Endoscopic Dacryocystorhinostomy
Introduction
Endoscopic dacryocystorhinostomy (DCR) is a surgical procedure performed to bypass an obstructed nasolacrimal duct by creating a new drainage pathway between the lacrimal sac and the nasal cavity.
Anatomy of the Nasolacrimal System
The nasolacrimal drainage system carries tears from the eye to the nose, and it starts at the eyelids and ends in the inferior meatus. Tears first enter the puncta (small openings) present on the upper and lower eyelids. From here, they pass into the superior and inferior canaliculi. Each canaliculus first runs vertically for 1–2 mm, then turns medially and runs horizontally for 8–10 mm. In about 90% cases, both canaliculi join to form a common canaliculus. The common canaliculus runs for 3–5 mm and enters the lacrimal sac high on its lateral wall. At this junction lies the valve of Rosenmuller, which prevents backflow of tears.
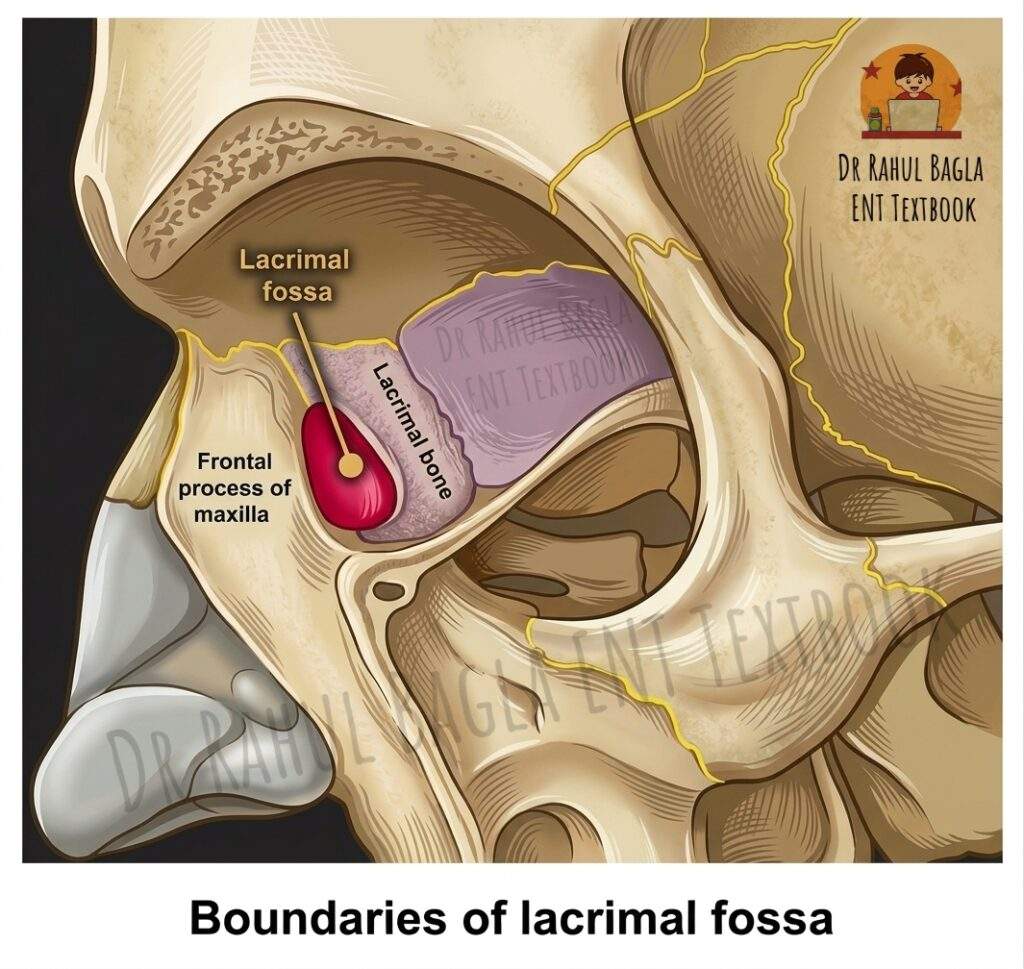
The lacrimal sac lies in the lacrimal fossa on the medial orbital wall. The fossa is formed anteriorly by the frontal process of the maxilla (hard bone) and posteriorly by the lacrimal bone (thin bone). The region posterior to the lacrimal sac, called the retrolacrimal area, consists of extremely thin bone where the uncinate process attaches to the lamina papyracea. Therefore, surgeons must avoid orbital penetration. The sac extends about 10 mm above the axilla of the middle turbinate, which is important during dacryocystorhinostomy. The nasolacrimal duct continues downward for about 12 mm and opens into the inferior meatus near the valve of Hasner, which prevents nasal reflux.
