|
The following CBME core competencies are covered in this chapter.
|
Disorders of the Pinna
Introduction
The pinna, or auricle, is the visible part of the external ear. Its complex shape helps collect sound and funnel it into the external auditory canal. However, the pinna is also prone to a wide range of congenital, traumatic, inflammatory, and neoplastic disorders. For students, understanding these conditions is essential for theory exams, practical viva, and NEET PG. This chapter provides a complete, easy-to-learn, and clinically relevant resource aligned with the CBME curriculum.
Table: Disorders of the Pinna
| 1. | Congenital Disorders of the Pinna | Microtia, Anotia, Macrotia, Bat ear (protruding ear), Coloboma, Lobule deformities |
| 2. | Trauma of the Pinna | Haematoma auris (boxer’s ear), Auricular pseudocyst, Lacerations, Avulsion of pinna, Frostbite |
| 3. | Infections / Inflammatory Disorders of the Pinna | Perichondritis, Relapsing polychondritis, Chondrodermatitis nodularis chronica helicis (Winkler’s nodule) |
| 4. | Non-inflammatory Disorders (Pinna and Preauricular) | Preauricular appendage (tag), Preauricular pit, Preauricular sinus, Keloid of pinna, Gouty tophi |
| 5. | Congenital Disorders of External Auditory Canal (Associated Topic) | Congenital aural atresia (solid and membranous), Collaural (cervico-aural) fistula |
Congenital Disorders of the Pinna
Congenital anomalies arise from errors in the development of the six hillocks of His during the first and second branchial arches. These disorders may be isolated or part of a syndrome.
1. Microtia and Anotia
Microtia means a small, underdeveloped pinna. It ranges from a small ridge of tissue to a partially formed ear. Anotia is the complete absence of the pinna, which is very rare.
- Key features: Unilateral (more common on the right) or bilateral. When bilateral, always assess for hearing loss because the external auditory canal (EAC) is often atretic.
- Peanut ear is a specific form of microtia where the pinna resembles a peanut.
- Association: Microtia frequently occurs with congenital aural atresia and ossicular anomalies, leading to conductive hearing loss.
- Management:
- Hearing rehabilitation: Bone-anchored hearing aid (BAHA) or bone conduction devices are the mainstay for bilateral cases.
- Surgical reconstruction: Usually performed after 6–8 years of age when the rib cartilage is large enough for grafting.
- Prosthetic ear: An option for patients who are not surgical candidates.
2. Macrotia
Macrotia refers to an abnormally large pinna. Usually, it is a normal variant with no functional impairment. Surgical reduction (otoplasty) is only for cosmetic reasons.
3. Bat Ear (Protruding Ear or Lop-Ear)
This is the most common congenital ear deformity. The ear protrudes more than 2 cm from the mastoid scalp at an angle greater than 30 degrees.
- Pathogenesis: The concha is deep and large, but the antihelical fold is absent or poorly developed. The scapha, therefore, does not fold inward.
- Clinical tip: The lobule is usually normal. The deformity is often bilateral.
- Surgical correction (Otoplasty): The best time for surgery is after 6 years of age. Waiting allows the ear to reach near-adult size and the child to participate in the decision.
4. Coloboma
A coloboma is a transverse cleft or split in the middle of the pinna, giving it a “question mark” appearance. It results from failed fusion of the hillocks.
5. Deformities of the Ear Lobule
The lobule (earlobe) can show several variants: complete absence, unusually large size, bifid (split) lobule, or attached lobule (instead of free-hanging). These are mainly cosmetic concerns.
Table: Congenital Pinna Disorders
| Disorder | Key Feature | Treatment |
| Microtia | Small, peanut-shaped ear | BAHA, reconstruction after age 6 |
| Anotia | Absent pinna | Prosthesis, BAHA |
| Macrotia | Large pinna | Cosmetic reduction |
| Bat Ear | Protruding >2 cm, no antihelical fold | Otoplasty after age 6 |
| Coloboma | Transverse cleft in pinna | Surgical closure if desired |
Trauma of Pinna
Trauma is common because the pinna is exposed. The key principle is to intervene early to prevent permanent deformity.
