|
The following CBME core competencies are covered in this chapter.
|
Acute Rhinitis
Introduction
Acute rhinitis is an acute inflammation of the nasal mucosa. It commonly presents with sneezing, nasal obstruction, rhinorrhoea (nasal discharge), and irritation in the nasal cavity. This condition is one of the most common upper respiratory infections seen in clinical practice. Most cases occur due to viral infection, particularly the common cold. However, bacterial infection or exposure to environmental irritants may also produce similar symptoms.
In most patients, the disease is self-limiting, which means it resolves on its own within a short period. Nevertheless, if infection spreads to nearby structures, complications may develop. These complications may involve the paranasal sinuses, middle ear, pharynx, or lower respiratory tract. Therefore, early recognition and proper symptomatic treatment remain important in clinical practice.
Types of Acute Rhinitis
Acute rhinitis is usually classified by its underlying cause. Three main types are recognised:
- Viral rhinitis (Common cold, Influenzal rhinitis, Rhinitis associated with exanthemas)
- Bacterial rhinitis
- Irritative rhinitis
Among these, viral rhinitis is the most common type, and it usually presents as the common cold.
Viral Rhinitis
A. Common Cold (Coryza)
The common cold, also known as coryza, represents the most frequent form of acute rhinitis. It occurs when respiratory viruses infect the nasal epithelial lining. The infection produces inflammation of the mucosa, which leads to the typical symptoms of sneezing, nasal blockage, and nasal discharge.
Aetiology. Several viruses can produce acute rhinitis, and rhinovirus is the most common cause. Rhinoviruses belong to the picornavirus family, and they account for approximately half of all cases of the common cold. Other viruses that can cause acute rhinitis include coronavirus, influenza virus, parainfluenza virus, respiratory syncytial virus, adenovirus, and enterovirus. The incubation period, which is the time between infection and the appearance of symptoms, usually ranges from 1 to 4 days. After symptoms appear, the illness generally lasts for 7 to 14 days, although mild symptoms such as nasal blockage or discharge may sometimes continue for two to three weeks.
Mode of Transmission. Acute viral rhinitis spreads mainly through droplet infection. When an infected person coughs or sneezes, numerous virus-containing droplets are released into the air. These droplets can remain suspended in the atmosphere for several hours. As a result, people nearby may inhale the droplets and become infected. In addition, very small droplets called microdroplets can travel in air currents and remain infectious for up to two days. Therefore, infection may also spread through contaminated surfaces, dust particles, or hand-to-hand contact.
Pathogenesis. After entering the nasal cavity, the virus attaches to and invades the epithelial cells of the nasal mucosa. The infected cells then release inflammatory mediators, which produce several changes in the nasal mucosa. These changes include vasodilatation of blood vessels, swelling of the mucosa, and increased secretion from seromucinous glands. As a result of these inflammatory changes, the patient develops the classic symptoms of acute rhinitis, namely nasal obstruction, rhinorrhoea, and sneezing.