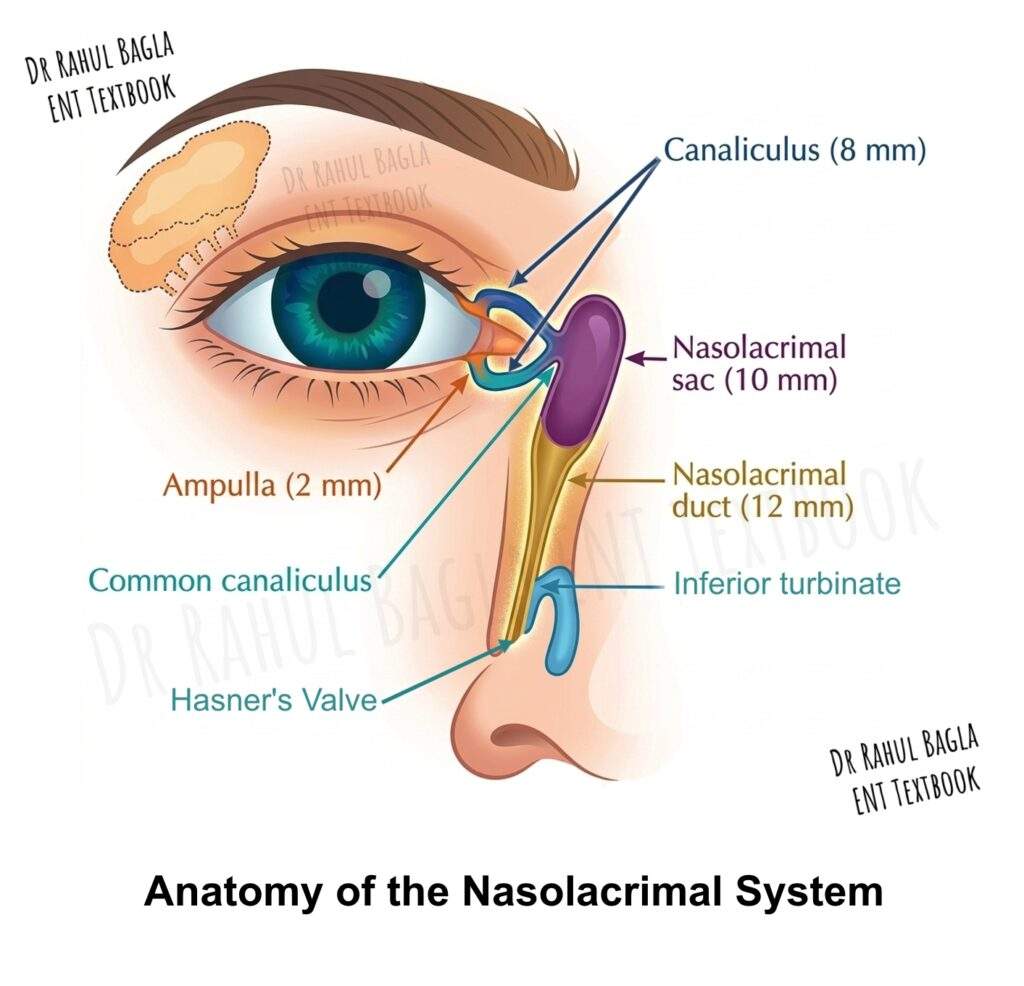
Table: Key Anatomical Landmarks for Endoscopic DCR
| Landmark | Location | Surgical Significance |
| Frontal process of maxilla | Anterior boundary of lacrimal fossa | Hard bone requiring drilling or punching |
| Lacrimal bone | Posterior boundary of lacrimal fossa | Thin bone easily removed with a round knife |
| Axilla of middle turbinate | Superior attachment of middle turbinate | Marks superior limit of lacrimal sac |
| Agger nasi cell | Anterior to middle turbinate attachment | Provides mucosal surface for healing |
| Uncinate process | Posterior to lacrimal sac | Avoid disturbance to prevent orbital injury |
| Hasner’s valve | Distal end of nasolacrimal duct | Site of congenital obstruction |
Pathophysiology of Epiphora
Definition of Epiphora. Epiphora refers to the abnormal overflow of tears onto the face despite normal tear production. Therefore, it results from either hypersecretion of tears (reflex tearing) or, more commonly, obstruction of the nasolacrimal drainage system.
Anatomical Versus Functional Obstruction. Approximately 70% of nasolacrimal system obstructions are anatomical, meaning a physical blockage exists somewhere from the punctum to the nasal cavity. The remaining 30 per cent are functional obstructions, in which the system appears patent on syringing but fails to drain tears adequately due to pump failure or functional narrowing. Functional obstruction often presents a diagnostic challenge because syringing demonstrates free flow, yet the patient continues to experience epiphora. Consequently, dacryoscintigraphy is useful in these cases to demonstrate delayed tear transit through the system.
Aetiology of Nasolacrimal Duct Obstruction
Most cases of nasolacrimal duct obstruction remain idiopathic. However, idiopathic obstruction shows a clear female preponderance and increases in frequency with advancing age.
Less common but important causes include:
- Traumatic Causes: Surgical trauma, particularly during functional endoscopic sinus surgery (FESS), can injure the nasolacrimal duct. Although up to 15% of FESS patients sustain some nasolacrimal injury, clinically significant epiphora remains very rare.
- Inflammatory Causes: Granulomatous conditions such as Wegener’s granulomatosis and sarcoidosis can cause obstruction. Additionally, chronic sinusitis may contribute to secondary inflammation and scarring.
- Neoplastic Causes: Tumours of the lacrimal sac or surrounding structures, though rare, must be excluded, especially in older patients with a mass in the medial canthal region or blood-stained reflux on syringing.
- Infectious Causes: Chronic dacryocystitis results from persistent obstruction and leads to recurrent episodes of acute infection.
- Congenital Causes: Congenital nasolacrimal duct obstruction typically presents with persistent epiphora in infants due to an imperforate Hasner’s valve.
Indications of Endoscopic Dacryocystorhinostomy
Indications
Endoscopic DCR is indicated when a symptomatic distal obstruction of the nasolacrimal duct fails to respond to conservative management. Specifically, the procedure bypasses the obstructed segment by creating a new drainage pathway directly from the lacrimal sac into the nasal cavity.
Primary indications include:
- Chronic epiphora due to complete nasolacrimal duct obstruction confirmed by syringing and probing.
- Recurrent acute dacryocystitis despite medical management with antibiotics and lacrimal massage.
- Chronic dacryocystitis with persistent mucocele or pyocele formation.
- Failed external DCR requiring revision surgery, where the endoscopic approach avoids the previous surgical scar.
