Vasomotor Rhinitis
Introduction
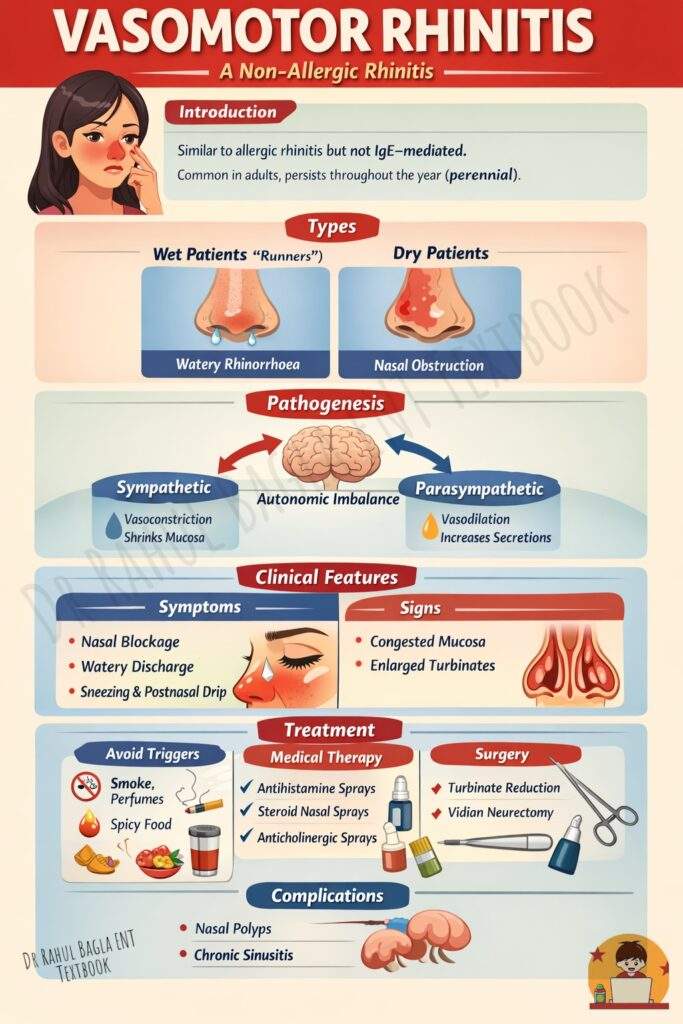
Vasomotor rhinitis is a type of non-allergic rhinitis that clinically resembles allergic rhinitis. However, it does not involve IgE-mediated hypersensitivity. Therefore, vasomotor rhinitis is diagnosed only after excluding allergic rhinitis through history, examination, and allergy testing. Unlike allergic rhinitis, which may be seasonal, vasomotor rhinitis usually persists throughout the year (perennial) and is seen more often in adults.
Types of Vasomotor Rhinitis
Patients with vasomotor rhinitis do not all present in the same way. Instead, they tend to fall into two broad clinical patterns.
- Wet Patients (“Runners”). These individuals mainly complain of profuse watery nasal discharge, which becomes their most troublesome symptom. This occurs because of increased glandular secretion driven by cholinergic (parasympathetic) overactivity.
- Dry Patients. In contrast, “dry type” patients predominantly experience nasal obstruction with minimal or no discharge. These patients have increased sensitivity of sensory (nociceptive) nerve endings in the nasal mucosa, which leads to exaggerated responses even to mild stimuli.
Pathogenesis
The exact cause of vasomotor rhinitis is not fully understood, but the central mechanism involves an imbalance in the autonomic nervous system.
The nasal mucosa contains a rich vascular network with venous sinusoids that behave like erectile tissue. These sinusoids regulate nasal airflow by alternating between congestion and decongestion.
- When the sympathetic system is activated, it produces vasoconstriction. This shrinks the mucosa and improves nasal airflow.
- When the parasympathetic system is activated, it causes vasodilation, mucosal swelling, and increased nasal secretions.
In vasomotor rhinitis, parasympathetic overactivity dominates, leading to persistent mucosal congestion and excessive secretion. At the same time, the nasal mucosa becomes hyper-reactive, responding excessively to trivial environmental stimuli such as cold air, humidity changes, smoke, or strong odours.
The hypothalamus, which regulates autonomic function, also explains why emotional stress and psychological factors can trigger or worsen symptoms.
Recent concepts further suggest that vasomotor rhinitis involves non-IgE inflammation, increased mucosal permeability, and abnormal neurogenic reflexes. This makes the nasal lining unusually sensitive even to harmless triggers such as cold air, smoke, or strong smells.
Clinical features
Symptoms. Patients typically present with a combination of symptoms that resemble allergic rhinitis, but with a key difference—allergy tests are negative. The most common complaints include persistent nasal obstruction, watery rhinorrhoea, bouts of sneezing (often worse in the morning), and postnasal drip. These symptoms often fluctuate and are triggered by environmental factors such as temperature changes, strong smells, smoke exposure, spicy food, or emotional stress.
