|
The following CBME core competencies are covered in this chapter.
|
Anatomy of Paranasal Sinuses
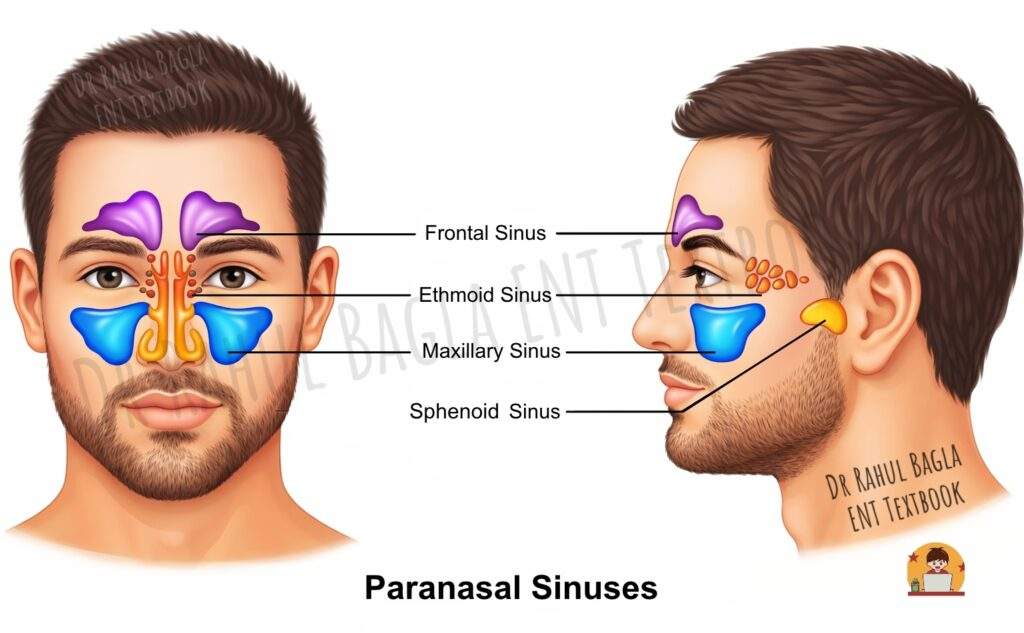
The paranasal sinuses are a group of air-filled cavities within the bones of the skull. They are named after the bones in which they reside: the maxillary, frontal, sphenoid, and ethmoid sinuses. Therefore, there are four on each side, making eight in total. These sinuses develop as outgrowths from the nasal cavity, which is why their mucosal lining is a direct continuation of the nasal mucosa. Consequently, infections can easily spread from the nose (rhinitis) to the sinuses (sinusitis). The function of the sinuses is to make the skull lighter and add resonance to the voice.
Clinical Grouping
Clinically, the paranasal sinuses are divided into two functional groups based on the location of their drainage pathways. This classification centres around the basal lamella. The basal lamella is a bony partition of the middle turbinate that serves as the anatomical dividing line between the anterior and posterior sinus groups.
- Anterior Group: This group includes the maxillary sinus, the frontal sinus, and the anterior ethmoidal cells. They all drain into the middle meatus of the nasal cavity. Their ostia (openings) are located anterior to the basal lamella. When infection affects this group, patients typically present with anterior sinusitis characterised by facial pain over the cheeks, forehead, and periorbital region. Because these sinuses share a common drainage pathway, they often become involved together in inflammatory processes.
- Posterior Group: This group includes the posterior ethmoidal cells and the sphenoid sinus. The posterior ethmoidal cells drain into the superior meatus, while the sphenoid sinus drains into the sphenoethmoidal recess, a small triangular space located posterosuperior to the superior turbinate. Their ostia lie posterior to the basal lamella. Their ostia lie posterior to the basal lamella, and infections in this group often present as posterior sinusitis with symptoms that can be more challenging to diagnose and treat. The proximity of these sinuses to vital structures such as the optic nerve, internal carotid artery, and cavernous sinus makes posterior sinusitis potentially more dangerous.
Maxillary Sinus (Sinus of Highmore)
The maxillary sinus is the largest of the paranasal sinuses and the first to develop. It occupies the body of the maxilla and is pyramidal in shape.
Anatomy and Dimensions of Maxillary Sinus: It is a pyramidal cavity with its base forming the lateral wall of the nasal cavity and its apex extending into the zygomatic process of the maxilla. In an adult, it has an average capacity of 15 ml. Its dimensions are 33 mm in height, 35 mm in depth, and 25 mm in width.
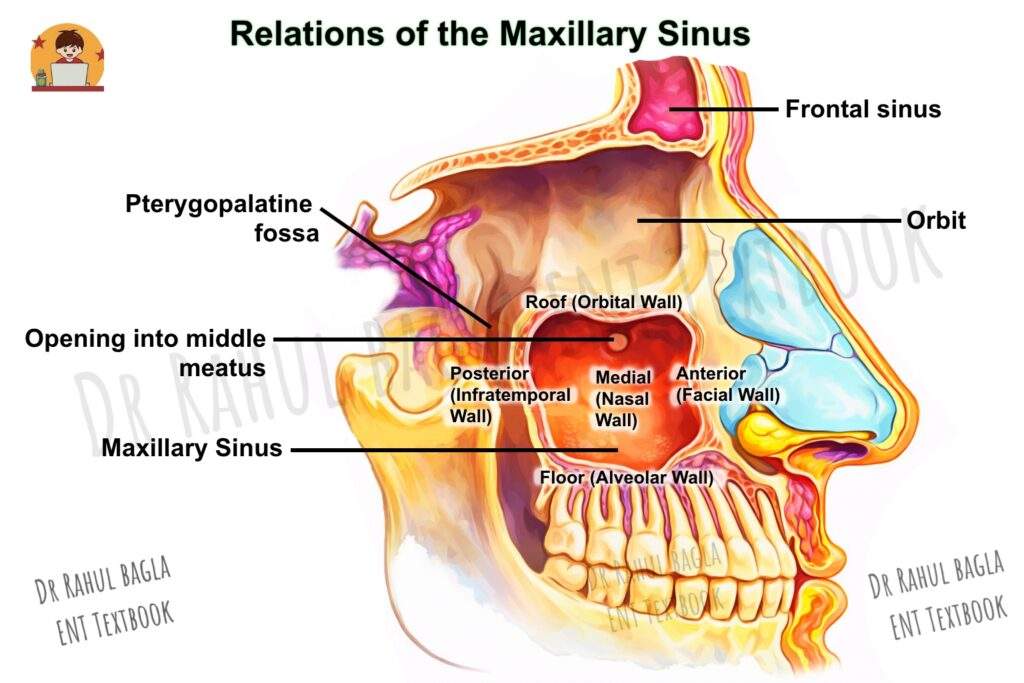
Relations (The Walls of the Pyramid):
- Roof (Orbital Wall): This is the floor of the orbit. It is traversed by the infraorbital nerve and vessels in a bony canal. A dehiscent (thin or absent) bony canal can make the nerve vulnerable to surgical injury.
