|
The following CBME core competencies are covered in this chapter.
|
Disorders of The External Auditory Canal
Introduction
The external auditory canal (EAC) is a narrow, skin-lined passage that often falls prey to a wide range of disorders, from simple wax impaction to severe, life-threatening infections. Understanding these conditions is essential for every medical student because EAC disorders are among the most common complaints encountered in ENT outpatient departments. This chapter provides a comprehensive, exam-oriented overview of obstructive, inflammatory, bony, and traumatic disorders of the EAC, aligned with the CBME curriculum for MBBS and ENT PG students.
Table: Disorders of the External Auditory Canal
| 1. | Obstructive Disorders of External Auditory Canal | Impacted Wax |
| 2. | Infections and Inflammatory Disorders of External Auditory Canal | Furuncle, Diffuse Acute Otitis Externa, Otomycosis, Haemorrhagic Otitis Externa, Herpes Zoster Oticus, Aural polyps, Acquired atresia of EAC |
| 3. | Bony Lesions of External Auditory Canal | Exostosis, Keratosis Obturans, Cholesteatoma of External Auditory Canal |
| 4. | Reactive Dermatological Disorders | Eczematous Otitis Externa, Neurodermatitis, Seborrhoeic Otitis Externa |
| 5. | Trauma | Trauma of External Auditory Canal |
Obstructive Disorders Of External Auditory Canal
1. Impacted Wax or Cerumen
Anatomy: Outer third hair-bearing canal skin lined by sebaceous glands and modified apocrine ceruminous glands. Sebaceous glands secrete sebum (oily material from the breakdown of fat-containing cells). Ceruminous glands secrete cerumen (fluid rich in lipids and pigment granules) excreted at the base of hair follicles. Wax is a mixture of desquamated cells, cerumen, sebum, shed hair, keratin, and dirt.
Types of Ear Wax:
- Dry wax: Lacks cerumen, yellow or grey in colour, and hard in consistency
- Wet wax: Brown in colour and soft and sticky in consistency.
Functions of Wax:
- Lubricates and cleans the canal
- Traps dirt and microbes by virtue of its antimicrobial properties.
- Bacteriostatic and fungistatic due to acidic pH
Pathogenesis of Impaction: Normally, self-cleaning, dry wax migrates down the hair and moves out by jaw movements. Narrow/tortuous canal, stiff hair, or obstructive lesions (exostosis) favour wax retention. May dry and form a hard impacted mass.
Clinical Features:
- Usually, an incidental, symptomless finding
- Sense of heaviness and a blocked ear with decreased hearing
- Complete occlusion may cause hearing loss up to 40 dB
- Itching, earache, tinnitus, cough
- Wax granuloma from ulceration of long-standing impacted wax
Indications for Wax Removal: Ear symptoms needing examination (ear discharge, otalgia, hearing loss).
Treatment:
- Wax softening agents: In young children or if there is hard impacted wax, softening agents like 5% sodium bicarbonate, olive oil, hydrogen peroxide, liquid paraffin and commercial agents such as 2% paradichlorobenzene are frequently used to help wax removal by syringing or instruments.
- Syringing and irrigation: It is the most common procedure used for wax removal in a clinical setting. A syringe containing water at body temperature is directed along the posterosuperior wall of the meatus. Pressure of water deep to the wax expels the wax out of the canal. Mopping is done with a cotton pledget following the procedure to make ear dry. It is performed after taking a complete history (past history of ear discharge or an existing perforation) and ear examination. The patient may complain of intense pain and giddiness. Contraindications are otitis externa, history of ear discharge, temporal bone fracture, Vegetable foreign body and uncooperative patients, especially young children. Complications of syringing are traumatic perforation, vasovagal attack, Impaction of a foreign body, and vertigo because of stimulation of the labyrinth.
- Removal under direct vision: It is done with the aid of a headlight, microscope or endoscope, with ear probes or suction tips. It also helps in wax removal from the attic and open mastoid cavities.
Infections And Inflammatory Disorders of External Auditory Canal
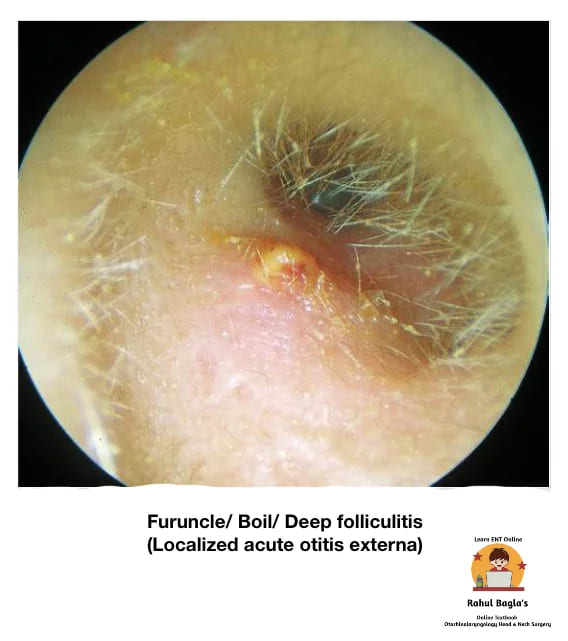
1. Furuncle / Boil / Deep Folliculitis (Localised Acute Otitis Externa)
Definition: It is an infection around the hair follicle (usually seen in the cartilaginous part of the meatus ) that turns into a pustule and progresses to form a local abscess. A furuncle may occur as a single lesion or may spread to involve surrounding structures (cellulitis).
