|
The following CBME core competencies are covered in this chapter.
|
Granulomatous Conditions of the Nose and Paranasal Sinuses
Introduction to Nasal Granulomas
A granuloma represents an organised collection of activated macrophages that forms in response to persistent chronic inflammation. These specialised macrophages transform into epithelioid cells, and many of them fuse together to create multinucleated giant cells, forming the characteristic granulomatous architecture. Granulomas develop in a wide spectrum of infective, inflammatory, and neoplastic conditions affecting the nose and paranasal sinuses, and they typically arise from bacterial infections, fungal infections, or idiopathic causes. Since many granulomatous lesions are intimately associated with systemic diseases, you must always evaluate the patient for systemic involvement at the time of diagnosis.
Biopsy remains essential in all suspected cases because it serves two critical purposes. First, it confirms the diagnosis of granulomatous disease definitively. Second, it helps exclude malignancy, as many of these conditions clinically mimic tumours with alarming similarity. These conditions often present with overlapping clinical features, which makes diagnosis challenging, but their treatment differs significantly. Therefore, accurate identification becomes critical for patient outcomes.
Classification of Granulomatous Diseases
Granulomatous diseases of the nose and paranasal sinuses fall into three major categories based on their underlying aetiology. Understanding this classification helps you approach diagnosis systematically.
| Category | Conditions | Key Features |
|---|---|---|
| Infective | Tuberculosis, Leprosy, Rhinoscleroma, Aspergillosis, Histoplasmosis, Blastomycosis, Syphilis, Rhinosporidiosis, Mucormycosis, Candidiasis | Specific organisms cause these conditions; they respond to antimicrobial therapy |
| Inflammatory | Granulomatosis with Polyangiitis (Wegener's), Churg–Strauss syndrome, Cholesterol granuloma, Eosinophilic granuloma, Sarcoidosis | Autoimmune or idiopathic origin; requires immunosuppressive therapy |
| Neoplastic | Extranodal NK/T-cell lymphoma | Malignant condition; treated with chemotherapy and radiotherapy |
Infective Granulomas
Rhinoscleroma
Rhinoscleroma is a chronic, progressive granulomatous condition that primarily affects the nose but can also involve the nasopharynx, larynx, trachea, and bronchi. When the larynx is involved, we specifically call it scleroma of the larynx. The disease shows a slight female preponderance, and it typically affects individuals between 10 and 30 years of age.
Epidemiology. Rhinoscleroma is considered a tropical disease, with the highest prevalence in Africa and Central America, though cases can occur worldwide due to migration. In India, it is seen more often in the northern than in the southern parts.
Aetiology. Klebsiella rhinoscleromatis causes rhinoscleroma. This gram-negative bacillus belongs to the Enterobacteriaceae family. Anton von Frisch first identified the organism in 1882, hence the alternative name “Frisch bacillus.”
Mode of spread. The bacterium spreads through droplet infection or by inhalation of contaminated material. Once inhaled, it establishes chronic infection in the nasal mucosa, leading to the characteristic granulomatous response.
Clinical Stages. The disease progresses through three distinct stages:
- Stage 1: Catarrhal or Atrophic Stage. The catarrhal stage begins with symptoms identical to nonspecific rhinitis. Patients initially experience nasal discharge and obstruction that resemble common cold symptoms. However, as the disease progresses, the nasal discharge becomes purulent and foul-smelling, and crusting develops within the nasal cavity. This stage can easily be mistaken for simple chronic rhinitis or atrophic rhinitis, which often leads to diagnostic delay.
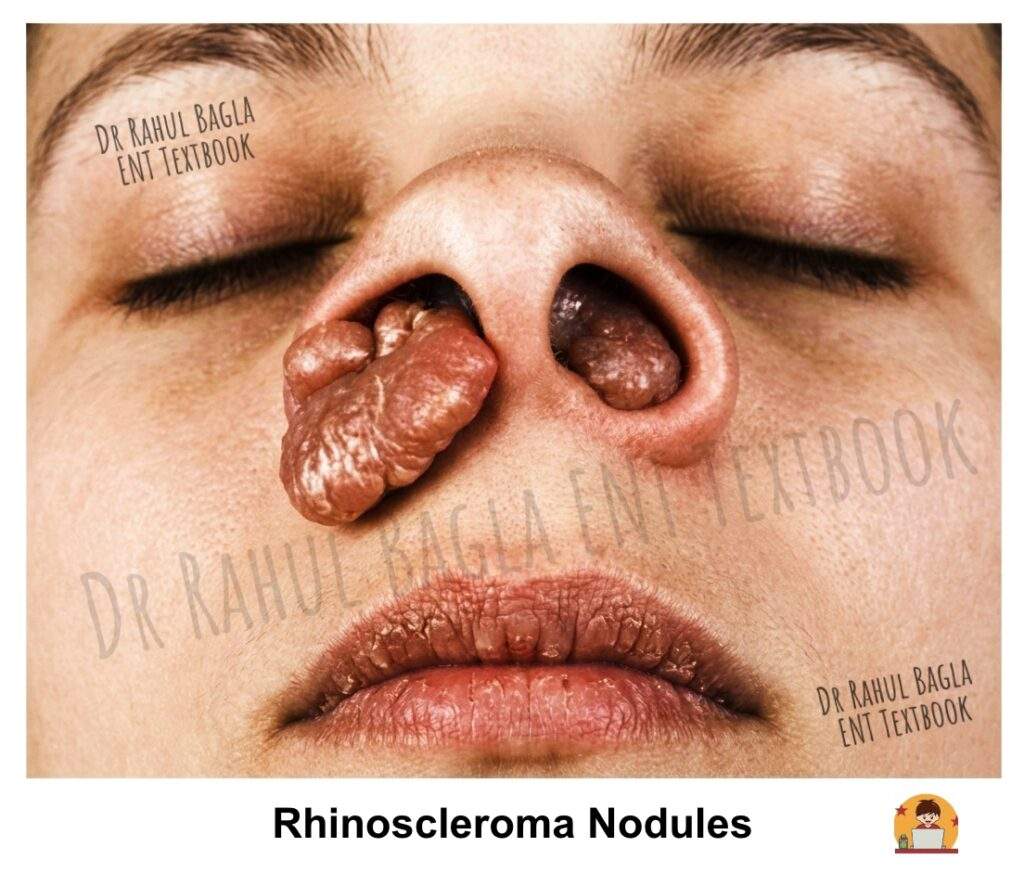
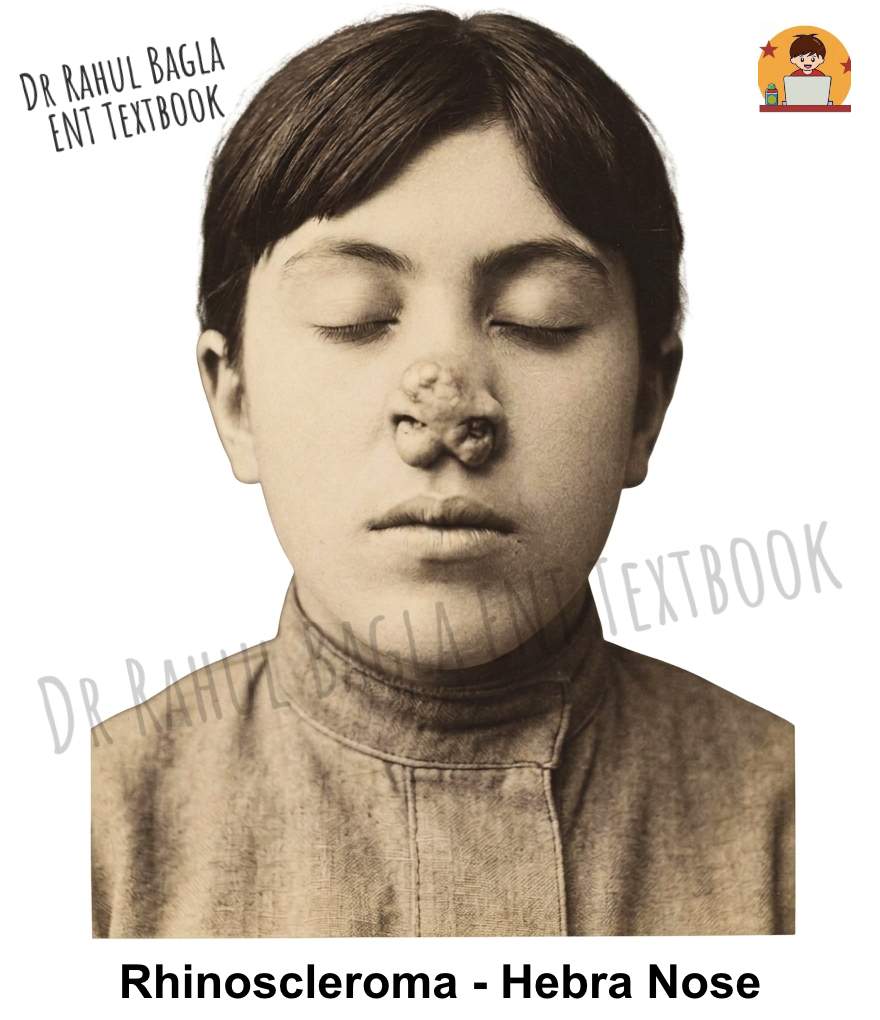
- Stage 2: Granulomatous, Proliferative, or Nodular Stage. During this stage, intranasal rubbery nodules or polyps develop. These lesions are firm to palpation and may bleed easily, causing epistaxis. As the disease advances, destruction of the nasal cartilage occurs, leading to nasal deformity. The external nose becomes swollen and develops a characteristic woody feel because of subdermal infiltration, and this appearance is known as Hebra nose. Furthermore, the external nose becomes enlarged and elongated, resembling the nose of a tapir, hence the term Tapir nose. Patients with laryngeal involvement may experience dysphonia, and tracheal involvement can cause various degrees of airway obstruction.