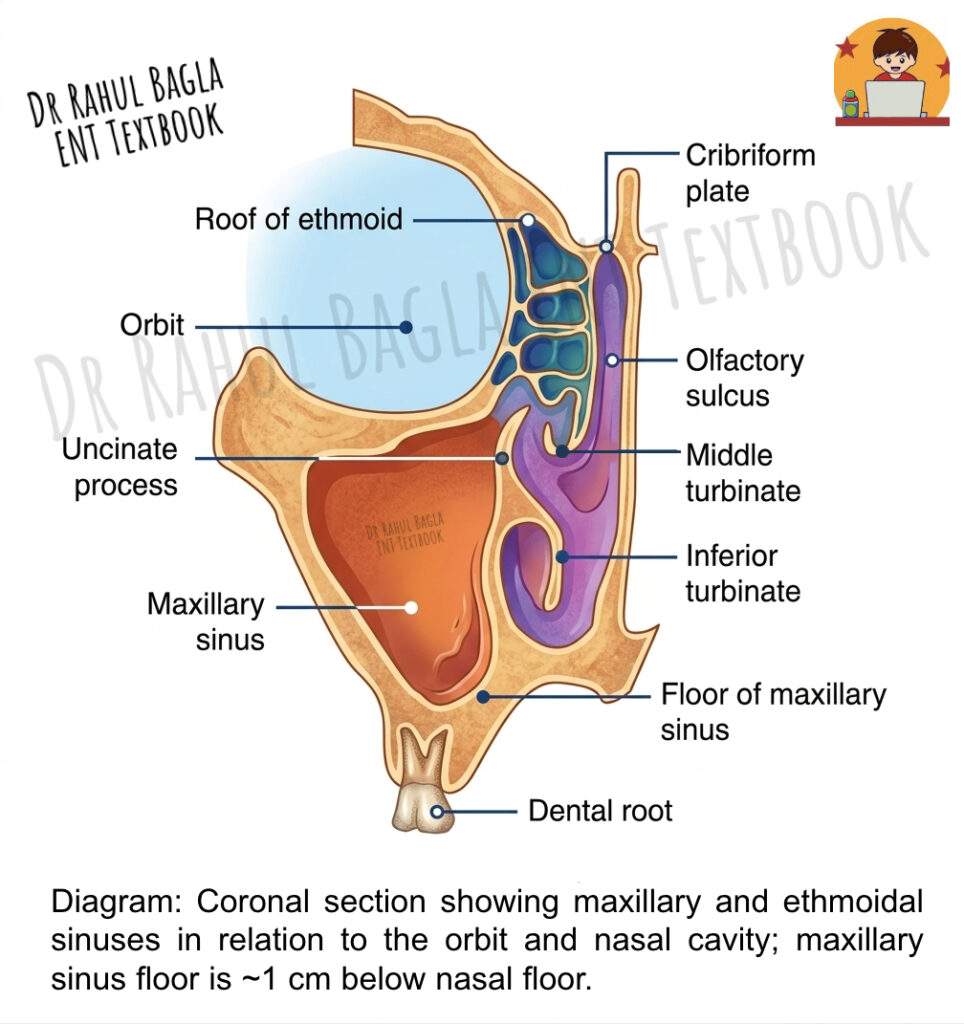
- Floor (Alveolar Wall): This is formed by the alveolar process of the maxilla and is the most clinically significant wall. Importantly, the floor is situated about 1 cm below the level of the floor of the nasal cavity and corresponds to the level of the lower border of the ala of the nose. It is intimately related to the roots of the second premolar and first molar teeth, often separated only by a thin layer of bone or even just by the mucous membrane. Clinical Insight: This close relationship explains why dental infections are a common cause of maxillary sinusitis (odontogenic sinusitis). Furthermore, an oroantral fistula (an abnormal communication between the mouth and the sinus) can occur during tooth extraction.
- Anterior Wall (Facial Wall): This is formed by the facial surface of the maxilla and is related to the soft tissues of the cheek.
- Posterior Wall (Infratemporal Wall): This wall separates the sinus from the infratemporal fossa and pterygopalatine fossa, which house important neurovascular structures, including the maxillary artery, pterygoid plexus of veins, and branches of the trigeminal nerve. Infection or tumour extending through this wall can therefore involve these vital structures.
- Medial Wall (Nasal Wall): This is the base of the pyramid and is the only wall that is not completely bone; it has membranous parts called the anterior and posterior fontanelles. It is related to the middle and inferior meatuses.
- Lateral Wall (Zygomatic Wall): This is the apex of the pyramid, and it extends into the zygomatic process of the maxilla.
Drainage and Neurovascular Supply of the Maxillary Sinus
- Ostium (Opening): The natural ostium for drainage is located high up on the medial wall, opening into the ethmoidal infundibulum in the middle meatus. Because it is situated high, gravity does not assist drainage, making this sinus particularly prone to infection. An accessory ostium is present behind the main ostium in approximately 30% of cases.
- Arterial Supply: It receives blood from the maxillary artery (via its infraorbital, posterior superior alveolar, and greater palatine branches) and the facial artery.
- Venous Drainage: The blood is drained by the maxillary vein.
- Nerve Supply: Sensory innervation is provided by branches of the maxillary nerve (CN V2), specifically the infraorbital, anterior superior alveolar, and middle superior alveolar nerves.
- Lymphatic drainage into the submandibular nodes.
Ethmoid Sinus (Ethmoidal Air Cells)
The ethmoid sinus is not a single cavity but a complex labyrinth of multiple air cells located between the nasal cavity and the orbit. These thin-walled air cells are located within the lateral masses (labyrinths) of the ethmoid bone. Their number varies from 3 to 18 on each side. They occupy the space between the upper third of the lateral nasal wall and the medial wall of the orbit. Clinically, ethmoidal cells are divided by the basal lamina into an anterior ethmoid group, which opens into the middle meatus and a posterior ethmoid group, which opens into the superior meatus and into the supreme meatus, if that be present.