Predisposing Factors:
- Scratching the canal with contaminated sticks or metallic objects
- Trauma to EAC
- Immunocompromised patients (diabetes)
- Allergy, hereditary factors
- Improper size of hearing aid moulds or stethoscope earpieces
Symptoms:
- Excruciating pain and tenderness out of proportion to furuncle size
- Pain in the ear during chewing and pinna movements
- Conductive hearing loss and ear blockage if the canal is stenosed
- Purulent discharge is sometimes seen
Signs:
- Tragal sign is positive (Tenderness present over tragus).
- EAC will be oedematous, making otoscopic examination difficult.
- Swelling over the mastoid with obliteration of the retroauricular groove.
- Periauricular lymph nodes may also be enlarged and tender.
Complication: Repeated infection may cause permanent scarring, fibrosis, and stenosis of the meatus.
Treatment:
- When there is no abscess, the patient can be managed with hot fomentation, systemic/oral antibiotics and analgesics.
- A small ear pack of 10% ichthammol glycerine alleviates pain, reduces oedema and has antiseptic action. Intranasal mupirocin ointment can be prescribed.
- If an abscess has formed, incision and drainage are required
- In recurrent furunculosis, diabetic status should be evaluated, and the patient’s nasal vestibules and fingers need to be checked for staphylococci. The pathogenic strain may even colonize in nostrils and the perineum.
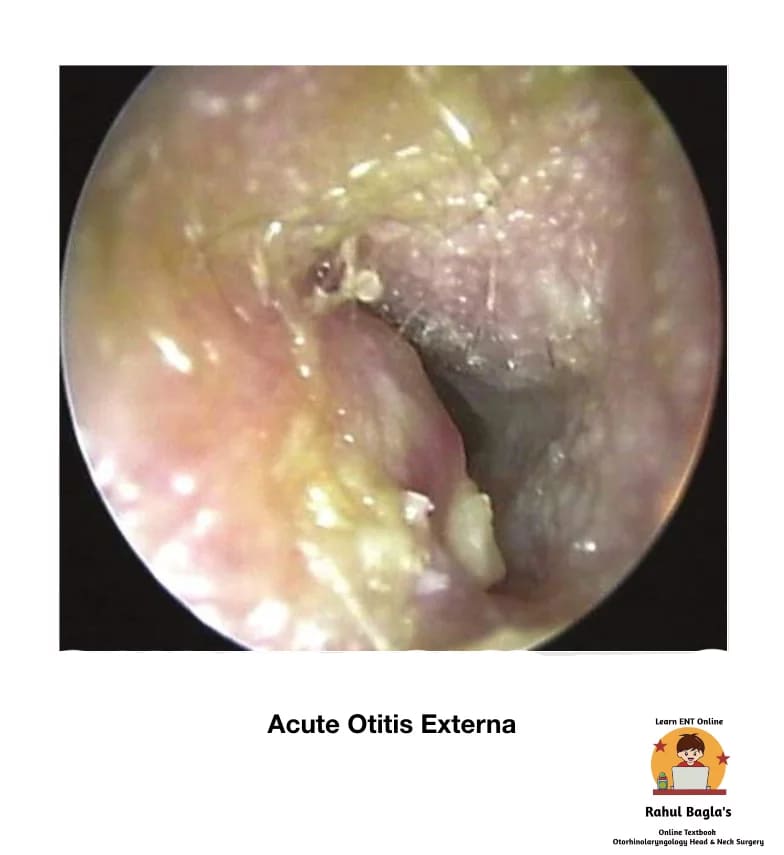
2. Diffuse Acute Otitis Externa (Swimmer’s Ear)
Definition: It is a generalised inflammation of the meatal skin and subcutaneous tissue of the external auditory canal. The infection may further spread to involve the pinna and epidermal layer of the tympanic membrane.
Aetiology:
- Anatomical: Narrow EAC (hereditary, iatrogenic, exostoses, trauma); EAC obstruction (keratosis obturans, wax, foreign body, hearing aid, in-ear headphones)
- Allergic: Atopy, non-atopic allergy, exposure to topical ear drops
- Trauma: Ear probing, skin maceration (bathing or irrigation), laceration, radiotherapy
- Bacterial: Staphylococcus aureus, Pseudomonas pyocyaneus, Bacillus proteus, Escherichia coli (most cases mixed infection). A warm, humid environment favours bacterial growth.
- Dermatological: Eczema, seborrheic dermatitis, psoriasis
- Immunocompromised states (diabetics)
Clinical Features: Clinical diagnosis from pain, itching, oedema, erythema of EAC with purulent otorrhoea and debris.