- Stage 3: Sclerotic, Cicatricial or Fibrotic Stage. This represents the end stage of the disease, characterised by extensive cicatrisation (the process of scar formation and tissue repair during healing) and fibrosis. The nasal passages become narrowed or stenosed due to the contracture of scar tissue. Patients may have persistent nasal obstruction and cosmetic deformity at this stage, and subglottic stenosis with respiratory distress may also occur.
Diagnosis. The diagnosis of rhinoscleroma relies on histopathological examination. Three characteristic findings are pathognomonic:
- Mikulicz cells: Appear as large, vacuolated histiocytes containing phagocytosed Klebsiella rhinoscleromatis organisms. They look like foam cells with clear cytoplasm on H&E staining.
- Russell bodies: These are homogeneous, eosinophilic inclusion bodies found within plasma cells. They represent accumulated immunoglobulins and appear as brightly eosinophilic spherical structures.
- Pseudoepitheliomatous hyperplasia: The overlying epithelium shows marked acanthosis and downward proliferation, mimicking squamous cell carcinoma.
Treatment
- Medical Management. Tetracycline or ciprofloxacin forms the mainstay of treatment. Continue antibiotics for weeks to months, depending entirely on the clinical response, and continue until two consecutive cultures are negative. Steroids can be combined to reduce fibrosis. Additionally, local application of 2% acriflavine dye for 6–8 weeks has shown effectiveness.
- Surgical Management. Surgical intervention becomes necessary for complications. Dilatation of the nasal cavity may be required for stenosis, and corrective rhinoplasty can address external deformities after the disease is controlled medically.
Nasal Tuberculosis
Aetiology. Mycobacterium tuberculosis, an acid-fast bacillus, causes nasal tuberculosis.
Mode of spread. The infection reaches the nose through three possible routes: direct inoculation by fingernail trauma (a common habit of picking the nose), spread from open pulmonary tuberculosis via infected sputum, or hematogenous dissemination from a primary infection elsewhere in the body.
Clinical Forms and Features. Nasal tuberculosis presents in three main clinical patterns:
- Lupus Vulgaris (Nodular Form). Lupus vulgaris is a low-grade tuberculous infection that typically begins in the nasal vestibule and spreads to adjacent skin and the skin of the nose and face. It results from direct bacterial inoculation into the nasal skin of an immunocompetent patient. Clinically, you will see apple jelly nodules, which are shiny, reddish-brown papules or nodules in the nasal vestibule. When you apply pressure or a vasoconstrictor, these nodules become more visible because the surrounding area blanches while the nodule remains unaffected. The nodules may eventually coalesce and form an ulcer with a pale, granular base and undermined edges.
- Ulcerative Form. Nasal tuberculosis mainly affects the cartilaginous part of the nasal septum, leading to septal perforation. Patients commonly present with nasal obstruction, crusting, discharge, and epistaxis. Importantly, it does not cause saddle nose deformity because it spares the bony septum. This feature helps differentiate it from syphilis, where involvement of the bony septum typically leads to saddle nose deformity.
- Sinus Granuloma.Tubercular sinus disease typically presents with diffuse soft-tissue swelling and multiple discharging sinuses. This presentation is usually secondary to bone destruction from osteomyelitis of the frontal bone, and rarely the maxilla or zygomatic bone. CT imaging reveals a soft tissue mass with or without bone destruction.
Diagnosis (Biopsy and Histopathology). The diagnosis is confirmed by biopsy. Histopathology shows characteristic epithelioid cell granulomas with Langhans-type giant cells, central caseation necrosis, and acid-fast bacilli on Ziehl-Neelsen staining.
Microbiological tests include culture on Löwenstein–Jensen medium, which typically takes around 6 weeks. CBNAAT (Cartridge-Based Nucleic Acid Amplification Test) can be performed on pus or discharge from sinuses or nodules, providing rapid diagnosis within hours. The Mantoux test involves purified protein derivative injected intradermally, producing a wheal and flare reaction due to delayed hypersensitivity, and you read the results after 48–72 hours.
When clinical suspicion is very strong but confirmatory tests are negative, a therapeutic trial with antitubercular therapy may be initiated. You should always exclude associated pulmonary tuberculosis by chest X-ray.
Treatment. Nasal tuberculosis responds well to standard antitubercular treatment (ATT). The intensive phase consists of isoniazid, rifampicin, ethambutol, and pyrazinamide for 2 months. The continuation phase involves isoniazid and rifampicin for 4 months. For multidrug-resistant tuberculosis (MDR-TB), treatment is guided by culture-sensitivity tests and requires a longer duration with second-line drugs.
Syphilis
Aetiology. Treponema pallidum, a spirochaete, causes syphilis. This spirochaete can involve the nose at any age. The disease is now uncommon, and early diagnosis often becomes difficult, especially when patients have already received antibiotics for other conditions.
Classification. Syphilis occurs as congenital or acquired disease. Congenital syphilis presents in early (first 2 years) and late forms, while acquired syphilis progresses through primary, secondary, and tertiary stages
Nasal Manifestations by Stage
- Primary Syphilis. The typical lesion is a chancre appearing 3–4 weeks after initial contact. Chancers are hard, non-tender ulcerated papules that disappear after 6–10 weeks of infection. Common sites are the external nose or vestibule.
- Secondary Syphilis. This stage starts 6–10 weeks after inoculation. Nasal involvement is rare during this stage, though mucous patches may occur.
- Tertiary Syphilis. The characteristic lesion of tertiary syphilis is the gumma, which can involve the mucous membrane, periosteum, and bone. Gummas consist of nodules containing plasma cells, lymphocytes, epithelioid cells, and fibroblasts. Perivascular cuffing and endarteritis by these cells lead to narrowing of the vessel lumen, ultimately causing necrosis and ulceration.
Clinical Features. Patients commonly present with nasal obstruction, crusting, bleeding, and foul-smelling discharge. The disease destroys the bony part of the nasal septum, which leads to the classical saddle nose deformity. This feature clearly distinguishes it from tuberculosis, which spares the bony septum. Patients may also report nasal tenderness and headache.
Complications. Advanced disease can cause septal perforation, palatal and nasal wall perforation, sequestrum formation, and collapse of the nasal bridge. Progressive scarring may lead to nasal stenosis and atrophic rhinitis. In rare cases, infection may spread intracranially.
Diagnosis. Syphilis progresses slowly over the years if untreated. Screening begins with the VDRL test. A positive result requires confirmation with specific tests such as FTA-ABS and TPHA.
Treatment
- Primary, Secondary, and Early Latent Syphilis – Single intramuscular dose of 2.4 million units of benzathine penicillin
- Latent and Tertiary Syphilis – 2.4 million units of intramuscular benzathine penicillin weekly for three weeks
- Local Treatment – Clearance of crusts and cleaning of nasal passages with alkaline nasal douches 2–3 times daily
Sequelae Management. Atrophic rhinitis and deformity may persist after the disease and require appropriate medical and surgical management.
Leprosy (Hansen’s Disease)
Aetiology. Mycobacterium leprae infection causes leprosy. This acid-fast bacillus has a long incubation period of 3–10 years.
Classification. The disease forms a spectrum based on host immunity.
- Tuberculoid (high immunity) – At the tuberculoid end, patients show few skin lesions, and microscopy reveals absent or very few bacilli. This form reflects strong immunity, so it remains the least contagious and relatively benign.
- Borderline-tuberculoid
- Borderline
- Borderline-lepromatous
- Lepromatous (low immunity) – At the lepromatous end, patients develop multiple widespread skin lesions filled with numerous bacilli. This pattern indicates poor immunity, making the disease more severe and highly infectious.
