranial fossa, cranial nerves other than V2, nasopharynx, or clivus |
Table: N Categories for Maxillary Sinus
| N Category | Description |
| N0 | No regional lymph node metastasis |
| N1 | Single ipsilateral lymph node, 3 cm or less |
| N2a | Single ipsilateral lymph node, 3-6 cm |
| N2b | Multiple ipsilateral lymph nodes, none >6 cm |
| N2c | Bilateral or contralateral lymph nodes, none >6 cm |
| N3 | Any lymph node >6 cm |
Table: Stage Grouping for Maxillary Sinus
| Stage | T Category | N Category | M Category |
| I | T1 | N0 | M0 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0 OR T1-3 with N1 |
| IVA | T4a | N0-1 | M0 |
| IVB | T4b | N2-3 | M0 |
| IVC | Any T | Any N | M1 |
Diagnostic Approach
A systematic diagnostic approach combining imaging, endoscopy, and histopathology yields the highest diagnostic accuracy. The sequence matters greatly: imaging must precede biopsy to prevent distortion of tumour architecture and to identify vascular lesions that could cause catastrophic bleeding.
Imaging Studies
- Computed Tomography (CT): CT scan excels at visualising bony expansion, erosion, remodelling, or destruction. Therefore, it remains the primary imaging modality for assessing bony involvement. CT also detects calcium deposits in tumours like esthesioneuroblastoma, chondrosarcoma, and osteosarcoma. The key areas requiring evaluation on CT include the cribriform plate, fovea ethmoidalis, posterior wall of the maxillary sinus, pterygopalatine fossa, sphenoid sinus, and posterior table of the frontal sinus.
- Magnetic Resonance Imaging (MRI): MRI offers multiplanar capability and lacks radiation exposure, making it valuable for specific indications. It provides excellent delineation of tumour margins, inflammatory tissue, and secretions. Approximately 95% of sinonasal tumours demonstrate low to intermediate signal intensity on both T1 and T2 imaging. For orbital extension assessment, T1 with fat suppression MRI proves essential. MRI can also delineate thickened enhancing dura (suggesting extradural periosteal invasion), brain oedema (indicating intradural spread), and nerve enhancement (showing perineural spread).
- Positron Emission Tomography (PET-CT): Whole body PET-CT serves two main purposes: detecting pretreatment distant metastasis and performing post-treatment surveillance for recurrence.
Biopsy Techniques
Nasal endoscopic biopsy represents the preferred method for tissue diagnosis. This approach allows direct visualisation and precise sampling while avoiding tumour spillage. The Caldwell-Luc approach should be avoided because it can lead to tumour spread through the surgical tract.
Critical Safety Points:
- The biopsy must be performed in an operating theatre setting because certain vascular tumours may bleed excessively and require nasal packing
- Radiologic imaging must precede biopsy to prevent distortion of tumour architecture and to identify vascular lesions
- For suspected esthesioneuroblastoma or melanoma, imaging before biopsy is particularly critical due to their vascular nature
Treatment and Management
Treatment planning depends on histological type, tumour stage, patient factors, and institutional expertise. A multidisciplinary approach involving surgical oncology, radiation oncology, and medical oncology yields the best outcomes. Modern management emphasises organ preservation when possible while maintaining oncologic safety.
Surgical Approaches for Maxillary Tumours
- Partial Maxillectomy: Medial maxillectomy: Clearance of the medial wall of the nose, including the ethmoid sinus. Inferior maxillectomy: Hard palate resection along with the adjacent alveolus
- Total Maxillectomy: This procedure involves the complete removal of the maxilla. Surgical approaches include lateral rhinotomy (Moure’s incision) for exposure and Weber-Ferguson incision (lip-splitting with infraorbital extension) for total maxillectomy. Midfacial degloving combines bilateral sublabial incision with elevation of facial skin off the nasal vault, though the superior extent remains limited by the infraorbital nerve.
- Extended Maxillectomy: This removes structures beyond the maxilla, including skin, orbit, or dura when involved.
- Endoscopic Excision: This approach works well for limited tumours. However, contraindications include soft tissue or skin involvement, dural involvement lateral to the orbit, significant brain invasion, internal carotid artery encasement, mandible involvement, or cavernous sinus involvement.