Relations:
- Roof: The roof of the ethmoid sinus is formed by the fovea ethmoidalis, which represents a medial extension of the orbital plate of the frontal bone. This thin bony plate separates the ethmoidal cells from the anterior cranial fossa, and its integrity is crucial for preventing intracranial complications of sinusitis. The fovea ethmoidalis is a critical landmark during endoscopic sinus surgery because the skull base lies immediately above it.
- Lateral Wall: This wall consists of the thin lamina papyracea (orbital plate of the ethmoid), which separates the ethmoidal air cells from the orbit. The lamina papyracea is paper-thin and can be easily breached by infection, leading to orbital cellulitis, subperiosteal abscess, or even cavernous sinus thrombosis. During endoscopic surgery, great care must be taken to avoid violating this delicate barrier.
- Medial Wall: Formed by the lateral wall of the nasal cavity (the middle and superior turbinates).
Clinical Grouping (by Basal Lamella):
Anterior Ethmoidal Cells (Open into the Middle Meatus): These lie anterior to the basal lamella of the middle turbinate. They are the most clinically important group for endoscopic sinus surgery.
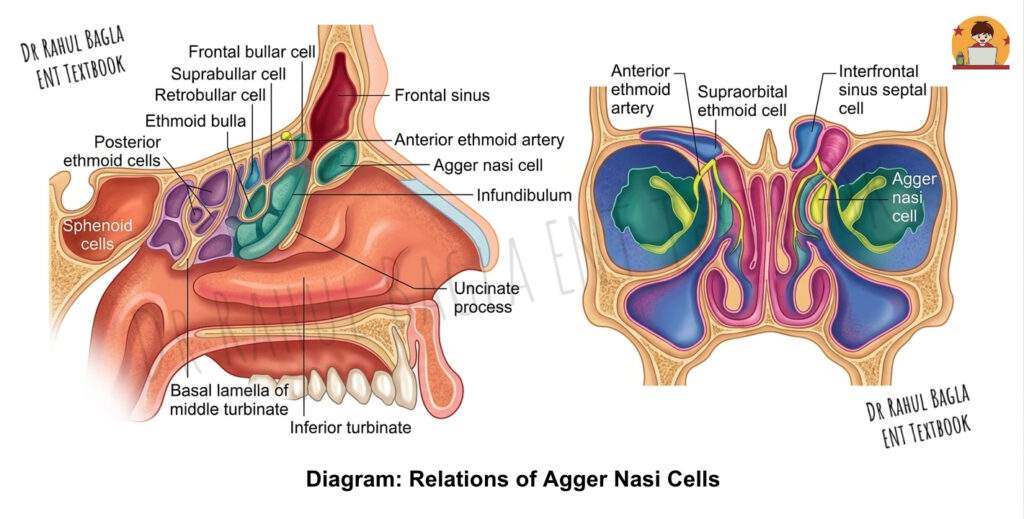
- Agger Nasi Cells: These represent the most anterior ethmoidal cells, located in the agger nasi ridge just anterior and superior to the insertion of the middle turbinate. These cells are surgically important because they define the anterior limit of the frontal recess, and failure to open them adequately can lead to persistent frontal sinus disease.
- Ethmoid Bulla: This is the largest and most constant anterior ethmoidal cell, forming the posterior boundary of the hiatus semilunaris—a key drainage channel in the middle meatus.
- Haller Cells: These are ethmoidal cells that extend laterally along the floor of the orbit. When enlarged, Haller cells can constrict the infundibulum and mechanically obstruct the maxillary sinus ostium, predisposing the patient to maxillary sinusitis.
Posterior Ethmoidal Cells (Open into the Superior Meatus): These lie posterior to the basal lamella and open into the superior meatus.
- Onodi Cell: This represents a highly significant anatomical variation in which a posterior ethmoidal cell extends laterally and superiorly, wrapping around the sphenoid sinus and coming into direct contact with the optic nerve. During endoscopic surgery, an Onodi cell can be mistaken for the sphenoid sinus, putting the optic nerve at risk of injury. Surgeons must therefore identify this variation on preoperative imaging to avoid catastrophic complications.
Neurovascular Supply of Ethmoid Sinus
- Arterial Supply: The anterior and posterior ethmoidal arteries (branches of the ophthalmic artery) supply the sinus.
- Venous Drainage: It is drained by the ethmoidal veins and the maxillary vein.
- Nerve Supply: Sensory innervation is from the anterior and posterior ethmoidal nerves (branches of the ophthalmic nerve, CN V1).
Frontal Sinus
The frontal sinus is situated within the frontal bone, and its development begins after birth.
Anatomy and Variations: It lies between the inner and outer tables of the frontal bone, above and deep to the supraorbital margin. It is not present at birth and begins to develop after birth, gradually increasing in size until it reaches full development after puberty. It is usually larger in males than in females. A bony septum separates the two sinuses, but they are often asymmetrical, and one may be absent.
The average dimensions of the frontal sinus are approximately 32 mm in height, 24 mm in width, and 16 mm in depth, with a volume of 4-7 mL. Functionally and developmentally, the frontal sinus is considered an anterior ethmoidal air cell that expands into the frontal bone postnatally.
Relations:
- The Anterior Wall: This thick outer table of the frontal bone relates to the skin of the forehead and provides protection against frontal trauma. Fractures of this wall may produce cosmetic deformity and require surgical repair.
- The Posterior Wall: This thin inner table separates the sinus from the meninges and the frontal lobe of the brain. This relationship is critically important because infection can spread through this wall to cause a frontal lobe abscess or meningitis. The posterior wall forms part of the anterior cranial fossa floor.
- The Inferior Wall (Orbital Roof): This thin bony plate forms the roof of the orbit and separates the frontal sinus from orbital contents. Infection or trauma breaching this wall can lead to orbital complications, including subperiosteal abscess or orbital cellulitis.

Drainage Pathway of Frontal Sinus: The frontal sinus drains through an opening called the ostium, located in the posteromedial part of its floor. The drainage pathway follows a characteristic pattern: from the sinus, secretions pass through the frontal ostium into the frontal recess, which then opens into the middle meatus of the nasal cavity, usually through the infundibulum. This pathway has an hourglass shape, with the frontal ostium being the narrowest part, making it prone to obstruction.