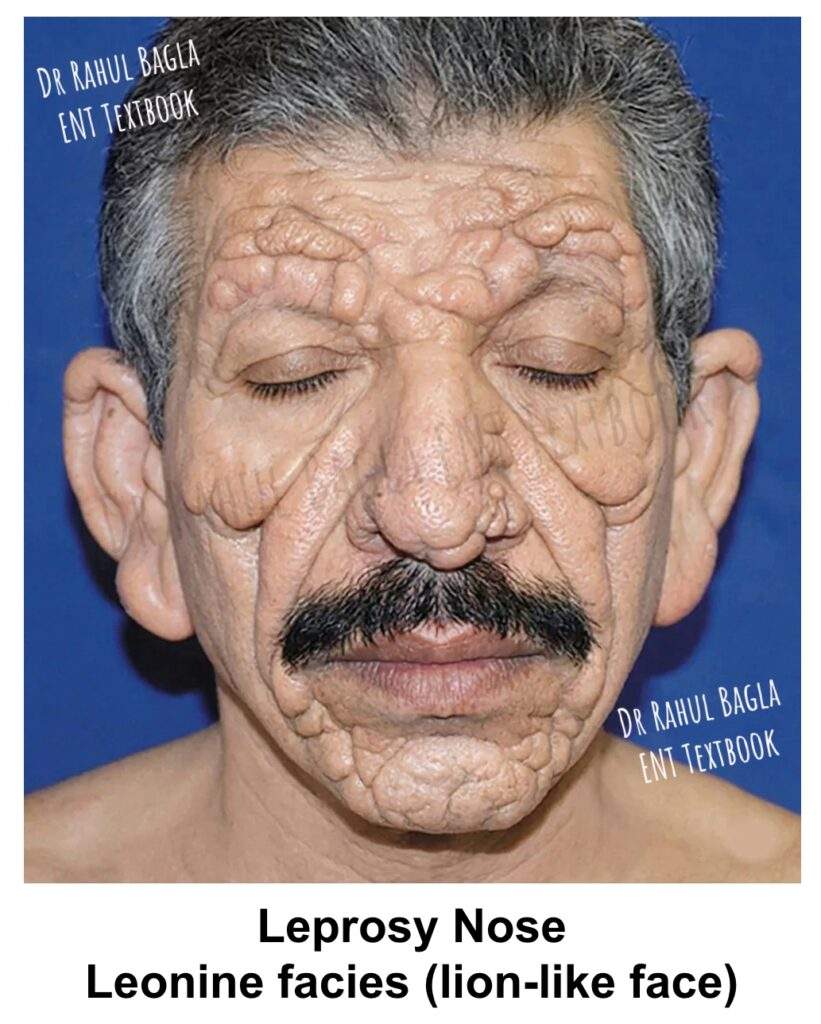
Unique Features of M. leprae. Leprae is unique among bacteria because it selectively invades peripheral nerves, causing irreversible cutaneous anaesthesia and paralysis of muscles in the extremities and face. The earlobes and nose are especially enlarged and infiltrated in lepromatous leprosy. Widespread facial skin lesions give rise to the characteristic Leonine facies (lion-like face).
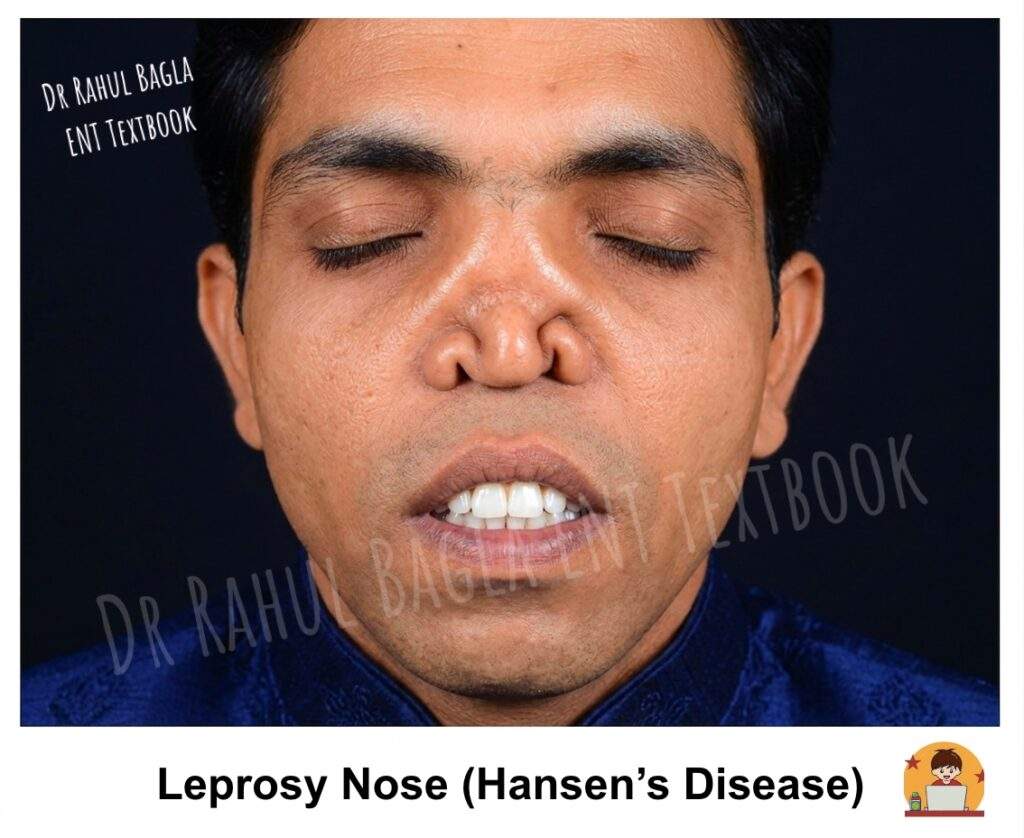
Clinical Features. Lepromatous leprosy involves the nose early in the disease course. Patients commonly present with nasal obstruction, crusting, bleeding, and a reduced sense of smell (hyposmia). The disease may also affect other head and neck sites such as the auricle, hard and soft palate, epiglottis, and larynx. On examination, the nasal mucosa shows pale yellowish thickening with nodules or plaques. As the disease progresses, it produces diffuse nodular infiltration, especially over the inferior turbinate and nasal septum. In advanced stages, patients may develop septal perforation, saddle nose deformity, and atrophic rhinitis.
Treatment. Long-term multidrug therapy, using dapsone, rifampicin, and clofazimine. Minocycline, a tetracycline antibiotic, also shows effectiveness against Mycobacterium leprae infection.
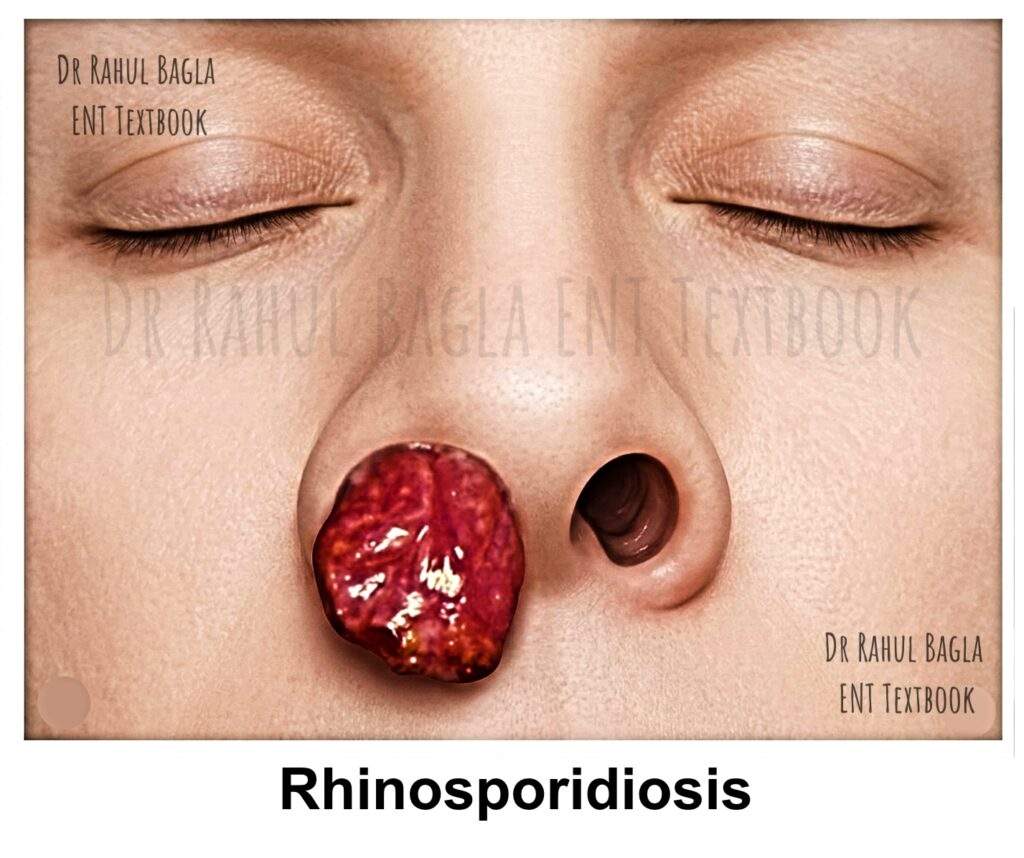
Rhinosporidiosis
Epidemiology. Rhinosporidiosis is a chronic, indolent granulomatous disease that is endemic in specific regions, most notably southern India and Sri Lanka. Therefore, it is a classic exam topic that highlights geographic predilection.