Acute Phase:
- Hot, burning sensation in the ear
- Pain aggravated by jaw movements
- Thin serous discharge is becoming thick and purulent
- Meatal lining inflamed and swollen
- Conductive deafness from debris, discharge, and meatal swelling
- Severe cases: enlarged and tender local lymph nodes, cellulitis of surrounding tissues
Chronic Phase (>6 months):
- Irritation and a strong desire to itch
- Itching increases the chances of acute exacerbations and recurrent infection
- Scanty discharge that may dry to crusts
- Thick, swollen meatal skin with scaling and fissuring
- Rarely: meatal skin becomes hypertrophic, leading to meatal stenosis (chronic stenotic otitis externa)
Pathology Stages:
| Stage | ||
| 1 | Pre-inflammatory | There is disruption of the protective lipid/acid balance (normal pH 4–5). Stratum corneum is oedematous, sebaceous and apocrine glands gets blocked producing features like aural fullness and itching. |
| 2 | Acute inflammatory | Further oedema, obliteration of the lumen and increase in pain. In the severe stages, cervical lymphadenopathy may be seen. |
| 3 | Chronic inflammatory | By definition, chronic otitis externa occurs after 6 months. It is characterised by thickening of the skin of ear canal. |
Treatment:
- Aural toilet: Regular and thorough removal of all exudate and debris.
- A wick soaked in an antibiotic-steroid preparation is inserted in the ear canal, and the patient is instructed to keep it moist by instilling the ear drops twice or thrice a day. The wick must be changed every day (for 2-3 days), and then it is substituted with ear drops.
- Steroid drops relieve oedema, erythema and prevent itching.
- A wick of mild astringent like aluminium acetate (8%) or silver nitrate (3%) can be used to form a protective coagulum and dry up oozing meatus.
- Ear pack with 10% ichthammol glycerine provides splintage and reduces pain. The hygroscopic action of glycerine reduces oedema, while ichthammol is mildly antiseptic.
- Analgesics are prescribed for pain relief.
- Broad-spectrum systemic antibiotics for treating complications.
Outcomes and Complications:
- A mild case of otitis externa resolves spontaneously because the epithelial barrier gets re-developed, pilo-apocrine units produce normal secretions, and the pH of the canal returns to normal.
- However, in cases where inflammation is progressing at a faster rate than repair, the condition of the patient deteriorates. There is an increase in intensity of pain, otorrhoea and oedema of the canal.
- Due to the rich lymphatic drainage of the area, lymphadenopathy often occurs, and soft-tissue infection can progress, leading to perichondritis, chondritis, cellulitis, parotitis and/or erysipelas.
- In the immunocompromised host, malignant otitis externa (periostitis/ osteomyelitis of the skull base) can develop.
3. Otomycosis
Definition: It is a superficial mycotic infection of the external ear canal. Otomycosis is suspected if patients with otitis externa fail to respond to topical antibiotic/steroid drops.
Predisposing Factors:
- Hot, humid climate (tropical and subtropical countries)
- Secondary fungal growth after prolonged topical antibiotics
- Diabetes and other immunocompromised states
- Swimming
Causative Micro-organisms:
- Aspergillus niger(commonest, black-headed filamentous growth)
- Aspergillus fumigatus(pale blue or green)
- Candida albicans(white or creamy deposit)
- Actinomycosis
- Dermatophytes
Clinical Features:
- Itching, irritation, discomfort, or severe pain (mainly in Aspergillus flavus)
- Meatal skin red and oedematous
- Watery discharge with musty odour
- Ear blockage, decreased hearing
- Fungal mass: white, brown, or black, looks like wet filter paper or sheets
Investigations:
- Culture sensitivity and fungal smear
- Blood sugar for diabetes
Treatment:
- Cleaning/debridement of the ear canal by syringing, suction or mopping.
- Keeping the ear canal dry is a paramount step in management.
- Antifungal drops for one week (nystatin, clotrimazole and povidone-iodine)
- Anti-histaminic ear drops to relieve itching
- Anti-inflammatory analgesics
- 2% salicylic acid in alcohol to remove the superficial epidermal layer along with fungal mycelium growing in this layer.
- Treat the underlying cause, e.g. diabetes.
- In cases of resistant otomycosis, fungal infection elsewhere in the body must be excluded and treated with systemic antibiotics.

4. Haemorrhagic Otitis Externa
It may develop as a post-influenza complication. The patient complains of severe pain in the ear, and there is formation of blood-filled haemorrhagic bullae on the tympanic membrane and deep meatal walls. If bullae rupture, there may be blood-stained discharge.
Treatment: Analgesics and antibiotics
5. Herpes Zoster Oticus (Ramsay Hunt Syndrome)
It is a viral infection involving the geniculate ganglion of the facial nerve. It is characterised by the appearance of vesicles on the tympanic membrane, deep meatus, concha and retroauricular sulcus. It is caused by the reactivation of the latent Varicella Zoster virus in the geniculate ganglion. It may involve the VIIth (more often) and the VIIIth cranial nerves. The syndrome is more common in old age,>60 years.