1. Haematoma of the Pinna (Boxer’s Ear)
A haematoma of the pinna is a collection of blood between the auricular cartilage and the overlying perichondrium, usually involving the anterior surface of the auricle following blunt trauma. It requires urgent drainage (preferably within 24–48 hours) to prevent cartilage necrosis and permanent cauliflower ear deformity.
Aetiology: Blunt trauma (e.g., wrestling, boxing, rugby). Rarely, spontaneous haematoma may occur in patients with bleeding disorders or those receiving anticoagulant therapy.
Pathogenesis: Shearing between the auricular cartilage and its perichondrium leads to the formation of a potential space, which rapidly fills with blood following the rupture of small vessels. The haematoma most commonly involves the anterior surface of the pinna. If untreated, fibrovascular granulation tissue develops within the haematoma. Mesenchymal cells differentiate into chondroblasts, producing irregular fibrocartilage that thickens and distorts the pinna (cauliflower ear).
Outcome: Separation of the perichondrium deprives the cartilage of its blood supply, leading to cartilage necrosis and irregular fibrocartilage formation. This produces the characteristic cauliflower ear (pugilistic ear or boxer’s ear) deformity.
Treatment (within 48 hours):
- Aspiration may be attempted for very small haematomas, but it has a higher recurrence rate. Use a wide-bore needle.
- Incision and drainage with a pressure dressing is the preferred method for most haematomas to prevent recurrence. Incision and drainage can also be done if aspiration fails or if the haematoma is solid. Re-examine after 24–48 hours because recurrence is common.
- Technique: A curvilinear incision is made over the most fluctuant part of the haematoma. The clot is evacuated, the cavity is irrigated, and a bolster pressure dressing or quilting sutures are applied to prevent recurrence.
- Antibiotics: Prophylactic antibiotics are commonly prescribed after incision and drainage, particularly when cartilage has been exposed, to reduce the risk of perichondritis. Coverage against Staphylococcus aureus is recommended, and antipseudomonal coverage may be considered in selected patients.
- Other agents (rarely used): Intralesional steroids, OK-432 (sclerosant), or fibrin glue may be used for recurrent cases.
2. Auricular Pseudocyst (Benign Idiopathic Cystic Chondromalacia).
It is an intracartilaginous cystic collection, containing viscous, straw-coloured, sterile fluid and devoid of any epithelial lining.
Key difference from haematoma: No history of trauma, no pain, and no granulation tissue on aspiration.
Treatment: Similar to haematoma (aspiration + pressure dressing), but curettage is not required as no granulation tissue is present here.
3. Lacerations of the Pinna
Aetiology: Same as external canal trauma
Treatment principles to avoid deformity:
- Clean and debride all necrotic tissue.
- Aspiration of blood in case of hematoma formation.
- Incision and drainage if required.
- The perichondrium is stitched with absorbable sutures and the skin with nonabsorbable sutures. Avoid stripping of the perichondrium from cartilage, as it may lead to avascular necrosis. Suturing with or without a free and or pedicled flap.
- Inj. TT as prophylaxis
- Course of broad-spectrum antibiotics for 1 week.
4. Avulsion of the Pinna
Partial avulsion with a small pedicle has a good prognosis with primary repair. Complete avulsion is challenging.
Treatment Options:
- Reimplantation using microvascular techniques (in selected centres).
- Temporary banking: Remove the skin from the avulsed cartilage and bury the cartilage under the postauricular skin. Reconstruct later.
- Prosthesis for complete loss.
5. Frostbite of the Pinna
Aetiology: Exposure to extreme cold.
Pathogenesis: Extreme cold causes ice crystals and obstruction of vessels, leading to erythema and oedema, bullae formation, necrosis of skin and subcutaneous tissue and complete necrosis with loss of the affected part.
Signs: Pinna initially may appear red, but later turns blue depending upon the duration of exposure.
Treatment:
- Rapid rewarming in circulating warm water (38–42°C) for 15–30 minutes.
- Protection of bullae from rupture.
- Topical 1% silver sulfadiazine for superficial infection.
- Analgesics for pain.