Stages of Acute Viral Rhinitis
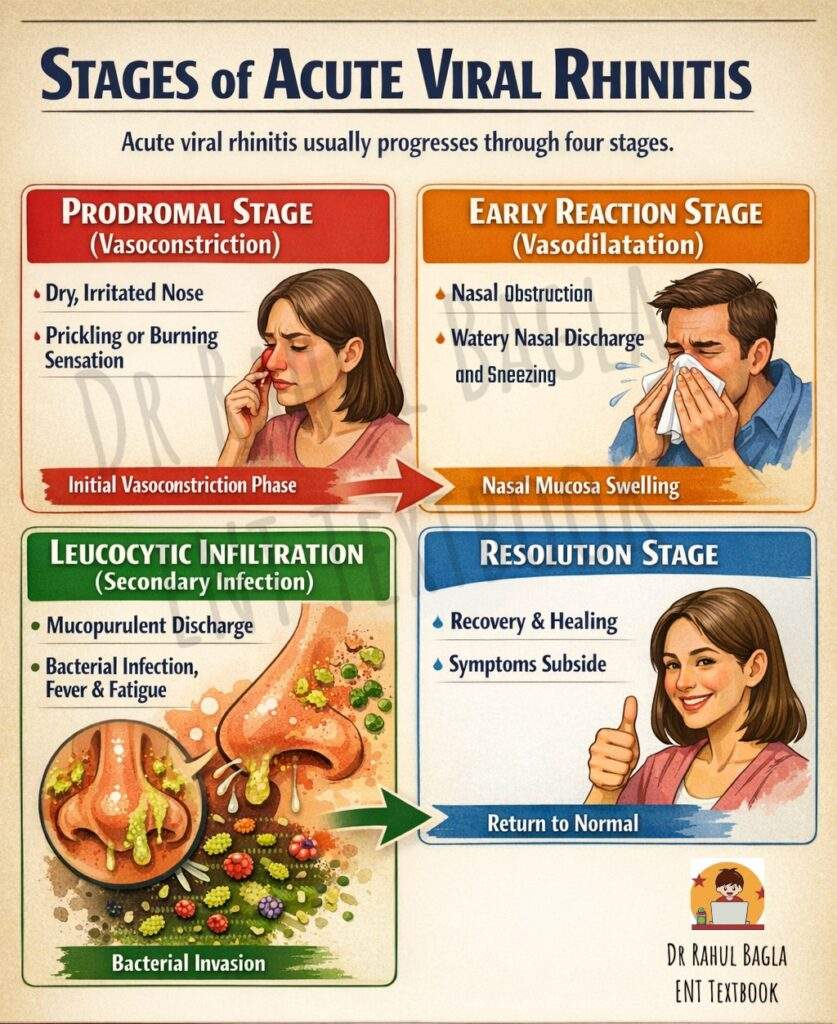
Acute viral rhinitis usually progresses through four stages. Understanding these stages is important because they are frequently asked in ENT theory examinations, viva questions, and NEET PG MCQs.
- Stage 1: Prodromal Stage (Stage of Vasoconstriction). The disease usually begins with a prodromal phase. During this stage, there is temporary vasoconstriction of the nasal blood vessels. The patient experiences a dry and irritated sensation inside the nose. Many patients also complain of a prickling or burning feeling at the back of the nose. Because these symptoms appear before the full disease develops, this phase is called the prodromal stage.
- Stage 2: Stage of Early Reaction (Stage of Vasodilatation). After the initial stage, the inflammatory process produces vasodilatation of the nasal blood vessels. This causes swelling of the nasal mucosa and increased activity of the seromucinous glands. Consequently, the patient develops nasal obstruction and profuse watery nasal discharge. Sneezing is also common during this stage.
- Stage 3: Stage of Leucocytic Infiltration (Secondary Infection Stage). After approximately three to four days, secondary bacterial infection often occurs. At this stage, white blood cells infiltrate the inflamed mucosa, and bacterial organisms begin to multiply. Because of this bacterial invasion, the nasal discharge changes from clear watery fluid to thick mucopurulent discharge. Common bacteria responsible for secondary infection include Haemophilus influenzae, Staphylococcus aureus, Streptococcus haemolyticus, Streptococcus pneumoniae, Moraxella catarrhalis, and Klebsiella pneumoniae. During this stage, the patient usually experiences maximum nasal obstruction, general weakness, and systemic symptoms such as malaise or fever.
- Stage 4: Stage of Resolution. Eventually, the body’s immune system eliminates the infection. As the inflammation subsides, the nasal mucosa gradually returns to normal. Symptoms usually improve within four to ten days, although mild nasal discharge may persist for a short period.
Clinical Features. Acute rhinitis produces both local nasal symptoms and systemic symptoms.
- Local Symptoms. The disease usually begins with a burning sensation or irritation inside the nose. Soon afterwards, the patient develops nasal stuffiness, sneezing, and rhinorrhoea. At first, the nasal discharge is clear and watery; after a few days, it may become thick and mucopurulent due to secondary bacterial infection.