Clinical features:
- Anaesthesia of the face, giddiness and hearing impairment due to involvement of the Vth and VIIIth nerves.
- Excruciating (severe) otalgia.
- Vesicles in EAC on the affected side
- Facial nerve palsy (LMN type).
- Tinnitus, vertigo and a sensorineural hearing loss.
Complications:
- Post-herpetic neuralgia.
- Eye damage (blurred vision) may occur.
- Hearing loss & facial weakness may be permanent.
Prognosis: The prognosis for Ramsay Hunt is worse than that of idiopathic facial palsy. Persistent weakness is observed in 30–50% of patients. Only 10% recover completely after a complete loss of function without treatment.
Prevention: Children are vaccinated against chickenpox, which reduces their chances of getting the infection
Treatment:
- The recommended regimen is prednisone 1mg/kg/day for 5 days, then tapered for 10 days, and intravenous acyclovir (250 mg three times daily). The combination of steroids and acyclovir also seems to reduce otalgia, vertigo and post-herpetic neuralgia.
- Oral acyclovir 800mg 5 times a day for 7-10 days.
- Surgical decompression is not indicated.

Herpes zoster oticus
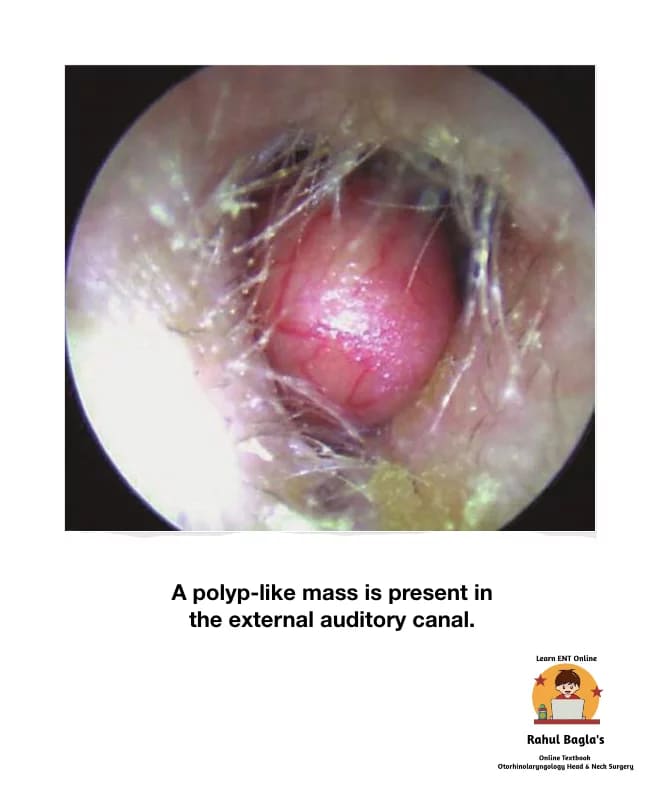
6. Aural polyps
Aural polyps are well-circumscribed, soft, fleshy masses frequently found in the EAC. They are inflammatory in nature and generally arise from the middle ear and are suggestive of active disease in the middle ear. Polyps may also result from secondary chronic inflammation due to a foreign body (i.e. grommet) in the middle ear. Additionally, polyps may be seen as a manifestation of myringitis, malignant otitis externa, or other neoplastic or inflammatory lesions. Histopathologic examination can be done if the cause of a polyp is unknown. A polyp has an epithelial lining that differentiates it from granulation tissue.
Differential diagnosis: Neoplastic and granulomatous conditions such as tuberculosis, syphilis, xanthomatosis and eosinophilic granuloma.
Investigations: CT scan is advisable if the polyp is not responding to medical treatment or if cholesteatoma is suspected.
Management
- Gentle aural toilet + antibiotic-steroid topical drops → reduces inflammatory response, decreases polyp size, allows access for examination
- Cauterization with silver nitrate
- Biopsy for polyps of uncertain origin to rule out malignancy
- Polypectomy if the polyp persists (under anaesthesia if necessary)
- WARNING: Polyps must not be removed or avulsed blindly, as they may be adherent to stapes superstructure, dehiscent facial nerve, or cholesteatoma overlying labyrinthine fistula.
7. Acquired atresia of EAC
Atresia is defined as the absence or closure of the EAC.
Causes:
- Inflammation
- Chronic otitis externa
- Reactive dermatological disorders (i.e. eczematous otitis externa)
- Chronic suppurative otitis media
- Trauma
- Open injury (lacerations, gunshot injury)
- Fracture mandible
- Facial injury
- Fracture of the tympanic plate
- Burns. It can be thermal, chemical, electrical or post-irradiation.
- Surgery. Any meatal approach surgery (i.e. tympanoplasty)
Treatment:
Medical
- Topical ear drops (corticosteroid and antibiotic preparation)
- Regular atraumatic aural toilet may prevent the need for surgical intervention.
- Cauterisation with silver nitrate or trichloroacetic acid of granulation tissue.