It is important to note that there is no true “nasofrontal duct”—this term is a misnomer. Instead, the drainage pathway is a complex three-dimensional space called the frontal recess. The frontal recess is often encroached upon by anterior ethmoidal cells, which can narrow it and obstruct frontal sinus drainage, leading to chronic frontal sinusitis.
The Frontal Recess: This is a critical anatomical region in the anterior part of the middle meatus. Its boundaries are:
- Medially: Middle turbinate
- Laterally: Lamina papyracea
- Anteriorly: Agger nasi cells
- Posteriorly: Ethmoid bulla
Clinical Insight: The frontal recess is often encroached upon by anterior ethmoidal cells, which can narrow it and obstruct the drainage of the frontal sinus, leading to frontal sinusitis.
Neurovascular Supply of Frontal Sinus
- Arterial Supply: The supratrochlear and supraorbital arteries (branches of the ophthalmic artery).
- Venous Drainage: The supraorbital and ophthalmic veins.
- Nerve Supply: The supratrochlear and supraorbital nerves (branches of CN V1).
- Lymphatic drainage: To the submandibular nodes.
Sphenoid Sinus
The sphenoid sinus is a paired air sinus located within the body of the sphenoid bone. It is the most posterior of all paranasal sinuses, lying deep in the skull base. A thin, often asymmetrical bony septum separates the two sinuses; this septum may even be partially deficient in some individuals.
Pneumatization of Sphenoid Sinus. The extent to which the sphenoid sinus is filled with air—known as pneumatization—varies greatly among individuals and is classified into three types:
- Conchal type: There is little or no pneumatization; only a small, shallow cavity exists within the sphenoid bone.
- Pre‑sellar type: Pneumatization extends forward to the anterior wall of the sella turcica but does not reach beneath it
- Sellar type: Pneumatization is extensive and extends below the sella turcica. In some cases, air cells further extend into adjacent structures such as the anterior clinoid processes, pterygoid processes, and even the vidian canal. This extensive pneumatization creates a lateral recess when it crosses the line connecting the vidian canal and foramen rotundum (the V–R line).
Drainage Pathway of Sphenoid Sinus: The sphenoid sinus drains through its ostium, which is located high on the anterior wall. The ostium opens into the sphenoethmoidal recess, which lies medial to the superior turbinate. The opening may be slit-like, oval, or round and can be visualized during nasal endoscopy. In adults, the ostium is situated approximately 1.5 cm above the upper border of the posterior choana and about 7 cm posterior to the anterior nasal spine.
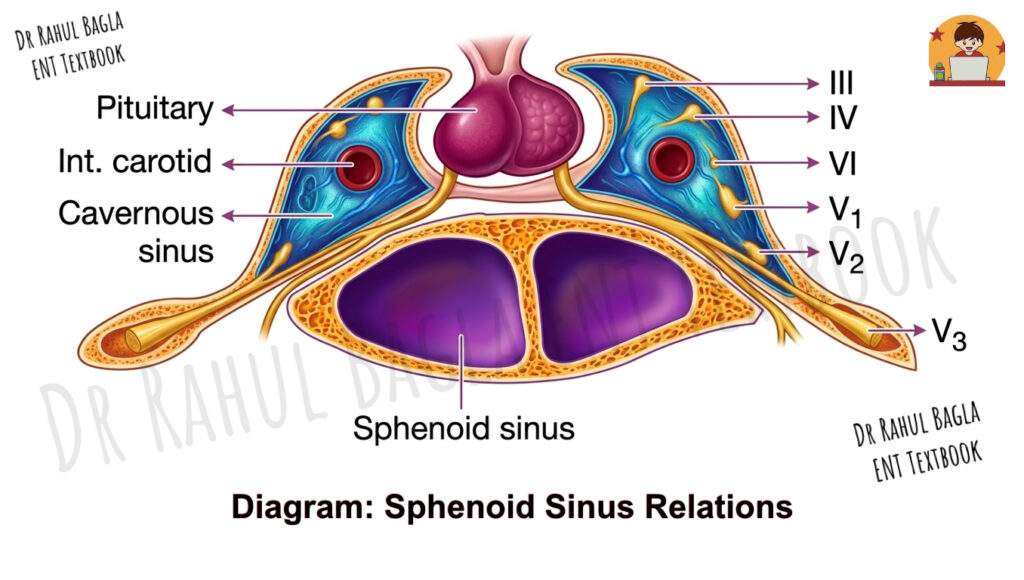
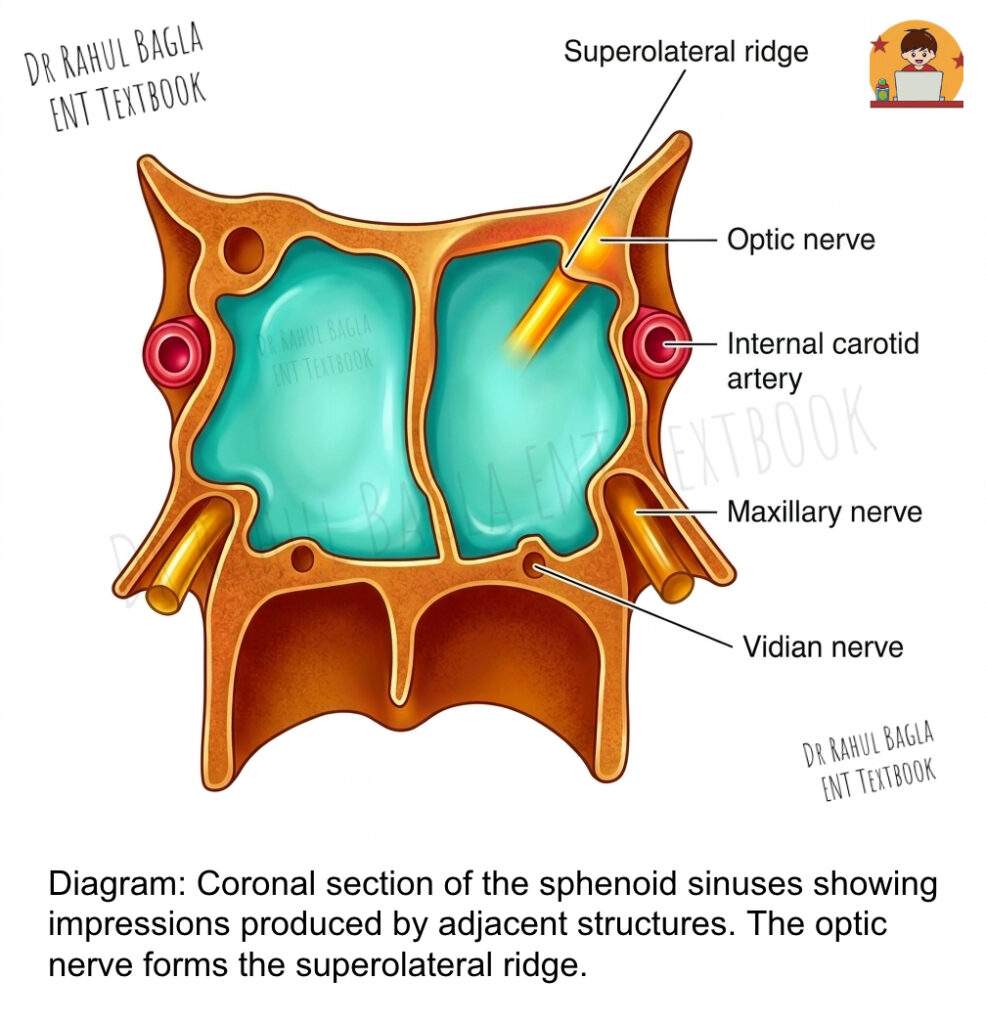
Relations:
The sphenoid sinus is intimately related to several vital neurovascular structures, often separated only by a thin bony wall that may be dehiscent (absent). These relations are crucial for surgical planning.