- Systemic Symptoms. In addition to nasal symptoms, many patients experience general systemic features. These commonly include mild fever, chills, headache, malaise, and generalised body aches. These symptoms occur because viral infection produces a systemic inflammatory response.
Complications. In most patients, acute rhinitis resolves spontaneously within two to three weeks. However, in some cases, the infection may spread to adjacent structures and produce complications. Common complications include sinusitis, pharyngitis, tonsillitis, nasopharyngitis, lower respiratory tract infection, lymphadenitis, pneumonia, cavernous sinus thrombosis, and otitis media. Among these complications, sinusitis and otitis media occur most frequently because inflammation in the nasal cavity may obstruct the sinus ostia or the Eustachian tube.
Treatment. The treatment of acute viral rhinitis is mainly symptomatic, because the disease is usually self-limiting.
- Adequate bed rest and sufficient fluid intake help improve the patient’s general condition and support the body’s natural immune response. Warm fluids and steam inhalation may also provide symptomatic relief by improving mucociliary clearance.
- Antihistamines are often prescribed because they help reduce sneezing and nasal discharge. Topical nasal decongestants may also be used to decrease mucosal swelling and relieve nasal obstruction.
- Analgesics such as paracetamol are useful for relieving fever, headache, and muscle pain. Aspirin should generally be avoided because it may increase viral shedding; non-aspirin analgesics are preferred.
- Antibiotics are not routinely required in uncomplicated viral rhinitis. However, if secondary bacterial infection develops, appropriate antibiotics may be prescribed.
B. Influenzal Rhinitis
Rhinitis may occur during infection with influenza viruses such as Influenza A virus, Influenza B virus, and Influenza C virus. In these infections, the nasal symptoms are similar to those seen in the Common Cold. Patients commonly experience nasal obstruction, rhinorrhoea, and sneezing. However, influenza infection usually produces more severe systemic symptoms than the common cold. Patients often develop high fever, marked malaise, headache, and generalised muscle pain. Secondary bacterial infections are also more common in influenza, which may lead to complications involving the nose, sinuses, or respiratory tract.
C. Rhinitis Associated with Exanthematous Diseases
Some viral illnesses that produce skin rashes (exanthematous diseases) also cause rhinitis in the early stage of the illness. Important examples include Measles, Rubella, and Chickenpox. In these diseases, rhinitis usually appears before the characteristic skin rash. In measles, coryza is a prominent early symptom and appears before the rash develops. In rubella, patients may develop mild rhinitis during the initial stage of the illness. In chickenpox, nasal symptoms may also occur before the appearance of the skin lesions. Typically, rhinitis develops two to three days before the skin rash. Therefore, the presence of rhinitis during the early phase of these infections can act as an important early clinical sign of the disease.
Bacterial Rhinitis
Bacterial rhinitis may occur as a primary infection or as a secondary infection following viral rhinitis.
- Primary bacterial rhinitis occurs mainly in children. It is commonly caused by bacteria such as Streptococcus pneumoniae, Streptococcus pyogenes, and Staphylococcus aureus. In some patients, a greyish-white, thick membrane may form inside the nasal cavity. When a clinician attempts to remove this membrane, bleeding may occur because the underlying nasal mucosa is inflamed.
- Secondary bacterial rhinitis develops when bacteria infect the nasal mucosa during a viral infection such as the Common Cold. It usually appears during the later stage of acute viral rhinitis, when the damaged nasal mucosa becomes more susceptible to bacterial invasion.
Diphtheritic Rhinitis
Diphtheritic rhinitis refers to nasal infection caused by Corynebacterium diphtheriae and is a manifestation of Diphtheria. This condition has become rare because of widespread vaccination, but it remains clinically important. Nasal diphtheria may occur as a primary infection in the nose or may develop secondarily after infection of the throat, known as faucial diphtheria. A greyish pseudomembrane usually covers the inferior turbinate and the floor of the nasal cavity. This membrane is thick and firmly attached to the mucosa. When clinicians attempt to remove it, bleeding usually occurs. Patients may also develop excoriation of the anterior nares and the upper lip because of the irritating nasal discharge.
