|
The following CBME core competencies are covered in this chapter.
|
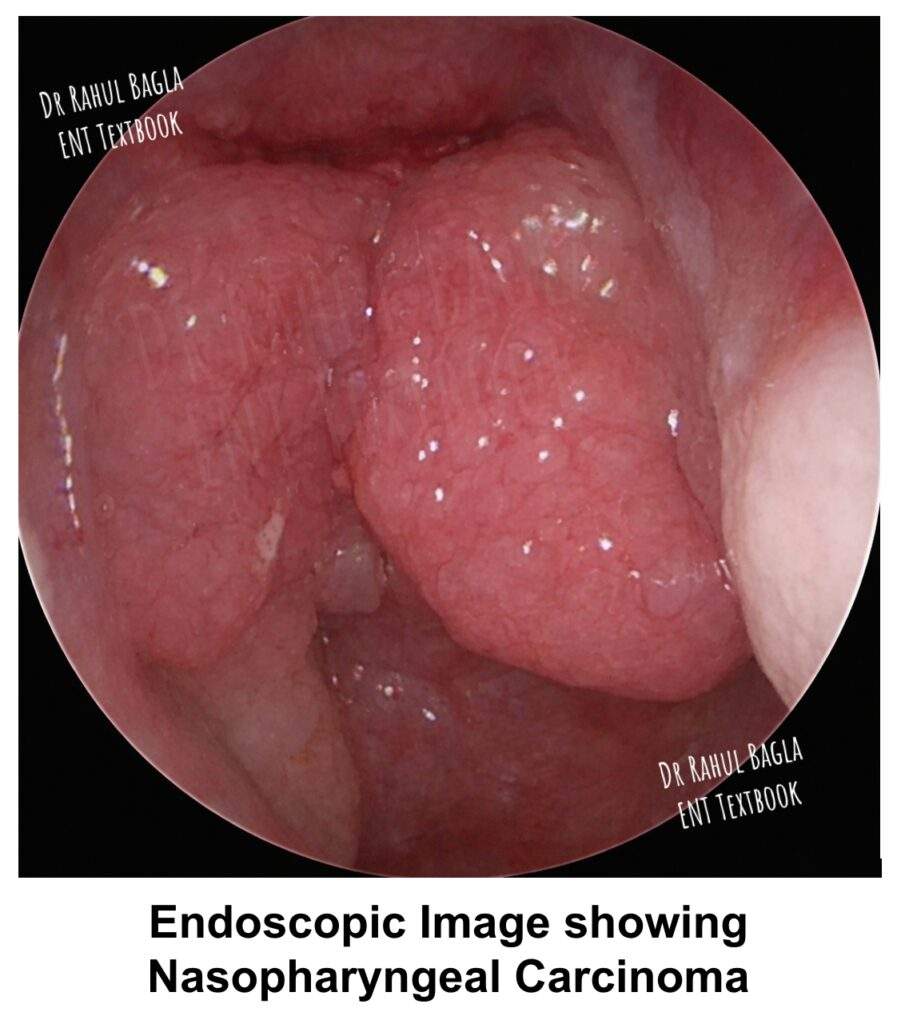
Nasopharyngeal Carcinoma (NPC)
Epidemiology and Geographical Distribution of Nasopharyngeal Carcinoma
NPC presents with the largest geographical variations among all head and neck cancers. Its incidence sharply increases in endemic areas, reaching as high as 50 times that of non‑endemic regions. The highest incidence globally comes from the Guangdong province in southern China. Therefore, physicians sometimes refer to NPC as “Cantonese cancer” because it commonly affects the Cantonese population from southern China and Taiwan. Other countries with a notably higher incidence include Tunisia, Algeria, northern Canada, and Greenland.
NPC is uncommon in India, constituting only 0.41% of all cancers (0.66% in males and 0.17% in females). However, the northeastern region of India shows a higher incidence because people there are predominantly of Mongoloid origin. This observation further supports the role of genetic susceptibility.
The male‑to‑female ratio is 3:1, meaning males are three times more prone than females. The highest age group affected is 50–55 years in endemic areas; nevertheless, NPC can also occur in younger individuals in their twenties and thirties.