- Functional epiphora with delayed transit on dacryoscintigraphy but patent system on syringing, provided conservative measures have failed.
Contraindications of Endoscopic Dacryocystorhinostomy
Absolute Contraindications:
- Obstruction proximal to the lacrimal sac, including canalicular or punctal obstruction, because endoscopic DCR cannot bypass these areas.
- Lacrimal sac malignancy requiring en bloc resection.
Relative Contraindications:
- Severe sinonasal disease with polyposis or extensive scarring, which may impair healing.
- Uncorrected bleeding diathesis or anticoagulation therapy that cannot be temporarily discontinued.
- Poor surgical access due to septal deviation or concha bullosa that the surgeon is unwilling to address concurrently.
Preoperative Evaluation for Endoscopic Dacryocystorhinostomy
History Taking
A thorough history forms the cornerstone of appropriate patient selection. Therefore, ask every patient about the following:
- Duration and laterality of epiphora, including whether it is constant or intermittent.
- Previous episodes of acute dacryocystitis, characterised by painful medial canthal swelling, erythema, and purulent discharge.
- History of midface trauma or previous sinonasal or orbital surgery, including FESS, septoplasty, or facial fracture repair.
- Systemic diseases such as sarcoidosis, granulomatosis with polyangiitis (Wegener’s), or rheumatoid arthritis.
- Radiation exposure to the head and neck region, which may cause late-onset nasolacrimal stenosis.
- Sinonasal symptoms, including nasal obstruction, discharge, or hyposmia, may require concurrent management.
Physical Examination
- Ocular Examination: Inspect the medial canthal area for swelling, erythema, or a palpable mass. Apply digital pressure over the lacrimal sac (Riolan’s test) to observe for mucopurulent reflux through the puncta, which confirms dacryocystitis.
- Nasal Endoscopy: Perform rigid nasal endoscopy to evaluate the lateral nasal wall anatomy, specifically the position of the middle turbinate, uncinate process, and agger nasi cell. Additionally, look for septal deviation, polyps, or tumours that may impede surgical access.
Diagnostic Tests
- Syringing and Probing: This remains the most practical office test. Insert a lacrimal cannula into the inferior punctum and gently irrigate with saline. Free flow into the nose indicates patency, while reflux through the same punctum suggests punctal or canalicular obstruction. Reflux through the opposite punctum indicates complete nasolacrimal duct obstruction.
- Fluorescein Dye Disappearance Test: Apply fluorescein dye to the conjunctival fornix. After 5 to 10 minutes, examine the nasal cavity with a blue light filter. The absence of dye in the nose suggests obstruction. This test also helps evaluate functional obstructions.
- Dacryocystography: This radiographic study involves injecting contrast into the lacrimal system, followed by X-ray imaging. It precisely identifies the level and cause of obstruction, including diverticula, strictures, dacryoliths, or tumours.
- Dacryoscintigraphy: This nuclear medicine study uses technetium-99m instilled into the conjunctival sac. Sequential images track the transit of tears through the system. It proves particularly valuable for diagnosing functional obstruction when syringing appears normal.
- Computed Tomography: CT scanning is generally reserved for suspected neoplastic aetiology, midface trauma requiring surgical reconstruction, or complicated sinus disease requiring concurrent management.
Endoscopic Dacryocystorhinostomy Surgical Technique
Anaesthesia and Patient Preparation
The procedure is typically performed under general anaesthesia to ensure patient comfort and optimise surgical conditions. Additionally, the surgeon should inject the lateral nasal wall with a local anaesthetic containing epinephrine to reduce bleeding and provide postoperative analgesia.
Using a dental syringe, infiltrate 2 ml of 1% lidocaine with 1:100,000 epinephrine into the axilla of the middle turbinate and the frontal process of the maxilla. Subsequently, place neurosurgical cottonoids soaked in 1:3,000 epinephrine into the middle meatus along the frontal process of the maxilla.
Septoplasty Consideration: If septal deviation prevents adequate access to the middle meatus and lateral nasal wall, perform a septoplasty concurrently. Position the septal incision on the contralateral side to avoid traumatising the septal flap with the endoscope. This approach also minimises endoscopic lens clouding from septal bleeding.