Management includes strict isolation of the patient, administration of diphtheria antitoxin, and treatment with systemic antibiotics such as Penicillin.
Irritative Rhinitis
Irritative rhinitis occurs when the nasal mucosa is exposed to irritating environmental or chemical substances. Common irritants include dust, smoke, ammonia fumes, formalin vapors, and acidic gases. Trauma to the nasal mucosa during intranasal procedures or during removal of a nasal foreign body may also lead to irritative rhinitis.
These irritants produce an immediate catarrhal reaction in the nasal mucosa. As a result, the patient develops sneezing, nasal discharge, and nasal congestion. In many cases, the symptoms improve quickly once the irritant is removed. However, if the nasal epithelium becomes damaged, the symptoms may continue for several days.
——– End of the Chapter——–
High-Yield Points for Exams
- Rhinovirus is the most common cause of the common cold.
- The incubation period of acute viral rhinitis is 1–4 days.
- The disease usually lasts 7–14 days.
- Nasal discharge changes from watery to mucopurulent.
- Four stages: Prodromal → Early reaction → Leucocytic infiltration → Resolution.
- Antibiotics are not required unless a bacterial infection occurs.
- Sinusitis and otitis media are common complications.
- Grey pseudomembrane suggests diphtheritic rhinitis.
NEET PG Style MCQs
- The most common cause of acute rhinitis is
A. Influenza virus
B. Rhinovirus
C. Adenovirus
D. Parainfluenza virus - Incubation period of common cold is
A. 12 hours
B. 1–4 days
C. 7 days
D. 14 days - Mucopurulent nasal discharge occurs in
A. Prodromal stage
B. Early reaction stage
C. Leucocytic infiltration stage
D. Resolution stage - The most common complication of acute rhinitis is
A. Sinusitis
B. Meningitis
C. Laryngitis
D. Epiglottitis - Rhinovirus belongs to
A. Picornavirus
B. Orthomyxovirus
C. Paramyxovirus
D. Retrovirus - Aspirin should be avoided in viral rhinitis because it
A. Causes bleeding
B. Increases viral shedding
C. Causes hypertension
D. Causes sedation - Coryza preceding rash is typical of
A. Measles
B. Tuberculosis
C. Typhoid
D. Cholera - Primary bacterial rhinitis is most common in
A. Adults
B. Elderly
C. Children
D. Pregnant women - Grey pseudomembrane in nose indicates
A. Allergic rhinitis
B. Atrophic rhinitis
C. Diphtheritic rhinitis
D. Vasomotor rhinitis - Which drug reduces nasal mucosal edema
A. Antihistamine
B. Nasal decongestant
C. Antibiotic
D. Antacid
MCQ Answers with Explanations
- B – Rhinovirus is the most common cause.
- B – 1–4 days is the incubation period.
- C – Leucocytic infiltration stage produces mucopurulent discharge.
- A – Sinusitis occurs most frequently.
- A – Picornavirus family.
- B – Aspirin increases viral shedding.
- A – Measles produces coryza before rash.
- C – Primary bacterial rhinitis occurs mainly in children.
- C – Diphtheritic rhinitis produces grey pseudomembrane.
- B – Decongestants reduce mucosal edema.
——– End——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Acute Rhinitis Ent Notes For Mbbs Students, Acute Rhinitis Exam Guide For Neet Pg Preparation, Acute Rhinitis Stages Explained For Medical Students, Acute Rhinitis Pathophysiology Simplified Ent Notes, Acute Rhinitis Clinical Features Diagnosis And Treatment Notes, Acute Rhinitis Complications Sinusitis Otitis Media Ent Guide, Acute Rhinitis Mnemonics Mcqs And Revision Notes, Acute Rhinitis Cbme Curriculum Ent Study Guide, Acute Rhinitis Viva Questions For Ent Practical Exam, Acute Rhinitis Quick Revision Notes For Medical Entrance Exams, Acute Rhinitis Viral Vs Bacterial Rhinitis Differences, Acute Rhinitis Summary For Mbbs And Pg Students, Acute Rhinitis Exam Preparation Notes For Indian Medical Students