Interestingly, people from low‑endemic areas do not show an increase in NPC when they migrate to highly endemic areas, and the reverse is also true. Therefore, genetic factors play a stronger role than environmental factors alone.
Aetiopathogenesis of Nasopharyngeal Carcinoma
The exact aetiology remains unknown; however, three main factors contribute significantly:
- Genetic Factors. There is a strong genetic predisposition to NPC. Chinese individuals have a higher genetic susceptibility, and even after migration to other countries, they continue to have a higher incidence than the local population. Recent studies have identified specific HLA subtypes—HLA A2, B14, and B66—that are associated with an increased risk of NPC.
- Epstein–Barr Virus (EBV). The exact role of EBV is still not fully understood; nevertheless, molecular genetics has confirmed the presence of EBV DNA sequences in the nucleus of carcinoma cells. EBV‑infected cells change the cytokine environment and help carcinoma cells escape detection by the host immune system. Importantly, EBV is only associated with poorly differentiated and undifferentiated forms of NPC (WHO types 2 and 3), not with the keratinising type.
- Environmental Factors. Smoking and eating smoked food items like fish and salmon increase the risk. Burning of incense or wood (which releases polycyclic hydrocarbons) and the use of preserved salted fish (which contains nitrosamines) are additional factors, particularly in China. A vitamin C-deficient diet may also contribute because vitamin C blocks the nitrosification of amines and is thus protective.
EBV for Screening. EBV has two important antigens: viral capsid antigen (VCA) and early antigen (EA). IgA antibodies against EA are highly specific for NPC but have a sensitivity of only 70–80%. In contrast, IgA antibodies against VCA are more sensitive but less specific. Therefore, you should perform both tests for screening patients in high‑incidence areas.
Pathology of Nasopharyngeal Carcinoma
The most common site of origin is the posterolateral nasopharynx, specifically the pharyngeal recess or fossa of Rosenmüller.
Gross Types. The tumour presents in three macroscopic forms:
- Proliferative type: A polypoid tumour fills the nasopharynx and causes obstructive nasal symptoms.
- Ulcerative type: Epistaxis (bleeding from the nose) is the common symptom.
- Infiltrative type: The growth infiltrates submucosally without a visible exophytic component, making diagnosis difficult.
WHO Histological Classification
The WHO classifies NPC into three types:
| WHO Type | Histological Name | Key Features |
| Type 1 | Keratinising squamous cell carcinoma | Similar to well‑differentiated SCC elsewhere, not associated with EBV |
| Type 2 | Non-keratinising carcinoma | Associated with EBV; better response to radiotherapy |
| Type 3 | Undifferentiated carcinoma | Most common in North America; strongly associated with EBV; best response to radiotherapy |
Types 2 and 3 are associated with higher titres of EBV antibodies and have higher local control rates with radiotherapy.
Spread of Nasopharyngeal Carcinoma
- Local spread: From the fossa of Rosenmüller, the tumour spreads in multiple directions. Anterior spread blocks the choana and the nasal cavity. Inferior spread extends towards the oropharynx and hypopharynx. Lateral spread involves the parapharyngeal space and infratemporal fossa through the sinus of Morgagni. Upward spread reaches intracranial structures via the foramen lacerum and foramen ovale. The VIth cranial nerve is the first to be involved intracranially.
- Lymphatic spread: The nasopharynx is rich in lymphatics; therefore, early lymphatic spread to cervical nodes occurs in 75% of patients at presentation. Ipsilateral nodes are involved more often, but contralateral or bilateral nodes can also occur. Spread may occur directly to cervical nodes or indirectly through retropharyngeal or parapharyngeal nodes. Involvement of retropharyngeal nodes causes neck stiffness and torticollis.
- Distant metastases: The lung, bone, and liver are the most common sites. Distant metastases may already be present at the time of diagnosis.