Aetiology. Rhinosporidiosis was previously thought to be caused by the fungus, Rhinosporidium seeberi; molecular studies have now confirmed it to be a prokaryotic Cyanobacterium, closely related to the Microcystis species.
Mode of spread. This organism thrives in stagnant, fresh water, and transmission typically occurs when individuals swim or bathe in contaminated ponds, allowing the pathogen to enter through minor cuts or abrasions in the nasal mucosa. Interestingly, the disease also affects animals like cattle, horses, and dogs, suggesting a common environmental source of infection.
Pathogenesis and Life Cycle. Understanding the life cycle of Rhinosporidium seeberi is key to grasping its clinical presentation. The organism progresses through three distinct stages within the host tissue:
- Trophic Stage: The cycle begins with a small, 6-8 μm endospore entering the submucosa. This endospore, with a distinct chitinous wall, contains a clear cytoplasm and a vesicular nucleus. It then begins to grow, undergoing multiple nuclear and cytoplasmic divisions. Trophocyte becomes large, filled with young endospores.
- Sporangium Development: The mature, enlarged trophocyte develops into a large, thick-walled sporangium. These sporangia are the pathognomonic feature of the disease, measuring a massive 200–250 μm in diameter—a size that can be seen with a low-power microscope. Each sporangium is filled with thousands (up to 16,000) of endospores.
- Endospore Production and Release: The mature sporangium eventually ruptures, releasing a cloud of infective endospores into the surrounding tissue. These liberated endospores then begin the cycle anew, leading to local spread and recurrence. Some endospores may also disseminate via lymphatics or bloodstream, though this is rare.
Clinical Features. Rhinosporidiosis most commonly affects young to middle-aged individuals (10-40 years) and shows a marked male predominance (4:1). The disease is characterised by a persistent, slow-growing, polypoidal mass in the nasal cavity, though it can affect other sites.
- Nasal Manifestations (85% of cases): The classic presentation is a fleshy, strawberry-like mass. This vascular, friable polyp is typically pink to purple and attached to the nasal septum or lateral wall. Its surface is studded with pathognomonic greyish-white dots, which are the visible sporangia. The mass is extremely vascular, bleeding easily upon the slightest touch (a key clinical sign). Patients often complain of progressive nasal obstruction and blood-stained nasal discharge.
- Extranasal Manifestations: While the nose is the primary site, the disease can occasionally involve the nasopharynx, lips, palate, uvula, conjunctiva, larynx, and even the genitals. Therefore, a diagnosis may be delayed when the disease presents at these less common sites.
Diagnosis and Histopathology
Diagnosis is primarily clinical, supported by histopathological examination of the excised mass. A biopsy is avoided pre-operatively due to the risk of severe bleeding.
- Gross Appearance: A fleshy, pedunculated or sessile polyp with a characteristic strawberry-like surface.
- Microscopy: Histopathology with Hematoxylin and Eosin (H&E) stain reveals the pathognomonic sporangia in various stages of development. These large, thick-walled structures, containing numerous endospores, are diagnostic. Fungal stains like Gomori methenamine silver (GMS) and periodic acid-Schiff (PAS) can also highlight the organism. A chronic inflammatory reaction with epithelioid cell granulomas and giant cells is seen in about 50% of cases.
Treatment. Treatment is primarily surgical, as medical therapy plays a limited role.
- Surgical Excision: Complete excision of the mass with electrocoagulation of its base is the treatment of choice to prevent recurrence. Endoscopic endonasal surgery is the preferred approach, as it allows for precise, complete excision and good visualisation of the base.
- Medical Therapy: Dapsone is the most studied medical therapy. It is believed to inhibit the maturation of sporangia. It is not a primary treatment but is often used as an adjuvant to surgery, given post-operatively for several months to help reduce the risk of recurrence.
Aspergillosis
Aspergillosis is most commonly caused by Aspergillus fumigatus, A. flavus, or A. niger. The clinical presentation depends on the host’s immune status.
- Non-Invasive (Fungus Ball): This is the most common form, occurring in immunocompetent individuals. It presents as a chronic, unilateral sinusitis. On exploration, the maxillary sinus is filled with a characteristic fungus ball—a compact, cheesy, greenish-black or brownish-black concretion.
- Invasive Aspergillosis: This occurs in immunocompromised patients (e.g., those on chemotherapy, steroids, or with uncontrolled diabetes). It is an aggressive, angioinvasive infection that can rapidly destroy tissue. Clinically, it may present with facial pain, swelling, and a black or greyish necrotic membrane on the nasal mucosa. Treatment requires aggressive surgical debridement and systemic antifungals like Amphotericin B or voriconazole.
Mucormycosis (Zygomycosis)
Mucormycosis is a rapidly progressive and potentially fatal fungal infection caused by fungi of the order Mucorales (e.g., Rhizopus, Mucor). Its high-yield association is with uncontrolled diabetes mellitus, especially in the setting of diabetic ketoacidosis (DKA). Immunosuppression is another major risk factor.
The hallmark of mucormycosis is its affinity for blood vessels. The hyphae invade the arterial wall, causing thrombosis, ischemia, and rapid tissue necrosis. This leads to the classic clinical sign: a black, necrotic eschar in the nasal cavity or on the palate. From the nose and sinuses, the infection can quickly spread to the orbit (causing proptosis, ophthalmoplegia), the brain (cavernous sinus thrombosis, meningitis), and the palate (leading to perforation).
Management is an emergency and involves a three-pronged approach:
- Urgent Surgical Debridement: Repeated, aggressive debridement of all necrotic tissue until healthy, bleeding tissue is encountered.
- Antifungal Therapy: High-dose intravenous Amphotericin B is the first-line drug. Posaconazole and isavuconazole are other options.
- Control of Underlying Disease: This is critical. Immediate correction of hyperglycemia and metabolic acidosis (DKA) is essential.
Inflammatory Granulomas
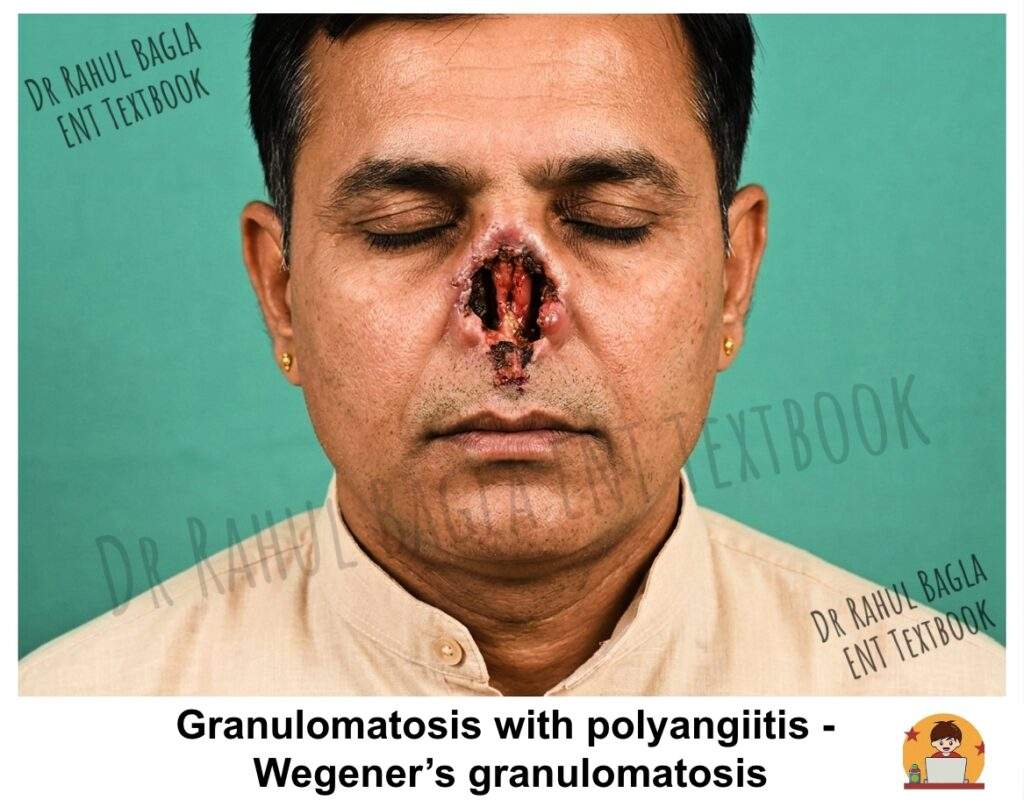
Granulomatosis with Polyangiitis (GPA)
Granulomatosis with polyangiitis (GPA), formerly known as Wegener’s granulomatosis, is a systemic, autoimmune, necrotising vasculitis that primarily affects small to medium-sized vessels. It is defined by the classic triad of involvement of the upper respiratory tract, lower respiratory tract (lungs), and kidneys.