Step-by-Step Surgical Procedure of Endoscopic Dacryocystorhinostomy
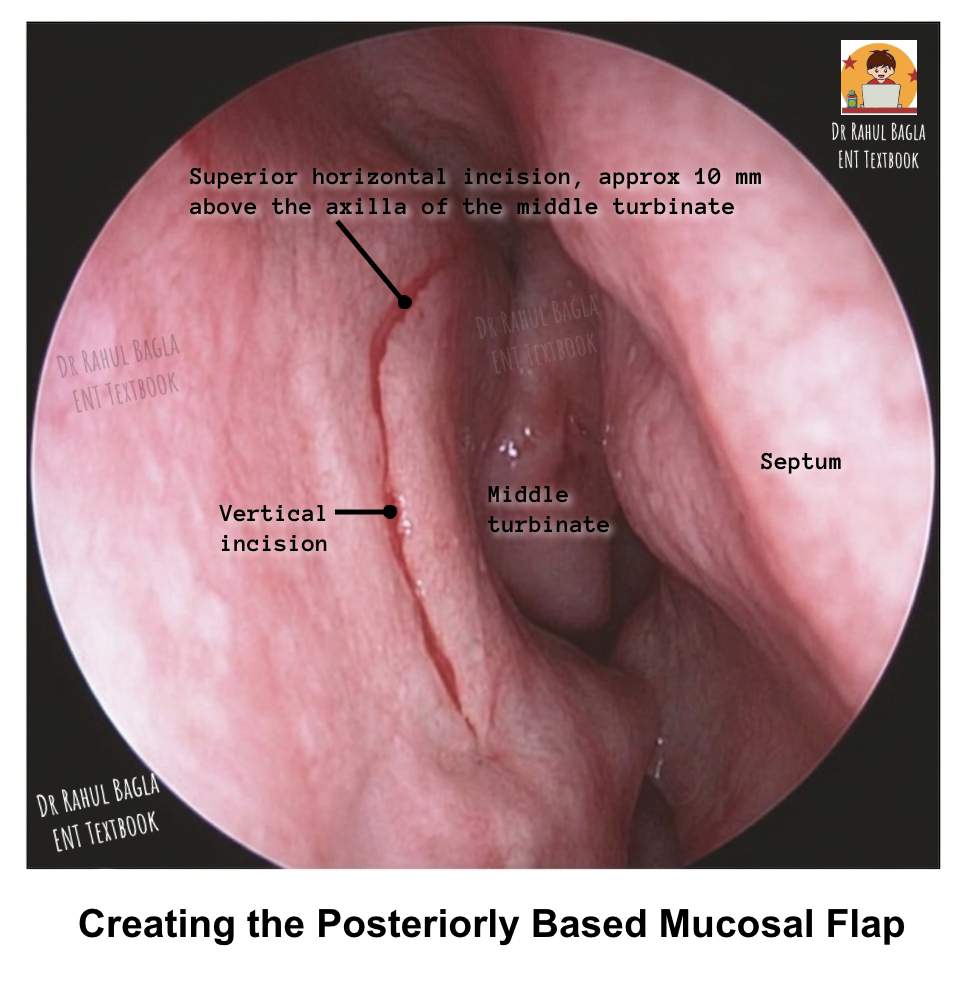
Step 1: Creating the Posteriorly Based Mucosal Flap aims to expose the lacrimal bone and the frontal process of the maxilla. First, a superior horizontal incision is made about 10 mm above the axilla of the middle turbinate, starting 2–3 mm posterior to the axilla and extending forward for about 10 mm onto the frontal process of the maxilla. Then, the blade is turned vertically, and a vertical incision is made on the frontal process of the maxilla, extending downward from the superior incision to just above the insertion of the inferior turbinate. Finally, an inferior horizontal incision is made from the insertion of the uncinate process and extended to meet the vertical incision. Together, these three incisions create a posteriorly based mucosal flap.
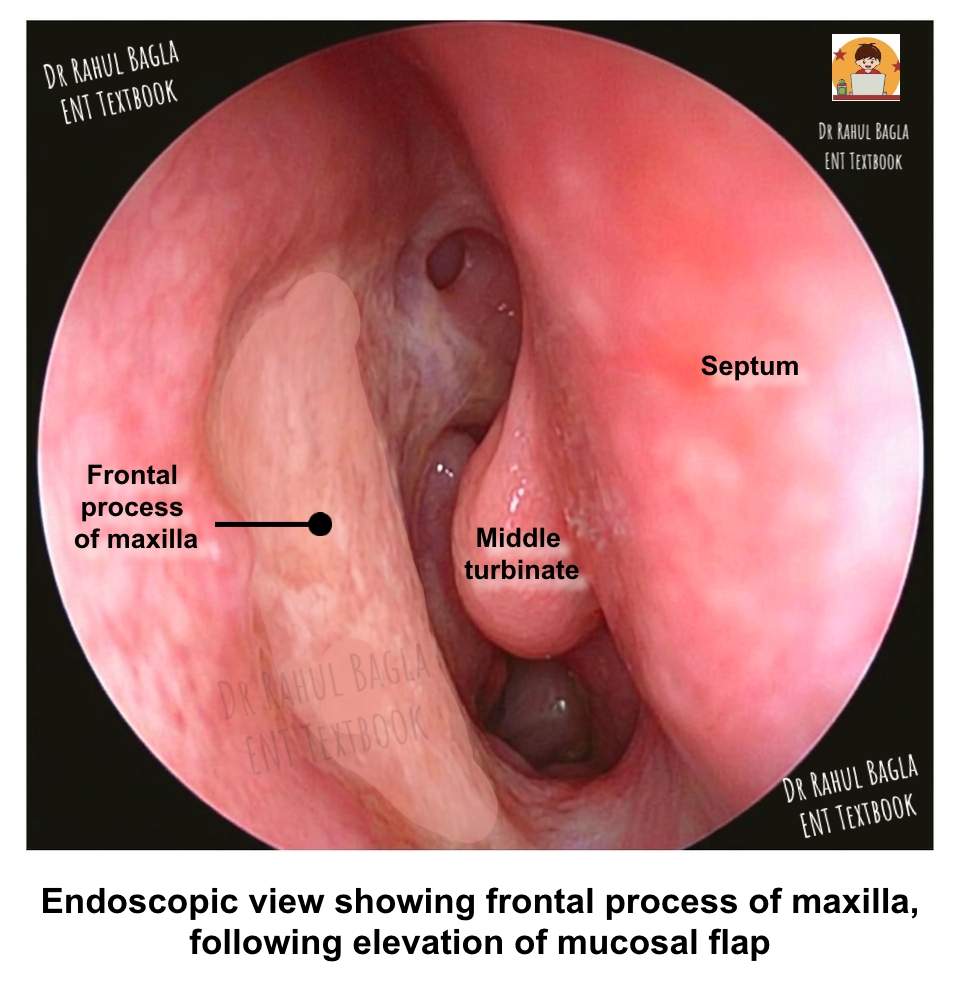
Step 2: Elevating the Mucosal Flap. Use a suction Freer elevator to raise the mucosal flap. Stay directly on the bone throughout this dissection to avoid losing the surgical plane. The transition from the hard frontal process of the maxilla to the soft lacrimal bone represents a critical point where the inexperienced surgeon may inadvertently stray into soft tissue.