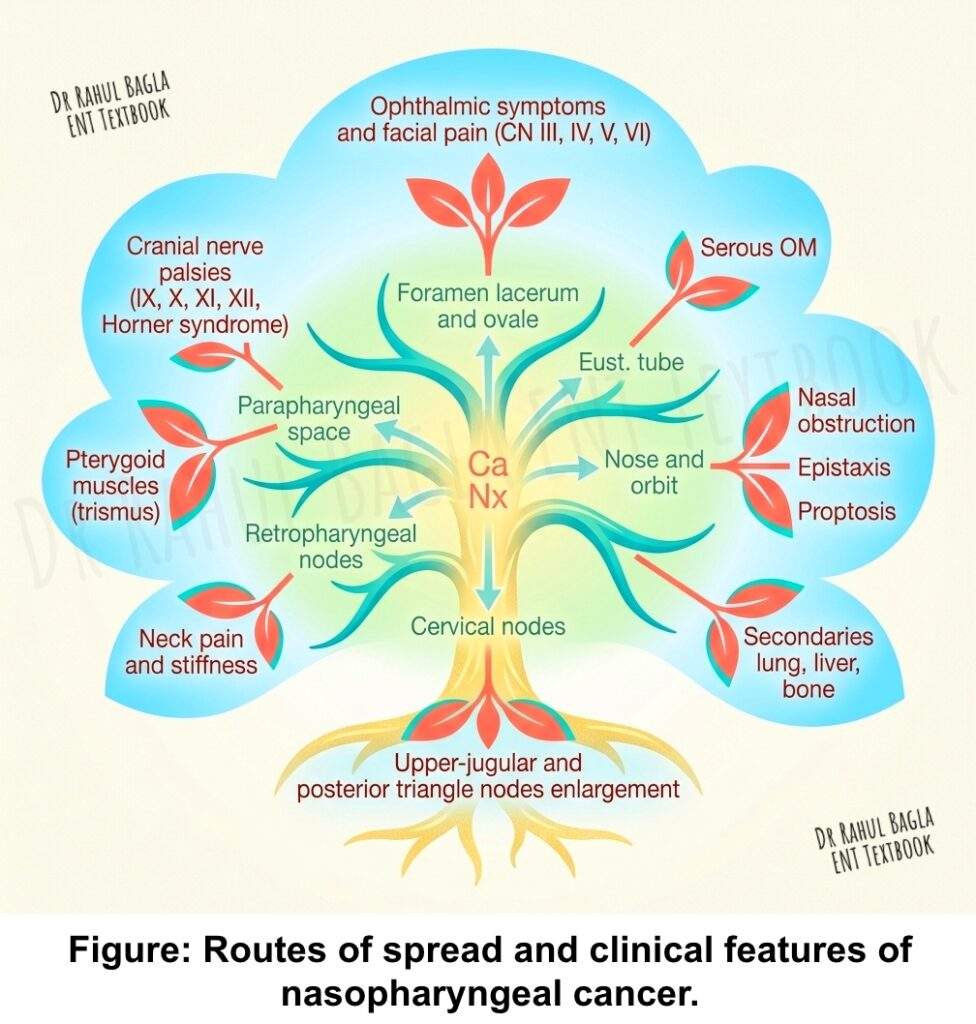
Clinical Features of Nasopharyngeal Carcinoma
- Cervical Nodal Metastases. Cervical lymphadenopathy is the most common presenting symptom (60–90% of patients). The patient typically feels a lump between the angle of the jaw and the mastoid, and some nodes appear along the spinal accessory nerve in the posterior triangle of the neck. About half of these patients have bilateral nodes at presentation.
- Nasal Symptoms. Patients present with nasal obstruction, nasal discharge, denasal speech (rhinolalia clausa), and epistaxis (blood‑stained nasal discharge or postnasal drip).
- Otologic Symptoms. Obstruction of the eustachian tube causes conductive hearing loss, serous or suppurative otitis media, tinnitus, and dizziness. Important clinical pearl: Unilateral serous otitis media in an adult should always raise suspicion of nasopharyngeal carcinoma until proven otherwise. Rarely, the tumour grows up the eustachian tube into the middle ear.