Surgical
Meatoplasty is done by removing the fibrous tissue by elevating it from the ear canal bone, the fibrous annulus and lamina propria of the tympanic membrane, through an endaural or retroarticular approach. It can be combined with tympanoplasty, especially in solid cases.
Bony Lesions of External Auditory Canal
These are non-inflammatory, non-infectious structural lesions of the bony EAC.
1. Exostosis
Definition: An exostosis of EAC is a benign bony growth of periosteal compact bone. It presents as a smooth, sessile, hemispherical swelling in the deep part of the canal, close to the tympanic membrane. They are usually multiple, usually three in number, and are bilateral, commonly arising from the anterior and posterior walls of EAC. Males are affected 3:1.
Aetiology:
- Chronic entry of cold water in ear, commonly seen among divers and swimmers.
- Repeated episodes of otitis externa
Symptoms:
- Usually asymptomatic, an incidental finding
- Blocked sensation and itching from wax collection
- Conductive hearing loss
Differential Diagnosis (Osteoma): It needs to be differentiated from osteoma, sometimes called a synonym of exostosis, which is generally a unilateral, solitary, discrete, pedunculated mass, arising from the lateral part of the bony EAC.
Investigation: High-resolution CT scan.
Management:
- In the majority of small and asymptomatic cases, no treatment is required.
- Avoidance of cold water with a recommendation to use earplugs.
- Aural toilet and Topical application of steroid, antibiotic, antifungal or combination ear drops may be necessary to treat inflammation or infection.
- Surgery. It is usually required for cases refractory to medical treatment or large-sized exostosis causing repeated infection or conductive hearing loss. Meatoplasty procedure via a postaural, endaural or permeatal approach is done to restore the normal size of the canal. with careful elevation and preservation of skin overlying the exostoses. The bone of exostoses is removed by high-speed drill, with preservation of skin above the exostosis. Avoid damage to the tympanic membrane and facial nerve.

2. Keratosis Obturans
Definition: Is due to failure of epithelial migration in TM, causing accumulation of a pearly white mass of desquamated keratin in the bony part of EAC. It is associated with osteitis and granulation tissue formation, causing extensive bony erosion leading to gross widening or ballooning of the canal to the point at which the facial nerve can also get involved. KO can occur in normal ears or in ears with plugs of keratin. Intracranial complications are not seen.
Pathophysiology: Normally, epithelium from the surface of the tympanic membrane migrates onto the posterior meatal wall. In KO, there is a grossly abnormal migration pathway of epithelium or obstruction to migration caused by wax, causing accumulation of large keratin plugs in the bony part of the EAC.
Aetiology: Unknown, Hyperaemia of the skin and Irritability of the epidermis.
Clinical features:
- Acute severe otalgia.
- Marked conductive hearing loss, occasionally bilateral.
- Tinnitus.
- Sometimes ear discharge.
- Facial palsy LMN type
- TM is not involved.
- Commonly seen at a young age.
- 90% of patients have a past history of bronchiectasis or sinusitis.
On examination:
- Pearly white mass of keratin material.
- Gross widening or ballooning of the bony meatus.
- Ulceration and even granuloma formation.
- The tympanic membrane shows moderate degrees of thickening.
Treatment:
- Local debridement of the plug by syringing or instrumentation in LA/GA.
- Waxolytic agents (2% sodium bicarbonate) to soften the mass.
- Periodic check-up and cleaning in follow-up with acetic acid solution or keratolytic agent such as 2% salicylic acid in alcohol may reduce the accumulation of debris.
- Meatoplasty with skin grafting is an effective treatment in cases of repeated canal occlusion and severe otalgia.
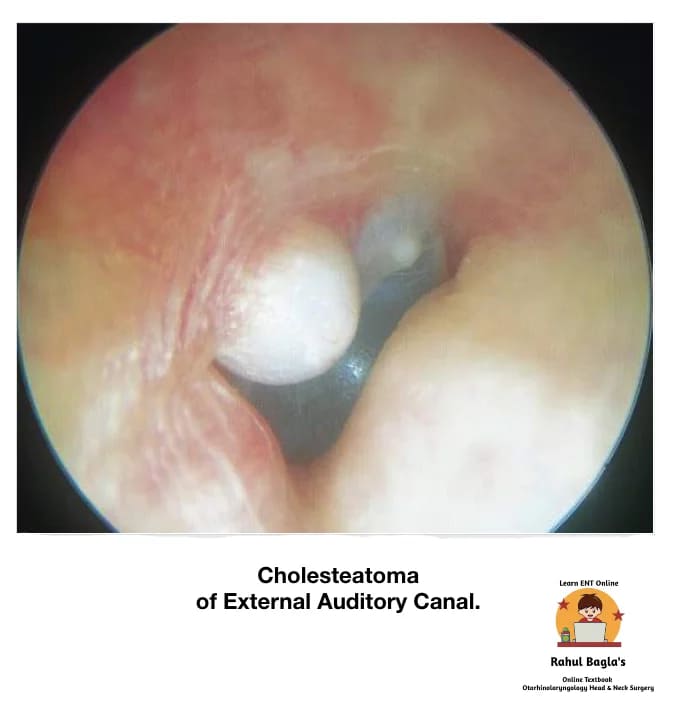
3. Cholesteatoma of External Auditory Canal
Definition: Cholesteatoma of the EAC is similar to keratosis obturans as both shows keratin debris in the canal. However, they are distinct clinical entities. It can be acquired secondary to trauma, surgery or chronic inflammation or may arise spontaneously. The lesion is typically in the floor of the EAC. it should also be differentiated from exostosis. A probe is used to palpate the mass. If its consistency is tender and soft, cholesteatoma is diagnosed.