- Systemic antibiotics directed against Pseudomonas aeruginosa and Staphylococcus aureus for secondary infection.
- Surgical debridement of necrotic tissue should be delayed until a reliable line of demarcation develops (weeks to months).
Infections or Inflammatory Disorders of the Pinna
Infections of the pinna can rapidly destroy cartilage, leading to permanent deformity.
1. Perichondritis
It is an inflammation of the perichondrium.
Causes:
- Results from the extension of an infection from cellulitis, diffuse otitis externa, furuncle of the meatus or ‘high’ piercing of the cartilaginous area of the auricle.
- Infection may be secondary to lacerations, untreated haematoma, frostbite, burns, chemical injury or surgical incisions.
Causative micro-organisms: Gram-positive: Pseudomonas, Staphylococcus aureus. Gram-negatives: Proteus, Enterococcus, and Escherichia coli. Mixed flora
Pathology: The cartilage gets its blood supply from perichondrium. Whenever serous fluid accumulates between the cartilage and perichondrium (due to trauma/ inflammation), the perichondrium is lifted from the cartilage. Avascular necrosis, fibrosis, intense infiltration with polymorphonuclear leukocytes, thickening of the perichondrium and destruction of the cartilage by phagocytes are usual pathological findings. The lobule, which contains no cartilage, is spared.
Symptoms:
- Red, hot, stiff and painful pinna movement.
- Pyrexia and malaise.
- Cauliflower ear deformity may occur because of extensive destruction of cartilage.
- Rare complications of perichondritis include fatal septicaemia, subacute bacterial endocarditis and necrotising fasciitis of the neck.
Signs:
- Tenderness
- Fluctuation, if pus is present.
Prevention:
- Avoid tight head bandages during ear surgery.
- Avoid ear piercing in the cartilaginous pinna.
- Drain haematomas under aseptic conditions.
- Burn injuries should be managed with prophylactic antibiotics against Gram-negative bacteria, daily dressings and the removal of eschars and crusts.
Treatment:
- Systemic antibiotics active against Pseudomonas (e.g., ciprofloxacin, piperacillin-tazobactam).
- Local application of 4% aluminium acetate compresses.
- Culture and sensitivity of the pus should be obtained.
- Abscess must be aspirated and irrigation with an antibiotic solution.
- The incision is made in the natural fold, and devitalized cartilage is removed. A fenestrated polyethylene tube/catheter may be placed in the subperiosteal tunnels on either side of the cartilage. The necrosed cartilage needs to be debrided in a non-responsive case.
- Total chondrectomy is done if the entire area is involved.
Viva Tip: In perichondritis, the lobule is normal. In cellulitis of the pinna, the lobule is also involved.
2. Relapsing Polychondritis
It is a rare autoimmune disorder and is characterised by a severe, episodic and progressive inflammatory condition involving cartilaginous structures throughout the body.
- Common sites affected (in order): Ears (most common) → Nose → Laryngotracheobronchial tree.
- Symptoms: Sudden, painful, red ear. The patient cannot sleep on that side. The ear becomes floppy due to cartilage destruction. Hearing loss may occur from canal stenosis or middle ear involvement.
- Key sign: The lobule is always spared (same as perichondritis, but here it is autoimmune, not infectious).
- Treatment: High-dose systemic corticosteroids (e.g., prednisolone 1mg/kg/day). Immunosuppressants for refractory cases.

3. Chondrodermatitis Nodularis Chronica Helicis (Wrinkler’s Nodule)
This is a painful, benign nodule on the helix or antihelix, typically in middle-aged or elderly men (40–70 years).
Aetiology: Chronic pressure (e.g., sleeping on one side), sun exposure, or trauma.
Presentation: A small (3–6 mm), firm, round, pale or erythematous nodule. It is exquisitely tender. The patient often complains that they cannot sleep on that ear.
Treatment:
- Medical: Topical steroids and protective padding (e.g., a doughnut-shaped pillow).
- Surgical (definitive): Complete excision of the nodule, including the involved cartilage and overlying skin.