Orbital Management. Minimal involvement of the orbital periosteum and limited fat of the periorbita does not warrant orbital exenteration. Orbital exenteration is indicated only when the tumour involves the orbital apex, extraocular muscles, conjunctiva, or sclera. Crucial Note: Orbital exenteration should not be performed when the clearance of malignancy remains incomplete in the rest of the nose and paranasal sinuses, as this would subject the patient to unnecessary morbidity without curative benefit.
Craniofacial Resection. When the tumour involves the skull base and paranasal sinuses, en bloc tumour removal requires craniofacial resection. This combined neurosurgical and otolaryngology procedure allows complete resection of tumours extending into the anterior cranial fossa. It represents the standard of care for tumours with limited intracranial extension.
Radiotherapy
Radiotherapy serves multiple roles in sinonasal malignancy management. It combines with surgery for advanced resectable lesions, typically delivering 5000-5500 cGy preoperatively or postoperatively. As a single modality, radiotherapy treats advanced unresectable lesions or patients unwilling or unable to undergo surgery.
Indications of Unresectability: A tumour is considered unresectable when it involves bilateral optic nerves, significant frontal lobe, prevertebral fascia, or cavernous sinus.
Modern Techniques: Three-dimensional conformal radiotherapy and intensity-modulated radiotherapy (IMRT) cover larger tumour volumes while reducing side effects to optic nerves and lens by providing accurate and homogenous radiation dose delivery.
Chemotherapy
Chemotherapy plays a specific role in certain histological types. It proves valuable in olfactory neuroblastoma, rhabdomyosarcoma, and lymphoma. Chemoradiation (concomitant chemotherapy and radiation) has been used for large and inoperable tumours, with some studies reporting 5-year survival exceeding 60%. Intra-arterial infusion of 5-fluorouracil or cisplatin with concomitant radiation has also shown good results while avoiding the deformities associated with extensive surgery.
Prognosis and Survival
Overall Outcomes
Overall five-year survival for sinonasal malignancies ranges from 40-50%. Survival diminishes significantly with advancing tumour stage. However, advances in multimodal therapy and improved radiation delivery techniques offer hope for better results while protecting the lens and optic nerve from injury.
Factors Affecting Prognosis
- Tumour site: Infrastructure tumours have a better prognosis than suprastructure tumours
- Histological type: Squamous cell carcinoma carries a better prognosis than adenoid cystic carcinoma or melanoma
- Stage at presentation: Early-stage disease has significantly better outcomes
- Surgical margins: Negative margins improve survival dramatically
- Lymph node involvement: Nodal metastases worsen prognosis considerably
—-End of the Chapter—-
High-Yield Points for NEET PG and University Exams
- Most common sinonasal malignancy overall: Squamous cell carcinoma (80%)
- Most common sinus involved: Maxillary sinus (70%)
- Most common site within nasal cavity for melanoma: Anterior nasal septum
- Wood dust exposure most strongly linked to: Adenocarcinoma of ethmoid sinuses
- Tumour with perineural spread and late distant metastases: Adenoid cystic carcinoma
- Tumour with bimodal age distribution (10-20 and 50-60 years): Esthesioneuroblastoma
- EBV-associated aggressive midface destructive lesion: T/NK-cell lymphoma
- Ohngren’s line joins: Medial canthus to angle of mandible
- Suprastructure tumours (above Ohngren’s line) have: Poor prognosis
- Most important investigation before biopsy: Imaging (CT or MRI)
- Contraindication to biopsy without prior imaging: Esthesioneuroblastoma (vascular)
- Tumour that should NOT undergo craniofacial resection: Malignant melanoma
- Most common metastatic site for adenoid cystic carcinoma: Lung
- Trismus in maxillary sinus cancer indicates: Posterior spread to the pterygoid muscles
- Five-year survival for sinonasal malignancies: 40-50%
NEET PG Style MCQs
- A 60-year-old woodworker presents with unilateral nasal obstruction and blood-stained discharge for 6 months. He has tried multiple antibiotics without relief. Most likely diagnosis: A. Allergic fungal sinusitis B. Chronic rhinosinusitis C. Sinonasal adenocarcinoma D. Nasal polyp