Aetiology and Pathogenesis
GPA is strongly associated with antineutrophil cytoplasmic antibodies (ANCA), specifically the cytoplasmic (c-ANCA) pattern, which targets proteinase 3 (PR3). This suggests an autoimmune aetiology, though the exact trigger remains unknown. The disease leads to necrotising granulomatous inflammation and vasculitis.
Clinical Features
The presentation is variable, but upper respiratory tract involvement occurs in over 80% of patients and is often the first manifestation. This can be “localised” (limited to the respiratory tract) or “generalised” (with systemic involvement like renal disease).
- Nasal and Sinus: Chronic rhinitis, nasal obstruction, purulent or bloody discharge, severe crusting, and epistaxis are common. Progressive destruction can lead to saddle-nose deformity (due to septal perforation and collapse of the nasal bridge) and erosion of the turbinates and sinus walls.
- Aural: Otitis media with effusion and sensorineural hearing loss can occur.
- Oral: “Strawberry gingival hyperplasia” is a characteristic, though not pathognomonic, finding, where the gums appear friable and hyperplastic.
- Laryngeal: Subglottic stenosis is a serious complication that can cause stridor and airway compromise.
- Systemic: This includes pulmonary involvement (cough, hemoptysis, cavitary lesions) and rapidly progressive glomerulonephritis (which can lead to renal failure). Other features include ocular involvement (proptosis), skin nodules, and arthritis.
Diagnosis
The diagnosis is based on a combination of clinical, serological, and histopathological findings.
- Serology: c-ANCA (anti-PR3) is highly sensitive and specific for GPA, especially in active, generalised disease. ESR and CRP are also elevated.
- Histopathology: Biopsy from the nasal mucosa or a pulmonary lesion typically shows a triad of necrosis, granulomatous inflammation, and necrotising vasculitis. The vasculitis involves small arteries and veins.
The American College of Rheumatology (ACR) criteria for GPA require at least 2 of the following 4 features:
- Nasal or oral inflammation (painful or painless oral ulcers, purulent or bloody nasal discharge).
- Abnormal chest X-ray (nodules, fixed infiltrates, or cavities).
- Urinary sediment with red cell casts or hematuria.
- Granulomatous inflammation on biopsy.
Treatment
Without treatment, GPA is rapidly fatal. The cornerstone of treatment is immunosuppression.
- Induction Therapy: The combination of cyclophosphamide and corticosteroids is the traditional gold standard for inducing remission in severe, active disease. Rituximab (a monoclonal antibody against CD20) is now an equally effective alternative, particularly for patients who cannot tolerate cyclophosphamide.
- Maintenance Therapy: After remission, patients are switched to less toxic agents like methotrexate or azathioprine to maintain remission and prevent relapse.
- Monitoring: Serial c-ANCA levels can be useful to monitor disease activity and guide treatment.
- Symptomatic Management: This includes nasal saline douching, topical steroids, and endoscopic sinus surgery to manage sinus disease. Surgical repair of a saddle-nose deformity or septal perforation is only performed when the disease has been in remission for at least one year.
Sarcoidosis
Sarcoidosis is a multisystem granulomatous disorder of unknown aetiology, characterised by the formation of non-caseating granulomas. While the lungs and lymph nodes are most commonly involved, sinonasal sarcoidosis occurs in a small percentage of patients (<5%).
Aetiology and Pathology. The exact cause of sarcoidosis is unknown, but it is thought to result from an exaggerated immune response to an unknown antigen in genetically susceptible individuals. The hallmark is the presence of non-caseating epithelioid cell granulomas on histopathology. This is the key feature that distinguishes it from tuberculosis.
Clinical Features. Sinonasal involvement can manifest in various ways:
- Nasal Symptoms: Nasal obstruction, crusting, epistaxis, and facial pain are common.
- Examination: The nasal mucosa may appear pale and hypertrophied. Multiple, small, pale granulomas can give the mucosa a “cobblestone” or granular appearance, sometimes referred to as “strawberry skin.” This can lead to ulceration, crusting, and eventually, septal perforation.
- Cutaneous Manifestations: Lupus pernio is a characteristic cutaneous manifestation of sarcoidosis, presenting as violaceous, indurated plaques on the nose, cheeks, and ears.
- Associated Syndromes: Heerfordt’s syndrome (uveoparotid fever) is a classic presentation involving parotid gland enlargement, facial nerve palsy, uveitis, and fever.
Diagnosis and Staging. Diagnosis is based on a combination of clinical, radiographic, and histopathological findings, with the exclusion of other granulomatous diseases like tuberculosis.
- Histopathology: Biopsy of the nasal lesion shows the pathognomonic non-caseating granulomas.
- Serology: Serum angiotensin-converting enzyme (ACE) levels are elevated in approximately 85% of patients with active disease. Serum and urinary calcium levels may also be elevated.
- Imaging: A chest X-ray or CT scan is crucial, often revealing bilateral hilar lymphadenopathy (BHL) and pulmonary infiltrates. A staging system (Stages I-IV) is used for pulmonary sarcoidosis. For sinonasal involvement, a simple staging system exists: Stage I (reversible nasal disease), Stage II (moderate, potentially reversible disease with sinus involvement), and Stage III (severe, irreversible, extensive disease).
Treatment. The course of sarcoidosis is variable, and many cases are self-limiting.
- Medical Therapy: Corticosteroids are the mainstay of treatment for symptomatic or progressive disease. For chronic or steroid-resistant cases, steroid-sparing agents like methotrexate, azathioprine, or hydroxychloroquine (especially for skin and sinonasal disease) are used.
- Supportive Care: For sinonasal symptoms, regular nasal douching with saline is essential to manage crusting. Glucose and glycerine drops can help moisturise the nasal mucosa. Surgery is reserved for cosmetic correction of nasal deformities (e.g., saddle-nose) only when the disease is inactive.
Neoplastic Granuloma
Extranodal NK/T-Cell Lymphoma (ENKTCL)
Extranodal NK/T-cell lymphoma (ENKTCL), previously known by many names including “lethal midline granuloma” and “polymorphic reticulosis,” is a rare, aggressive type of non-Hodgkin lymphoma. It is characterised by a destructive, necrotic lesion of the midface.
Aetiology and Pathology. ENKTCL is strongly associated with the Epstein-Barr virus (EBV). It arises from natural killer (NK) cells or, less commonly, T-cells. The defining histological features are an angiocentric and angioinvasive growth pattern, where the neoplastic lymphoid cells infiltrate and destroy blood vessel walls, leading to massive tissue necrosis.
Clinical Features. The disease typically presents in middle-aged to older adults (5th-6th decade) with a male predominance.
- Localized Disease: The disease usually starts unilaterally in the nasal cavity. Patients present with progressive nasal obstruction, purulent and often foul-smelling discharge, and severe epistaxis.
- Midfacial Destruction: The hallmark is relentless, progressive destruction of the midface. It can erode through the nasal septum, hard palate, and the skin of the nose and face, creating a large, central facial defect. Unlike GPA, there is no associated renal or pulmonary involvement in the early stages.
- Systemic Involvement: The disease can disseminate to involve the skin, gastrointestinal tract, and other sites.
Diagnosis and Differential Diagnosis. A high index of suspicion is necessary, as the early presentation mimics chronic sinusitis.
- Histopathology and Immunohistochemistry: Multiple, deep biopsies are required to make the diagnosis. The tissue shows a dense, atypical lymphoid infiltrate with angioinvasion and extensive necrosis. Immunohistochemistry is essential and typically shows positivity for CD56 (a marker for NK cells), CD2, and cytoplasmic CD3ε. The tumour cells are also EBV-positive.
- Imaging: CT and MRI are crucial to assess the extent of local destruction and for staging the disease.
- Differential Diagnosis: It is critical to differentiate ENKTCL from GPA, as the treatments are entirely different. The absence of renal, pulmonary, and c-ANCA positivity, coupled with the aggressive local destruction, points towards ENKTCL.
Treatment. The management of ENKTCL has evolved, and it is no longer a uniformly fatal disease.
- Combined Modality Therapy: The current standard of care for localised ENKTCL is combined chemotherapy and radiotherapy. “Sandwich” regimens, where patients receive a few cycles of chemotherapy (e.g., SMILE protocol: dexamethasone, methotrexate, ifosfamide, L-asparaginase, etoposide) followed by radiation, are effective. For disseminated disease, chemotherapy is the mainstay.