Lateral wall – This is the most clinically significant area.
- The optic nerve runs along the superolateral wall and may be exposed in some individuals.
- The internal carotid artery courses along the inferolateral wall; in a significant percentage of cases, the bony covering is missing.
- The maxillary nerve(V2) lies along the lower part of the lateral wall.
Roof – The roof has both anterior and posterior parts.
- Anteriorly, it relates to the olfactory tract, frontal lobe, and optic chiasma.
- Posteriorly, it forms the sella turcica, which houses the pituitary gland; laterally, it is adjacent to the cavernous sinus.
Posterior wall – This contributes to the formation of the clivus.
Floor – The floor is related to the vidian nerve as it travels through the pterygoid canal.
Lateral recess – When pneumatization is excessive (sellar type), a lateral recess develops beyond the V–R line, bringing the sinus into close contact with the foramen rotundum and vidian canal.
Neurovascular Supply of Sphenoid Sinus
- Arterial supply: The sphenopalatine artery, a terminal branch of the maxillary artery, provides the main blood supply.
- Venous drainage: Venous blood drains via the maxillary vein.
- Nerve supply: Sensory innervation comes from the posterior ethmoidal branch of the ophthalmic nerve (V1) and from the maxillary nerve (V2) through orbital branches originating from the pterygopalatine ganglion.
- Lymphatic drainage: Lymph from the sphenoid sinus drains to the retropharyngeal nodes.
Mucous Membrane and Development
The Mucociliary Apparatus
The paranasal sinuses are lined by a ciliated pseudostratified columnar epithelium with goblet cells, forming a respiratory mucosa that is continuous with the nasal mucosa. However, this sinus mucosa is thinner and less vascular than its nasal counterpart. The cilia beat in a coordinated manner toward the ostium, propelling the mucus—which traps inhaled debris and pathogens—into the nasal cavity. This mucociliary clearance represents the primary defence mechanism of the sinuses, and any disruption of this process predisposes to sinusitis.
The mucus produced by goblet cells contains immunoglobulins, particularly IgA, and antimicrobial substances that help protect against infection. The direction of ciliary beat is genetically determined and follows a specific pattern that ensures effective clearance.
Developmental Timeline and Radiological Appearance
Understanding the developmental timeline is crucial for interpreting radiographs in children and for understanding the pathogenesis of sinusitis in different age groups.
- At birth, only the maxillary and ethmoidal sinuses are present, though they are small and continue to develop.
- Maxillary sinus: Becomes radiologically visible at 4-5 months of age.
- Ethmoidal sinus: Becomes visible at approximately 1 year of age.
- Sphenoid sinus: Becomes visible at 4 years of age.
- Frontal sinus: Becomes visible at 6 years of age.
The sinuses continue to grow throughout childhood and adolescence, reaching their final size after puberty. The frontal sinus in particular may continue to pneumatize into early adulthood. This developmental pattern explains why young children rarely develop frontal or sphenoid sinusitis, while maxillary and ethmoidal sinusitis are common in this age group.
Applied Anatomy of Paranasal Sinuses and Clinical Correlations
This section bridges the gap between anatomy and clinical practice, which is essential for exams and practicals.