Step 3: Removing the Lacrimal Bone. The lacrimal bone overlies the posterior portion of the lacrimal sac and is relatively soft. Therefore, use a round otologic knife to flake off this bone carefully. This manoeuvre exposes the posterior aspect of the lacrimal sac.
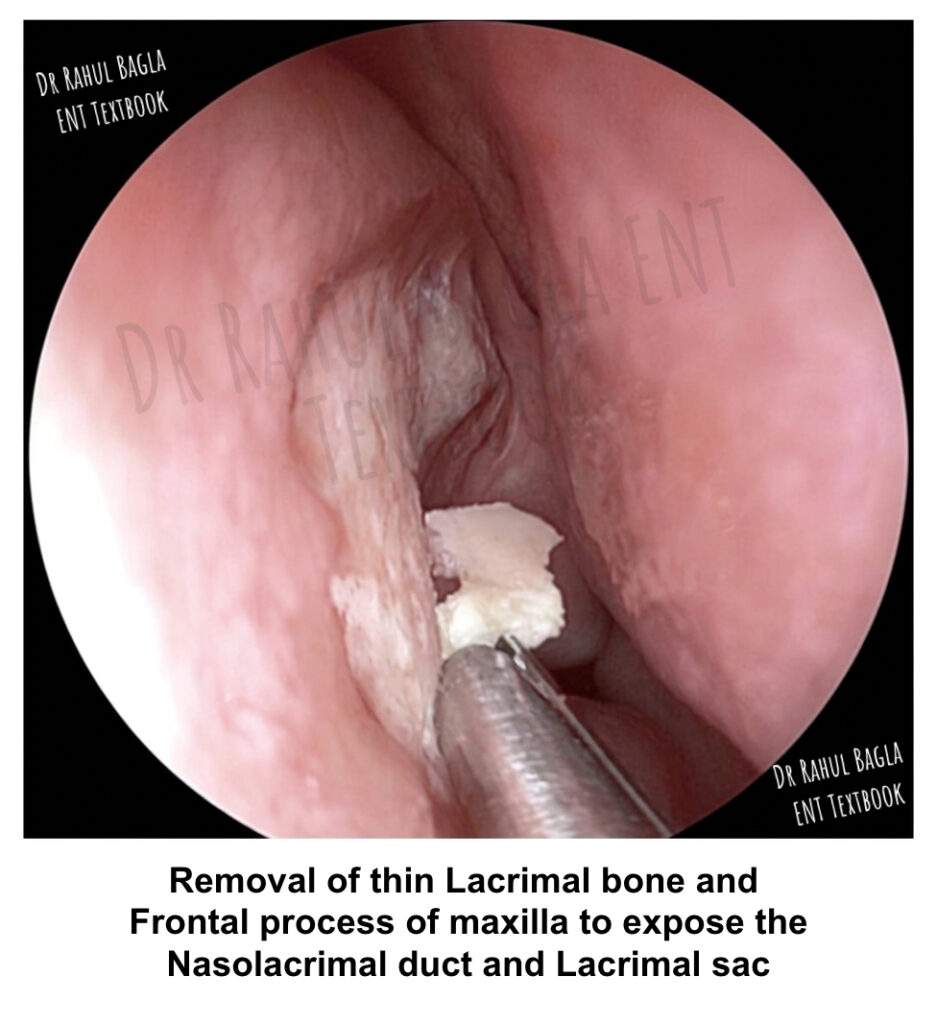
Step 4: Removing the Frontal Process of the Maxilla. This bone is considerably harder and overlies the anterior aspect of the lacrimal sac. Use a Kerrison punch to remove this bone. When the punch can no longer grip the bone adequately, switch to the DCR drill bur. A critical technical tip involves releasing the punch jaws after each bite. If a small piece of the lacrimal sac gets caught between the jaws, releasing the punch allows it to fall free, thereby preventing inadvertent sac trauma. Remove the bone until the entire sac bulges prominently into the nasal cavity. The sac should be fully exposed up to the mucosal incisions.