Aetiology: Uncertain. Infection of abnormal bone exposed in EAC later sequestrates, leading to epithelial migration onto the bony abnormality, forming cholesteatoma.
Clinical features:
- Chronic otorrhoea with dull pain or itching
- Feeling of blockage
- Normal TM
- No associated hearing impairment
- Usually unilateral
- Mostly older patients
Note: Granulations associated with sequestrated bone need histological examination to differentiate it from carcinoma, necrotising otitis externa and a benign sequestrum.
Differential diagnosis:
- Skull base osteomyelitis (SBO)
- Squamous cell carcinoma.
Treatment:
- If the extent of the cholesteatoma erosion is visible – Conservative management.
- If the extent of the cholesteatoma erosion is not visible – Removal of necrotic bone and cholesteatoma and repair of the defect using temporalis fascia.
- Disease involving the mastoid may warrant tympanomastoidectomy to remove the involved bone and repair associated defects.
Reactive Dermatological Disorders
Pathology: The epidermis of the skin of EAC is susceptible to the same dermatologic conditions seen elsewhere in the body. As the skin is very thin and present in almost a closed space, it gives the most annoying symptoms. Usually, all these disorders will respond to local care and removal of allergic factors. Systemic steroids can be given in severe inflammatory disease.
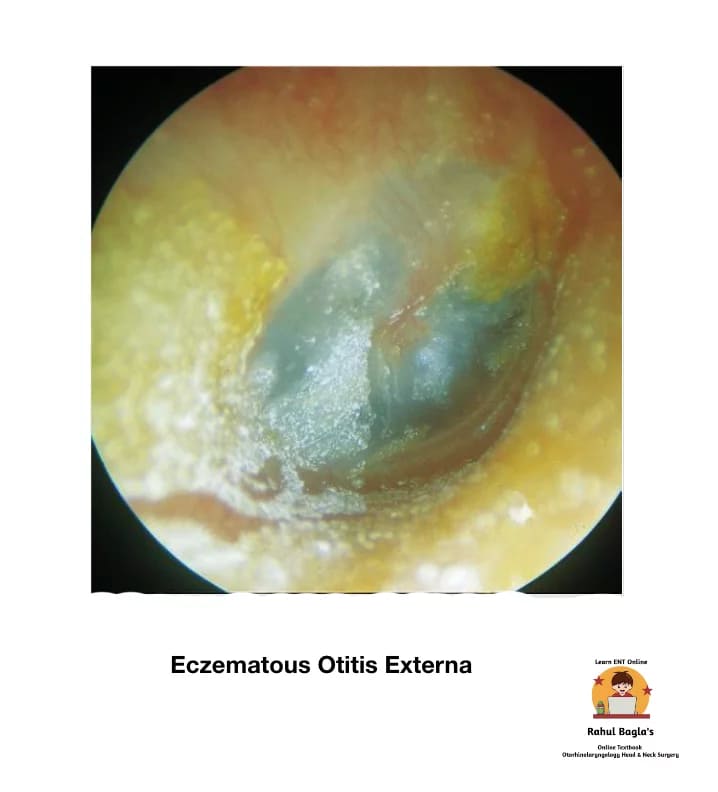
1. Eczematous Otitis Externa
It is an allergic dermatitis and hypersensitivity reaction due to topical ear drops (chloromycetin or neomycin, etc.), infective organisms, jewellery or cosmetic products. It is marked by severe chronic itching, redness, vesicle formation, oozing, crusting, fissuring, and even stenosis of the canal may be present. Treatment is removal of allergic factors (ear drops) causing sensitivity and use of antihistaminics with application of steroid cream and prophylactic antibiotics.
2. Neurodermatitis (lichen simplex chronicus)
It is a neurological disorder characterised by chronic and compulsive itching due to psychological factors. Otitis externa may occur due to repeated scratching. The aetiology is unknown, but insect bite and stress may trigger this condition. Treatment: Psychotherapy and a bandage on the ear to avoid compulsive itching.
3. Seborrhoeic Otitis Externa
It is a very common clinical condition and may remain unnoticed by many patients. It is usually associated with seborrhoeic capitis. It is believed to be triggered by excessive growth of “yeast-like fungi” called Malassezia that live harmlessly on the skin, or a hypersensitivity reaction by the skin’s immune system to this yeast. Affected areas can be itchy, sore, and greasy, and yellow scales may be present. Treatment is aural toilet, application of ointment containing salicylic acid and sulphur, and treating the scalp condition.