Non-Inflammatory Disorders (Pinna and Preauricular)
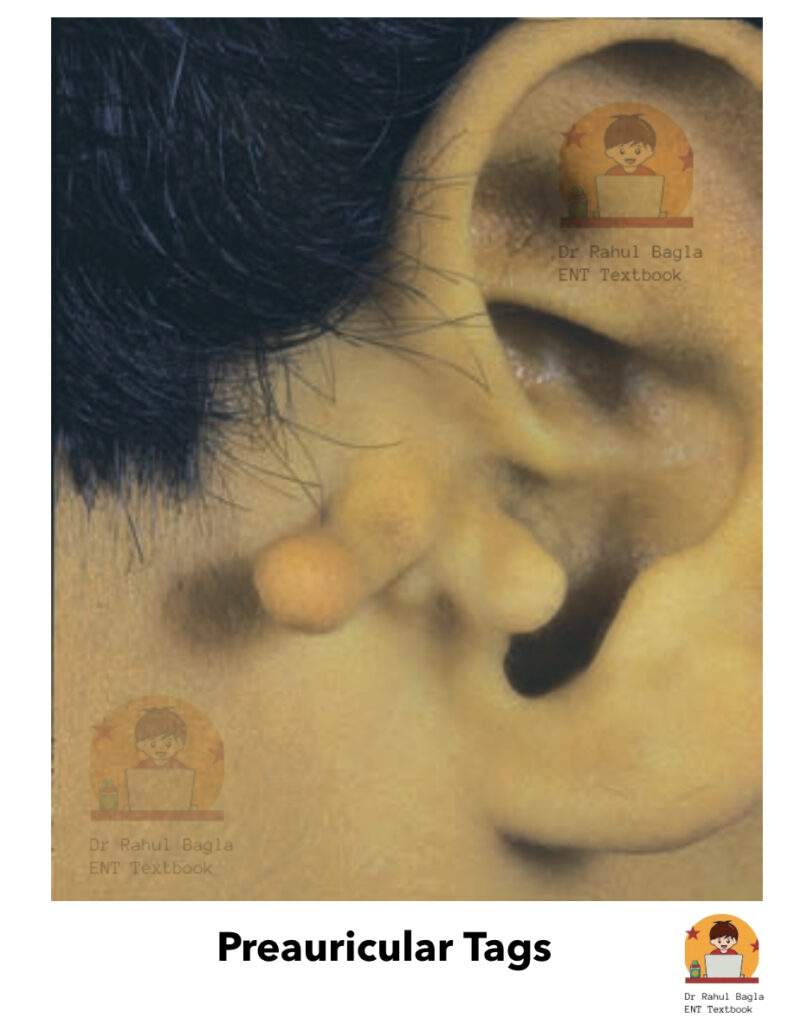
1. Pre-auricular appendage (tags)
It consists of skin and fat that appear on an imaginary line drawn from the tragus to the angle of the mandible. A few pieces of cartilage may be present and are called the accessory auricle.
Treatment: Simple excision may be done after 1 year of age to improve facial symmetry and cosmesis.
2. Preauricular Pit and Sinus
A pit is a small depression anterior to the crus of the helix. A sinus is an epithelial-lined tract that may extend medially towards the EAC, parotid, or even the middle ear.
- Presentation: Usually asymptomatic. When infected, it causes pain, swelling, and purulent discharge. Recurrent infection is common.
- Treatment:
- Acute infection: Antibiotics and incision/drainage of any abscess.
- Definitive: Complete surgical excision of the entire tract after the infection resolves. A fistulogram/sinogram helps map the tract before surgery.
High-Yield Point: Preauricular sinus can be associated with branchio-oto-renal (BOR) syndrome. Always check renal function if bilateral.
3. Keloid of the Pinna
Keloids are benign, hypertrophic, fibrous lesions that often invade adjacent normal areas, causing cosmetic deformities. They usually develop as a result of ear piercing, trauma or surgery. Common sites are the earlobe or helix.
Treatment options:
- Small/fresh keloids: Intralesional triamcinolone injection every 4–6 weeks.
- Large/mature keloids: Surgical excision combined with intraoperative and postoperative steroid injections every 4–6 weeks (minimum 3 sessions).