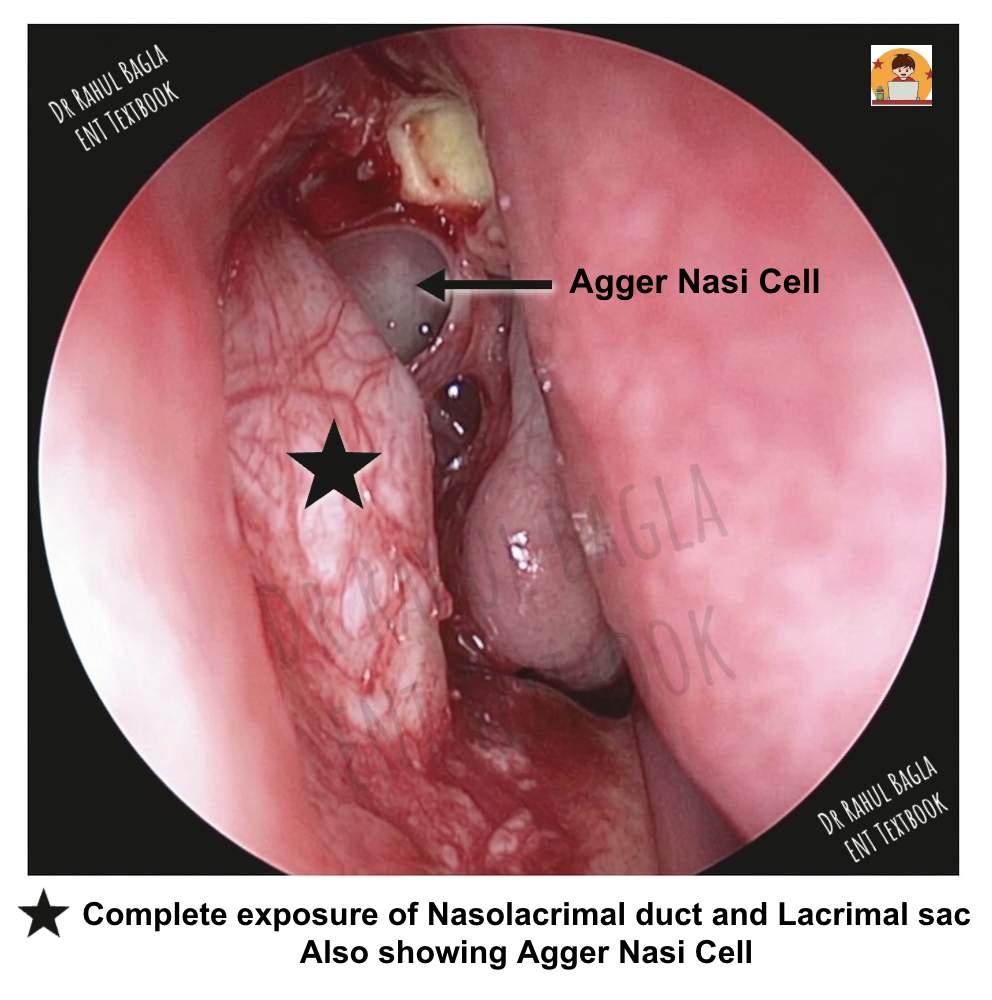
Step 5: Exposing the Agger Nasi Cell. The agger nasi cell sits anterior to the attachment of the middle turbinate. Exposing this cell allows the lacrimal sac mucosa to lie against the agger nasi cell mucosa, allowing for a wider marsupialisation of the lacrimal sac and promoting healing by primary intention. This step significantly improves surgical outcomes.
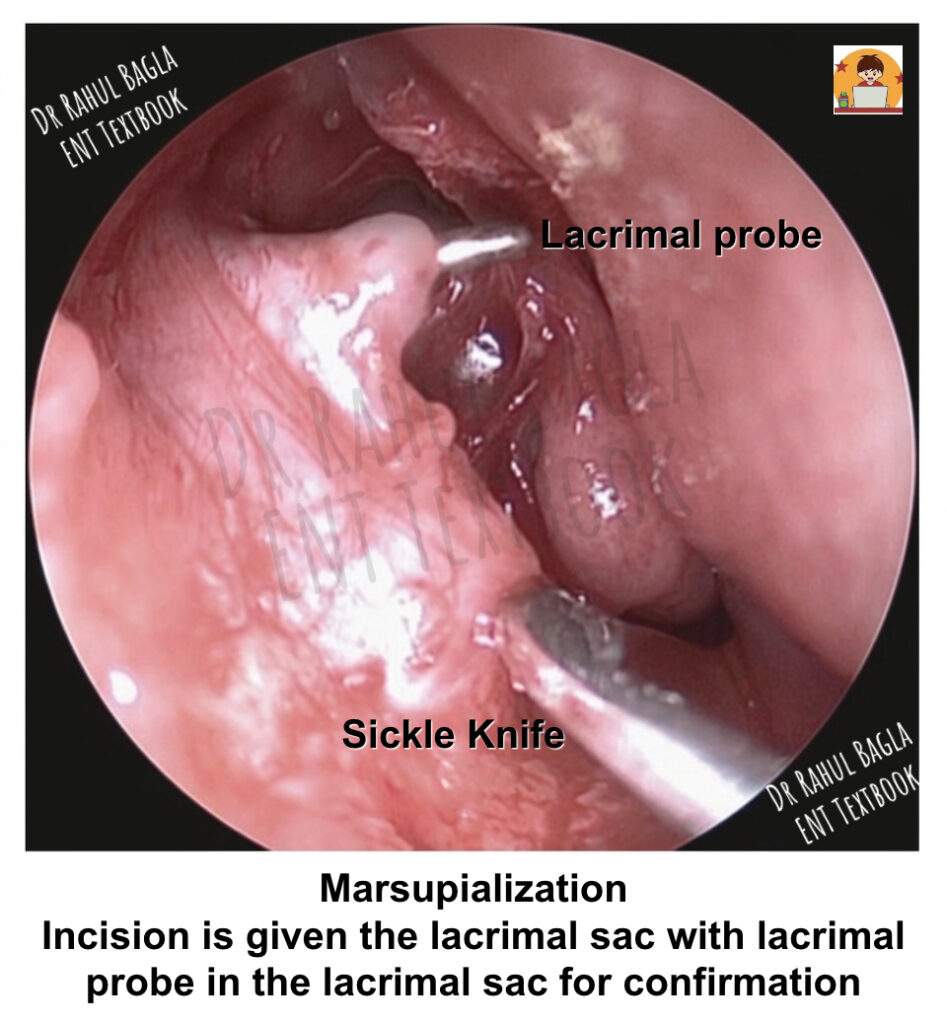
Step 6: Marsupializing the Lacrimal Sac. Insert a lacrimal probe through the inferior canaliculus and tent the lacrimal sac mucosa. Before incising the sac, confirm that you can clearly see the probe prominence on the sac wall. This precaution prevents injury to the common canaliculus. Use a DCR spear knife to make a vertical incision in the sac as far posteriorly as possible. Then use Bellucci micro ear scissors to create superior and inferior releasing incisions in the posterior flap. Finally, use a DCR sickle knife to create corresponding incisions in the anterior flap. The goal is to create the widest possible opening. After complete marsupialisation, the sac should lie flat against the lateral nasal wall.