Trauma of External Auditory Canal
Aetiology:
- Injury with a blunt or sharp object.
- Physical assault.
- Fall from height.
- Road traffic accident.
- Sports injury.
Treatment:
- Minor injuries (injury by scratching the ear with sharp or blunt objects like hair pins, needles or matchsticks or unskilled instrumentation by the physician) or abrasions usually require no treatment and heal spontaneously.
- If blood is coming out of the meatus, suspect injury in the ear canal and tympanic membrane.
- Extreme bleeding may indicate an associated jugular bulb tear.
- If trismus is present, suspect temporal bone and mandible (trismus) fractures. Any meatal soft tissue should be left alone pending imaging to exclude herniation of the brain/meninges. The goal of treatment is to achieve a skin-lined meatus of sufficient diameter to prevent stenosis of the ear canal.
- CSF leaks close spontaneously requires conservative management. Surgical intervention is via a middle fossa approach if required.
Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear Diseases of External Ear
———— End of the chapter ————
High-Yield Points
- Wax forms in outer 1/3 cartilaginous canal due to sebaceous and ceruminous glands.
- Ear wax is protective because it is acidic (pH 4–5) and antimicrobial.
- Syringing is contraindicated in otitis externa and suspected TM perforation.
- Furuncle occurs in hair-bearing cartilaginous canal, and tragal tenderness is positive.
- Diffuse otitis externa is commonly caused by Pseudomonas aeruginosa.
- Otomycosis causes intense itching and appears like wet blotting paper debris.
- Keratosis obturans causes keratin plug + ballooning of bony canal.
- EAC cholesteatoma causes localized erosion, commonly on canal floor.
- Malignant otitis externa is suspected in elderly diabetic with severe otalgia + granulation tissue.
- Aural polyp suggests middle ear disease, and blind avulsion is dangerous.
- Exostosis is usually multiple and bilateral, while osteoma is solitary and unilateral.
- Chronic otitis externa may lead to acquired canal stenosis/atresia.
NEET PG-Style MCQs
- A 25-year-old swimmer presents with bilateral, painless, smooth, hemispherical bony swellings in the deep part of both ear canals. The most likely diagnosis is: A. Osteoma B. Exostosis C. Keratosis obturans D. Cholesteatoma.
- A patient with impacted wax fails syringing. The next best step is: A. Repeat syringing with higher pressure B. Removal under direct vision using a microscope C. Instill antifungals D. Advise mastoid exploration.
- Severe otalgia, tragal tenderness, and swelling over the mastoid with a normal tympanic membrane suggest: A. Acute mastoiditis B. Furuncle C. Otomycosis D. Glomus tumour.
- Which of the following is an absolute contraindication to ear syringing? A. Hard wax B. Elderly patient C. History of ear discharge D. Unilateral symptom.
- A diabetic patient presents with severe otalgia, purulent discharge, and granulation tissue in the EAC. The most likely diagnosis is: A. Furuncle B. Malignant otitis externa C. Otomycosis D. Cholesteatoma.
- Ramsay Hunt syndrome involves all except: A. Vesicles in EAC B. LMN facial palsy C. Conductive hearing loss D. Vertigo.
- A patient with chronic ear discharge has a fleshy polyp in the EAC. What should you not do? A. Perform aural toilet B. Prescribe antibiotic-steroid drops C. Avulse the polyp blindly D. Biopsy the polyp.
- A 60-year-old male has unilateral, dull otalgia, normal TM, and a soft mass on the floor of the EAC with bone erosion. Diagnosis is: A. Exostosis B. Keratosis obturans C. Cholesteatoma of EAC D. Osteoma.
- All are true about keratosis obturans except: A. Pearly white keratin plug B. Ballooning of EAC C. Intracranial complications are common D. Associated with bronchiectasis.
- The first step in managing otomycosis is: A. Antifungal drops B. Systemic antifungals C. Thorough cleaning of the canal D. Steroid drops.
Answers: 1-B, 2-B, 3-B, 4-C, 5-B, 6-C, 7-C, 8-C, 9-C, 10-C.
Clinical Case Scenarios
Case 1
A 22-year-old swimmer has severe ear pain, itching, and purulent discharge. Pain increases when the tragus is pressed. Most likely diagnosis: Diffuse acute otitis externa, Best management: Aural toilet + topical antibiotic-steroid drops + wick if canal is swollen.
Case 2
A 65-year-old diabetic has severe deep otalgia worse at night with foul discharge. Otoscopy shows granulation tissue on the canal floor. Most likely diagnosis: Malignant otitis externa, Best next step: Hospital referral + imaging + long-term anti-pseudomonal antibiotics + strict glycemic control.
Case 3
A 30-year-old patient has intense itching and musty smelling watery discharge. Otoscopy shows black debris like wet paper. Most likely diagnosis: Otomycosis (Aspergillus), Best management: Aural toilet + keep ear dry + topical clotrimazole.