- Ophthalmoneurologic Symptoms. These occur due to the extension of the tumour to the surrounding regions. Nearly all cranial nerves may be involved. Squint and diplopia occur due to involvement of CN VI. Ophthalmoplegia involves CN III, IV, and VI. Facial pain and reduced corneal reflex occur from invasion of CN V through the foramen lacerum. Tumours may directly invade the orbit, leading to exophthalmos and blindness (CN II at the orbital apex). Involvement of CN IX, X, and XI constitutes jugular foramen syndrome, usually due to pressure from enlarged lateral retropharyngeal lymph nodes. CN XII involvement occurs via extension to the hypoglossal canal. Horner syndrome (ptosis, miosis, anhidrosis) occurs due to involvement of the cervical sympathetic chain.
- Other Features. Headache, neck pain, weight loss, trismus (if pterygoid muscles are involved), decreased vision, proptosis, and ophthalmoplegia may also occur.
What Is Trotter’s Triad?
Trotter’s triad (also called sinus of Morgagni syndrome) consists of three ipsilateral findings:
- Palatal palsy due to direct infiltration of the levator palatini muscles (causing nasal regurgitation)
- Hearing loss due to eustachian tube blockage
- Trigeminal neuralgia affecting the mandibular division (V3) of the trigeminal nerve
Diagnosis of Nasopharyngeal Carcinoma
- Endoscopic evaluation: You can perform nasopharyngeal endoscopy under local anaesthesia using rigid or flexible endoscopes. The growth may appear proliferative, ulcerative, or infiltrative (submucosal). You then take a biopsy under endoscopic vision.
- Biopsy: If the growth is not visible but you highly suspect NPC because of metastatic nodes, you can take blind biopsies from multiple sites in the nasopharynx, especially from the fossa of Rosenmüller and the posterior wall. General anaesthesia is preferred if you suspect an occult primary.
- Imaging studies: Contrast‑enhanced CT of the neck and nasopharynx is the study of choice. It reveals the primary growth, erosion of the skull base and clivus, and extensions to parapharyngeal, retropharyngeal, and intracranial regions. MRI is better for soft‑tissue extension. PET‑CT is becoming popular to detect metastases anywhere in the body.
- Audiogram: A baseline audiogram is important for two reasons. First, it establishes the diagnosis of serous otitis media. Second, it serves as a baseline because radiation and chemotherapy can cause sensorineural hearing loss.
- Chest X‑ray or CT chest detects lung secondaries, and ultrasound or CT abdomen detects liver secondaries.
Treatment of Nasopharyngeal Carcinoma
Radiotherapy is the treatment of choice for NPC because the tumour is highly radiosensitive.
Radiotherapy. External beam radiation delivers 6000–7000 cGy to the primary tumour and both sides of the neck using a linear accelerator. Intensity‑modulated radiation therapy (IMRT) uses 3D images of the tumour’s size and shape to deliver external beam radiotherapy with precise dose distribution at different intensities from multiple angles. IMRT allows higher dose delivery to the tumour with reduced damage to adjacent normal structures such as the spinal cord, brainstem, and parotid glands. IMRT is also useful for recurrent disease, where conventional radiotherapy produces more serious side effects such as transverse myelitis.
Chemotherapy. Some stage III and IV cancers can be cured by radiotherapy alone; however, the cure rate doubles when you combine chemotherapy with radiotherapy. You can give chemotherapy concomitantly (concurrent) or after radiotherapy (adjuvant). Cisplatin alone or cisplatin with 5‑FU are the most commonly used regimens. For metastatic disease, you can use 5‑FU with cisplatin, paclitaxel with cisplatin, or cisplatin with gemcitabine. The goal of chemoradiotherapy is to improve local control of the tumour and to treat distant metastases.
Immunotherapy. Immunotherapy is an option for a few patients, especially those with recurrent or metastatic disease who have failed standard chemotherapy.
Stage‑Based Treatment
| Stage | Treatment |
| Stage I | Radiotherapy alone |
| Stage II | Radiotherapy alone or concomitant chemoradiotherapy |
| Stage III and IV | Concomitant chemoradiotherapy (radiotherapy + chemotherapy) |
Treatment of Recurrent or Residual Disease
Recurrent disease can occur in the neck nodes or in the nasopharynx.