Step 7: Trimming and Repositioning the Mucosal Flap. Trim the original mucosal flap so that only the superior and inferior limbs remain. Reposition these limbs to approximate the corresponding superior and inferior borders of the marsupialized sac. This step covers exposed bone and promotes mucosal healing.
Step 8: Passing Crawford Silastic Tubes. Insert Crawford tubes through the superior and inferior puncta and advance them into the nasal cavity. These tubes serve three important purposes: they dilate the common canaliculus, they facilitate flap positioning by allowing Gelfoam to be slid up along them, and they promote tear drainage by capillary action. Secure the tubes by tying their ends together or using a ligating clip. Finally, slide a small piece of absorbable gelatin sponge (Gelfoam) along the tubes to hold the mucosal flaps in position.
Flowchart: Endoscopic DCR Surgical Steps
Create mucosal flap → Elevate flap → Remove lacrimal bone → Remove frontal process → Expose agger nasi cell → Marsupialize sac → Trim flaps → Pass Crawford tubes.
Postoperative Management of Endoscopic Dacryocystorhinostomy
Immediate Postoperative Care. Discharge the patient with specific instructions to use saline nasal sprays frequently for moisture and crust removal. Prescribe a 7-day course of oral antibiotics to prevent infection. Additionally, administer topical antibiotic eye drops for 2 weeks.
Follow-Up Schedule
- At 2 Weeks: Perform endoscopic examination and gently remove any crusts from the surgical site. The mucosal flaps should appear pink and healthy.
- At 4 to 6 Weeks: Remove the Crawford tubes. Check patency of the lacrimal system using the fluorescein dye disappearance test. Additionally, perform the Valsalva bubble test by asking the patient to blow against a closed nose while observing bubbles emerging from the DCR ostium.
Long-Term Outcomes. Success rates for endoscopic DCR range from 85 to 95%, comparable to the external approach. Success is defined as complete resolution of epiphora or significant improvement such that the patient requires no further intervention.
Complications and Their Management of Endoscopic Dacryocystorhinostomy
Intraoperative Complications
- Epistaxis: Bleeding occurs in approximately 2% of patients. Control bleeding with topical epinephrine, bipolar cautery, or nasal packing as needed.
- Orbital Penetration: This complication results from aggressive dissection posterior to the lacrimal sac, where the bone is extremely thin. Prevent this by staying anterior to the uncinate process insertion. If orbital fat is visualised, stop further dissection in that area and observe for signs of extraocular muscle dysfunction or orbital hematoma.
- Cerebrospinal Fluid Leak: This rare but serious complication occurs if dissection extends too superiorly toward the skull base. The cribriform plate sits approximately 10 to 15 mm above the axilla of the middle turbinate. Therefore, staying below this level prevents CSF leak.
- Damage to Common Canaliculus: This complication typically results from incising the sac without clearly visualising the lacrimal probe. Prevent this by always confirming probe visibility before making the sac incision.
Postoperative Complications
- Restenosis: The most common cause of late failure is inadequate exposure of the common canaliculus or sac. Revision surgery requires creating a larger osteotomy and may benefit from mitomycin C application or mucosal grafting.
- Granulation Tissue Formation: Excessive granulation tissue can obstruct the ostium. Manage with endoscopic debridement and topical steroid sprays.
- Synechiae Formation: Adhesions between the lateral nasal wall and septum or turbinate can occur. Prevent by placing Gelfoam between raw surfaces.
- Rhinosinusitis: Obstruction of frontal or maxillary sinus drainage may occur if the surgery disrupts normal sinus outflow pathways. Manage with medical therapy and endoscopic sinus surgery if persistent.
Table: Complications of Endoscopic DCR
| Complication | Prevention | Management |
| Epistaxis | Careful hemostasis | Topical epinephrine, packing |
| Orbital penetration | Stay anterior to uncinate | Observe, ophthalmology consult |
| CSF leak | Avoid superior dissection | Lumbar drain, repair if persistent |
| Common canaliculus injury | Visualize probe before incision | Stenting, revision surgery |
| Restenosis | Wide marsupialization | Revision DCR with mitomycin C |
| Granulation tissue | Mucosal flap coverage | Debridement, steroid spray |
Special Considerations: Revision Endoscopic DCR
Failed DCR most commonly results from inadequate exposure of the common canaliculus and lacrimal sac superiorly. Therefore, in revision surgery, palpate the bone above the axilla of the middle turbinate to assess the previous osteotomy size. Sharply dissect a mucosal flap from the underlying prelacrimal sac tissue. Consider harvesting a free mucosal graft from the agger nasi cell to prevent secondary fibrosis and granulation tissue formation. Application of mitomycin C, an antifibrotic agent, has demonstrated benefit in revision endoscopic DCR. Apply mitomycin C 0.4 milligrams per millilitre to the osteotomy site for 5 minutes before rinsing. Leave Crawford stents in place for 6 to 8 weeks postoperatively, longer than in primary surgery. Additionally, prescribe topical steroid drops for 1 to 2 weeks to reduce inflammation.
Endoscopic Versus External DCR
External DCR remains an excellent procedure with success rates exceeding 90%. However, endoscopic DCR offers distinct advantages, including no facial scar, shorter operative time, avoidance of the angular vessel, and the ability to address concurrent sinus disease.
The primary disadvantage of endoscopic DCR is the steep learning curve. Additionally, equipment costs are higher, and the success rate may be slightly lower in the hands of inexperienced surgeons.