——– End of the Chapter——–
High-yield points for revision
| Feature | Rhinoscleroma | Tuberculosis | Syphilis | Leprosy | Rhinosporidiosis | GPA | ENKTCL |
|---|---|---|---|---|---|---|---|
| Aetiology | K. rhinoscleromatis | M. tuberculosis | T. pallidum | M. leprae | Microcystis (cyanobacterium) | Autoimmune (c-ANCA) | EBV-associated |
| Nasal septum | Cartilage destruction | Cartilaginous perforation | Bony destruction → Saddle nose | Septal perforation | Not typically involved | Saddle nose | Midfacial destruction |
| Pathognomonic feature | Mikulicz cells, Russell bodies | Caseating granulomas, Langhans giant cells | Gumma | Nerve involvement, Leonine facies | Strawberry-like mass with white dots | c-ANCA positivity, strawberry gingiva | Angioinvasion, CD56+ |
| Treatment | Tetracycline, ciprofloxacin | ATT | Penicillin | MDT (dapsone, rifampicin, clofazimine) | Surgical excision + dapsone | Cyclophosphamide + steroids | Chemotherapy + radiotherapy |
NEET PG MCQs
-
A 25-year-old woman from northern India presents with progressive nasal obstruction and a woody, swollen external nose resembling a tapir. Biopsy reveals large vacuolated histiocytes containing intracellular bacilli. What is the most likely diagnosis?
A) Nasal tuberculosis B) Rhinoscleroma C) Leprosy D) Sarcoidosis -
A patient presents with a fleshy, strawberry-like polyp in the nasal cavity with greyish-white dots on its surface. The mass bleeds profusely on touch. What is the treatment of choice?
A) Systemic amphotericin B B) Complete surgical excision with electrocoagulation C) Tetracycline for 6 weeks D) Radiotherapy -
A diabetic patient with uncontrolled blood sugar presents with black eschar over the palate and nasal cavity, proptosis, and ophthalmoplegia. What is the most appropriate next step in management?
A) Start oral fluconazole B) Perform urgent surgical debridement C) Prescribe broad-spectrum antibiotics D) Order an MRI brain -
A 45-year-old man presents with saddle nose deformity, chronic nasal crusting, hemoptysis, and hematuria. Which investigation is most likely to confirm the diagnosis?
A) Chest X-ray B) c-ANCA (anti-PR3) antibodies C) Nasal biopsy for acid-fast bacilli D) VDRL test -
A 55-year-old man presents with a progressively destructive midline facial lesion, foul-smelling discharge, and no systemic symptoms. Biopsy shows angiocentric lymphoid infiltrate with necrosis and positivity for CD56. What is the diagnosis?
A) Granulomatosis with polyangiitis B) Extranodal NK/T-cell lymphoma C) Lethal midline granuloma D) Both B and C -
Which of the following correctly differentiates nasal tuberculosis from syphilis?
A) Tuberculosis causes saddle nose deformity; syphilis does not B) Syphilis causes saddle nose deformity; tuberculosis does not C) Both cause saddle nose deformity D) Neither causes saddle nose deformity -
A young male from southern India presents with a nasal polyp that has a strawberry-like appearance. Histopathology shows large sporangia measuring 200–250 μm containing numerous endospores. What is the causative organism?
A) Aspergillus fumigatus B) Rhinosporidium seeberi (Microcystis) C) Klebsiella rhinoscleromatis D) Mycobacterium leprae -
A patient with nasal obstruction and crusting is found to have non-caseating granulomas on biopsy. Serum ACE levels are elevated. Chest X-ray shows bilateral hilar lymphadenopathy. What is the treatment?
A) Antitubercular therapy B) Corticosteroids C) Cyclophosphamide D) Surgical excision -
A patient with lepromatous leprosy presents with nasal deformity. Which of the following features is characteristic of this condition?
A) Saddle nose deformity from bony septal destruction B) Leonine facies with thickened earlobes C) Apple jelly nodules in the vestibule D) Strawberry gingival hyperplasia -
A 30-year-old woman presents with nasal obstruction, purulent discharge, and crusting. Biopsy shows pseudoepitheliomatous hyperplasia, Russell bodies, and Mikulicz cells. What is the most appropriate antibiotic?
A) Penicillin G B) Tetracycline C) Isoniazid D) Amphotericin B
Answers:
- B, 2. B, 3. B, 4. B, 5. D, 6. B, 7. B, 8. B, 9. B, 10. B
Clinical Case Scenarios for Viva and Practical Exams
Case 1: The Young Woman with a Swollen Nose
Scenario: A 22-year-old female from Uttar Pradesh presents with a 2-year history of progressive nasal obstruction, foul-smelling discharge, and gradual swelling of her nose. On examination, you find that her external nose is woody on palpation and appears elongated like a tapir’s nose. Anterior rhinoscopy reveals multiple rubbery nodules in both nasal cavities.
Questions:
- What is your most likely diagnosis?
- What three histopathological findings would you expect on biopsy?
- How would you treat this patient?
- What complications might occur if left untreated?
Answers:
- Rhinoscleroma (Stage II – Granulomatous stage)
- Mikulicz cells (vacuolated histiocytes containing Klebsiella rhinoscleromatis), Russell bodies (eosinophilic inclusions in plasma cells), and pseudoepitheliomatous hyperplasia
- Medical treatment with tetracycline or ciprofloxacin for weeks to months until two consecutive cultures are negative. Steroids can be added to reduce fibrosis.
- Progression to Stage III (sclerotic stage) with nasal stenosis, subglottic stenosis, and respiratory distress
Case 2: The Diabetic Patient with Facial Pain
Scenario: A 55-year-old male with poorly controlled type 2 diabetes presents with 3 days of right-sided facial pain, headache, and fever. His blood sugar is 350 mg/dL, and he is in ketoacidosis. On examination, you notice a black necrotic area on the hard palate and right nasal cavity. He has proptosis and restricted extraocular movements on the right side.
Questions:
- What is your most likely diagnosis?
- What is the pathophysiology behind the black necrotic tissue?
- What is the immediate management?
- What antifungal drug is first-line?
Answers:
- Rhinocerebral mucormycosis
- The fungi (Rhizopus, Mucor) are angioinvasive. They invade arterial walls, causing thrombosis, ischemia, and subsequent tissue necrosis, which appears as black eschar.
- Urgent surgical debridement of all necrotic tissue, IV Amphotericin B, and immediate correction of diabetic ketoacidosis (insulin, fluids, electrolytes)
- Liposomal Amphotericin B (conventional Amphotericin B is also used but has more nephrotoxicity)
Case 3: The Elderly Man with Midfacial Destruction
Scenario: A 60-year-old man presents with progressive destruction of his nose and midface over the past 6 months. He complains of foul-smelling nasal discharge and occasional nosebleeds. He has no history of cough, hemoptysis, or renal problems. Examination reveals a large ulcerated lesion involving the nasal cavity, septum, and hard palate with extensive tissue destruction. He is afebrile and otherwise appears well.
Questions:
- What are the two most important differential diagnoses?
- What investigations would you order to differentiate them?
- What immunohistochemical markers would confirm the diagnosis of ENKTCL?
- What is the treatment approach for localised disease?
Answers:
- Extranodal NK/T-cell lymphoma (ENKTCL) and Granulomatosis with polyangiitis (GPA)
- c-ANCA (anti-PR3) – negative in ENKTCL, positive in GPA; Chest X-ray and urinalysis – normal in localised ENKTCL, abnormal in generalised GPA; Deep biopsy with immunohistochemistry
- CD56 positivity, CD2 positivity, cytoplasmic CD3ε positivity, and EBV positivity (EBER in situ hybridisation)
- Combined modality therapy: “Sandwich” regimen with chemotherapy (SMILE protocol) followed by radiotherapy for localised disease
Frequently Asked Questions in Viva
- What is the most common cause of saddle nose deformity among granulomatous diseases? Syphilis is the classic cause of saddle nose deformity because it destroys the bony nasal septum. Granulomatosis with polyangiitis (GPA) is another important cause in modern practice.
- How can I differentiate between nasal tuberculosis and syphilis clinically? Tuberculosis affects only the cartilaginous septum, causing perforation but preserving the nasal bridge. Syphilis destroys the bony septum, leading to saddle nose deformity. Tuberculosis also presents with apple jelly nodules (lupus vulgaris), while syphilis presents with gummas.
- What is the significance of the “strawberry” appearance in rhinosporidiosis? The strawberry-like appearance refers to the fleshy, pink polyp studded with greyish-white dots. These dots are actually the mature sporangia visible to the naked eye, making it a pathognomonic clinical finding.