For positive neck nodes: You perform a radical neck dissection with removal of the sternocleidomastoid muscle, spinal accessory nerve (CN XI), and internal jugular vein. Modified neck dissection is not preferred because histopathology often shows extensive disease even when only a single node was clinically present. Bilateral neck disease may require bilateral neck dissection, but you should preserve at least one internal jugular vein to avoid cerebral and facial oedema. Before treating positive neck nodes, you must confirm that no disease exists in the nasopharynx and that there are no distant metastases.
For recurrent or residual disease in the nasopharynx: First, evaluate with CT and MRI to assess the size, location, and regional extent. Treatment options include:
- Second course of external radiation using IMRT. However, a second course is more hazardous and can cause injury to the brainstem, eye, ear, pituitary gland, and temporal lobe.
- Brachytherapy delivers a high dose to the tumour with less radiation to surrounding structures. Gold grains (Gold 198) have been used.
- Nasopharyngectomy(surgical removal). You can perform this via several approaches: endoscopic approach, lateral rhinotomy with medial maxillectomy, maxillary swing approach, or Le Fort I approach. Before undertaking nasopharyngectomy, you must exclude intracranial extension, parapharyngeal space extension, or extension around the internal carotid artery. Recurrent localised tumours are now increasingly removed endoscopically.
Staging and Classification of Nasopharyngeal Carcinoma
The WHO classifies NPC histopathologically into three types as described above. Types 2 and 3 are associated with higher EBV antibody titres and show better response to radiotherapy.
For TNM staging, refer to the current AJCC/UICC staging system (8th edition). The key points to remember are that the presence of cervical nodes does not upstage the tumour as aggressively as in other head and neck cancers because NPC is highly radiosensitive and chemosensitive.
Table: TNM Classification of Nasopharyngeal Carcinoma (AJC/UICC 2002)
Primary Tumour (T)
| Category | Description |
| Tis | Carcinoma in situ |
| T1 | Tumour confined to the nasopharynx |
| T2 | Tumour extends to soft tissues of oropharynx and/or nasal fossa |
| T2a | Tumour extends without parapharyngeal extension |
| T2b | Tumour extends with parapharyngeal extension |
| T3 | Tumour invades bony structures and/or paranasal sinuses |
| T4 | Tumour with intracranial extension and/or involvement of cranial nerves, infratemporal fossa, hypopharynx, orbit, or masticator space |
Regional Lymph Nodes (N)
(Special classification for nasopharyngeal carcinoma due to different prognostic behavior)
| Category | Description |
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Unilateral metastasis in lymph node(s), ≤ 6 cm, above the supraclavicular fossa |
| N2 | Bilateral metastasis in lymph nodes, ≤ 6 cm, above the supraclavicular fossa |
| N3 | Metastasis in lymph node(s) > 6 cm and/or in supraclavicular fossa |
| N3a | Lymph node(s) > 6 cm |
| N3b | Metastasis in supraclavicular fossa |
Distant Metastasis (M)
| Category | Description |
| MX | Distant metastasis cannot be assessed |
| M0 | No distant metastasis |
| M1 | Distant metastasis present |
Stage Grouping (AJC 2002)
| Stage | T | N | M |
| 0 | Tis | N0 | M0 |
| I | T1 | N0 | M0 |
| IIA | T2a | N0 | M0 |
| IIB | T1 | N1 | M0 |
| T2 | N1 | M0 | |
| T2a | N1 | M0 | |
| T2b | N1 | M0 | |
| III | T1 | N2 | M0 |
| T2a | N2 | M0 | |
| T2b | N2 | M0 | |
| T3 | N2 | M0 | |
| T3 | N0/N1 | M0 | |
| IVA | T4 | N0/N1/N2 | M0 |
| IVB | Any T | N3 | M0 |
| IVC | Any T | Any N | M1 |
In nasopharyngeal carcinoma, the N classification differs from other head and neck mucosal cancers. Enlarged nodes in the lower neck (supraclavicular fossa) are directly classified as N3, regardless of size. Nodes in the upper neck are given less prognostic weight; therefore, nodes up to 6 cm can still be categorised as N1 or N2, unlike other sites.