- A 55-year-old patient with maxillary sinus carcinoma develops difficulty opening the mouth. This indicates spread to which structure: A. Orbit B. Pterygoid muscles C. Hard palate D. Cribriform plate
- Which tumour is classically associated with perineural spread and late pulmonary metastases: A. Squamous cell carcinoma B. Malignant melanoma C. Adenoid cystic carcinoma D. Esthesioneuroblastoma
- A cherry-red friable mass in the upper nasal cavity of a 15-year-old boy. Biopsy before imaging is contraindicated because: A. It may cause CSF leak B. The tumour is highly vascular C. It may seed the needle tract D. The tumour is radioresistant
- According to Ohngren’s classification, a tumour above the line joining the medial canthus to the angle of the mandible has: A. Better prognosis B. Poor prognosis C. Same prognosis as below line D. Cannot predict prognosis
- Most common histological type of sinonasal malignancy: A. Adenocarcinoma B. Squamous cell carcinoma C. Lymphoma D. Melanoma
- A patient with sinonasal malignancy develops cheek anaesthesia. Which nerve is involved: A. Ophthalmic nerve (V1) B. Mandibular nerve (V3) C. Maxillary nerve (V2) D. Facial nerve
- Which sinonasal tumour shows immunological symbiosis with the host: A. Squamous cell carcinoma B. Malignant melanoma C. Adenoid cystic carcinoma D. Chondrosarcoma
- Twenty-year survival rate for adenoid cystic carcinoma is approximately: A. 50% B. 30% C. 5% or less D. 70%
- Orbital exenteration is indicated when tumour involves: A. Orbital periosteum only B. Limited periorbital fat C. Orbital apex or extraocular muscles D. Any orbital extension
MCQ Answers:
- C. 2. B. 3. C. 4. B. 5. B. 6. B. 7. C. 8. B. 9. C. 10. C.
Clinical Case Scenarios for Practical Exams and Viva
Case 1. A 58-year-old male carpenter presents with 7 months of progressive left-sided nasal obstruction, intermittent blood-stained discharge, and recent onset of left cheek swelling. He has been treated for “sinusitis” three times with no improvement. He has no significant past medical history. Most likely diagnosis: Sinonasal malignancy, likely adenocarcinoma given occupational exposure. Best next step: Non-contrast CT of paranasal sinuses followed by endoscopic biopsy if imaging suggests resectable disease. Key examination point: Look for cheek tenderness, hard palate involvement, and cervical lymph nodes.
Case 2. A 52-year-old female presents with double vision, left eye proptosis, and numbness over her left cheek for 2 months. Nasal endoscopy reveals a friable mass in the left middle meatus. CT shows erosion of the medial orbital wall and cribriform plate. Most likely diagnosis: Advanced maxillary sinus carcinoma with orbital and skull base extension (T4a or T4b). Best next step: MRI with contrast to assess intracranial and perineural spread, followed by biopsy and PET-CT for staging. Management consideration: Multidisciplinary discussion for possible craniofacial resection with adjuvant radiotherapy.
Case 3. A 45-year-old patient underwent “complete excision” of a nasal mass 3 years ago, reported as adenoid cystic carcinoma on histopathology. She now presents with new-onset facial pain and diplopia. She has no cervical lymphadenopathy. Most likely diagnosis: Recurrent adenoid cystic carcinoma with perineural spread. Best next step: MRI with contrast to evaluate perineural spread along the trigeminal nerve branches. Important teaching point: Adenoid cystic carcinoma can recur late, even after 10-20 years, requiring long-term follow-up.
Case 4. A 70-year-old man presents with a blackish-blue mass on the anterior nasal septum. He has noticed it for 4 months, but has ignored it. He has no epistaxis or obstruction. Biopsy confirms malignant melanoma. Management plan: Endoscopic wide local excision, no craniofacial resection. Prognosis discussion: 5-year survival approximately 28%, tumour exhibits immunological symbiosis with variable outcomes.
Frequently Asked Questions in Viva
- What is the most common malignant tumour of the nose and paranasal sinuses? Squamous cell carcinoma accounts for approximately 80% of all sinonasal malignancies, making it the most common by a substantial margin.