Case 4
A 15-year-old has severe otalgia and marked conductive hearing loss. Otoscopy reveals pearly white keratin plug with widening of bony canal. Most likely diagnosis: Keratosis obturans, Best management: Debridement under vision + periodic cleaning + keratolytics.
FAQ Section in Viva
- Q: What is the most common cause of otitis externa? A: Moisture exposure with bacterial infection, especially Pseudomonas aeruginosa,
- Q: Why is tragal tenderness important in diagnosis? A: It strongly suggests otitis externa, especially furuncle or diffuse inflammation,
- Q: Can ear wax cause hearing loss? A: Yes, impacted wax can cause conductive hearing loss up to 40 dB,
- Q: What is the best first step in treating otomycosis? A: Aural toilet and keeping the ear canal dry, followed by antifungal drops,
- Q: Why is malignant otitis externa dangerous? A: It can spread to skull base and cause osteomyelitis with cranial nerve palsies,
- Q: How do you differentiate keratosis obturans from EAC cholesteatoma? A: Keratosis obturans causes ballooning canal widening and severe pain, while EAC cholesteatoma causes localized erosion and dull pain,
- Q: When is surgery needed for exostosis? A: Surgery is needed when it causes recurrent infections or significant conductive hearing loss,
———— End ————
Download full PDF Link:
Diseases of External Ear Best Lecture Notes Dr Rahul Bagla ENT Textbook
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: The external auditory canal (EAC) is a narrow, skin-lined tube extending from the concha to the tympanic membrane. It plays a major role in sound conduction and the protection of the middle ear. However, because the canal skin is thin, moist, and exposed to trauma and infection, it commonly develops obstructive, inflammatory, fungal, traumatic, dermatological, and bony disorders. Therefore, a strong understanding of EAC pathology is essential for MBBS theory exams, ENT practicals, viva, and NEET PG MCQs. Microtia, Macrotia, Bat ear, Coloboma, Deformities of Ear Lobule, Congenital Atresia, Collaural fistula, Perichondritis, Relapsing Polychondritis,Wrinkler’s Nodule, Furuncle, Diffuse Acute Otitis Externa, Otomycosis, Haemorrhagic otitis externa, Herpes Zoster Oticus, Aural polyps, Acquired atresia of EAC, Tympanic Membrane Retraction, Retraction Pockets and Atelectasis, Myringitis, Atrophic Tympanic Membrane, Tympanosclerosis, Tympanic Membrane Perforations, Pre-auricular appendage (tags), Preauricular pit, Preauricular Sinus, Keloid of Auricle, Gouty Tophi, Haematoma of the Auricle, Auricular Pseudocyst, Lacerations, Avulsion of Pinna, Frostbite, External canal trauma, Traumatic rupture of tympanic membrane, Exostosis, Keratosis Obturans, Cholesteatoma of External Auditory Canal, Malignant (Necrotizing) Otitis Externa, Skull base osteomyelitis, Eczematous Otitis Externa, Neurodermatitis, Seborrhoeic Otitis Externa, Impacted Wax or Cerumen.Perichondritis, Otomycosis, Herpes Zoster Oticus, Myringitis bullosa, Tympanosclerosis, Malignant (Necrotizing) Otitis Externa, Diseases of External Ear, Disorders of external auditory canal notes, Otitis externa causes and management, Furuncle of ear canal symptoms treatment, Diffuse otitis externa swimmer’s ear notes, Otomycosis diagnosis and treatment, Keratosis obturans vs cholesteatoma difference, External auditory canal cholesteatoma management, Exostosis of external auditory canal surfer’s ear, Osteoma vs exostosis EAC comparison, Malignant otitis externa diabetic patient, Necrotizing otitis externa skull base osteomyelitis, Ear wax impaction removal guidelines, Contraindications of ear syringing, Aural toilet technique ENT, Aural polyp causes management ENT, Acquired atresia of external auditory canal treatment, Eczematous otitis externa allergy ear drops, Seborrhoeic otitis externa treatment, Ramsay Hunt syndrome vesicles facial palsy ENT, Hemorrhagic otitis externa influenza complication, External auditory canal trauma management, ENT external ear canal viva questions, External auditory canal disorders MCQs NEET PG, Otitis externa CBME ENT notes, Ear canal infection treatment guidelines India, External auditory canal revision summary, External auditory canal exam guide MBBS, Otitis externa mnemonics for NEET PG, External auditory canal diseases short notes, Best book notes external auditory canal ENT, Disorders of External Auditory Canal Notes for MBBS, Otitis Externa and Otomycosis Exam Guide ENT, Ear Wax Impaction and Syringing Notes for Students, Keratosis Obturans vs Cholesteatoma Easy Comparison, Malignant Otitis Externa NEET PG High Yield Notes, Exostosis and Osteoma of EAC Simplified ENT Notes, Aural Polyp and Acquired Atresia ENT Revision Guide, Ramsay Hunt Syndrome and Viral Ear Disorders Notes, External Auditory Canal Disorders MCQs with Explanations, External Auditory Canal Viva and Practical Exam Notes, ENTlecture External Auditory Canal Complete Notes