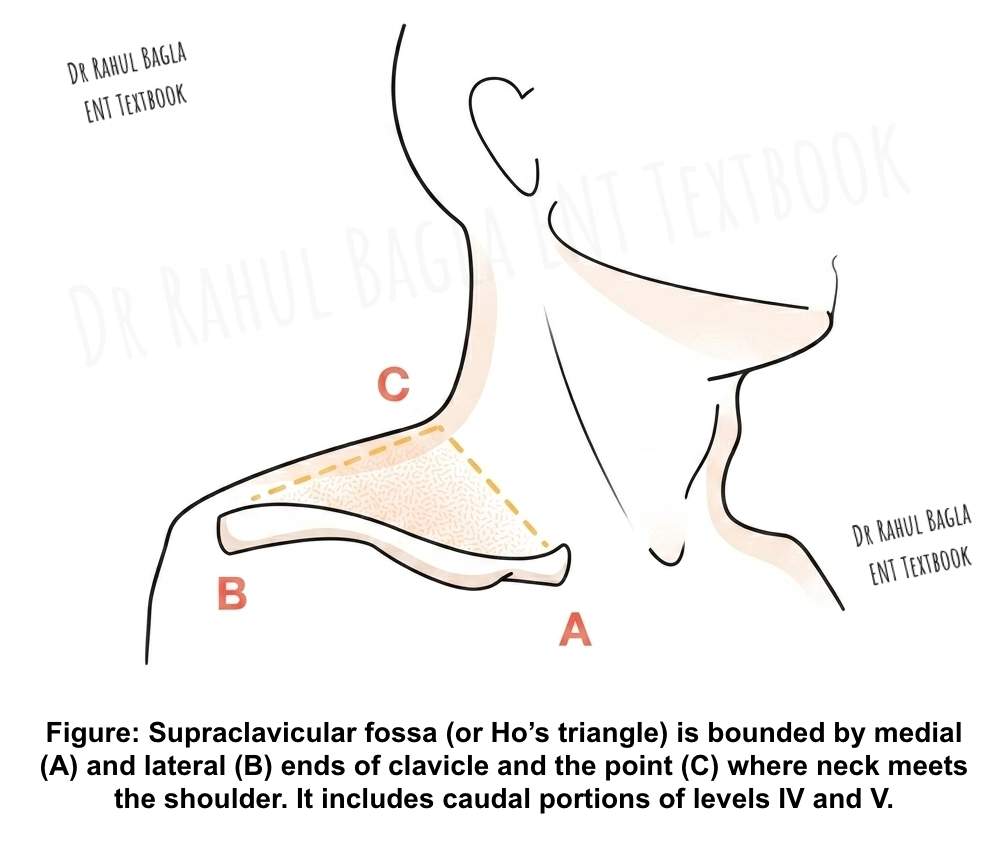
Supraclavicular Fossa (Ho’s Triangle) Definition. Ho’s triangle is the area bounded by:
- Medial end of clavicle,
- Lateral end of clavicle,
- The point where the neck meets the shoulder,
Any lymph node within this triangle is classified as N3b irrespective of size.
—-End of the chapter—-
High-Yield Points (NEET PG & University Revision)
- NPC shows the greatest geographical variation among head and neck cancers.
- Highest incidence occurs in southern China (Guangdong province) – called “Cantonese cancer.”
- Male:female ratio is 3:1; peak age is 50–55 years in endemic areas.
- Genetic factors (HLA A2, B14, B66) play a stronger role than environmental factors.
- EBV is associated only with WHO types 2 and 3 (non‑keratinizing and undifferentiated).
- IgA antibodies against EA (specific) and VCA (sensitive) are used for screening.
- The most common site is the fossa of Rosenmüller (posterolateral nasopharynx).
- The most common presenting symptom is cervical lymphadenopathy (60–90%).
- Unilateral serous otitis media in an adult = rule out NPC until proven otherwise.
- CN VI is the most common cranial nerve involved in NPC.
- Trotter’s triad: palatal palsy + hearing loss + trigeminal neuralgia (mandibular division).
- WHO type 3 (undifferentiated) has the best response to radiotherapy.
- Radiotherapy is the treatment of choice for all stages.