- Adjuncts: KTP or CO2 laser, or low-dose superficial radiotherapy (risk of malignancy, so reserved for resistant cases).
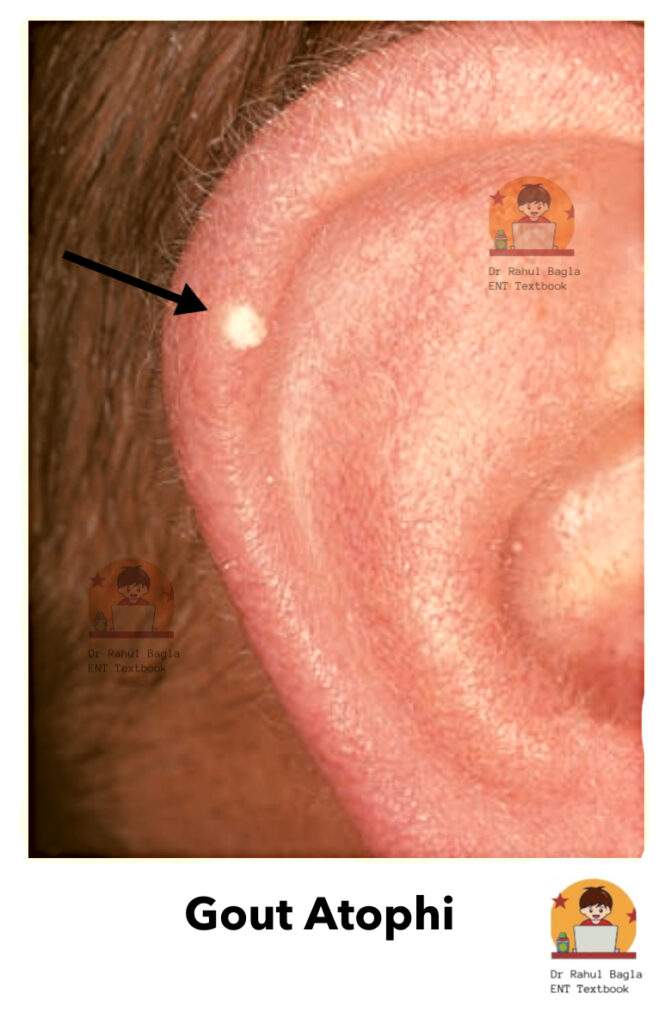
5. Gouty Tophi
It is generally seen in patients suffering from hyperuricemia. Patient presents with a small subcutaneous nodule due to deposition of uric acid crystals. The most common site is the helix. Nodules appear as moderately painful, salmon-pink in colour. A whitish, chalky substance consisting of sodium biurate comes out on compression.
Treatment: Anti-inflammatory analgesics for pain relief and correction of abnormality in uric acid metabolism
Congenital Disorders of the External Auditory Canal
Although not strictly pinna disorders, these are clinically linked because they often coexist with pinna anomalies.
1. Congenital Aural Atresia (absence of passage)
Congenital atresia of the meatus may occur alone (as a result of the failure of canalisation of the ectodermal core that fills the dorsal part of the first branchial cleft) or, more commonly, it may occur in association with microtia.
Pathogenesis: As re-canalisation of EAC starts from the deeper part near the tympanic membrane and progresses outwards, at times the deeper meatus is developed while the outer canal is obliterated with fibrous tissue or bone. Atresia may be associated with abnormalities of the middle ear, internal ear and other structures.
Types of atresia:
- Solid atresia occurs with fibrous tissue alone or with both fibrous and bony material. The solid atresia may be blunt or tapering in shape and produce a funnel-shaped medial aspect to the lumen of the ear canal. Surgery is challenging.
- Membranous atresia: The skin of the ear canal is covered with a skin that separates the ear canal into a medial and lateral segment. The skin of the medial segment may at times desquamate, collect keratin and even become erosive (to form external canal cholesteatoma).
Investigations:
- Examine thoroughly to detect any other associated anomaly.
- Hearing tests.
- CT scan is needed to detect the bony and soft-tissue parts of the external ear and differentiate solid from membranous atresia.