- Why are sinonasal malignancies often diagnosed late? They initially mimic chronic rhinosinusitis with symptoms like nasal obstruction and discharge, leading to repeated medical treatment before proper evaluation, causing an average diagnostic delay of 6-8 months.
- What is Ohngren’s line, and why is it important? Ohngren’s line joins the medial canthus to the angle of the mandible, dividing the maxilla into suprastructure (poor prognosis) and infrastructure (better prognosis), helping predict surgical resectability and outcomes.
- Which sinonasal tumour has the worst long-term prognosis despite good initial survival? Adenoid cystic carcinoma shows good 5-year survival (70-80%) but drops to 5% or less at 20 years due to late recurrences and perineural spread.
- Can sinonasal malignancies be treated endoscopically? Yes, selected limited tumours can be treated with endoscopic excision, but contraindications include soft tissue involvement, dural involvement lateral to the orbit, brain invasion, or carotid artery encasement.
- What is the most important diagnostic step before biopsy? Imaging (CT or MRI) must precede biopsy to identify vascular tumours like esthesioneuroblastoma that could bleed catastrophically and to prevent distortion of tumour architecture.
- Which occupational exposure is most strongly linked to sinonasal adenocarcinoma? Wood dust exposure, particularly hardwoods like beech and oak, is linked specifically to adenocarcinoma of the ethmoid sinuses and upper nasal cavity.
—-End—-
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Sinonasal malignancy notes, Maxillary sinus carcinoma symptoms, Malignant tumour nose and paranasal sinuses, Sinonasal carcinoma diagnosis, Sinonasal tumour CT MRI differences, Ohngren line ENT, Ohngren line maxillary sinus carcinoma, Lederman classification paranasal sinuses, AJCC staging maxillary sinus carcinoma, Squamous cell carcinoma nasal cavity notes, Adenocarcinoma ethmoid wood dust exposure, Adenoid cystic carcinoma perineural spread ENT, Esthesioneuroblastoma olfactory neuroblastoma notes, Sinonasal undifferentiated carcinoma SNUC, Mucosal malignant melanoma nasal cavity, NK T cell lymphoma nose EBV, Midline granuloma lymphoma ENT, Maxillectomy types ENT surgery, Weber Ferguson incision maxillectomy, Lateral rhinotomy Moure incision ENT, Midfacial degloving approach ENT, Orbital exenteration indications sinonasal cancer, Craniofacial resection skull base tumour, IMRT in sinonasal malignancy, Chemoradiation for sinonasal carcinoma, Sinonasal malignancy high yield points, Sinonasal malignancy mnemonics, Sinonasal malignancy MCQs with answers, Sinonasal malignancy viva questions, Sinonasal malignancy CBME notes, Sinonasal malignancy NEET PG questions, Unilateral nasal obstruction epistaxis differential diagnosis, Maxillary sinus carcinoma spread directions, Pterygopalatine fossa involvement trismus, Perineural spread tumours ENT, Wood dust exposure ENT cancer, Sinonasal malignancy case scenarios, Sinonasal cancer management algorithm, Sinonasal tumour staging summary, Paranasal sinus cancer notes for MBBS, ENT PG revision sinonasal malignancy, Sinonasal malignancy exam guide India, ,Sinonasal malignancies malignant tumours nose paranasal sinuses notes, Malignant tumours of nose and paranasal sinuses MBBS notes, Sinonasal cancer NEET PG questions, Paranasal sinus malignancy etiology and risk factors, Wood dust exposure sinonasal adenocarcinoma adenocarcinoma woodworkers, Ohngren line classification maxillary sinus cancer, Ohngren classification suprastructure infrastructure prognosis, Maxillary sinus carcinoma staging AJCC TNM, Squamous cell carcinoma nose paranasal sinus most common, Adenoid cystic carcinoma perineural spread sinonasal, Esthesioneuroblastoma olfactory neuroblastoma cherry red mass, Malignant melanoma nose anterior septum immunological symbiosis, Sinonasal undifferentiated carcinoma SNUC management, Lymphoma midline granuloma EBV sinonasal T NK cell, Chondrosarcoma nasal septum skull base treatment, Craniofacial resection sinonasal skull base surgery, Endoscopic