| Clinical Concept | Anatomical Basis |
|---|---|
| Rhinosinusitis | The continuity of the nasal and sinus mucosa allows infection to spread easily from the nose (rhinitis) to the sinuses (sinusitis). |
| Oroantral Fistula | The close relationship of the maxillary sinus floor to the roots of the maxillary premolars and molars. |
| Odontogenic Sinusitis | Infection from the premolar or molar teeth can directly spread through the thin bony floor into the maxillary sinus. |
| Facial Pain in Sinusitis | Maxillary Sinusitis: Pain over the cheek, often referred to the upper teeth. Frontal Sinusitis: Pain over the forehead. Ethmoidal Sinusitis: Pain behind the eye (retro-orbital). Sphenoidal Sinusitis: Deep-seated vertex or occipital pain. |
| Orbital Complications | The thin lamina papyracea can be breached by infection, leading to orbital cellulitis, abscess, or even cavernous sinus thrombosis. |
| Intracranial Complications | Infection can spread via the thin posterior walls of the frontal and sphenoid sinuses or through the valveless veins (like the ophthalmic veins) to the cavernous sinus and anterior cranial fossa, causing meningitis or brain abscess. |
| Endoscopic Surgery Risks | Onodi Cell: Confusing it for the sphenoid sinus risks optic nerve injury. Debiscent Carotid Artery: A thin or absent bony covering over the ICA in the sphenoid sinus makes it vulnerable to injury. Optic Nerve: A dehiscent optic nerve can be damaged during posterior ethmoidal or sphenoid sinus surgery. |
| Lateral Recess of Sphenoid | This is a surgical challenge and a risk area for injury to the ICA and CN V2 during transsphenoidal approaches. |
——– End of the Chapter——–
High-Yield Points
- Number of sinuses – Four paired sinuses total of eight: maxillary, frontal, ethmoidal, sphenoid
- Largest sinus – Maxillary sinus (Sinus of Highmore)
- First sinus to develop – Maxillary sinus
- Last sinus to develop – Frontal sinus (visible at 6 years, completes growth after puberty)
- Most posterior sinus – Sphenoid sinus
- Drainage site of anterior sinuses – Middle meatus
- Drainage site of posterior ethmoids – Superior meatus
- Drainage site of the sphenoid – Sphenoethmoidal recess
- Basal lamella significance – Divides anterior from posterior sinuses
- Maxillary sinus ostium location – High on the medial wall (gravity-dependent drainage)
- Accessory ostium prevalence – Approximately 30% of maxillary sinuses
- Odontogenic sinusitis cause – Relationship of maxillary sinus floor to premolar/molar roots
- Lamina papyracea – Thin lateral wall of ethmoid, separates sinus from orbit
- Fovea ethmoidalis – Roof of ethmoid, separates sinus from the anterior cranial fossa
- Onodi cell – Posterior ethmoidal cell wrapping around the sphenoid, risks the optic nerve
- Agger nasi cell – Most anterior ethmoidal cell, defines the frontal recess’s anterior limit
- Haller cell – Ethmoidal cell along the orbital floor, which may obstruct the maxillary ostium
- Ethmoid bulla – Largest constant anterior ethmoidal cell, forms the posterior boundary of hiatus semilunaris
- Frontal recess boundaries – Medial: middle turbinate, Lateral: lamina papyracea, Anterior: agger nasi, Posterior: ethmoid bulla
- Sphenoid sinus pneumatization types – Conchal, presellar, sellar
- Critical relations of sphenoid – Optic nerve (superolateral), ICA (inferolateral), V2 (lower lateral), pituitary (roof)
- Blood supply of anterior sinuses – Branches of ophthalmic and maxillary arteries
- Blood supply of posterior sinuses – Sphenopalatine artery
- Nerve supply of sinuses – CN V1 (ethmoidal, frontal, sphenoid), CN V2 (maxillary)
- Sinus development timeline – Maxillary/ethmoid: birth, Sphenoid: 4 years, Frontal: 6 years
NEET PG-Style Multiple Choice Questions
Question 1
- A 28-year-old patient presents with a deep-seated vertex headache that worsens with head movement. Nasal endoscopy reveals purulent discharge in the sphenoethmoidal recess. Which sinus is most likely involved?
A. Maxillary sinus B. Frontal sinus C. Anterior ethmoidal cells D. Sphenoid sinus - During endoscopic sinus surgery, the surgeon encounters a posterior ethmoidal cell that extends laterally to wrap around the sphenoid sinus, placing the optic nerve at risk. This anatomical variation is called:
A. Haller cell B. Agger nasi cell C. Onodi cell D. Ethmoid bulla - A 45-year-old patient develops maxillary sinusitis following the extraction of an upper first molar. The anatomical basis for this complication is:
A. The maxillary sinus ostium is located high on the medial wall B. The floor of the maxillary sinus is intimately related to the roots of maxillary molars C. The maxillary sinus has a thin lateral wall D. The maxillary sinus drains into the middle meatus - All of the following sinuses drain into the middle meatus EXCEPT:
A. Maxillary sinus B. Frontal sinus C. Posterior ethmoidal cells D. Anterior ethmoidal cells - A 32-year-old patient presents with proptosis, ophthalmoplegia, and visual disturbance following a week of worsening sinusitis. Which anatomical structure has most likely been breached?
A. Fovea ethmoidalis B. Lamina papyracea C. Basal lamella D. Posterior wall of frontal sinus - The frontal sinus drains through the frontal recess. Which of the following structures forms the posterior boundary of the frontal recess?
A. Middle turbinate B. Lamina papyracea C. Agger nasi cell D. Ethmoid bulla - A 16-year-old boy undergoes CT imaging for recurrent sinusitis. The scan reveals that his sphenoid sinus extends below the sella turcica. This pneumatization pattern is classified as:
A. Conchal type B. Presellar type C. Sellar type D. Lateral type - Which of the following statements regarding the maxillary sinus is TRUE?
A. Its floor is located above the level of the nasal cavity floor B. Its natural ostium is located on the anterior wall C. It develops after the frontal sinus D. Its arterial supply is exclusively from the maxillary artery - The anterior and posterior ethmoidal arteries, which supply the ethmoid sinus, are branches of which artery?
A. Maxillary artery B. Facial artery C. Ophthalmic artery D. Internal carotid artery - A 55-year-old patient undergoing transsphenoidal pituitary surgery has a sphenoid sinus with a lateral recess extending beyond the V-R line. Which structures are at increased risk during the approach?
A. Optic nerve and internal carotid artery B. Vidian nerve and maxillary nerve (V2) C. Olfactory tract and frontal lobe D. Pituitary gland and cavernous sinus
Answers
- 2. C. 3. B 4. C 5. B 6. D 7. C 8. A 9. C 10. B
Clinical Case Scenarios
Case 1: The Dental Patient with Persistent Sinusitis
Presentation: A 35-year-old woman presents with a 3-week history of right-sided facial pain, nasal congestion, and purulent nasal discharge. She reports that her symptoms began shortly after undergoing the extraction of her upper right first molar. She has completed a 10-day course of amoxicillin but continues to experience pain and now notices that fluid regurgitates into her nose when she drinks.
Questions:
- What is the most likely diagnosis?
- What anatomical relationship explains this presentation?
- How would you confirm the diagnosis?
- What is the definitive management?
Answers:
- The most likely diagnosis is an oroantral fistula with secondary maxillary sinusitis. The fluid regurgitation into the nose is pathognomonic of an oroantral communication.
- The floor of the maxillary sinus is intimately related to the roots of the maxillary first molar. During extraction, the thin bone separating the tooth socket from the sinus may be breached, creating a communication between the oral cavity and the maxillary sinus. This allows oral contents, bacteria, and fluid to enter the sinus, causing persistent sinusitis.