- IMRT delivers precise radiation with fewer side effects.
- Chemotherapy is added for stages II, III, and IV (concomitant chemoradiotherapy).
- For recurrent neck nodes: radical neck dissection (not modified).
- For recurrent nasopharyngeal disease: nasopharyngectomy (endoscopic approach preferred).
NEET PG Style MCQs (10)
- A 55‑year‑old Chinese male presents with unilateral serous otitis media. What is the most appropriate next step? A. Myringotomy with tube insertion B. Prescribe oral antibiotics C. Nasopharyngeal endoscopy with biopsy D. MRI brain.
- The most common presenting symptom of nasopharyngeal carcinoma is: A. Epistaxis B. Hearing loss C. Cervical lymphadenopathy D. Headache.
- Which of the following WHO types of NPC is most strongly associated with Epstein–Barr virus? A. Type 1 (keratinising) B. Type 2 (non-keratinising) C. Type 3 (undifferentiated) D. Both B and C.
- A patient with NPC develops ipsilateral palatal palsy, hearing loss, and trigeminal neuralgia. This triad is called: A. Horner’s syndrome B. Jugular foramen syndrome C. Trotter’s triad D. Cavernous sinus syndrome.
- The first cranial nerve to be involved in intracranial extension of NPC is: A. CN III B. CN V C. CN VI D. CN VII.
- Which of the following antibodies is most specific for screening nasopharyngeal carcinoma? A. IgA against VCA B. IgA against EA C. IgG against VCA D. IgM against EA.
- A 50‑year‑old man completes radiotherapy for stage I NPC. Six months later, a 2 cm node appears in the ipsilateral neck. Nasopharyngoscopy is normal. What is the best treatment? A. Modified radical neck dissection B. Radical neck dissection C. Chemotherapy alone D. Repeat radiotherapy.
- The definitive treatment of choice for stage I nasopharyngeal carcinoma is: A. Chemotherapy alone B. Surgery alone C. Radiotherapy alone D. Chemoradiotherapy.
- Which of the following is NOT a component of Trotter’s triad? A. Ipsilateral palatal palsy B. Ipsilateral hearing loss C. Ipsilateral facial paralysis D. Trigeminal neuralgia.
- A patient with NPC develops ptosis, miosis, and anhidrosis on the left side. This indicates involvement of: A. Oculomotor nerve B. Cervical sympathetic chain C. Facial nerve D. Trochlear nerve.
- Answers: 1: C. 2: C. 3: D. 4: C. 5: C. 6: B. 7: B. 8: C. 9: C. 10: B.
Clinical Case Scenarios
Case 1. A 55‑year‑old Chinese male presents with a 3‑month history of right‑sided nasal obstruction and blood‑stained postnasal drip. He also complains of right ear fullness for 2 months. On examination, you find right serous otitis media. Most likely diagnosis: Nasopharyngeal carcinoma until proven otherwise. Best next step: Nasopharyngeal endoscopy with biopsy. What is the most common histological type in this patient? WHO type 2 or 3 (non-keratinising or undifferentiated) because of the EBV association.
Case 2. A 45‑year‑old male from northeastern India presents with a painless lump in the upper neck on the left side for 4 weeks. He has no nasal or ear symptoms. Examination reveals a 3 cm firm, non‑tender node at level II. The nasopharynx appears normal on mirror examination. Most likely diagnosis: Occult nasopharyngeal carcinoma presenting as cervical metastasis. Best next step: Nasopharyngeal endoscopy under anaesthesia with blind biopsies from the fossa of Rosenmüller. What serological test would you order? IgA antibodies against EBV VCA and EA.
Case 3. A 50‑year‑old man presents with double vision, right facial numbness, and difficulty swallowing for 2 months. On examination, you find right VIth nerve palsy, reduced sensation in V2 and V3 distribution, and palatal deviation to the left. Most likely diagnosis: Advanced NPC with intracranial extension. What is this triad called? Trotter’s triad (palatal palsy + hearing loss + trigeminal neuralgia) – though this patient also has VIth nerve involvement. Best next imaging study: MRI nasopharynx with contrast to assess skull base and intracranial extension.