excision sinonasal malignancy indications contraindications, Orbital exenteration indications maxillary sinus cancer, Lateral rhinotomy Moure incision Weber Ferguson midfacial degloving, Unilateral nasal obstruction blood stained discharge chronic sinusitis red flag, Trismus maxillary sinus cancer posterior spread pterygoid muscles, Cheek anaesthesia maxillary nerve V2 involvement sinonasal cancer, How to diagnose sinonasal malignancy early, Sinonasal cancer biopsy before imaging contraindication, Why imaging before biopsy esthesioneuroblastoma vascular tumour, Sinonasal malignancy clinical case scenarios for viva, Malignant tumours nose paranasal sinuses MCQ with answers, Sinonasal cancer CBME curriculum ENT, Paranasal sinus malignancy prognosis five year survival rate, Adenoid cystic carcinoma 20 year survival less than 5 percent, Esthesioneuroblastoma bimodal age distribution treatment protocol, Sinonasal adenocarcinoma radiotherapy resistance combined therapy, Sinonasal malignant melanoma endoscopic resection only no craniofacial, Nose picker cancer septal squamous cell carcinoma low grade, Antroethmoidal tumour complex spread pattern, Pterygopalatine fossa involvement maxillary sinus cancer, Retropharyngeal lymph nodes sinonasal cancer drainage, Sinonasal cancer hematogenous metastasis lung liver brain bone, Lederman classification paranasal sinuses Sebileau line, Difference between Ohngren and Lederman classification, Midface degloving approach limitations infraorbital nerve, Intensity modulated radiotherapy IMRT sinonasal cancer optic nerve protection, Chemoradiation unresectable sinonasal cancer 5 year survival 60 percent, Intra arterial chemotherapy 5 fluorouracil cisplatin concomitant radiation, Sinonasal malignancy diagnostic delay 6 to 8 months, Bantu tribe maxillary sinus cancer African mahogany wood, Nickel refining leather tanning sinonasal cancer occupational risk, HPV EBV sinonasal carcinoma viral etiology, Sinonasal tract histological diversity tumour types, Medial maxillectomy inferior maxillectomy partial maxillectomy, Total maxillectomy surgical steps, Unresectable sinonasal tumour criteria bilateral optic nerve cavernous sinus, PET CT sinonasal cancer surveillance recurrence detection, MRI sinonasal tumour perineural spread fat suppression T1, CT scan sinonasal malignancy bony erosion cribriform plate, Sinonasal cancer treatment multidisciplinary approach, ENT PG exam guide sinonasal tumours, Sinonasal malignancy mnemonics for NEET PG, Paranasal sinus cancer high yield points revision, How to present sinonasal cancer case in viva, Common examiner questions sinonasal malignancy practical exam, Sinonasal tumours summary table for quick revision, Nose and paranasal sinus cancer epidemiology India incidence, Maxillary sinus most common site 70 percent, Infrastructure tumours better prognosis suprastructure poor prognosis, Sinonasal cancer neck node metastasis late retropharyngeal, Vascular tumour nose biopsy operating theatre nasal packing, Sinonasal undifferentiated carcinoma rare aggressive, Mesenchymal chondrosarcoma young patients aggressive, Adenoid cystic carcinoma lung metastasis classic, Sinonasal lymphoma B cell T cell NK cell EBV association, Esthesioneuroblastoma Hyams grading system, Craniofacial resection anterior cranial fossa en bloc removal, Orbital apex involvement orbital exenteration indication, Sinonasal cancer dental symptoms loosening teeth denture fit, Epiphora sinonasal tumour nasolacrimal duct obstruction, Sinonasal cancer differential diagnosis benign sinusitis, Unilateral sinusitis not responding to antibiotics malignancy red flag, Sinonasal malignancy patient age 5th to 6th decade male predominance, White race predilection sinonasal cancer, Sinonasal cancer metastatic workup, Sinonasal cancer adjuvant radiotherapy dose 5000 5500 cGy, Sinonasal cancer neoadjuvant chemotherapy, Endoscopic skull base surgery sinonasal malignancy, Sinonasal cancer quality of life post maxillectomy, Obturator prosthesis after maxillectomy, Sinonasal cancer follow up protocol long term surveillance.