- Diagnosis is confirmed by clinical examination (visualising the fistula in the tooth socket), water drinking test (asking the patient to drink water and observing nasal regurgitation), and CT imaging showing the bony defect and sinus opacification.
- Definitive management involves surgical closure of the fistula using a buccal advancement flap or palatal rotational flap, along with endoscopic sinus surgery to clear the infected sinus contents. Antibiotics and decongestants are used perioperatively.
Case 2: The Patient with Frontal Headache and Periorbital Swelling
Presentation: A 22-year-old man presents with severe frontal headache, fever, and swelling around his left eye. He reports a 10-day history of upper respiratory infection followed by worsening facial pain. On examination, he has erythema and edema of the left upper eyelid, proptosis, and restricted extraocular movements. He is febrile (38.9°C) and appears toxic.
Questions:
- What is the most likely diagnosis?
- What is the anatomical pathway for this complication?
- What imaging study is indicated?
- What is the urgent management?
Answers:
- This patient likely has orbital cellulitis secondary to acute sinusitis, most likely originating from the ethmoidal or frontal sinuses. The proptosis and ophthalmoplegia suggest orbital involvement rather than preseptal cellulitis.
- Infection spreads from the ethmoidal sinuses through the thin lamina papyracea (orbital plate) into the orbit. Alternatively, infection from the frontal sinus can spread through the orbital roof or via valveless veins. The lamina papyracea is the most common route for orbital spread.
- Contrast-enhanced CT of the paranasal sinuses and orbits is the imaging modality of choice. It will show sinus opacification, orbital inflammation, and can differentiate between cellulitis, subperiosteal abscess, and orbital abscess.
- Urgent management includes intravenous antibiotics (covering both aerobic and anaerobic organisms), nasal decongestants, and emergent surgical drainage if a subperiosteal or orbital abscess is present. Endoscopic sinus surgery with orbital decompression may be required.
Case 3: The Patient with Recurrent Sinusitis and Anatomical Variation
Presentation: A 28-year-old woman presents with recurrent episodes of right-sided maxillary sinusitis over the past 2 years. She has failed multiple courses of antibiotics and nasal steroids. CT imaging reveals a well-pneumatized ethmoidal cell extending along the roof of the maxillary sinus, narrowing the infundibulum and obstructing the maxillary ostium.
Questions:
- What is the anatomical variation seen on CT?
- How does this variation predispose to sinusitis?
- What is the surgical approach to correct this problem?
- What other anatomical variations should the surgeon look for on preoperative imaging?
Answers:
- The anatomical variation is a Haller cell—an ethmoidal air cell that extends laterally along the floor of the orbit, lying along the roof of the maxillary sinus.
- Haller cells narrow the ethmoidal infundibulum, which is the drainage pathway for the maxillary sinus. When this pathway becomes compromised, mucus drainage is impaired, leading to recurrent or chronic maxillary sinusitis.
- The surgical approach is endoscopic sinus surgery with removal of the Haller cell to widen the infundibulum and restore normal drainage. This is performed using powered instruments or curettes under endoscopic visualization.
- The surgeon should also look for: Onodi cells (posterior ethmoidal cells adjacent to optic nerve), agger nasi cells (defining frontal recess), concha bullosa (pneumatized middle turbinate), and dehiscent internal carotid artery or optic nerve in the sphenoid sinus.
Case 4: The Patient with Deep Occipital Headache
Presentation: A 45-year-old man presents with a 2-week history of deep, dull occipital headache that worsens when lying flat. He has mild nasal congestion but minimal anterior facial pain. He has no fever but reports fatigue and malaise. Nasal endoscopy reveals a small amount of purulent discharge in the sphenoethmoidal recess.
Questions:
- Which sinus is most likely involved?
- Why is this sinus difficult to diagnose clinically?
- What are the critical anatomical relations that make this sinus high-risk?
- What imaging modality is preferred, and what features should be evaluated?
Answers:
- The sphenoid sinus is most likely involved, given the deep occipital/vertex headache and the endoscopic finding of discharge in the sphenoethmoidal recess.
- Sphenoid sinusitis is difficult to diagnose because symptoms are often non-specific (occipital headache, retro-orbital pain), and anterior facial pain is absent. Physical examination may show no anterior nasal discharge, and the sphenoid ostium is difficult to visualise without angled endoscopes.
- The sphenoid sinus is intimately related to vital structures: the optic nerve (superolateral), internal carotid artery (inferolateral), maxillary nerve (V2) (lower lateral), cavernous sinus (lateral), and pituitary gland (roof). Infection or surgery in this region can lead to blindness, stroke, cranial nerve deficits, or cavernous sinus thrombosis.
- Contrast-enhanced CT is the preferred imaging modality for bony anatomy and surgical planning. MRI with gadolinium is useful for assessing intracranial or cavernous sinus extension. Features to evaluate include: degree of pneumatization (conchal/presellar/sellar), presence of Onodi cells, relationship to the optic nerve and carotid artery, and any dehiscent bone over these structures.
Frequently Asked Questions in Viva
- What are the four paranasal sinuses? The four paranasal sinuses are the maxillary sinuses (largest, in the cheekbones), frontal sinuses (in the forehead), ethmoidal air cells (between the eyes), and sphenoid sinuses (deep in the skull behind the nose), each present as a paired structure, making eight total sinuses.
- Why is the maxillary sinus more prone to infection than other sinuses? The maxillary sinus is more prone to infection because its natural ostium is located high on the medial wall, which prevents gravity-assisted drainage and allows secretions to accumulate, making it difficult for the mucociliary clearance system to effectively empty the sinus.
- What is an Onodi cell, and why is it clinically important? An Onodi cell is a posterior ethmoidal air cell that extends laterally and superiorly to wrap around the sphenoid sinus, placing it in direct contact with the optic nerve; this variation is clinically important because surgeons may mistake it for the sphenoid sinus during endoscopic surgery, risking catastrophic optic nerve injury.
- What is the clinical significance of the lamina papyracea? The lamina papyracea is the paper-thin lateral wall of the ethmoidal air cells that separates the ethmoid sinus from the orbit; it is clinically significant because infection can easily breach it to cause orbital cellulitis, abscess, or cavernous sinus thrombosis, and it is a critical landmark to avoid violating during endoscopic sinus surgery.
- How does dental pathology affect the maxillary sinus? Dental pathology affects the maxillary sinus because the roots of the maxillary premolars and first molar lie directly beneath the sinus floor, often separated by only a thin layer of bone; periapical infections can spread directly into the sinus, causing odontogenic sinusitis, and tooth extraction can create an oroantral fistula.