Management:
- Hearing rehabilitation: BAHA, Cochlear implant.
- Surgical: Atresiaplasty can reduce conductive hearing loss to 25 dB. Cosmesis can be achieved with a prosthesis or other surgical techniques.

2. Collaural fistula or cervico-aural fistula
It is a rare abnormality of the first branchial cleft. The fistula has one opening in the neck just below and behind the angle of the mandible and the other opening in the external canal or the middle ear. The track of the fistula passes close to the facial nerve and through the parotid gland. The definitive treatment is surgical exploration and excision.
———— End of the chapter ————
High-Yield Points for NEET PG & University Exams
- Bat ear surgery: Only after 6 years of age. Reason: Ear reaches near-adult size; child can consent.
- Cauliflower ear: Due to an untreated or recurrent pinna haematoma.
- Lobule spared in: Perichondritis, relapsing polychondritis, and frostbite (late).
- Most common organism in perichondritis: Pseudomonas aeruginosa.
- Best imaging for aural atresia: High-resolution CT temporal bone.
- Best initial hearing rehabilitation for bilateral microtia with atresia: BAHA (not surgery).
- Preauricular sinus association: BOR syndrome (Branchial fistula, Otologic anomalies, Renal anomalies).
- Winkler’s nodule: Exquisitely tender nodule on helix; patient cannot sleep on that side.
- Collaural fistula danger: Tract runs near the facial nerve.
- Pseudocyst vs Haematoma: No trauma, no pain, no granulation tissue in pseudocyst.
NEET PG-Style MCQs
- A 22-year-old boxer presents with a swollen, distorted right pinna after a match. On examination, there is a fluctuant swelling on the anterior surface. The lobule is normal. What is the most appropriate next step? A. Observe and apply ice B. Incision and drainage under local anaesthesia C. Aspiration with a wide-bore needle and pressure dressing D. Systemic steroids.
- A newborn has a small, peanut-shaped pinna with a closed external auditory canal. Which of the following is the most appropriate initial step? A. CT scan of the temporal bone B. Hearing assessment (OAE/ABR) C. Surgical reconstruction at 1 year D. Prosthetic ear fitting.
- A 15-year-old girl wants surgery for her protruding ears. Her father asks when is the best time is to operate. Your reply is: A. Before 2 years of age B. Any time after 3 years C. After 6 years of age D. After 12 years of age.
- A 45-year-old man presents with a painful red right ear. He had a high ear piercing 2 weeks ago. The lobule is normal, but the helix and antihelix are swollen and tender. What is the most likely diagnosis? A. Pinna cellulitis B. Relapsing polychondritis C. Perichondritis D. Chondrodermatitis nodularis.
- Which of the following is the most common organism causing perichondritis of the pinna? A. Staphylococcus aureus B. Pseudomonas aeruginosa C. Streptococcus pyogenes D. Escherichia coli.
- A 50-year-old man has a small, pale, extremely tender nodule on his helix. He cannot sleep on that side. The most likely diagnosis is: A. Keloid B. Gouty tophus C. Chondrodermatitis nodularis chronica helicis D. Basal cell carcinoma.
- A patient with bilateral microtia and aural atresia has a 60 dB conductive hearing loss. What is the best initial hearing rehabilitation? A. Atresiaplasty B. BAHA C. Conventional hearing aid D. Cochlear implant.
- A 25-year-old woman has a recurrently discharging pit just anterior to the helix. What is the definitive treatment? A. Antibiotics for 6 weeks B. Complete surgical excision of the tract C. Incision and drainage D. Topical silver nitrate cautery.
- In a patient with a collaural fistula, which structure is most at risk during surgery? A. Great auricular nerve B. External carotid artery C. Facial nerve D. Parotid duct.
- A 30-year-old man presents with a painless, fluctuant swelling on the anterior pinna. He denies any trauma. Aspiration yields straw-coloured fluid. What is the diagnosis? A. Pinna haematoma B. Auricular pseudocyst C. Perichondrial abscess D. Relapsing polychondritis.
Answers: 1: C. 2: B. 3: C. 4: C. 5: B. 6: C. 7: B. 8: B. 9: C. 10: B.