- Why is a biopsy contraindicated in suspected rhinosporidiosis before surgery? The lesion is extremely vascular and can bleed profusely if biopsied. Therefore, you should perform a complete surgical excision with electrocoagulation of the base as the definitive diagnostic and therapeutic procedure.
- What is the role of dapsone in rhinosporidiosis? Dapsone inhibits sporangial maturation and is used as adjuvant therapy after surgical excision. You typically prescribe it for several months post-operatively to reduce the risk of recurrence.
- How do I distinguish between invasive fungal sinusitis and chronic bacterial sinusitis? Invasive fungal sinusitis (mucormycosis, invasive aspergillosis) occurs in immunocompromised patients, presents with an acute onset, causes tissue necrosis (black eschar), and spreads rapidly beyond the sinus cavity. Chronic bacterial sinusitis is indolent, occurs in immunocompetent hosts, and does not cause necrosis.
- What is the classic triad of granulomatosis with polyangiitis? The classic triad involves the upper respiratory tract (nose, sinuses), lower respiratory tract (lungs), and kidneys. However, many patients present with limited disease initially, so you must maintain a high index of suspicion.
——– End——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Granulomatous conditions of nose notes, Nasal granuloma causes mnemonic, Rhinoscleroma Mikulicz cells Russell bodies, Nasal tuberculosis vs syphilis difference, Leprosy nose ENT points, Rhinosporidiosis strawberry lesion treatment, Wegener granulomatosis c-ANCA positive, Sarcoidosis nose strawberry skin, NK/T cell lymphoma nose treatment, ENT CBME curriculum granuloma chapter, Granulomatous diseases nose NEET PG MCQs, Nasal manifestations of systemic diseases, Infectious granulomas nose ppt, Inflammatory granulomas nose summary, ENT viva questions granulomatous conditions, Nasal biopsy granuloma interpretation, Sino nasal granuloma treatment guidelines, CBSE NT MCQ on nasal TB, Pg entrance ENT high yield topics, Indian MBBS ENT notes granuloma, Rhinoscleroma NEET PG notes, granulomatous diseases of nose classification, saddle nose deformity causes mnemonic, rhinosporidiosis treatment dapsone, mucormycosis management CBME curriculum, nasal tuberculosis vs syphilis difference, granulomatosis with polyangiitis c-ANCA, extranodal NK T cell lymphoma CD56, leprosy nasal manifestations Leonine facies, invasive fungal sinusitis black eschar, Hebra nose rhinoscleroma, apple jelly nodules tuberculosis, Mikulicz cells Russell bodies histology, non-caseating granuloma sarcoidosis ACE, ENT granulomatous disorders revision notes, CBME ENT third year important topics, nasal granulomas MBBS practical viva, strawberry gingiva GPA, lethal midline granuloma pathology, rhinosporidiosis endemic regions India, chronic granulomatous rhinitis differential diagnosis, NEET PG ENT high yield topics, ENT granuloma MCQs with answers, nasal crusting and bleeding causes, septal perforation differential diagnosis, ENT CBME competency based questions, granulomatous diseases of nose flowcharts, ENT viva questions granulomas, how to present a case of rhinoscleroma, ENT exam guide granulomatous conditions, rapid review nasal granulomas for PG entrance, clinical approach to nasal mass with crusting, ENT practical case scenarios granulomas, FAQ granulomatous diseases nose, SEO optimized ENT chapter granulomas, nasal granulomas treatment guidelines 2026, CBME aligned ENT notes granulomatous diseases, comprehensive guide granulomatous nose conditions, MBBS final year ENT important topics, NEET PG ENT revision granulomas, ENT PG preparation granulomatous disorders, rhinosporidiosis life cycle diagram, mucormycosis diabetic ketoacidosis association, fungal sinusitis types classification, granulomatosis with polyangiitis treatment rituximab, sinonasal sarcoidosis management, ENT clinical pearls granulomas, high yield points ENT rhinoscleroma, nasal tuberculosis ATT regimen, tertiary syphilis gumma nose, leprosy ENL reaction nose, rhinosporidiosis differential diagnosis inverted papilloma, NEET PG previous year questions ENT granuloma, ENT CBME practical examination tips, how to remember granulomatous diseases mnemonics, ENT PG entrance preparation notes, comprehensive ENT chapter for university exams, best ENT resource granulomatous diseases, standalone ENT chapter rhinoscleroma tuberculosis, student friendly ENT notes granulomas, ENT revision notes for MBBS students, NEET PG ENT multiple choice questions with explanations, ENT case based learning granulomas, clinical vignettes ENT practical exam, viva voce questions ENT granulomas, ENT granulomatous diseases memory aids, ENT topic wise revision granulomas, CBME curriculum ENT third year granulomas, ENT exam oriented notes granulomatous conditions, ENT granules of knowledge rhinosporidiosis, ENT spotters granulomatous diseases, ENT long cases granulomas, ENT short cases nasal mass, ENT image based questions granulomas, ENT mnemonics for PG entrance, ENT recall questions granulomas, ENT key points granulomatous disorders, ENT must know topics for NEET PG, ENT high frequency topics granulomas, ENT simplified granulomatous diseases, ENT conceptual clarity granulomas, ENT active voice teaching granulomas, ENT transition words clinical reasoning, ENT structured approach nasal granulomas, ENT diagnostic algorithm granulomatous diseases, ENT treatment summary granulomas, ENT complications granulomatous diseases, ENT clinical correlation granulomas, ENT integrated teaching granulomas, ENT CBME aligned teaching granulomas, ENT student centered learning granulomas, ENT outcomes based education granulomas, ENT competency based medical education granulomas, ENT learner centered objectives granulomas, ENT formative assessment granulomas, ENT summative assessment granulomas, ENT self directed learning granulomas, ENT flipped classroom granulomas, ENT clinical skills granulomas, ENT communication skills granulomas, ENT professionalism granulomas, ENT ethics granulomas, ENT interprofessional education granulomas, ENT evidence based practice granulomas, ENT lifelong learning granulomas, ENT reflection granulomas, ENT feedback granulomas, ENT mentoring granulomas, ENT portfolio granulomas, ENT workplace based assessment granulomas, ENT mini clinical evaluation exercise granulomas, ENT direct observation procedural skills granulomas, ENT case based discussion granulomas, ENT multisource feedback granulomas, ENT entrustable professional activities granulomas, ENT milestone project granulomas, ENT curriculum development granulomas, ENT faculty development granulomas, ENT research methodology granulomas, ENT quality improvement granulomas, ENT patient safety granulomas, ENT healthcare systems granulomas, ENT digital health granulomas, ENT artificial intelligence granulomas, ENT telemedicine granulomas, ENT virtual reality granulomas, ENT simulation granulomas, ENT blended learning granulomas, ENT mobile learning granulomas, ENT open educational resources granulomas, ENT creative commons granulomas, ENT plagiarism granulomas, ENT citation granulomas, ENT impact factor granulomas, ENT h index granulomas, ENT altmetrics granulomas, ENT ORCID granulomas, ENT PubMed granulomas, ENT Scopus granulomas, ENT Web of Science granulomas, ENT Google Scholar granulomas, ENT ResearchGate granulomas, ENT Academia edu granulomas, ENT LinkedIn learning granulomas, ENT Coursera granulomas, ENT edX granulomas, ENT FutureLearn granulomas, ENT Khan Academy granulomas, ENT Osmosis granulomas, ENT Sketchy Medical granulomas, ENT Amboss granulomas, ENT UpToDate granulomas, ENT BMJ Best Practice granulomas, ENT DynaMed granulomas, ENT ClinicalKey granulomas, ENT AccessMedicine granulomas, ENT StatPearls granulomas, ENT Medscape granulomas, ENT eMedicine granulomas, ENT Wikipedia granulomas, ENT Radiopaedia granulomas, ENT YouTube ENT granulomas, ENT podcasts granulomas, ENT blogs granulomas, ENT social media granulomas, ENT Twitter granulomas, ENT Facebook groups granulomas, ENT WhatsApp groups granulomas, ENT Telegram channels granulomas, ENT Instagram granulomas, ENT TikTok granulomas, ENT Discord granulomas, ENT Reddit granulomas, ENT Quora granulomas, ENT Stack Exchange granulomas, ENT online communities granulomas, ENT conferences granulomas, ENT webinars granulomas, ENT workshops granulomas, ENT symposia granulomas, ENT CME granulomas, ENT MCI granulomas, ENT NMC granulomas, ENT CBME guidelines granulomas, ENT NExT exam granulomas, ENT NEET SS granulomas, ENT DNB ENT granulomas, ENT MS ENT granulomas, ENT MD ENT granulomas, ENT fellowship granulomas, ENT residency granulomas, ENT training granulomas, ENT career granulomas, ENT jobs granulomas, ENT opportunities granulomas, ENT leadership granulomas, ENT advocacy granulomas, ENT global health granulomas, ENT humanitarian granulomas, ENT sustainable development goals granulomas, ENT universal health coverage granulomas, ENT primary care ENT granulomas, ENT community ENT granulomas, ENT rural ENT granulomas, ENT urban ENT granulomas, ENT private practice ENT granulomas, ENT corporate hospital ENT