Case 4. A 60‑year‑old man completes radical radiotherapy for stage III NPC. Six months later, he develops a solitary 2 cm node in the right posterior triangle. Repeat nasopharyngeal endoscopy and biopsy show no evidence of disease. PET‑CT shows no distant metastases. Most likely diagnosis: Isolated cervical nodal recurrence. Best next step: Radical neck dissection (not modified neck dissection). Why not modified neck dissection? Because histopathology often shows extensive disease even when only a single node is clinically present.
Case 5. A patient with recurrent NPC in the nasopharynx after primary radiotherapy is being evaluated for surgery. Which findings would contraindicate nasopharyngectomy? Intracranial extension, parapharyngeal space extension, or encasement of the internal carotid artery.
Frequently Asked Questions in Viva
- What is the most common cause of nasopharyngeal carcinoma? The exact cause is multifactorial; however, the strongest associations include genetic predisposition (Chinese ethnicity), Epstein–Barr virus infection, and environmental factors such as consumption of salted fish and exposure to smoke.
- Why is nasopharyngeal carcinoma called Cantonese cancer? Because the highest incidence in the world occurs in the Guangdong province of southern China, where the Cantonese population lives, and the incidence remains high even after migration.
- What is Trotter’s triad in nasopharyngeal carcinoma? Trotter’s triad consists of ipsilateral palatal palsy (causing nasal regurgitation), ipsilateral conductive hearing loss (due to eustachian tube blockage), and trigeminal neuralgia affecting the mandibular division (V3) of the trigeminal nerve.
- How do you diagnose nasopharyngeal carcinoma? You confirm the diagnosis by nasopharyngeal endoscopy and biopsy. Additionally, you perform contrast‑enhanced CT or MRI for local staging and PET‑CT or chest/abdomen imaging for distant metastases.
- What is the treatment of choice for nasopharyngeal carcinoma? Radiotherapy is the primary treatment. For early stages (I and II), radiotherapy alone suffices. For advanced stages (III and IV), you add concomitant chemotherapy (chemoradiotherapy).
- Which cranial nerve is most commonly involved in NPC? The abducens nerve (CN VI) is the most commonly involved cranial nerve because of its long intracranial course and proximity to the clivus.
- What is the role of Epstein–Barr virus serology in NPC? IgA antibodies against viral capsid antigen (VCA) and early antigen (EA) help screen high‑risk populations. IgA against EA has higher specificity, whereas IgA against VCA has higher sensitivity.
- Can nasopharyngeal carcinoma be treated surgically? Surgery is not the primary treatment. However, you may perform nasopharyngectomy for recurrent or residual disease after radiotherapy, using an endoscopic or open approach.
—-End—-
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Cummings, Otolaryngology-Head and Neck Surgery.
- Stell and Maran’s Textbook of Head and Neck Surgery and Oncology.
- Ballenger’s, Otorhinolaryngology Head And Neck Surgery
- Susan Standring, Gray’s Anatomy.
- Frank H. Netter, Atlas of Human Anatomy.
- B.D. Chaurasiya, Human Anatomy.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery.
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
- Ganong’s Review of Medical Physiology.
- Guyton & Hall Textbook of Medical Physiology.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Keywords: Nasopharyngeal carcinoma notes for MBBS, NPC epidemiology Cantonese cancer, Epstein Barr virus NPC association, Trotter triad nasopharyngeal carcinoma, Unilateral serous otitis media adult NPC, Cervical lymphadenopathy nasopharyngeal carcinoma, WHO classification nasopharyngeal carcinoma types, Radiotherapy nasopharyngeal carcinoma treatment, IMRT intensity modulated radiation therapy NPC, Chemoradiotherapy stage III NPC, Nasopharyngectomy recurrent NPC, Fossa of Rosenmüller nasopharyngeal carcinoma, IgA EBV VCA EA screening NPC, Cranial nerve VI palsy NPC, NEET PG ENT questions nasopharyngeal carcinoma, CBME curriculum NPC head neck cancer, NPC clinical features viva questions, Management of recurrent neck nodes NPC, Radical neck dissection NPC recurrence, NPC distant metastases bone lung liver.