Clinical Case Scenarios for Viva & Practical Exams
Case 1. A 16-year-old boy comes to the emergency department with a swollen, purple left ear after a school rugby match 6 hours ago. The anterior surface has a soft, fluctuant swelling. He has no other injuries. What is your diagnosis? What is the first step in management? What complication will occur if left untreated? Answer: Diagnosis: Pinna haematoma. First step: Aspiration with a wide-bore needle followed by a firm pressure dressing (or referral for same). Untreated complication: Cauliflower ear deformity.
Case 2. A 35-year-old woman presents with a red, hot, and very painful right ear. She had her upper ear cartilage pierced at a mall 10 days ago. On examination, the lobule is normal, but the rest of the pinna is swollen and tender. There is no fluctuation. What is the most likely diagnosis? Which two organisms should your antibiotics cover? When would you consider incision and drainage? Answer: Diagnosis: Perichondritis. Cover Pseudomonas and Staph aureus. Consider incision and drainage if fluctuance appears (abscess formation).
Case 3. A 55-year-old man presents with a small, painful nodule on the helix of his left ear for 6 months. He says he cannot sleep on that side because the pain wakes him. He has tried over-the-counter painkillers with no relief. What is the likely diagnosis? What is the non-surgical treatment you can offer? What is the definitive treatment? Answer: Likely diagnosis: Chondrodermatitis nodularis chronica helicis (Winkler’s nodule). Non-surgical: Topical steroids and a protective doughnut pillow. Definitive: Surgical excision of the nodule, including the involved cartilage.
Frequently Asked Questions in Viva
- What is the most common cause of cauliflower ear? Untreated or recurrent pinna haematoma following blunt trauma, especially in contact sports like wrestling or boxing.
- Why is the ear lobule spared in perichondritis? The lobule contains no cartilage, so the infection that tracks along the perichondrium cannot involve it.
- At what age is bat ear surgery best performed? After 6 years of age to allow near-complete ear growth and ensure the child can participate in the decision.
- What is the first-line imaging for congenital aural atresia? High-resolution CT scan of the temporal bone to assess bony anatomy, ossicles, and facial nerve course.
- What is the difference between a preauricular pit and a preauricular sinus? A pit is a small blind depression. A sinus is an epithelial-lined tract that extends deeper, sometimes to the EAC or parotid.
- Which antibiotic is most important to cover in pinna perichondritis? Anti-pseudomonal coverage, such as ciprofloxacin or piperacillin-tazobactam.
- Can a completely avulsed pinna be reattached? Yes, in selected cases using microvascular reimplantation. Otherwise, the cartilage can be buried under postauricular skin for later reconstruction.
———— End ————
Download full PDF Link: Diseases of External Ear Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Microtia, Macrotia, Bat ear, Coloboma, Deformities of Ear Lobule, Congenital Atresia, Collaural fistula, Perichondritis, Relapsing Polychondritis,Wrinkler’s Nodule, Furuncle, Diffuse Acute Otitis Externa, Otomycosis, Haemorrhagic otitis externa, Herpes Zoster Oticus, Aural polyps, Acquired atresia of EAC, Tympanic Membrane Retraction, Retraction Pockets and Atelectasis, Myringitis, Atrophic Tympanic Membrane, Tympanosclerosis, Tympanic Membrane Perforations, Pre-auricular appendage (tags), Preauricular pit, Preauricular Sinus, Keloid of Auricle, Gouty Tophi, Haematoma of the Auricle, Auricular Pseudocyst, Lacerations, Avulsion of Pinna, Frostbite, External canal trauma, Traumatic rupture of tympanic membrane, Exostosis, Keratosis Obturans, Cholesteatoma of External Auditory Canal, Malignant (Necrotizing) Otitis Externa, Skull base osteomyelitis, Eczematous Otitis Externa, Neurodermatitis, Seborrhoeic Otitis Externa, Impacted Wax or Cerumen.Perichondritis, Otomycosis, Herpes Zoster Oticus, Myringitis bullosa, Tympanosclerosis, Malignant (Necrotizing) Otitis Externa, Diseases of External Ear