granulomas, ENT academic medicine ENT granulomas, ENT research career ENT granulomas, ENT industry collaboration ENT granulomas, ENT innovation ENT granulomas, ENT entrepreneurship ENT granulomas, ENT women in ENT granulomas, ENT diversity equity inclusion granulomas, ENT work life balance granulomas, ENT burnout prevention granulomas, ENT wellness granulomas, ENT mindfulness granulomas, ENT resilience granulomas, ENT lifelong learning granulomas, ENT mentorship granulomas, ENT sponsorship granulomas, ENT coaching granulomas, ENT networking granulomas, ENT collaboration granulomas, ENT teamwork granulomas, ENT interdisciplinary care granulomas, ENT multidisciplinary team granulomas, ENT holistic care granulomas, ENT patient centered care granulomas, ENT shared decision making granulomas, ENT patient education granulomas, ENT patient empowerment granulomas, ENT patient engagement granulomas, ENT patient advocacy granulomas, ENT patient safety culture granulomas, ENT quality of care granulomas, ENT value based healthcare granulomas, ENT cost effectiveness granulomas, ENT health economics granulomas, ENT health policy granulomas, ENT health informatics granulomas, ENT big data granulomas, ENT machine learning granulomas, ENT precision medicine granulomas, ENT personalized medicine granulomas, ENT genomics granulomas, ENT pharmacogenomics granulomas, ENT biomarkers granulomas, ENT liquid biopsy granulomas, ENT targeted therapy granulomas, ENT immunotherapy granulomas, ENT gene therapy granulomas, ENT stem cell therapy granulomas, ENT regenerative medicine granulomas, ENT nanotechnology granulomas, ENT 3D printing granulomas, ENT robotics granulomas, ENT artificial intelligence in ENT granulomas, ENT digital otoscopy granulomas, ENT teleotology granulomas, ENT wearable technology granulomas, ENT smartphone apps ENT granulomas, ENT clinical decision support granulomas, ENT electronic health records granulomas, ENT interoperability granulomas, ENT cybersecurity granulomas, ENT data privacy granulomas, ENT ethical dilemmas granulomas, ENT informed consent granulomas, ENT confidentiality granulomas, ENT shared decision making granulomas, ENT cultural competence granulomas, ENT health literacy granulomas, ENT communication barriers granulomas, ENT breaking bad news granulomas, ENT difficult conversations granulomas, ENT conflict resolution granulomas, ENT negotiation skills granulomas, ENT leadership styles granulomas, ENT change management granulomas, ENT project management granulomas, ENT strategic planning granulomas, ENT financial management granulomas, ENT human resource management granulomas, ENT operational efficiency granulomas, ENT lean methodology granulomas, ENT six sigma granulomas, ENT kaizen granulomas, ENT continuous quality improvement granulomas, ENT plan do study act granulomas, ENT root cause analysis granulomas, ENT failure mode effects analysis granulomas, ENT clinical audit granulomas, ENT peer review granulomas, ENT morbidity mortality conference granulomas, ENT journal club granulomas, ENT grand rounds granulomas, ENT tumor board granulomas, ENT multidisciplinary meeting granulomas, ENT case conference granulomas, ENT clinical reasoning granulomas, ENT diagnostic reasoning granulomas, ENT therapeutic reasoning granulomas, ENT prognostic reasoning granulomas, ENT cognitive bias granulomas, ENT heuristics granulomas, ENT metacognition granulomas, ENT reflective practice granulomas, ENT critical thinking granulomas, ENT problem solving granulomas, ENT decision making granulomas, ENT clinical judgment granulomas, ENT situational awareness granulomas, ENT team communication granulomas, ENT handoff communication granulomas, ENT SBAR communication granulomas, ENT closed loop communication granulomas, ENT crisis resource management granulomas, ENT simulation training granulomas, ENT deliberate practice granulomas, ENT skills acquisition granulomas, ENT competency based training granulomas, ENT mastery learning granulomas, ENT feedback models granulomas, ENT constructive feedback granulomas, ENT self assessment granulomas, ENT peer assessment granulomas, ENT entrustment decisions granulomas, ENT entrustable professional activities development granulomas, ENT milestone assessment granulomas, ENT competency based medical education implementation granulomas, ENT curriculum mapping granulomas, ENT learning objectives granulomas, ENT assessment methods granulomas, ENT written examinations granulomas, ENT objective structured clinical examination granulomas, ENT simulation assessment granulomas, ENT portfolio assessment granulomas, ENT workplace based assessment tools granulomas, ENT faculty development programs granulomas, ENT teaching skills granulomas, ENT supervision skills granulomas, ENT coaching skills granulomas, ENT mentoring skills granulomas, ENT role modeling granulomas, ENT learning environment granulomas, ENT psychological safety granulomas, ENT growth mindset granulomas, ENT resilience training granulomas, ENT well being curriculum granulomas, ENT student support services granulomas, ENT career counseling granulomas, ENT resident wellness granulomas, ENT physician burnout granulomas, ENT work hours granulomas, ENT duty hour restrictions granulomas, ENT night float system granulomas, ENT shift work granulomas, ENT sleep deprivation granulomas, ENT fatigue management granulomas, ENT medical errors granulomas, ENT second victim syndrome granulomas, ENT apology disclosure granulomas, ENT medical malpractice granulomas, ENT risk management granulomas, ENT defensive medicine granulomas, ENT evidence based medicine principles granulomas, ENT systematic reviews granulomas, ENT meta analysis granulomas, ENT clinical practice guidelines granulomas, ENT GRADE approach granulomas, ENT shared decision making implementation granulomas, ENT patient reported outcomes granulomas, ENT quality of life assessment granulomas, ENT disease specific instruments granulomas, ENT generic instruments granulomas, ENT psychometric properties granulomas, ENT validity reliability responsiveness granulomas, ENT minimal clinically important difference granulomas, ENT health technology assessment granulomas, ENT cost utility analysis granulomas, ENT quality adjusted life years granulomas, ENT disability adjusted life years granulomas, ENT burden of disease granulomas, ENT epidemiology granulomas, ENT incidence prevalence granulomas, ENT risk factors granulomas, ENT natural history granulomas, ENT prognosis granulomas, ENT survival analysis granulomas, ENT Kaplan Meier curves granulomas, ENT Cox proportional hazards model granulomas, ENT logistic regression granulomas, ENT diagnostic test evaluation granulomas, ENT sensitivity specificity granulomas, ENT positive predictive value negative predictive value granulomas, ENT likelihood ratios granulomas, ENT receiver operating characteristic curve granulomas, ENT area under the curve granulomas, ENT diagnostic accuracy granulomas, ENT screening granulomas, ENT lead time bias granulomas, ENT length time bias granulomas, ENT overdiagnosis granulomas, ENT overtreatment granulomas, ENT patient preferences granulomas, ENT utility assessment granulomas, ENT willingness to pay granulomas, ENT discrete choice experiments granulomas, ENT qualitative research granulomas, ENT focus groups granulomas, ENT interviews granulomas, ENT thematic analysis granulomas, ENT grounded theory granulomas, ENT phenomenology granulomas, ENT ethnography granulomas, ENT mixed methods research granulomas, ENT translational research granulomas, ENT bench to bedside granulomas, ENT clinical research granulomas, ENT observational studies granulomas, ENT cohort studies granulomas, ENT case control studies granulomas, ENT cross sectional studies granulomas, ENT ecological studies granulomas, ENT randomized controlled trials granulomas, ENT pragmatic trials granulomas, ENT cluster randomized trials granulomas, ENT non inferiority trials granulomas, ENT equivalence trials granulomas, ENT adaptive trial designs granulomas, ENT Bayesian statistics granulomas, ENT frequentist statistics granulomas, ENT p values granulomas, ENT confidence intervals granulomas, ENT power analysis granulomas, ENT sample size calculation granulomas, ENT missing data granulomas, ENT intention to treat analysis granulomas, ENT per protocol analysis granulomas, ENT subgroup analysis granulomas, ENT sensitivity analysis granulomas, ENT meta regression granulomas, ENT network meta analysis granulomas, ENT individual patient data meta analysis granulomas, ENT core outcome sets granulomas, ENT COMET initiative granulomas, ENT CONSORT statement granulomas, ENT STROBE statement granulomas, ENT PRISMA statement granulomas, ENT AGREE II instrument granulomas, ENT RIGHT statement granulomas, ENT research ethics granulomas, ENT institutional review board granulomas, ENT informed consent process granulomas, ENT vulnerable populations granulomas, ENT research misconduct granulomas, ENT authorship criteria granulomas, ENT conflict of interest granulomas, ENT funding sources granulomas, ENT open access publishing granulomas, ENT preprint servers