Signs. Anterior rhinoscopy may show congested nasal mucosa and hypertrophied turbinates, although the mucosa may sometimes appear normal between episodes.
Complications.
If left untreated, long-standing vasomotor rhinitis can lead to structural and inflammatory changes in the nose. Patients may develop hypertrophic rhinitis, nasal polyps, or even chronic rhinosinusitis due to persistent mucosal oedema and obstruction.
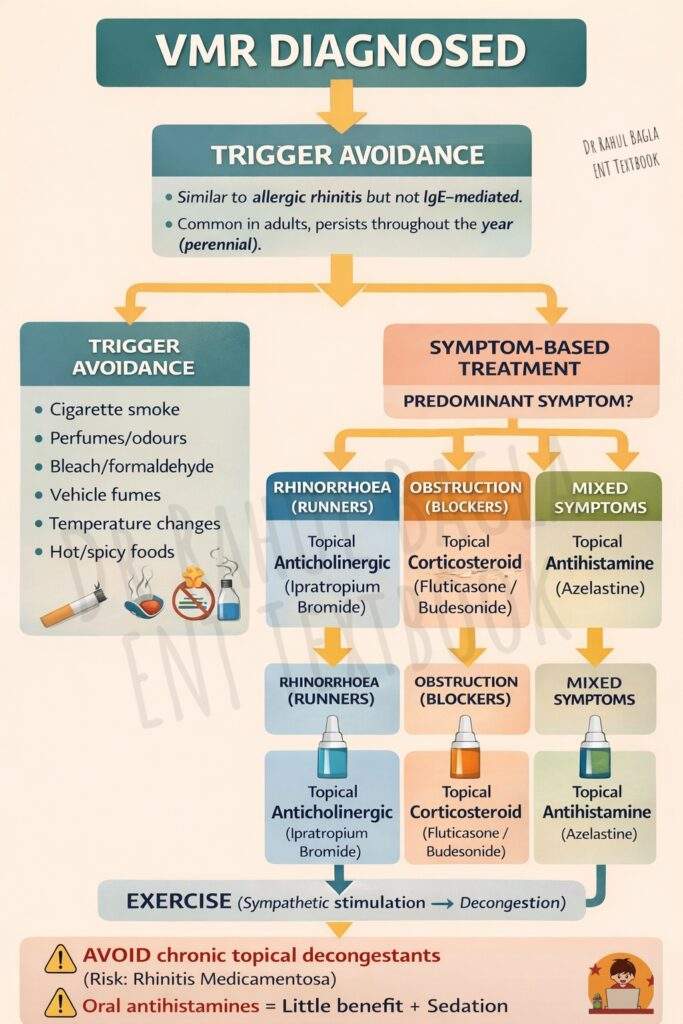
Diagnosis.
There is no specific diagnostic test for vasomotor rhinitis. The diagnosis is primarily clinical and by exclusion. A detailed history, absence of allergen-specific triggers, and negative allergy testing help confirm the condition.
Treatment
Management focuses on reducing symptoms and improving quality of life by targeting both triggers and underlying mechanisms.
- Avoid Triggers. The first and most important step is avoidance of triggers. Patients should identify and minimise exposure to factors such as cigarette smoke, perfumes, chemical fumes, vehicle emissions, sudden temperature changes, and spicy foods.
- Medical Treatment. Medical treatment depends on the predominant symptom pattern. When rhinorrhoea is the main complaint, topical anticholinergic nasal sprays are most effective as they reduce glandular secretion. When nasal obstruction dominates, intranasal corticosteroids help by reducing mucosal inflammation and oedema. In patients with multiple symptoms, topical antihistamines may provide relief, even though the condition is non-allergic. Oral antihistamines generally have limited benefit and may cause sedation. Long-term use of topical nasal decongestants should be avoided, as they can lead to rhinitis medicamentosa (rebound congestion).
- Exercise. Regular exercise improves nasal airflow. Exercise stimulates the sympathetic nervous system, which produces nasal decongestion and improves breathing.
- Surgical management. Surgery is reserved for patients who do not respond adequately to medical therapy. Procedures such as turbinate reduction surgery help relieve persistent nasal obstruction by reducing mucosal bulk. Any associated structural abnormalities, such as a deviated nasal septum or nasal polyps, should be corrected simultaneously. In severe cases with persistent, troublesome rhinorrhoea, vidian neurectomy may be considered. This procedure reduces parasympathetic stimulation to the nasal glands and thereby decreases nasal secretions.
——– End——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Vasomotor rhinitis notes for MBBS students, Vasomotor rhinitis ENT exam guide, Vasomotor rhinitis NEET PG MCQs, Non-allergic rhinitis causes and treatment ENT, Vasomotor rhinitis symptoms diagnosis management, Vasomotor rhinitis summary ENT residents, Difference between allergic rhinitis and vasomotor rhinitis, Vasomotor rhinitis CBME ENT notes, Vidian neurectomy indications ENT, Rhinorrhoea causes ENT revision notes