Table: Endoscopic Versus External DCR
| Feature | Endoscopic DCR | External DCR |
| Scar | None | Facial scar (medial canthus) |
| Operative time | 30-45 minutes | 45-60 minutes |
| Success rate | 85-95% | 90-95% |
| Equipment | Endoscopes, drills | Basic instruments |
| Learning curve | Steeper | Gradual |
| Sinus disease | Can address concurrently | Cannot address |
| Bleeding | Less | More (angular vessel) |
—-End of the Chapter—-
High-Yield Points for NEET PG and University Exams
- Endoscopic DCR treats distal nasolacrimal duct obstruction.
- It does not bypass punctal/canalicular obstruction.
- The lacrimal sac extends ~10 mm above the axilla of the middle turbinate.
- Common canaliculus enters high in the lacrimal sac; therefore, high osteotomy is essential.
- The frontal process of the maxilla is hard, lacrimal bone is thin.
- The retrolacrimal region near the uncinate insertion is thin → risk of orbital injury.
- The most common failure cause is inadequate sac exposure and a small osteotomy.
- Crawford stents help maintain patency and reduce the canalicular narrowing effect.
- Post-op endoscopic cleaning at 2 weeks is critical for long-term success.
- Epistaxis is the most common immediate complication.
Common examiner viva questions
- What is the principle of DCR?
- Why must osteotomy extend above the axilla?
- What is the valve of Hasner?
- What is ROPLAS?
- What causes the failure of DCR?
- Why open agger nasi cell?
- Why do we use Crawford tubes?
NEET PG Style MCQs
- The most important factor for success in endoscopic DCR is: A. Use of Crawford stent B. Wide marsupialization of lacrimal sac C. Packing the nose for 48 hours D. Removing inferior turbinate
- Lacrimal sac lies in the lacrimal fossa formed by: A. Ethmoid and sphenoid B. Frontal bone and ethmoid C. Frontal process of maxilla and lacrimal bone D. Palatine bone and vomer
- The nasolacrimal duct opens into: A. Middle meatus B. Superior meatus C. Inferior meatus D. Sphenoethmoidal recess
- Endoscopic DCR is contraindicated in: A. Distal nasolacrimal duct obstruction B. Canalicular obstruction C. Chronic dacryocystitis D. Failed external DCR
- The lacrimal sac extends approximately how much above the axilla of middle turbinate? A. 2 mm B. 5 mm C. 10 mm D. 20 mm
- The thick hard bone that overlies the anterior lacrimal sac is: A. Lacrimal bone B. Frontal process of maxilla C. Vomer D. Palatine bone
- Most common cause of endoscopic DCR failure is: A. CSF leak B. Inadequate sac exposure and small ostium C. Excessive antibiotics D. Use of nasal steroids
- Functional epiphora refers to: A. Complete blockage of nasolacrimal duct B. Excess tear production only C. Delayed tear drainage without complete blockage D. Obstruction at punctum only
- The valve guarding opening of nasolacrimal duct is: A. Valve of Rosenmüller B. Valve of Hasner C. Valve of Eustachius D. Valve of Krause
- During endoscopic DCR, the danger of orbital penetration increases if the surgeon injures: A. Inferior turbinate head B. Uncinate insertion region C. Septal cartilage D. Nasal floor
Answers with Explanations
1: B 2: C 3: C 4: B 5: C 6: B 7: B 8: C 9: B 10: B
Clinical Case Scenarios
- Case 1. A 7-year-old child presents with fever and eyelid swelling. Vision is normal, and ocular movements are full. CT shows only preseptal swelling. Question: Diagnosis and management? Answer: Preseptal cellulitis. Treat with IV antibiotics, nasal decongestants, and close observation.
- Case 2. A 16-year-old boy has a severe headache, fever, vomiting, and drowsiness. He had mild sinus symptoms 5 days ago. CT PNS shows frontal sinusitis, but neurological signs persist. Question: Next best investigation and likely complication? Answer: MRI brain with contrast. Likely subdural empyema or cerebritis.
- Case 3. A patient has proptosis, chemosis, ophthalmoplegia, and decreased colour vision. CT shows a medial rim-enhancing collection adjacent to the lamina papyracea. Question: Diagnosis and management? Answer: Subperiosteal abscess. Requires IV antibiotics + urgent surgical drainage (endoscopic ethmoidectomy).
- Case 4. A diabetic patient presents with facial pain, black nasal crusts, orbital swelling, and cranial nerve palsy. Question: Most likely diagnosis and immediate management? Answer: Rhino-orbito-cerebral mucormycosis. Emergency antifungal therapy (liposomal amphotericin B), surgical debridement, and strict glycemic control.
—-End—-
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Endoscopic dacryocystorhinostomy (Endoscopic DCR) is a standard minimally invasive ENT procedure used to treat epiphora caused by nasolacrimal duct obstruction. It creates a direct drainage pathway between the lacrimal sac and nasal cavity. Therefore, it restores tear drainage and prevents recurrent dacryocystitis. This chapter explains anatomy, indications, evaluation, surgical steps, complications, revision surgery, and exam-focused points in a structured and student-friendly format. Endoscopic DCR notes for MBBS students, Endoscopic dacryocystorhinostomy step by step, Endoscopic DCR surgery procedure ENT, Dacryocystorhinostomy indications and contraindications, Endoscopic DCR anatomy middle turbinate axilla, Nasolacrimal duct obstruction diagnosis and treatment, Epiphora causes and management in ENT, Difference between external and endoscopic DCR, Endoscopic DCR complications and prevention, Endoscopic DCR viva questions and answers, Endoscopic DCR NEET PG MCQs, Endoscopic DCR revision surgery technique, Fluorescein dye disappearance test interpretation, Syringing and probing test in epiphora, Crawford tube stenting in DCR, Valve of Hasner location and significance, Lacrimal sac anatomy for endoscopic DCR, Endoscopic DCR operative steps with diagram, DCR surgery CBME ENT curriculum, Endoscopic DCR high yield points for exams