- What are the types of sphenoid sinus pneumatization? The three types of sphenoid sinus pneumatization are conchal (minimal pneumatization, small cavity), presellar (pneumatization extends to the anterior wall of the sella turcica), and sellar (extensive pneumatization extends below the sella turcica, often with lateral recess formation).
- What is the frontal recess and why is it important? The frontal recess is the drainage pathway connecting the frontal sinus to the middle meatus, bounded by the middle turbinate (medial), lamina papyracea (lateral), agger nasi cells (anterior), and ethmoid bulla (posterior); it is important because narrowing or obstruction of this hourglass-shaped pathway is the primary cause of frontal sinusitis.
Practical Tips for Viva and Clinical Exams
How to Present a Case of Chronic Sinusitis. When presenting a patient with chronic sinusitis during clinical exams, follow this structured approach:
- Step 1: History. “Sir/Ma’am, this is a [age]-year-old [gender] who presents with [duration] of [symptoms]. The patient reports nasal obstruction, purulent nasal discharge, facial pain or pressure, and reduced sense of smell. [Describe any aggravating factors, like bending forward, and any relieving factors. Notably, there is [mention any dental history, trauma history, or previous sinus surgeries].”
- Step 2: Examination. “On anterior rhinoscopy, I observe [describe nasal mucosa, turbinates, discharge]. Nasal endoscopy reveals [describe findings, including which meatus shows discharge, presence of polyps, anatomical variations]. Systemic examination is unremarkable.”
- Step 3: Investigations. “I would obtain a contrast-enhanced CT scan of the paranasal sinuses to assess for [describe anatomical variations, extent of disease, and any complications]. Allergy testing may also be indicated.”
- Step 4: Diagnosis and Management. “Based on the findings, this is a case of chronic rhinosinusitis [with/without nasal polyps]. Management involves [medical therapy including nasal steroids, saline irrigations, antibiotics if indicated] and consideration of functional endoscopic sinus surgery if medical therapy fails.”
Common Viva Questions and Model Answers
- Q: How does the position of the maxillary sinus ostium affect drainage? A: The maxillary sinus ostium is located high on the medial wall, near the roof of the sinus. Because the ostium is not at the lowest point of the sinus, gravity actually works against drainage. Effective drainage depends entirely on the mucociliary clearance mechanism, which transports mucus upward toward the ostium. Any impairment of mucociliary function or obstruction of the ostium leads to sinusitis.
- Q: What are the boundaries of the frontal recess? A: The frontal recess is bounded medially by the middle turbinate, laterally by the lamina papyracea, anteriorly by the agger nasi cells, and posteriorly by the ethmoid bulla. I remember this using the mnemonic “My Lap AP” (Medial: Middle turbinate, Lateral: Lamina papyracea, Anterior: Agger nasi, Posterior: Ethmoid bulla).
- Q: Why is the sphenoid sinus considered the “danger sinus”? A: The sphenoid sinus is considered dangerous because of its intimate relations to vital structures: the optic nerve runs along its superolateral wall, the internal carotid artery courses along its inferolateral wall, the maxillary nerve (V2) lies along its lower lateral wall, and the roof relates to the pituitary gland and cavernous sinus. These structures may be separated from the sinus by only a thin layer of bone that can be dehiscent, making them vulnerable to infection and surgical injury.
- Q: What is the significance of the basal lamella? A: The basal lamella is a bony partition of the middle turbinate that serves as the anatomical dividing line between the anterior sinus group (maxillary, frontal, anterior ethmoidal), which drains into the middle meatus, and the posterior sinus group (posterior ethmoidal, sphenoid), which drains into the superior meatus and sphenoethmoidal recess. This classification guides both diagnostic and surgical approaches.
- Q: How do you distinguish between pre-septal cellulitis and orbital cellulitis? A: Pre-septal cellulitis involves only the eyelids anterior to the orbital septum, with preserved extraocular movements, normal vision, and no proptosis. Orbital cellulitis involves tissues posterior to the orbital septum, presenting with proptosis, ophthalmoplegia, visual disturbance, and pain with eye movement. The lamina papyracea is the key anatomical barrier—when infection breaches this, orbital cellulitis develops.
Tips for Endoscopic Surgery Viva
- Know your landmarks: Be able to identify the middle turbinate, uncinate process, hiatus semilunaris, ethmoid bulla, and sphenoethmoidal recess on endoscopic views.
- Understand the concept of “functional” endoscopic sinus surgery: The goal is not to remove all sinus mucosa but to restore normal ventilation and drainage by removing obstructing anatomical variations and diseased tissue.
- Recognise high-risk variations: Onodi cells, dehiscent carotid artery, low-lying fovea ethmoidalis, and Haller cells should be identified on CT before surgery.
- Know the vessels: Anterior and posterior ethmoidal arteries are at risk during surgery—they lie approximately 24 mm and 12 mm from the anterior lacrimal crest, respectively. Injury can cause retrobulbar hematoma and blindness.
——– End ——–
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s, Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Anatomy of paranasal sinuses for MBBS students, Paranasal sinuses notes for NEET PG, Maxillary sinus anatomy and clinical importance, Ethmoid sinus air cells Onodi cell Haller cell, Frontal sinus drainage pathway frontal recess, Sphenoid sinus relations internal carotid artery optic nerve, CBME curriculum ENT anatomy, Paranasal sinus MCQ for NEET PG, Sinus anatomy viva questions and answers, Clinical anatomy of paranasal sinuses, Endoscopic sinus surgery anatomy, Paranasal sinuses revision notes high yield, Mnemonics for paranasal sinuses, Paranasal sinuses drainage mnemonic, Difference between anterior and posterior ethmoidal cells, Sinusitis anatomical basis, Paranasal sinuses development and radiology, What is the basal lamella in ethmoid sinus, Paranasal sinuses nerve supply, Paranasal sinuses blood supply, Anatomy of paranasal sinuses MBBS notes, paranasal sinuses anatomy for NEET PG, maxillary sinus anatomy and relations, frontal sinus drainage pathway explained, ethmoid sinus air cells anatomy, sphenoid sinus relations to optic nerve, basal lamella clinical significance, Onodi cell surgical risk, Haller cell sinusitis, agger nasi cell frontal recess